
Abstract
Background
The aim of this study was to ascertain the effect of the extent and severity of bronchiectasis as determined with high-resolution computed tomography (HRCT) on lung function in patients with pure bronchiectasis, bronchiectasis and asthma, and bronchiectasis and chronic obstructive pulmonary disease (COPD).
Methods
One hundred nineteen patients (71 with pure bronchiectasis, 25 asthmatic patients with bronchiectasis, and 23 COPD patients with bronchiectasis) underwent HRCT and pulmonary function tests. Computed tomography features were scored by the consensus of 2 radiologists.
Results
There were no statistically significant differences among the 3 patient groups regarding the extent of bronchiectasis, bronchial dilatation degree, bronchial wall thickening, decreased attenuation in the lung parenchyma, or presence of mucus in the large and small airways. In the pure bronchiectasis group, a negative correlation was found between forced vital capacity (FVC) % of predicted, forced expiratory volume in 1 sec (FEV1) % of predicted, the FEV1/FVC ratio and the extent of bronchiectasis, bronchial wall thickening, bronchial wall dilatation, and decreased attenuation. At multivariate analysis the main morphologic changes associated with impairment of FVC and FEV1 were the extent of bronchiectasis and a decreased attenuation in the lung parenchyma. The decrease in the FEV1/FVC ratio was associated with bronchial wall dilatation. No correlation was found between morphologic changes and indices of pulmonary function in the asthma and COPD patients.
Conclusions
Morphologic changes associated with bronchiectasis do not influence lung function in patients with asthma and COPD directly, although they do play a role in impairing pulmonary function in patients with bronchiectasis alone.
Riassunto
Premessa
Scopo di questo studio era verificare l'effetto della estensione e della gravità delle bronchiectasie, determinate mediante tomografia computerizzata ad alta risoluzione (HRCT), sulla funzionalità respiratoria nei pazienti con bronchiectasie semplici, bronchiectasie e asma, e con broncopneumopatia cronica ostruttiva (BPCO) e bronchiectasie.
Metodi
119 pazienti (71 pazienti con bronchiectasie semplici, 25 pazienti asmatici con bronchiectasie, e 23 pazienti con BPCO e bronchiectasie) sono stati sottoposti ad HRCT e prove di funzionalità respiratoria. I punteggi delle HRCT sono stati attribuiti sulla base di un consenso tra 2 radiologi.
Risultati
Non ci sono state differenze statisticamente significative tra i 3 gruppi di pazienti riguardo all’estensione delle bronchiectasie, al grado di dilatazione bronchiale, all’ispessimento della parete bronchiale, alla riduzione di attenuazione del parenchima polmonare, o alla presenza di muco nelle grandi e piccole vie aeree. Nel gruppo con bronchiectasie semplici, una correlazione negativa è stata trovata fra FVC (% del teorico), FEV1 (% del teorico), rapporto FEV1/FVC ed estensione delle bronchiectasie, ispessimento della parete bronchiale, dilatazione della parete bronchiale e riduzione di attenuazione. L'analisi multivariata ha mostrato che i cambiamenti morfologici principali associati al deterioramento di FVC e FEV1 sono l’estensione delle bronchiectasie e la riduzione di attenuazione nel parenchima polmonare. La diminuzione del rapporto FEV1/FVC è associata a dilatazione della parete bronchiale. Nessuna correlazione è stata riscontrata tra le variazioni morfologiche e gli indici respiratori nei pazienti con asma e BPCO.
Conclusioni
Le modificazioni morfologiche associate a bronchiectasie non influenzano direttamente la funzionalità respiratoria nei pazienti con asma e BPCO, ma hanno un ruolo nel deterioramento della funzionalità respiratoria nei pazienti con bronchiectasie semplici.
Similar content being viewed by others

Introduction
Bronchiectasis is defined as a permanent abnormal dilatation of an airway [1]. Characteristically, most patients with bronchiectasis have an obstructive pulmonary function defect; however, those with limited disease can maintain their pulmonary function, while those with diffuse and severe disease can have restrictive or mixed impairment. The mechanism of airway obstruction is not known with certainty. Previous studies have found that it might be associated with the collapse of large airways at expiration [2], the retention of endobronchial secretion [3], bronchial wall thickening [4], obliterative bronchitis [5, 6], or accompanying asthma [7].
Bronchiectasis can be diagnosed accurately with high-resolution computed tomography (HRCT), and morphologic changes caused by bronchiectasis can be evaluated quantitatively. Previous studies have shown that the degree of the morphologic changes caused by bronchiectasis is associated with impaired pulmonary function [4, 8–11].
Bronchiectasis, chronic obstructive pulmonary disease (COPD) and asthma are the diseases that cause obstructive pulmonary functional impairment. In patients with COPD it is seen radiologically in 2 to 29% of patients with asthma [12–14], and in 29 to 50% of patients with COPD [15, 16]. Bronchiectasis has been found to be associated with the clinical severity of the disease in asthma patients [13, 14]. In patients with COPD it has been shown to be associated with increased inflammatory airway markers, bacterial colonization, and severe exacerbations [16]. However, the relationship between the morphologic changes associated with bronchiectasis and the impairment in pulmonary function in patients with asthma and COPD has not yet been clearly elucidated.
In this retrospective study, we investigated the effect of the extent and severity of bronchiectasis on lung function of patients with asthma, COPD, and bronchiectasis alone.
Materials and methods
The study included 119 consecutive clinically stable patients (54 males, 65 females) with bronchiectasis confirmed by HRCT at our institution between January 2004 and December 2007. Patients who did not have PFTs within two months of the HRCT were excluded. Patients younger than 18 years of age and those with a history of lung resection, as well as those with bronchial carcinoma, interstitial lung disease, active tuberculosis, or lobar consolidation on HRCT were also excluded. No patients had allergic bronchopulmonary aspergillosis or cystic fibrosis.
Patients were classified into 3 groups: those who had only bronchiectasis (bronchiectasis group); those with asthma and bronchiectasis (asthma group); and those with COPD and bronchiectasis (COPD group). The diagnosis of asthma was made in accordance with the Global Strategy for Asthma Management and Prevention (GINA) criteria [17] and the diagnosis of COPD was made based on the American Thoracic Society criteria [18]. The HRCT results and pulmonary function parameters of the 3 groups were compared.
Lung function tests
Pulmonary function tests were performed using a spirometer (Vmax 22, SensorMedics Corp., Yorba Linda, CA, USA) in compliance with European Respiratory Society standards. Forced vital capacity (FVC) % of predicted, forced expiratory volume in 1 sec (FEV1) % of predicted, and the FEV1/FVC ratio were measured and indicated as percentage values in accordance with the age, sex and height of the patients [19]. Airway obstruction was defined as an FEV1/FVC value < 70%.
High resolution computed tomography
Computed tomography images of the lungs were obtained using a multidetector computed tomography scanner (Sensation 4, Siemens, Erlangen, Germany). Scanning parameters included a collimation of 1.3 mm, section interval of 10 mm, 120 kVp, and 200 mAs. All images were obtained with the patient in supine position at full inspiration and without injection of a contrast medium. Scanned images were reconstructed into a bone algorithm through a 512 × 512 matrix with a small field of view to image only pulmonary areas. Images were obtained at a window width of 800 to 1500 H and a window level of -500 to -700 H.
Radiologic evaluation
Computed tomography images were evaluated simultaneously by 2 radiologists (FT and UO) who were blinded to patients' data. The final decision was made by consensus.
The extent of bronchiectasis, severity of bronchial dilatation, bronchial wall thickness (BWT), the presence of mucus plugging in large and small airways, and decrease in parenchymal attenuation (DA) were scored for each lung lobe (the lingula was considered as a different lobe, making a total of 6 lobes) separately, according to the modified Bhalla system [20]. The scoring system was as follows: 1) extent of bronchiectasis (0 = none, 1 = one or partial broncho pulmonary segment involved, 2 = two or more bronchopulmonary segments involved, 3 = generalized cystic bronchiectasis); 2) severity of bronchial dilatation (0 = normal, 1 = less than twice the diameter of the adjacent pulmonary artery, 2 = more than twice the diameter of adjacent pulmonary artery); 3) severity of bronchial wall thickening (0 = normal, 1 = 0.5 × the diameter of the adjacent pulmonary artery, 2 = 0.5 - 1.0 × the diameter of the adjacent pulmonary artery, 3 = ≥ 1.0 × the diameter of the adjacent pulmonary artery); 4) presence of mucous plugging in large airways (0 = none, 1 = present); 5) presence of mucous plugging in small airways (0 = none, 1 = present); and 6) extent of decreased attenuation (0 = normal, 1 = ≤ 50% of lobar volume, 2 = > 50% of lobar volume).
Statistical analyses
Data analyses were carried out using SPSS software (Statistical Product and Services Solutions, version 11.5, SPSS Inc, Chicago, IL, USA). Depending on the distribution, patient features, PFT parameters and HRCT results, scores were expressed as means plus standard deviation (SD) or medians with ranges. Comparisons of pulmonary function test results among the groups and the differences in HRCT scores were performed using independent sample t test or the Mann-Whitney U test. Univariate analyses of the associations between PFT results and HRCT scores were determined using the Spearman rank correlation. Stepwise forward regression analysis was performed to identify which HRCT score in the bronchiectasis group had an independent determinant effect on pulmonary function. Values for p < 0.05 were accepted as statistically significant.
Results
Patient characteristics
The characteristics of the patients in each of the 3 groups are summarized in Table 1. While the mean age of patients in the bronchiectasis and asthma groups was not significantly different, it was higher in the COPD group than in the other 2 groups (p < 0.05).
Computed tomography scores and lung function test results
As shown in Table 2, there were no statistically significant differences in HRCT scores among the 3 groups. When PFT was evaluated, FVC% in the bronchiectasis group was found to be higher than in the asthma group. The predicted FEV1/FVC ratio was higher in the bronchiectasis group than in the other 2 groups.
Correlation between lung function test results and HRCT scores
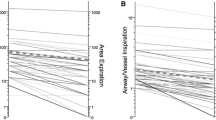
In Table 3, the relationships between the PFT results and HRCT scores are summarized for each of the 3 groups. For the patients in the bronchiectasis group, a strong negative correlation was found between the extent of bronchiectasis, the severity of bronchial wall dilatation, BWT, the extent of DA, and all functional parameter values (FVC%, FEV1% and FEV1/FVC). There were no statistically significant correlations between the HRCT scores and PFT parameters in the asthma and COPD groups.
Multiple regression analyses
According to stepwise regression analysis (Table 4), the extent of bronchiectasis and the DA score were found to be positively related to impairment in FVC% (both p < 0.05) and FEV1% (p < 0.001 and p < 0.05, respectively). In addition, the bronchial dilatation score was consistently associated with the FEV1/FVC ratio (p < 0.001).
Discussion
To the best of our knowledge, this is the first study to concomitantly determine a correlation between the structural changes associated with bronchi ectasis and lung function impairment in patients with pure bronchiectasis, as well as in patients with asthma and COPD who have bronchiectasis. There was no statistical difference between groups with regard to structural change (the extent of bronchiectasis, bronchial dilatation, BWT, DA in lung parenchyma, and the presence of mucus plugging in large and small airways) on HRCT. Notwithstanding, while the HRCT scores of bronchiectasis were found to be correlated with pulmonary functional impairment only in patients with pure bronchiectasis, morphologic changes associated with bronchiectasis were observed to be not influential on pulmonary function in asthma and COPD patients.
We found a strong inverse correlation between the extent of bronchiectasis, the degree of bronchial dilatation, BWT, DA in lung parenchyma, and PFT parameters (FVC%, FEV1% and FEV1/FVC) in patients with pure bronchiectasis. Conversely, the presence of mucus plugging in airways (large and small) was found to have less effect on PFT results; for instance, mucus plugging in small airways correlated only with the decrease in the FEV1/FVC ratio. Shah et al. suggested that the presence of mucus plugging in large and small airways in patients with cystic fibrosis did not affect pulmonary function [21]. In our study, multivariate analyses revealed that the presence of mucus plugging in airways of patients with bronchiectasis was not the primary cause of lung function impairment. However, as stated by Sheehan et al., when the mucus load of airways varies over time this could be a reason for some fluctuation in pulmonary function [9].
Multivariate analysis showed that the extent of bronchiectasis and DA in the lung parenchyma were the main determinants of the reduction of both FVC% and FEV1%. These findings suggest that the morphologic changes in patients with pure bronchiectasis could lead both to restrictive and obstructive functional impairment.
The increase in the extent of bronchiectasis reflects the extension of inflammation and destruction in airways, and thus a proportional impairment of pulmonary function could be expected. The restrictive component of impairment in lung function can be explained by atelectasis, pleural disease, parenchymal scarring, and peribronchial fibrosis that accompany bronchiectasis.
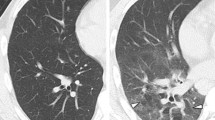
The decrease of attenuation in the pulmonary parenchyma that surrounds the bronchiectatic bronchi implies an association of bronchiectasis and obliterative bronchitis, and it can be seen as a mosaic pattern radiologically. Reports have shown that obliterative bronchitis that is accompanied by bronchiectasis is one of the primary causes of the obstructive type of pulmonary function impairment [4, 8, 9]. It has been known since the 1960s that when the small airways are obliterated due to chronic infections and inflammation in bronchiectatic large airways, the result is a continued collateral air flow through Khon pores instead of a collapse in distal obstruction, with air trapping emerging as a check-valve effect which is thought to cause the decreased attenuation in the pulmonary parenchyma [5]. Moreover, obliterative bronchitis is considered by some authors to be a part of bronchiectasis, and it is an early finding in the pathogenesis of the disease. Hansell et al. contend that monitoring the attenuation decrease in the pulmonary lobes, which have no sign of bronchiectasis in patients with bronchiectasis, supports this view [7]. On the assumption that the DA in the parenchyma indirectly shows inflammation in the lungs and the extent of destruction, as in our study, the development of a mixed-type of pulmonary functional defect can be expected when obliterative bronchitis becomes widespread.
According to the multivariate analysis, in our pure bronchiectatic patients the degree of bronchial dilatation (p < 0.001) was the main independent variable associated with a decrease of the FEV1/FVC ratio. In the literature, contradictory results have been obtained regarding the impact of the degree of bronchial dilatation on pulmonary function in patients with bronchiectasis. Lee et al. [11] reported that the degree of bronchial dilatation correlated with airway obstruction, whereas Roberts et al. suggested that the increase in the degree of bronchial dilatation correlated with the amount of airway obstruction at lower levels [4]. Bronchial dilatation is one of the main signs of bronchiectasis morphologically. It has been previously shown that small airway disease correlates with bronchial dilatation in patients with bronchiectasis [22]. In parallel with the increase of bronchial dilatation in the patients with bronchiectasis, the increase in airway obstruction can be associated with morphologic changes in small airways, which cannot be demonstrated radiologically with HRCT.
In the case of the coexistence of asthma and bronchiectasis, it has been shown that bronchiectasis can contribute to severe and difficult-to-control asthma with pulmonary complications [13, 14]. Lynch et al. noted that bronchial dilatation in asthmatic patients did not influence pulmonary function; however, airway obstruction was seen to be more severe in patients when emphysema was detected [23]. Paganini et al. stated that the prevalence of irreversible structural changes such as bronchiectasis, bronchial wall thickening, and emphysema increased in patients with asthma, and that these changes could be seen more frequently in severely asthmatic patients [24]. Our study suggests that the aggravating effect of bronchiectasis on asthma is independent of the effect on pulmonary function. Impairment in the clearance of the bronchial tree and the increase in epithelial permeability after inflammation caused by bronchiectasis may result in bacterial colonization and be the cause of more severe and complicated asthma.
Similarly, there was no significant correlation between the morphologic changes caused by bronchiectasis and pulmonary function in the COPD group. The presence of bronchiectasis in patients with COPD caused bacterial colonization in the lower respiratory tract, increased bronchial inflammation and, as a result, there were more severe exacerbations [16]. While impairment in pulmonary function was found to be correlated with radiological extension of emphysema, the extent of associated bronchiectasis and the degree of bronchial dilatation did not affect airway obstruction [25]. Radiologically, it is difficult to differentiate the hyperaeration of the lung caused by emphysema from the decrease in attenuation in pulmonary parenchyma associated with bronchiectasis accompanied by obliterative bronchitis. Therefore, a correlation between the decreased attenuation in pulmonary parenchyma and pulmonary functions may not be found in patients with COPD.
It is known that the morphologic changes detected at HRCT in COPD, asthma and bronchiectasis arise secondary to the airway remodelling process. These morphologic changes have been defined mostly in patients with only either asthma or COPD; for example, the increase in BWT is characteristic of asthma [26]. In our study, no difference was detected in the morphologic changes of all 3 groups. The presence of bronchiectasis in our patients with asthma or COPD might have formed a mixed-type inflammatory response resulting in the remodelling process, leading to similar morphologic changes. Further histopathologic studies are required to explain the pathogenesis of inflammatory and remodelling-related morphologic changes in patients with more than one type of airway disease. On the other hand, in our study, BWT was determined by a semi-quantitative technique based on the diameter of the pulmonary artery accompanying the bronchus. Probably, if BWT were evaluated quantitatively, the difference between groups could be interpreted more clearly. Taking into consideration that hyperplasia of the pulmonary vasculature can develop in patients with bronchiectasis, the relative thickening of BWT occurring in each of the 3 diseases could be expected.
The functional changes that emerge as a consequence of the interaction between COPD and asthma with bronchiectasis may be related to causes other than the morphologic changes arising from bronchiectasis. In recent years, as a result of factor analysis studies on asthma, COPD and bronchiectasis patients, inflammatory, microbiologic, and functional parameters, as well as morphologic changes, have been observed to affect the course and severity of these diseases independently [27, 28]. Therefore, it has been emphasized that considering the different parameters together is required while evaluating the course of these diseases. In a study by Garcia et al., the extension of the disease, airway obstruction, dyspnea, and pulmonary hyperinflation in patients with bronchiectasis were observed to be independent entities affecting the clinical course of bronchiectasis [28]. In the same study, the degree of dyspnea was correlated more with pulmonary hyperinflation than with airway obstruction. Therefore, the lack of a correlation between functional parameters and morphologic changes associated with bronchiectasis, particularly in asthmatic and COPD patients, can be considered not to be a contradictory result. The radiologic findings and airway obstruction should be considered as independent factors affecting the severity of both diseases.
Our study has several limitations due to its retrospective nature. Firstly, the number of patients in the asthma and COPD groups was relatively low. However, we tried to select well defined patients with asthma and COPD according to international guidelines to allocate patients to three different groups without overlapping. Increasing the number of patients in the asthma and COPD groups would have enhanced the power of our results. Secondly, the HRCT evaluation was carried out by the consensus of two radiologists rather than by independent observers. However, we believe that our radiologic findings were not affected significantly because the radiologists were blinded to the lung function test results of the patients. Thirdly, the lack of expiratory CT scans may have led to low sensitivity in detecting DA of the lung parenchyma. Finally, total lung capacity (TLC) values were lacking in our patients. Currently, the gold-standard diagnosis of restrictive pulmonary impairment requires the measurement of the TLC through helium dilution or plethysmograph techniques. However, a low FVC together with a normal or high FEV1/FVC ratio has traditionally been accepted as a restrictive abnormality and a low FVC with a low FEV1/FVC ratio as a mixed-type abnormality [29].
In conclusion, our findings show that although the morphologic changes associated with bronchiectasis might be a determinant in impairing the pulmonary function of patients with bronchiectasis alone, the pulmonary function of patients with asthma and COPD were not affected directly. Even though bronchiectasis does not affect pulmonary function in these patients, it might be considered as an independent factor which plays a role in the clinical course of asthma and COPD patients.
Conflict of interest statement
None of the authors has any conflict of interest to declare in relation to the subject matter of this manuscript.
References
Tsang KW, Tipoe GL: Bronchiectasis: not an orphan disease in the East. Int J Tuberc Lung Dis. 2004, 8: 691-702.
Fraser RG, Macklem PT, Brown WG: Airway dynamics in bronchiectasis; a combined cinefluorographic-manometric study. Am J Roentgenol Radium Ther Nucl Med. 1965, 93: 821-835.
Cochrane GM, Webber BA, Clarke SW: Effects of sputum on pulmonary function. Br Med J. 1977, 2: 1181-1183. 10.1136/bmj.2.6096.1181.
Roberts HR, Wells AU, Milne DG, Rubens MB, Kolbe J, Cole PJ, Hansell DM: Airflow obstruction in bronchiectasis: correlation between computed tomography features and pulmonary function tests. Thorax. 2000, 55: 198-204. 10.1136/thorax.55.3.198.
Culiner MM: Obliterative bronchitis and bronchiolitis with bronchiectasis. Dis Chest. 1963, 44: 351-360. 10.1378/chest.44.4.351.
Hansell DM, Wells AU, Rubens MB, Cole PJ: Bronchiectasis: functional significance of areas of decreased attenuation at expiratory CT. Radiology. 1994, 193: 369-374.
Ip MS, So SY, Lam WK, Yam L, Liong E: High prevalence of asthma in patients with bronchiectasis in Hong Kong. Eur Respir J. 1992, 5: 418-423.
Ooi GC, Khong PL, Chan-Yeung M, Ho JC, Chan PK, Lee JC, Lam WK, Tsang KW: High-resolution CT quantification of bronchiectasis: clinical and functional correlation. Radiology. 2002, 225: 663-672. 10.1148/radiol.2253011575.
Sheehan RE, Wells AU, Copley SJ, Desai SR, Howling SJ, Cole PJ, Wilson R, Hansell DM: A comparison of serial computed tomography and functional change in bronchiectasis. Eur Respir J. 2002, 20: 581-587. 10.1183/09031936.02.00284602.
Lynch DA, Newell J, Hale V, Dyer D, Corkery K, Fox NL, Gerend P, Fick R: Correlation of CT findings with clinical evaluations in 261 patients with symptomatic bronchiectasis. AJR Am J Roentgenol. 1999, 173: 53-58.
Lee JH, Kim YK, Kwag HJ, Chang JH: Relationships between high-resolution computed tomography, lung function and bacteriology in stable bronchiectasis. J Korean Med Sci. 2004, 19: 62-68. 10.3346/jkms.2004.19.1.62.
Säynäjäkangas O, Keistinen T, Tuuponen T, Kivelä SL: Links between hospital diagnoses of bronchiectasis and asthma. Allergy. 1997, 52: 1120-1122. 10.1111/j.1398-9995.1997.tb00186.x.
Harmanci E, Kebapci M, Metintas M, Ozkan R: High-resolution computed tomography findings are correlated with disease severity in asthma. Respiration. 2002, 69: 420-426. 10.1159/000064018.
Oguzulgen IK, Kervan F, Ozis T, Turktas H: The impact of bronchiectasis in clinical presentation of asthma. South Med J. 2007, 100: 468-471. 10.1097/SMJ.0b013e31802fa16f.
O'Brien C, Guest PJ, Hill SL, Stockley RA: Physiological and radiological characterisation of patients diagnosed with chronic obstructive pulmonary disease in primary care. Thorax. 2000, 55: 635-642. 10.1136/thorax.55.8.635.
Patel IS, Vlahos I, Wilkinson TM, Lloyd-Owen SJ, Donaldson GC, Wilks M, Reznek RH, Wedzicha JA: Bronchiectasis, exacerbation indices, and inflammation in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2004, 170: 400-407. 10.1164/rccm.200305-648OC.
Global Strategy for Asthma Management and Prevention: Revised 2006: Global Initiative for Asthma (GINA) NHLB. [http://www.ginasthma.org]
Celli BR, MacNee W: ATS/ERS Task Force. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004, 23: 932-946. 10.1183/09031936.04.00014304.
Standardized lung function testing: Official statement of the European Respiratory Society. Eur Respir J Suppl. 1993, 16: 1-100.
Bhalla M, Turcios N, Aponte V, Jenkins M, Leitman BS, McCauley DI, Naidich DP: Cystic fibrosis: scoring system with thin-section CT. Radiology. 1991, 179: 783-788.
Shah RM, Sexauer W, Ostrum BJ, Fiel SB, Friedman AC: High-resolution CT in the acute exacerbation of cystic fibrosis: evaluation of acute findings, reversibility of those findings and clinical correlation. AJR Am J Roentgenol. 1997, 169: 375-380.
Becroft DM: Histopathology of fatal adenovirus infection of the respiratory tract in young children. J Clin Pathol. 1967, 20: 561-569. 10.1136/jcp.20.4.561.
Lynch DA, Newell JD, Tschomper BA, Cink TM, Newman LS, Bethel R: Uncomplicated asthma in adults: comparison of CT appearance of the lungs in asthmatic and healthy subjects. Radiology. 1993, 188: 829-833.
Paganin F, Trussard V, Seneterre E, Chanez P, Giron J, Godard P, Sénac JP, Michel FB, Bousquet J: Chest radiography and high resolution computed tomography of the lungs in asthma. Am Rev Respir Dis. 1992, 146: 1084-1087.
Aziz ZA, Wells AU, Desai SR, Ellis SM, Walker AE, MacDonald S, Hansell DM: Functional impairment in emphysema: contribution of airway abnormalities and distribution of parenchymal disease. AJR Am J Roentgenol. 2005, 185: 1509-1515. 10.2214/AJR.04.1578.
Jeffery PK: Remodeling and inflammation of bronchi in asthma and chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2004, 1: 176-183. 10.1513/pats.200402-009MS.
Rosi E, Ronchi MC, Grazzini M, Duranti R, Scano G: Sputum analysis, bronchial hyperresponsiveness, and airway function in asthma: results of a factor analysis. J Allergy Clin Immunol. 1999, 103: 232-237. 10.1016/S0091-6749(99)70496-3.
Martínez-García MA, Perpiñá-Tordera M, Soler-Cataluña JJ, Román-Sánchez P, Lloris-Bayo A, González-Molina A: Dissociation of lung function, dyspnea ratings and pulmonary extension in bronchiectasis. Respir Med. 2007, 101: 2248-2253. 10.1016/j.rmed.2007.06.028.
Crapo RO: Pulmonary-function testing. N Engl J Med. 1994, 331: 25-30. 10.1056/NEJM199407073310107.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Habesoglu, M.A., Tercan, F., Ozkan, U. et al. Effect of radiological extent and severity of bronchiectasis on pulmonary function. Multidiscip Respir Med 6, 284 (2011). https://doi.org/10.1186/2049-6958-6-5-284
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/2049-6958-6-5-284