
Abstract
Background
Non-drug interventions are recommended for chronic condition prevention and management yet are underused in clinical practice. Understanding barriers and enablers to using non-drug interventions may help implement non-drug interventions in primary care. We aimed to conduct an overview of reviews to identify and summarise common barriers and enablers for using non-drug interventions for common chronic conditions in primary care.
Methods
We included qualitative and quantitative reviews that used systematic process or methods to examine barriers and enablers to using non-drug interventions for chronic condition prevention and management in primary care settings. We searched 5 electronic databases (PubMed, Cochrane Database of Systematic Reviews, EMBASE, PsycInfo and CINAHL) from inception to September 2022. Two authors independently screened reviews. One author extracted and deductively coded data to Consolidated Framework of Implementation Research (CFIR) (and where relevant, Theoretical Domains Framework [TDF]). A second author validated 10% of extracted data and coding. Data was synthesised thematically using CFIR and TDF. One author assessed the methodological quality of included reviews using a modified AMSTAR 2 tool, with 10% validated by a second author. We assessed overlap between primary studies in included reviews.
Results
From 5324 records, we included 25 reviews, with data predominately from patients. Overall, 130 subthemes (71 barrier and 59 enabler) were identified across 4 CFIR domains (Innovation, Outer Setting, Inner Setting, and Individuals), and all TDF domains. Common barrier and enabler subthemes were identified for CFIR constructs of Innovation Adaptability, Innovation Cost, Innovation Relative Advantage, Local Attitudes, External Pressure, Local Conditions, Relational Connections, Available Resources, and Access to Knowledge and Information. For TDF domains, important barrier and enabler subthemes were identified for Knowledge, Skills, Environmental Context and Resources, Beliefs about Consequences, Reinforcement, and Emotion.
Conclusions
We synthesised reviews to provide new insight into common barriers and enablers for using non-drug interventions to prevent and manage chronic conditions in primary care. The factors identified can inform the development of generalisable implementation interventions to enhance uptake of multiple non-drug interventions simultaneously.
Trial Registration
This study was registered in PROSPERO (CRD42022357583).
Similar content being viewed by others


Background
Chronic health conditions are a major health burden, attributed to nearly three-quarters of all deaths annually [1, 2], and rates are rising [3]. Primary care services play a key role in chronic condition management, particularly through treatment and risk factor prevention and modification [4, 5]. Non-drug interventions (NDIs; also called lifestyle, or non-pharmacological interventions), such as dietary strategies, exercise, physical therapies, and psychological therapies, are frequently recommended in chronic condition prevention guidelines [6], and condition-specific management guidelines [7,8,9,10]. For example, international clinical practice guidelines for the management of osteoarthritis routinely recommend lifestyle and non-drug management options as first-line treatment [7,8,9, 11].
Despite this, observational evidence from the United States and United Kingdom suggests that patients with chronic conditions do not always receive lifestyle advice, when appropriate [12,13,14,15]. Analysis of the National Health and Nutrition Examination Survey (NHANES) from 2011 to 2016 show the proportion of patients in the United Kingdom with chronic conditions who receive advice varies, with patients with type 2 diabetes most likely to receive advice (56.5%), while patients with hypertension or high cholesterol received advice less often (31.4 to 27% respectively) [13]. Interestingly, lifestyle advice was rarely provided to adults without chronic conditions in the normal weight range (1–9%), despite being a known preventative strategy to reduce incidence of chronic conditions [13]. Subsequent analysis of NHANES data from 2015 to 2018 shows that receiving lifestyle advice is associated with higher likelihood of weight loss, increased physical activity, and reduced dietary sodium and fat intake, suggesting advice provision is associated with a reduction in risk factors [15].
The underuse of effective NDIs [16, 17] suggest factors inhibit their use in practice. Existing reviews of barriers and enablers often focus on specific stakeholders, interventions, or conditions. For example, a 2021 systematic review of primary care clinicians’ perceived barriers and enablers to dietary management of people with type 2 diabetes reported barriers including limited time for staff training, limited dietary knowledge, and lack of confidence in discussing dietary advice [18, 19]. While it is useful to understand condition or context-specific factors to implementing dietary management interventions, they may not generalise to different health conditions or interventions (i.e., we do not know whether clinician’s lack of confidence to discuss NDIs is unique to dietary advice interventions, or applies to other NDIs, such as physical activity advice). To address underuse of effective NDIs in primary care, understanding common reasons why clinicians and patients do or do not use effective NDIs more routinely is required.
To enable broader NDI implementation or to target multiple NDIs simultaneously, identifying and summarising the common factors for using or not using NDIs for chronic conditions is needed. Therefore, we aimed to conduct an overview of reviews to identify and summarise common barriers and enablers for using non-drug interventions for common chronic conditions in primary care. To encapsulate different domains for implementation and to ground our analysis in theory, we examined the results using the Consolidated Framework of Implementation Research (CFIR) and the Theoretical Domains Framework (TDF) [20].
Methods
We prospectively developed a protocol for this overview and registered it in PROSPERO (CRD42022357583) and published it on Open Science Framework [21]. The Cochrane Handbook on Systematic Reviews of Interventions guided the study methods (“Overview of Reviews” chapter V) [22], and we reported results according to Preferred Reporting Items for Overview of Reviews (PRIOR) guidelines (see Additional File 1) [23]. Systematic review automation tools were used to facilitate deduplication, screening, and dispute resolution [24, 25].
Eligibility criteria
We included full-text articles fulfilling Sample, Phenomenon of Interest, Design, Evaluation, Research type (SPIDER) criteria (Table 1) [26].
Search
Information sources
We searched 5 electronic databases: PubMed (MEDLINE), Cochrane Database of Systematic Reviews, EMBASE, PsycInfo, and CINAHL from inception to 7 September 2022 without language restrictions.
Search strategy
The search strategy combined free text and MeSH terms around 4 key concepts: ‘non-drug interventions’, ‘barriers/enablers’, ‘primary care’ and ‘systematic/scoping review’, and was peer-reviewed by a librarian, with additional input from a senior information specialist (Additional File 2). The search string was developed for PubMed and was translated using the Polyglot Search translator [28]. We deduplicated search results using an automated duplicate detection tool [25].
Study selection
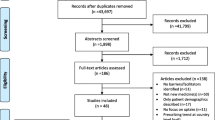
Two reviewers (HG and AD) independently screened deduplicated titles and abstracts against inclusion criteria (Table 1). Non-English title and abstracts were translated using Google translate, though no eligible non-English studies were identified. Two reviewers (HG and AD) independently screened full text articles (retrieved by HG). Any disagreements were resolved by discussion or referral to another reviewer (LA), if no consensus. We manually searched for and screened full text articles of abstract-only records excluded at the full text stage (“other methods”). A flow diagram is used to represent study selection (Fig. 1) [29].

PRISMA 2020 Study 1 Flow Diagram
Quality assessment
Risk of bias assessment
We adapted AMSTAR 2 risk of bias (RoB) assessment tool referring to items from the CASP tool for systematic reviews, to assess RoB in reviews of qualitative studies. This adapted AMSTAR2 was piloted on two reviews by two independent reviewers (HG and LA) with good agreement (see Additional File 3 for a summary of changes). One reviewer (LA) assessed the RoB of the remaining included reviews. We elected to use an adapted AMSTAR tool as no dedicated tool to assess reviews of qualitative studies exists and our study includes a combination of qualitative, quantitative and mixed methods studies. The adjustments made were informed by examining JBI systematic review tools which includes some guidance on assessing quality of qualitative reviews [30]. We also extracted the RoB of the primary studies in included reviews. We did not independently assess the RoB of primary studies, if not reported by the original review authors.
Certainty of evidence
When reported in the included systematic reviews, we extracted the GRADE-CERQual assessment conducted by the original review author. We did not independently assess the certainty of evidence if not reported.
Data collection and analysis
One reviewer (HG) extracted data from all review articles using a data extraction sheet piloted by two reviewers (HG and AD) on 10% of included reviews. A second independent reviewer (AD) validated extracted data and coding for 10% of reviews and was discussed between the two reviewers (HG and AD) until agreement achieved. If multiple reviews of the same NDI and condition (e.g., exercise for heart disease) were found, the most recent review was extracted first, working backward by publication date until no new barriers or enablers were identified. In instances where data was unclear or incomplete, study authors were contacted. The following data was extracted from reviews:
-
Characteristics: countries of included primary studies, number and type of included primary studies, number of participants, participant type and description, reported chronic condition, reported NDI, method used for analysis, method used for RoB assessment;
-
Primary study overlap: Included primary studies within reviews and RoB rating;
-
Outcomes: barriers and/or enablers including theme and certainty of evidence.
Two key determinant frameworks (i.e., frameworks which help understand or explain factors which influence implementation outcomes) were applied in this review of reviews. First, the Consolidated Framework of Implementation Research (CFIR) was used to assess contextual factors to inform implementation strategies [31]. Reflective of the dynamic nature of implementation theory, CFIR was recently updated to centre intervention recipients and include equity determinants, with further critique and advancements encouraged by the authors [31]. Second, the Theoretical Domains Framework (TDF), which was developed to understand health professional implementation behaviour and is used to examine influences on behaviour [20].
We deductively coded each extracted barrier or enabler extracted using CFIR (and TDF if in the Individual CFIR domain). We examined each CFIR and TDF code to identify barrier and enabler theme and subtheme groups. During this, CFIR and TDF codes were iteratively revised to ensure consistency across extracted barriers and enablers. Due to the variety of interventions identified, barriers and enablers were not tabulated by intervention or condition, as per protocol.
We assessed the degree of overlap between primary studies by building a matrix of included reviews and their included primary studies. We used the graphical representation of the degree of overlap (GROOVE) tool to graphically represent the degree of overlap and calculate the Corrected Covered Area (CCA), a measure of the degree of overlap between primary studies [32,33,34]. Overlap is considered slight if the CCA is < 5%, moderate if it is ≥5% and < 10%, high if it is ≥10% and < 15%, and very high if CCA is ≥15% [33, 34]. Due to the variation in primary study health condition and NDI, structural missingness was not assessed.
Results
Study selection
After deduplication, 5324 title and abstract records were screened to identify 192 full-text records of which we included 24 reviews. One study was identified via other methods (Fig. 1). Overall, 25 reviews were included (Fig. 1). See Supplementary Table 1, Additional File 4 for a list of excluded reviews and reasons for exclusion.
Characteristics of included reviews
Characteristics of included reviews (and the primary studies included in those reviews, where relevant) are summarised in Table 2; see Supplementary Table 2, Additional File 5 for detailed characteristics. Primary studies of included reviews were conducted in 24 countries across Africa, Asia, Europe, the Americas, and Oceania, but mostly in Europe or North America. Most included reviews reported data from patients (n = 23, 92%) and included qualitative (n = 24, 96%) or mixed methods (n = 8, 32%) primary studies. Included reviews were conducted across a range of specific chronic health conditions, while some reviews included studies from various chronic health conditions (n = 5, 20%). Physical activity or exercise were the most common NDIs examined in included reviews (n = 10, 40%). Some reviews addressed several interventions (e.g., included a combination of physical and nutritional components; n = 4, 16%).
Primary study overlap
Twenty-five included reviews had 452 unique primary studies. Of these, 410 appear in 1 review, 15 appear in 2 reviews, and 4 appear in 3 reviews. There is slight (< 5%) overlap of primary studies between included reviews (CCA = 0.21%). Of 300 nodes (pairs of review), 296 nodes have slight overlap (< 5%), while 4 nodes have very high (≥15%) overlap (Additional File 6). We identified two of these review pairs ([35, 36] and [37, 38]) during data extraction. As per protocol, we extracted the most recently published review first, and only extracted novel barriers and enablers for the older review. Another review [39] had very high overlap with 2 reviews [37, 38], but was not identified during data extraction, so extracted it in full. As no measure of effect size is estimated, we took no further action.
Critical appraisal of included reviews
Included reviews
Modified AMSTAR assessment indicates most reviews used a comprehensive search strategy (n = 15, Yes 60%; n = 9, Partial Yes 36%), a satisfactory technique for assessing RoB (n = 15, Yes 60%; n = 5, Partial Yes 20%) and appropriate methods to combine results (n = 18; Yes 72%). Approximately half the reviews had a registered protocol (n = 8, Yes 32%; n = 4, Partial Yes 16%). In most reviews, authors did not: perform data extraction in duplicate (n = 18, No 72%), report sources of primary study funding (n = 23, No 92%), or assess the potential impact of primary study RoB on the results (n = 22, No 88%). AMSTAR ratings are represented graphically by question (Fig. 2) and by study (Fig. 3). See Additional file 7 for a summary of primary study RoB.

Modified AMSTAR rating by question

Modified AMSTAR rating by study
Summary of findings
We identified 71 barrier and 59 enabler subthemes across 4 CFIR domains: Innovation, Outer Setting, Inner Setting, and Individuals [31]. See Table 3 for subthemes for Innovation, Inner Setting and Outer Setting domains, and Table 4 for subthemes related to Individual Domain with TDF codes [20].
Innovation domain
Across constructs of Innovation Relative Advantage, Innovation Adaptability, Innovation Complexity, Innovation Design and Innovation Cost, we identified seven barrier and five enabler subthemes from 21 reviews [31] (Table 3), and highlight five key subthemes (4 barriers and 1 enabler).
Flexibility of intervention characteristics and delivery (CFIR: innovation adaptability)
We identified two factors around the theme of intervention flexibility. When the intervention adopts a ‘one size fits all’ approach, patients and clinicians perceive it as impersonal or patronising, creating a barrier (4 reviews [37, 38, 40, 45]). “A lot of the participants reported feeling they already knew the information presented in [e-cognitive behavioural therapy], and that this was not tailored to their individual needs and situation […] there was a general sense that it was not a complete intervention, often summed up in a phrase to the effect that ‘It wasn’t for me but could help someone else’” [45]. Conversely, a flexible, tailored or personalised intervention facilitates both patient and clinician acceptability of and engagement with the NDI (14 reviews [35, 37, 38, 40,41,42,43, 45,46,47,48,49,50,51], low certainty of evidence from 1 review [43]).
Costs associated with the intervention (CFIR: innovation cost)
We identified that actual or perceived costs of the intervention as a key barrier for patients (8 reviews [37, 38, 40, 46, 52,53,54,55]). “Look, the barrier to those goal settings is budget, you know […] So, don’t go telling poor people ‘you’re going to get diabetes if you eat this and this and this’; so we want you to eat this food, but it’s too expensive for you to buy, you know” [46].
Relative benefit of NDIs (CFIR: innovation relative advantage)
One review reported a barrier that healthcare practitioners were less likely to prescribe a NDI due to comparative ease of prescribing medication (moderate to high certainty of evidence from 1 review [18]). This may relate to clinician or patient perception that NDIs are irrelevant to health management (5 reviews [40,41,42,43,44], 2 reviews reported variable certainty of evidence: very low [44], high [43]).
Outer setting domain
We identified nine barriers and seven enabler subthemes from 19 reviews across constructs of Local Attitudes, Local Conditions, Policies and Laws, Financing, External Pressure, and subconstruct Societal Pressure [31] (Table 3) and highlight four key subthemes (three barriers and 1 enabler).
Attitudes and awareness towards medical condition in local community (CFIR: local attitudes)
We identified negative societal attitudes towards the health condition as a barrier for patients in seven reviews [18, 38, 39, 43, 45, 54, 55] (low certainty evidence from one review [18]). Examples included peer pressure to fit in by concealing health condition symptoms and social stigma (e.g., actual or perceived negative perception towards health condition). “Most participants described negative experiences of being misunderstood, judged and stigmatised because of their depression. They learned to mask their feelings, adopting an appearance of wellness and keeping people at a distance. Most participants described this as an isolating experience” [45].
Sociocultural pressures (CFIR: external pressure)
Similarly, we identified external sociocultural pressures (e.g., the intersection between food and culture or traditional gender roles around food preparation), as a patient barrier in five reviews [18, 46, 53, 55, 58] (low certainty evidence from 1 study [18]). “My whole family eats white rice since young, it has become a habit, a culture in us. Now say change to brown rice, not easy, it takes time for us to adjust to the new taste of brown rice” [46].
Access to facilities and services (CFIR: local condition)
Access to facilities and services is an important factor for patients. Five reviews [36, 38, 44, 46, 53] identified lack of available goods or services to access the NDI as a barrier (moderate to high certainty evidence from 2 reviews [36, 44]). Ease of access to places/spaces to participate in the NDI enabled engagement (2 reviews [46, 56]).
Inner setting domain
We identified 20 barrier and 21 enabler subthemes from 24 reviews across constructs of Structural Characteristics [all subconstructs], Relational Connections, Communication, Culture [Recipient Centredness subconstruct], Compatibility, Incentive Systems, Available Resources [Space, and Materials and Equipment subconstructs], and Access to Knowledge and Information) [31] (Table 3). Eleven key subthemes (six barriers and five enablers) are highlighted.
Personal, therapeutic, and professional relationships (CFIR: relational connections)
The therapeutic relationship between clinician and patient is crucial. When poor, due to lack of continuity, disagreement or distrust, it can act as a barrier for both parties (11 reviews [18, 37, 40,41,42,43, 51, 55,56,57,58]). Conversely, a high-quality, trusting relationship enables use of NDIs (12 reviews [18, 37,38,39,40,41,42,43, 45, 47, 54, 55]). Similarly, lack of support from family/friends or others with the same condition acts as a barrier (12 reviews [35,36,37,38,39,40,41, 49,50,51, 54, 55, 57]), while good relationships, support and encouragement serve as an enabler (18 reviews [37,38,39,40, 42, 43, 45,46,47,48,49,50,51, 54,55,56,57,58]). “And I found the whole process valuable, particularly going along with other people who had similar problems and sharing their problems with them” [56]. Three reviews reported variable certainty of evidence ratings for these themes: low [43], moderate [18, 43], high [18, 36, 43].
Access to NDI prescriptions and information (CFIR: available resources, access to knowledge and information)
Patients and clinicians face barriers in accessing NDI prescriptions and information about them. A patient barrier in 6 reviews was the challenge in accessing services for NDI prescription, due to service unavailability or prohibitive wait times [4,5,6, 8, 18, 20, 24]. Insufficient time or staffing to provide the NDI prescription was a key barrier for clinicians in health service settings (13 reviews [18, 37, 38, 40, 41, 43, 44, 48, 51, 52, 54, 56, 58]). Other important patient enablers were the availability of, and access to, relevant education materials (availability: 5 reviews [40, 45, 47, 51, 57], high certainty evidence from one review [18]) (access: seven reviews [40, 46, 47, 50, 52, 54, 55]). Lack of these materials is a barrier (three reviews [18, 39, 41]).
Individual domain
Across the roles subdomain constructs of Innovation Deliverers, Innovation Recipients, and Other Implementation Support and characteristics subdomain constructs of Capability, Opportunity and Motivation, we identified 35 barrier and 26 enabler subthemes from 25 reviews, which mapped to all TDF domains [20] (Table 4). Seventeen key subthemes (11 barriers and 6 enablers) are highlighted.
Knowledge and awareness (CFIR: capability; TDF: knowledge)
We identified lack of knowledge about the health condition (10 reviews [35, 36, 39,40,41, 43, 45, 52,53,54], high certainty evidence from 1 review [43]) or NDI (9 reviews [18, 36, 38, 42, 44, 45, 52, 53, 55], variable certainty evidence from 3 reviews [18, 36, 44]) as a major patient and clinician barrier. “Most [general practitioners] were unfamiliar with the conservative interventions other than medication, such as cognitive-behavioural therapy, spinal manipulations, and exercises.” [44]. Conversely, knowledge about the health condition or health condition management is a patient enabler in 6 reviews [36, 43, 47, 54, 55, 57], with moderate certainty evidence from 1 review [43].
Health condition management skills (CFIR: capability; TDF: skills)
Clinicians face a key barrier in lack of skills to clearly and effectively communicate about benefits and harms or lifestyle changes (seven reviews [40, 41, 43, 44, 53,54,55], moderate to high certainty evidence from two reviews [43, 44]). For patients, lack of self-management skills acts as a barrier (five reviews [38, 40, 48, 54, 55]), while presence of self-management skills enables use of NDIs (seven reviews [38, 40, 43, 46, 47, 52, 57], moderate certainty evidence from 1 review [43]).
Personal circumstances and resources (CFIR: opportunity; TDF: environmental context and resources)
Patient’s symptoms such as pain or fatigue, due to the target health condition (14 reviews [35,36,37,38,39, 42, 43, 47, 49, 51, 52, 55, 56, 58], high certainty evidence from 1 review [36]) or a comorbid health condition (7 reviews [38, 40, 49, 50, 52, 54, 55]), inhibit NDI engagement. “I can’t exercise too much sometimes. My knees can’t take it. Because we are getting on in years as well as sometimes it hurts. There was once when I went for a walk and I had leg cramps after I went back. It’s really painful” [58]. Barriers of personal or family stressors, such as workload or difficulties accessing childcare, also interfere with NDI engagement (8 reviews [37, 38, 40, 46, 47, 52, 53, 55]). “I am always so busy. .. in the evenings there are always papers to look at, I have no time for exercise.. . I simply don’t have the time” [46].
Beliefs and assumptions (CFIR: motivation; TDF: beliefs about consequences)
The belief that using a NDI is either useless or harmful is a barrier for clinicians and patients (9 reviews [35,36,37,38, 40, 42, 43, 51, 52], variable certainty evidence from 2 reviews: low [43]; high [36]). “…there is nothing that can be done about the [osteoarthritis]; therefore, I do nothing…” [36]. However, the perception that the NDI can control the condition and condition progression is an enabler (4 reviews [35, 36, 39, 40], low certainty evidence from 1 review [36]). Disbelief or denial about the health condition also inhibits NDI engagement for patients (4 reviews [38, 40, 46, 53]).
Reinforcement and feedback loops (CFIR: motivation, TDF: reinforcement)
Several factors enable NDI engagement via reinforcement. Patient health improvements from using the NDI prompts further engagement (9 reviews [36,37,38,39, 42, 46, 47, 49, 55], high certainty evidence from 1 review [36]). Using reminder or monitoring systems to track progress, medication or symptoms is also helpful (5 reviews [37, 38, 40, 46, 52] ““I have a Fitbit that makes it easier, because I like to challenge myself to make sure I get my steps every day. So, lots of times, I’ll get home in the evening and I’ll see them at 9000 steps, and I’ll like go out and walk up and down the driveway” [46].
Emotion as a regulator of engagement (CFIR: motivation, TDF: emotion)
Negative emotions regulate patient engagement with NDIs in various ways. Emotions like fear, anxiety, and powerlessness can inhibit engagement with NDIs (8 reviews [18, 38, 40, 46,47,48,49,50], moderate certainty evidence from 1 review [18]). Feelings of depression or anxiety can impact general wellbeing, coping and self-esteem (7 reviews [38,39,40, 42, 49, 51, 56]). Interestingly, emotions like guilt and shame can enable engagement with NDIs (4 reviews, [40, 46, 47, 52]).
Discussion
In this overview of reviews, we aimed to thematically synthesise reviews examining barriers and enablers to using NDIs for chronic condition management in primary care. Overall, across 25 included reviews, we identified 71 common barrier and 59 common enabler subthemes across Innovation, Inner Setting, Outer Setting and Individual CFIR Domains [31]. As the included reviews examined barriers and enablers to using NDIs after implementation in practice, we did not identify any subthemes for the CFIR Process domain. We also examined factors identified in the Individual domain using the TDF to allow for more in-depth analysis [20, 59].
Key themes related to the Innovation (NDI) are flexible intervention characteristics for patients and clinicians alike, costs associated with the intervention for patients, and the relative benefit of NDIs. The ability to tailor or personalise an NDI facilitates engagement, while a “one size fits all” approach is perceived as impersonal and represents a barrier. Recent meta-ethnographic evidence suggests that patients receiving weight management care from their general practitioners sought care tailored to their individual needs. However, general practitioners may be ill-equipped to provide individualised advice, due to lack of available guidance, training or resources [60]. Providing clinicians with appropriate training and resources to tailor NDIs may enable clinicians to provide this personalised advice. Actual or perceived NDI costs (e.g., cost associated with a prescribed dietary strategy or exercise plan) are an engagement barrier for patients. Many studies examine cost-effectiveness of delivering NDIs from a health system perspective (e.g., nutrition care [61] or hypertension treatments [62]), but there is less consideration of the intervention cost to patients. There may be an incorrect perception that NDIs are costly. For example, while there are some programs for internet-delivered cognitive behavioural therapy for depression that have associated costs, there are also no-cost options available [63]. Ensuring that NDIs are affordable compared to drug interventions, supporting patients to access no or low-cost options, providing comparison of medication vs NDI costs, and challenging beliefs that they are inherently unaffordable, may help support uptake of NDIs. Although only identified in one included review, the barrier of clinician not prescribing NDIs due to the comparative ease of prescribing medication is noteworthy. Although some progress has been made on NDI prescription, particularly for exercise [64, 65], further examination of the NDI prescription process would be beneficial.
Some Outer Setting (e.g., community) factors influence patient engagement in NDIs, include local attitudes towards the health condition, sociocultural pressures, and access to facilities and services. The first two factors are difficult to address, but lack of available goods and services to access the NDI once prescribed is potentially changeable. Although not in primary care, recent systematic review evidence shows that a major external factor influencing self-management for chronic pain was intervention accessibility, including location of facilities and service availability [66]. Having accessible spaces and places to engage with prescribed NDIs, as well as having available community services to provide NDIs may enhance engagement with NDIs. For example, a water-based exercise prescription for knee osteoarthritis is inappropriate if the patient does not have access to private or public pool facilities.
We identified two key themes in the Inner Setting domain: access to NDIs (both prescription and information), and personal, therapeutic, and professional relationships. The availability of, and access to educational information about NDIs enables patient engagement, though the availability of these resources may be lacking. Online non-drug resources like Royal Australian College of General Practitioners’ Handbook of Non-Drug Interventions (HANDI) provides information for clinicians, though some interventions also have patient resources [67]. There is some evidence from a recent, unpublished Australian survey exploring clinicians awareness and use of HANDI, that one-third of clinicians are unaware of this resource, and of those that are aware, half rarely use it [68]. Given that this is a clinician-focussed resource, without clinician guidance it is unlikely that patients will be aware of such guidelines. Improving educational materials about NDIs, and enhancing access to these materials, may support delivery of NDIs in primary care. Further, for patients, accessing services to prescribe NDIs can be a challenge, possibly related to the clinician barrier of insufficient time or staffing to deliver the NDI. A systematic review of barriers and enablers to implementation of physical activity interventions in primary care found similar barriers in the Environmental Context and Resources TDF domain, including lack of professionals to deliver the intervention [69]. Similarly, evidence from a narrative review examining underuse of NDIs for headache found there are few clinicians trained in NDI approaches, potentially explaining these access difficulties [70]. The therapeutic relationship between clinician and patient can act as a barrier or enabler to use of NDIs, depending on the quality of the relationship. It has been well-established that quality of the relationship between clinicians and patients has a positive effect on patient outcomes [71, 72]. Our results suggest that an aligned clinician-patient relationship can influence engagement in NDIs. This is somewhat supported by recent integrative review evidence that person-centred communication and trust in the relationship was an important factor in lifestyle risk communication [73]. Several of the factors in this domain (access to educational resources and skills to communicate about NDIs) are related to findings in the Individual domain.
Within the Individual domain, some key, interrelated factors influence use of NDIs include knowledge and awareness, skills to manage the health condition with NDIs, and assumptions and beliefs about NDIs. Lack of knowledge about NDIs is a major barrier for both clinicians and patients, and has been consistently identified as a factor in previous research [66, 74]. For clinicians, this may be due to a lack of awareness of non-drug guidelines [75], and broader lack of training, skills or confidence in skills in delivering NDIs [73]. For patients, a problem with availability of, or access to, NDI educational resources may explain this knowledge gap. We also found that some patients and clinicians believe NDIs are useless or harmful. Improving availability of, or access to, high quality information about NDI may have the dual benefit of addressing this belief and improving knowledge about NDIs more broadly. Another major barrier for clinicians is a lack of skills to communicate about risk or lifestyle changes clearly and effectively, also related to other theme of confidence and self-efficacy. An integrative review of nurses delivery of lifestyle interventions found that nurses lacked the knowledge, skills, and confidence to deliver NDIs, providing support that these factors are interrelated [76].
Identification of common factors impacting use of non-drug interventions for chronic conditions in primary care has several possible applications. This includes as a starting-point for developing implementation strategies for specific non-drug interventions, identifying top-level implementation strategies for addressing multiple non-drug intervention simultaneously, or to inform important factors for scale-up of existing non-drug interventions. Existing tools, such as the CFIR-ERIC matching tool, can be used to map identified barrier and enabler factors to effective implementation strategies [77, 78]. For example, for key Inner Setting domain factor of availability of, and access to, patient education material about NDIs, implementation activities may include conducting educational meetings, accessing new funding, and developing and distributing education material [77].
This review has several strengths. First, this study goes beyond condition or intervention-specific barriers and enablers to identify common factors across NDIs. Second, we used the updated CFIR framework to analyse factors at Innovation, Outer Setting, Inner Setting and Individual domain levels [31] and applied the TDF to gain a more nuanced view of the Individual domain [20, 59]. Finally, we used rigorous methods: we developed a comprehensive search with a search specialist and librarian, two reviewers screened reviews, we pre-specified a study protocol [21] and reported the results in accordance with the PRIOR checklist [23]. There are several limitations that should be considered when interpreting the study findings. First, the data was extracted by one author (HG). Although a second author validated 10% of extracted data and codes, with good agreement (~ 90%), the review could have been improved by a second author coding all extracted data. Given the use of a coding framework (instead of iteratively developed codes) and that the data in included reviews was generally qualitative (i.e., no quantitative estimate of effect was measured). We determined our approach sufficient for the review type. Second, we did not conduct a forward and backward citation searching as specified in the protocol. Due to the breadth of included reviews and that we identified many common barriers and enablers, after data extraction we determined that inclusion of further reviews would not likely provide any additional barrier or enabler subthemes. Third, RoB assessment was conducted by one author (LA), with 10% validated by a second author (HG). As assessment of RoB is somewhat contentious for qualitative syntheses, due to the inherently subjective nature of the data [79], we determined this approach sufficient for completeness of reporting but recognise the limitation of our decision. This is also reflected in the RoB assessments of primary studies within included reviews. While most of these did conduct some form of RoB assessment, many did not provide an overall rating, though this is a limitation of the literature, not the study (Additional File 7). Fourth, as there is currently no dedicated tool for assessing RoB of qualitative reviews, we used the prominent systematic review appraisal tool, AMSTAR 2, and made adjustments to also assess qualitative reviews. This adjusted tool is not validated, representing a limitation. However, given that quality assessment of qualitative review is contentious [79], no overall ratings have been given, and the quality of reviews had no bearing on inclusion, we believe this adjusted tool is sufficient for the intended purpose (reporting of quality of included reviews). Validation of this tool or development of quality appraisal tool for qualitative reviews may be a future direction of research.
Conclusions
As prevalence of chronic conditions is expected to rise [3], it is crucial to understand factors that help and hinder effective treatment, including non-drug treatments. This overview used implementation frameworks (CFIR and TDF) to synthesise 71 common barriers and 69 common enablers to using effective NDIs. Our findings can be used to inform top-level implementation strategies or scale-up of the adoption of NDIs across various conditions and settings. By understanding common factors affecting the use of NDIs generally, broader, and generalisable implementation interventions can be developed to address multiple NDIs.
Availability of data and materials
All data generated or analysed during this study are included in this published article as a supplementary information file (see Additional File 8).
Abbreviations
- CCA:
-
Corrected Covered Area
- CFIR:
-
Consolidated Framework of Implementation Research
- GROOVE:
-
Graphical representation of the degree of overlap
- HANDI:
-
Handbook of Non-Drug Interventions
- NDI(s):
-
Non-drug intervention(s)
- NHANES:
-
National Health and Nutrition Examination Survey
- PRIOR:
-
Preferred Reporting Items for Overview of Reviews
- RoB:
-
Risk of Bias
- SPIDER:
-
Sample, Phenomenon of Interest, Design, Evaluation, Research type
- TDF:
-
Theoretical Domains Framework
- US:
-
United States
References
Australian Institute for Health and Welfare. Chronic conditions and multimorbidity. Aust Inst Health Welf. 2021; https://www.aihw.gov.au/reports/chronic-disease/chronic-condition-multimorbidity/contents/chronic-conditions-and-multimorbidity. Accessed 17 Aug 2022)
World Health Organization. Non communicable diseases. World Health Organization. 2021. https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases. Accessed 17 Aug 2022.
Ansah JP, Chiu C-T. Projecting the chronic disease burden among the adult population in the United States using a multi-state population model. Front Public Health. 2023;10:1082183. https://doi.org/10.3389/fpubh.2022.1082183.
Reynolds R, Dennis S, Hasan I, Slewa J, Chen W, Tian D, et al. A systematic review of chronic disease management interventions in primary care. BMC Fam Pract. 2018;19:11. https://doi.org/10.1186/s12875-017-0692-3.
Rothman AA, Wagner EH. Chronic illness management: what is the role of primary care? Ann Intern Med. 2003;138:256–61. https://doi.org/10.7326/0003-4819-138-3-200302040-00034.
Royal Australian College of General Practitioners. Guidelines for preventative activities in general practice: prevention of chronic disease. Guidel Prev Act Gen Pract. 2021; https://www.racgp.org.au/clinical-resources/clinical-guidelines/key-racgp-guidelines/view-all-racgp-guidelines/guidelines-for-preventive-activities-in-general-pr/preamble/introduction. Accessed 17 Aug 2022)
American Academy of Orthopaedic Surgeons. Management of Osteoarthritis of the Knee (Non-Arthroplasty) Evidence-Based Clinical Practice Guideline (3rd Edition) 2021. https://www.aaos.org/oak3cpg. Accessed 17 Aug 2022.
National Institute for Health and Care Excellence. Osteoarthritis: care and management 2020. https://www.nice.org.uk/guidance/cg177/chapter/Recommendations. Accessed 17 Aug 2022.
Royal Australian College of General Practitioners. Guideline for the management of knee and hip osteoarthritis. 2nd ed; 2018. https://www.racgp.org.au/clinical-resources/clinical-guidelines/guidelines-by-topic/view-all-guidelines-by-topic/musculoskeletal-health/knee-and-hip-osteoporosis
Tuballa A, Connell D, Smith M, Dowsett C, O’Neill H, Albarqouni L. Introduction of allergenic food to infants and allergic and autoimmune conditions: a systematic review and meta-analysis. BMJ Evid-Based Med. 2023;bmjebm-2023-112445 https://doi.org/10.1136/bmjebm-2023-112445.
Albarqouni L, Moynihan R, Clark J, Scott AM, Duggan A, Del Mar C. Head of bed elevation to relieve gastroesophageal reflux symptoms: a systematic review. BMC Fam Pract. 2021;22:24. https://doi.org/10.1186/s12875-021-01369-0.
Booth AO, Nowson CA. Patient recall of receiving lifestyle advice for overweight and hypertension from their general practitioner. BMC Fam Pract. 2010;11:8. https://doi.org/10.1186/1471-2296-11-8.
Grabovac I, Smith L, Stefanac S, Haider S, Cao C, Waldhoer T, et al. Health care providers’ advice on lifestyle modification in the US population: results from the NHANES 2011-2016. Am J Med. 2019;132:489–497.e1. https://doi.org/10.1016/j.amjmed.2018.11.021.
Henry JA, Jebb SA, Aveyard P, Garriga C, Hippisley-Cox J, Piernas C. Lifestyle advice for hypertension or diabetes: trend analysis from 2002 to 2017 in England. Br J Gen Pract J R Coll Gen Pract. 2022;72:e269–75. https://doi.org/10.3399/BJGP.2021.0493.
Williams AR, Wilson-Genderson M, Thomson MD. A cross-sectional analysis of associations between lifestyle advice and behavior changes in patients with hypertension or diabetes: NHANES 2015-2018. Prev Med. 2021;145:106426. https://doi.org/10.1016/j.ypmed.2021.106426.
Glasziou P. Making non-drug interventions easier to find and use. Aust Fam Physician. 2013;42:35. https://pubmed.ncbi.nlm.nih.gov/23529457/
Sigurdsson EL. Up and running: an underutilized prescription in primary care. Scand J Prim Health Care. 2013;31:1–2. https://doi.org/10.3109/02813432.2013.762171.
Boocock RC, Lake AA, Haste A, Moore HJ. Clinicians’ perceived barriers and enablers to the dietary management of adults with type 2 diabetes in primary care: a systematic review. J Hum Nutr Diet. 2021;34:1042–52. https://doi.org/10.1111/jhn.12875.
Albarqouni L, Greenwood H, Dowsett C, Hoffmann T, Thomas R, Glasziou P. Attitudes, beliefs, behaviours and perspectives on barriers and enablers of Australian general practitioners towards non-drug interventions: a national survey. Fam med. Community Dent Health. 2024:12. https://doi.org/10.1136/fmch-2023-002457.
Birken SA, Powell BJ, Presseau J, Kirk MA, Lorencatto F, Gould NJ, et al. Combined use of the consolidated framework for implementation research (CFIR) and the theoretical domains framework (TDF): a systematic review. Implement Sci. 2017;12:2. https://doi.org/10.1186/s13012-016-0534-z.
Greenwood H, Albarqouni L, Thomas R. Common barriers and enablers to the use of non-drug interventions for managing common chronic conditions in primary care: a study protocol for an overview of reviews. OSF Regist. 2022; https://osf.io/qp928. Accessed 25 Apr 2023
Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions. Chichester: Wiley; 2019.
Gates M, Gates A, Pieper D, Fernandes RM, Tricco AC, Moher D, et al. Reporting guideline for overviews of reviews of healthcare interventions: development of the PRIOR statement. BMJ. 2022;378:e070849. https://doi.org/10.1136/bmj-2022-070849.
Clark J, Glasziou P, Del Mar C, Bannach-Brown A, Stehlik P, Scott AM. A full systematic review was completed in 2 weeks using automation tools: a case study. J Clin Epidemiol. 2020;121:81–90. https://doi.org/10.1016/j.jclinepi.2020.01.008.
Institute for Evidence-Based Healthcare. Systematic Review Accelerator 2023. https://sr-accelerator.com/#/. Accessed 28 Jun 2023.
Cooke A, Smith D, Booth A. Beyond PICO: the SPIDER tool for qualitative evidence synthesis. Qual Health Res. 2012;22:1435–43. https://doi.org/10.1177/1049732312452938.
Australian Government, Department of Health and Aged Care. What we’re doing about primary care 2023. https://www.health.gov.au/topics/primary-care/what-we-do. Accessed 17 Jan 2024
Clark JM, Sanders S, Carter M, Honeyman D, Cleo G, Auld Y, et al. Improving the translation of search strategies using the polyglot search translator: a randomized controlled trial. J Med Libr Assoc JMLA. 2020;108:195–207. https://doi.org/10.5195/jmla.2020.834.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71.
Joanna Briggs Institute J. Critical appraisal tools, JBI n.d. https://jbi.global/critical-appraisal-tools.
Damschroder LJ, Reardon CM, Widerquist MAO, Lowery J. The updated consolidated framework for implementation research based on user feedback. Implement Sci. 2022;17:75. https://doi.org/10.1186/s13012-022-01245-0.
Hennessy EA, Johnson BT. Examining overlap of included studies in meta-reviews: guidance for using the corrected covered area index. Res Synth Methods. 2020;11:134–45. https://doi.org/10.1002/jrsm.1390.
Pérez-Bracchiglione J, Meza N, Bangdiwala SI, Niño de Guzmán E, Urrútia G, Bonfill X, et al. Graphical representation of overlap for OVErviews: GROOVE tool. Res synth. Methods. 2022;13:381–8. https://doi.org/10.1002/jrsm.1557.
Pieper D, Antoine S-L, Mathes T, Neugebauer EAM, Eikermann M. Systematic review finds overlapping reviews were not mentioned in every other overview. J Clin Epidemiol. 2014;67:368–75. https://doi.org/10.1016/j.jclinepi.2013.11.007.
Kanavaki AM, Rushton A, Efstathiou N, Alrushud A, Klocke R, Abhishek A, et al. Barriers and facilitators of physical activity in knee and hip osteoarthritis: a systematic review of qualitative evidence. BMJ Open. 2017;7:e017042. https://doi.org/10.1136/bmjopen-2017-017042.
Hurley M, Dickson K, Hallett R, Grant R, Hauari H, Walsh N, et al. Exercise interventions and patient beliefs for people with hip, knee or hip and knee osteoarthritis: a mixed methods review. Cochrane Database Syst Rev. 2018; https://doi.org/10.1002/14651858.CD010842.pub2.
Christensen ME, Brincks J, Schnieber A, Soerensen D. The intention to exercise and the execution of exercise among persons with multiple sclerosis--a qualitative metasynthesis. Disabil Rehabil. 2016;38:1023–33. https://doi.org/10.3109/09638288.2015.1091859.
Learmonth YC, Motl RW. Physical activity and exercise training in multiple sclerosis: a review and content analysis of qualitative research identifying perceived determinants and consequences. Disabil Rehabil. 2016;38:1227–42. https://doi.org/10.3109/09638288.2015.1077397.
Newitt R, Barnett F, Crowe M. Understanding factors that influence participation in physical activity among people with a neuromusculoskeletal condition: a review of qualitative studies. Disabil Rehabil. 2016;38:1–10. https://doi.org/10.3109/09638288.2014.996676.
Miles C, Arden-Close E, Thomas M, Bruton A, Yardley L, Hankins M, et al. Barriers and facilitators of effective self-management in asthma: systematic review and thematic synthesis of patient and healthcare professional views. NPJ Prim Care Respir Med. 2017;27:57. https://doi.org/10.1038/s41533-017-0056-4.
Wandell PE, de Waard A-KM, Holzmann MJ, Gornitzki C, Lionis C, de Wit N, et al. Barriers and facilitators among health professionals in primary care to prevention of cardiometabolic diseases: a systematic review. Fam Pract. 2018;35:383–98. https://doi.org/10.1093/fampra/cmx137.
Vadas D, Prest K, Turk A, Tierney S. Understanding the facilitators and barriers of stroke survivors’ adherence to recovery-oriented self-practice: a thematic synthesis. Disabil Rehabil. 2021:1–12. https://doi.org/10.1080/09638288.2021.1968512.
Scope A, Leaviss J, Booth A, Sutton A, Parry G, Buszewicz M, et al. The acceptability of primary care or community-based behavioural interventions for persistent physical symptoms: qualitative systematic review. Br J Health Psychol. 2021;26:1069–94. https://doi.org/10.1111/bjhp.12521.
Hall AM, Scurrey SR, Pike AE, Albury C, Richmond HL, Matthews J, et al. Physician-reported barriers to using evidence-based recommendations for low back pain in clinical practice: a systematic review and synthesis of qualitative studies using the theoretical domains framework. Implement Sci. 2019;14:49. https://doi.org/10.1186/s13012-019-0884-4.
Finazzi E, MacBeth A. Service users experience of psychological interventions in primary care settings: a qualitative meta-synthesis. Clin Psychol Psychother. 2022;29:400–23. https://doi.org/10.1002/cpp.2650.
Skoglund G, Nilsson BB, Olsen CF, Bergland A, Hilde G. Facilitators and barriers for lifestyle change in people with prediabetes: a meta-synthesis of qualitative studies. BMC Public Health. 2022;22:553. https://doi.org/10.1186/s12889-022-12885-8.
Hilberdink B, van der Giesen F, Vliet Vlieland T, Nijkamp M, van Weely S. How to optimize exercise behavior in axial spondyloarthritis? Results of an intervention mapping study. Patient Educ Couns. 2020;103:952–9. https://doi.org/10.1016/j.pec.2019.12.017.
Dash K, Goyder EC, Quirk H. A qualitative synthesis of the perceived factors that affect participation in physical activity among children and adolescents with type 1 diabetes. Diabet Med. 2020;37:934–44. https://doi.org/10.1111/dme.14299.
Tierney S, Mamas M, Skelton D, Woods S, Rutter MK, Gibson M, et al. What can we learn from patients with heart failure about exercise adherence? A systematic review of qualitative papers. Health Psychol. 2011;30:401–10. https://doi.org/10.1037/a0022848.
Davenport K, Hardy G, Tai S, Mansell W. Individual experiences of psychological-based interventions for bipolar disorder: a systematic review and thematic synthesis. Psychol Psychother Theory Res Pract. 2019;92:499–522. https://doi.org/10.1111/papt.12197.
Trappes-Lomax T. Self-care for people coping with long-term health conditions in the community. J Integr Care. 2016;24:76–106. https://doi.org/10.1108/JICA-05-2015-0019.
Messina J, Campbell S, Morris R, Eyles E, Sanders C. A narrative systematic review of factors affecting diabetes prevention in primary care settings. PLoS One. 2017;12:e0177699. https://doi.org/10.1371/journal.pone.0177699.
Spencer A, Jablonski R, Loeb SJ. Hypertensive African American women and the DASH diet. Nurse Pract. 2012;37:41–6. https://doi.org/10.1097/01.NPR.0000410278.75362.a2.
Othman N, Wong YY, Lean QY, Mohd Noor N, Neoh CF. Factors affecting self-management among adolescents and youths with type 2 diabetes mellitus: a meta-synthesis. Eur J Integr Med. 2020;40 https://doi.org/10.1016/j.eujim.2020.101228.
Spenceley SM, Williams BA. Self-care from the perspective of people living with diabetes. Can J Nurs Res. 2006;38:124–45. https://pubmed.ncbi.nlm.nih.gov/17037117/
Albert FA, Crowe MJ, Malau-Aduli AEO, Malau-Aduli BS. Functionality of physical activity referral schemes (PARS): a systematic review. Front Public Health. 2020;8:257. https://doi.org/10.3389/fpubh.2020.00257.
Havas K, Bonner A, Douglas C. Self-management support for people with chronic kidney disease: patient perspectives. J Ren Care. 2016;42:7–14. https://doi.org/10.1111/jorc.12140.
Nguyen TNM, Whitehead L, Saunders R, Dermody G. Systematic review of perception of barriers and facilitators to chronic disease self-management among older adults: implications for evidence-based practice. Worldviews Evid-Based Nurs. 2022;19:191–200. https://doi.org/10.1111/wvn.12563.
Atkins L, Francis J, Islam R, O’Connor D, Patey A, Ivers N, et al. A guide to using the theoretical domains framework of behaviour change to investigate implementation problems. Implement Sci. 2017;12:77. https://doi.org/10.1186/s13012-017-0605-9.
Norman K, Chepulis L, Burrows L, Lawrenson R. Barriers to obesity health care from GP and client perspectives in New Zealand general practice: a meta-ethnography review. Obes Rev. 2022:e13495. https://doi.org/10.1111/obr.13495.
Barnes K, Scewczyk Z, Kelly JT, Campbell K, Ball L. Is nutrition care in primary care settings cost effective? A systematic review of trial-based economic evaluations. Aust J Prim Health. 2021;27:v–vi. https://doi.org/10.1071/PYv27n4abs.
Dhungana RR, Pedisic Z, de Courten M. Implementation of non-pharmacological interventions for the treatment of hypertension in primary care: a narrative review of effectiveness, cost-effectiveness, barriers, and facilitators. BMC Prim Care. 2022;23:298. https://doi.org/10.1186/s12875-022-01884-8.
Royal Australian College of General Practitioners. Internet-based cognitive behaviour therapy for depression and anxiety. Aust Fam Physician. 2013; https://www.racgp.org.au/afp/2013/november/cbt
Orchard J. Prescribing and dosing exercise in primary caret. Aus J Gen Pract. 2020; https://www1.racgp.org.au/ajgp/2020/april/prescribing-and-dosing-exercise-in-primary-care. Accessed 3 Jun 2022
Hoffmann TC, Maher CG, Briffa T, Sherrington C, Bennell K, Alison J, et al. Prescribing exercise interventions for patients with chronic conditions. CMAJ. 2016;188:510–8. https://doi.org/10.1503/cmaj.150684.
Spink A, Wagner I, Orrock P. Common reported barriers and facilitators for self-management in adults with chronic musculoskeletal pain: a systematic review of qualitative studies. Musculoskelet Sci Pract. 2021;56:102433. https://doi.org/10.1016/j.msksp.2021.102433.
Royal Australian College of General Practitioners. Handbook of Non-Drug Interventions (HANDI) 2022. https://www.racgp.org.au/clinical-resources/clinical-guidelines/handi. Accessed 6 Dec 2022.
Albarqouni L, Greenwood H, Dowsett C, et al. Attitudes, beliefs, behaviours and perspectives on barriers and enablers of Australian general practitioners towards non-drug interventions: a national survey Family Medicine and Community Health 2024;12:e002457. https://doi.org/10.1136/fmch-2023-002457.
Wolker Manta S, Fabrício Sandreschi P, Christofoletti Dos Santos M, Maria Konrad L, Miranda Tassitano R, Benedetti RB, et al. Barriers and facilitators on the implementation of physical activity in primary health care: a systematic review. Prev Med Rep. 2022;28:101875. https://doi.org/10.1016/j.pmedr.2022.101875.
Langenbahn D, Matsuzawa Y, Lee YSC, Fraser F, Penzien DB, Simon NM, et al. Underuse of behavioral treatments for headache: a narrative review examining societal and cultural factors. J Gen Intern Med. 2021;36:3103–12. https://doi.org/10.1007/s11606-020-06539-x.
Kelley JM, Kraft-Todd G, Schapira L, Kossowsky J, Riess H. The influence of the patient-clinician relationship on healthcare outcomes: a systematic review and meta-analysis of randomized controlled trials. PLoS One. 2014;9:e94207. https://doi.org/10.1371/journal.pone.0094207.
Pereira Gray DJ, Sidaway-Lee K, White E, Thorne A, Evans PH. Continuity of care with doctors-a matter of life and death? A systematic review of continuity of care and mortality. BMJ Open. 2018;8:e021161. https://doi.org/10.1136/bmjopen-2017-021161.
James S, Halcomb E, Desborough J, McInnes S. Lifestyle risk communication by general practice nurses: an integrative literature review. Collegian. 2019;26:183–93. https://doi.org/10.1016/j.colegn.2018.03.006.
Alexandre K, Campbell J, Bugnon M, Henry C, Schaub C, Serex M, et al. Factors influencing diabetes self-management in adults: an umbrella review of systematic reviews. JBI Evid Synth. 2021;19:1003–118. https://doi.org/10.11124/JBIES-20-00020.
Rethorn ZD, Covington JK, Cook CE, Bezner JR. Physical therapists’ knowledge, skills, beliefs, and organizations impact physical activity promotion: a systematic review and Meta-analysis. Phys Ther. 2022;102. https://doi.org/10.1093/ptj/pzab291.
Morris M, Halcomb E, Mansourian Y, Bernoth M. Understanding how general practice nurses support adult lifestyle risk reduction: an integrative review. J Adv Nurs. 2022;78:3517–30. https://doi.org/10.1111/jan.15344.
Powell BJ, Waltz TJ, Chinman MJ, Damschroder LJ, Smith JL, Matthieu MM, et al. A refined compilation of implementation strategies: results from the expert recommendations for implementing change (ERIC) project. Implement Sci. 2015;10:21. https://doi.org/10.1186/s13012-015-0209-1.
Waltz TJ, Powell BJ, Fernández ME, Abadie B, Damschroder LJ. Choosing implementation strategies to address contextual barriers: diversity in recommendations and future directions. Implement Sci. 2019;14:42. https://doi.org/10.1186/s13012-019-0892-4.
Mays N, Pope C. Assessing quality in qualitative research. BMJ. 2000;320:50–2. https://doi.org/10.1136/bmj.320.7226.50.
Acknowledgements
We would like to acknowledge and thank Sarah Bateup for peer-reviewing the search string and Justin Clark for providing additional input on the search strategy.
Funding
HG is supported by an Australian Government Research Training Program Scholarship. LA is supported by Australian National Health and Medical Research Council (NHMRC) Investigator Grant (2008379). The funders had no role in the conceptualization, design, data collection, analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the conception and design of the work. HG conducted the majority of data acquisition and analysis, with 10% validated by AD. LA conducted risk of bias assessment, with 10% validated by HG. HG led interpretation of data, with guidance from LA and RT. HG drafted the manuscript. All authors read the final manuscript, provided critical revision and give approval of this manuscript for publication. HG accepts responsibility for the accuracy and integrity of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable – synthesis of review studies.
Consent for publication
Not applicable.
Competing interests
LA is an editorial board member at BMC Primary Care. HG, AD and RT have no competing interests to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Greenwood, H., Davidson, A.R., Thomas, R. et al. Common barriers and enablers to the use of non-drug interventions for managing common chronic conditions in primary care: an overview of reviews. BMC Prim. Care 25, 108 (2024). https://doi.org/10.1186/s12875-024-02321-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12875-024-02321-8