
Abstract
Objective
To investigate bronchiectasis variations in different computed tomography (CT) respiratory phases, and their correlation with pulmonary function test (PFT) data, in adults.
Methods
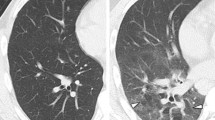
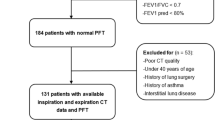
Retrospective data analysis from 63 patients with bronchiectasis according to CT criteria selected from the institution database and for whom PFT data were also available. Bronchiectasis diameter was measured on inspiratory and expiratory phases. Its area and matched airway–vessel ratios in both phases were also calculated. Finally, PFT results were compared with radiological measurements.
Results
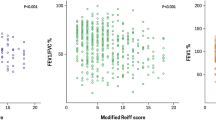
Bronchiectatic airways were larger on inspiration than on expiration (mean cross-sectional area, 69.44 vs. 40.84 mm2; p < 0.05) as were airway–vessel ratios (2.1 vs. 1.4; p < 0.05). Cystic bronchiectasis cases showed the least variation in cross-sectional area (48%). Mean predicted values of forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC) were 81.5 and 77.2%, respectively, in the group in which bronchiectasis could not be identified on expiratory images, and 58.3 and 56.0%, respectively, in the other group (p < 0.05). Variation in bronchiectasis area was associated with poorer lung function (r = 0.32).
Conclusion
Bronchiectasis detection, diameter, and area varied significantly according to CT respiratory phase, with non-reducible bronchiectasis showing greater lung function impairment.



Similar content being viewed by others
Abbreviations
- CT:
-
Computed tomography
- PFT:
-
Pulmonary function test
- FEV1:
-
Forced expiratory volume in 1 s
- FVC:
-
Forced vital capacity
References
Barker AF (2002) Bronchiectasis. N Engl J Med 346:1383–1393
King P, Holdsworth S, Freezer N, Holmes P (2006) Bronchiectasis. Intern Med J 36(11):729–37
Milliron B, Henry TS, Veeraraghavan S, Little BP (2015) Bronchiectasis: mechanisms and imaging clues of associated common and uncommon diseases. Radiographics 35(4):1011–30
Cole PJ (1986) Inflammation: a two-edged sword—the model of bronchiectasis. Eur J Respir Dis Suppl 147:6–15
Pasteur MC, Bilton D, Hill AT, British Thoracic Society Bronchiectasis non-CF Guideline Group (2010) British Thoracic Society guideline for non-CF bronchiectasis. Thorax 65(Suppl. 1):i1–i58
Diederich S, Roos N, Thomas M, Peters PE (1996) Diagnostic imaging in bronchiectasis: value of CT and HRCT. Radiologe 36:550–559 (in German)
Hansell DM (1998) Bronchiectasis. Radiol Clin North Am 36:107–128
Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J (2008) Fleischner Society: glossary of terms for thoracic imaging. Radiology 246(3):697–722. doi:10.1148/radiol.2462070712
Lynch DA, Newell JD, Tschomper BA et al (1993) Uncomplicated asthma in adults: comparison of CT appearance of the lungs in asthmatic and healthy subjects. Radiology 188:829–833
Dodd JD, Souza CA, Muller NL (2006) Conventional high-resolution CT versus helical high-resolution MDCT in the detection of bronchiectasis. AJR Am J Roentgenol 187:414–420
Grenier P, Maurice F, Musset D et al (1986) Bronchiectasis: assessment by thin-section CT. Radiology 161:95–99
Loeve M, Lequin MH, deBruijne et al (2009) Cystic fibrosis: are volumetric ultra-low-dose expiratory CT scans sufficient for monitoring related lung disease? Radiology 253:223–229
Tiddens HA, de Jong PA (2006) Update on the application of chest computed tomography scanning to cystic fibrosis. Curr Opin Pulm Med 12:433–439
Martinez TM, Llapur CJ, Williams TH et al (2005) High-resolution computed tomography imag- ing of airway disease in infants with cystic fibrosis. Am J Respir Crit Care Med 172:1133–1138
Bonnel AS, Song SM, Kesavarju K et al (2004) Quantitative air-trapping analysis in children with mild cystic fibrosis lung disease. Pediatr Pulmonol 38:396–405
Mott LS, Graniel KG, Park J et al (2013) Assessment of early bronchiectasis in young children with cystic fibrosis is dependent on lung volume. Chest 144:1193–1198
Johns DP, Walters JA, Walters EH (2014) Diagnosis and early detection of COPD using spirometry. J Thorac Dis 6(11):1557–1569
Miller MR, Crapo R, Hankinson J et al (2005) Standardisation of spirometry. ATS/ERS task force: standardisation of lung function testing. Eur Respir J 26:319–338
da Silva LCC, Rubin AS, da Silva LMC, Fernandes JC (2005) Spirometry in medical practice. Rev AMRIGS 49(3):183–194
Timmins SC, Diba C, Farrow CE et al (2012) The relationship between airflow obstruction, emphysema extent, and small airways function in COPD. Chest 142:312–319
Chung JH, Kanne JP, Gilman MD (2011) CT of diffuse tracheal disease. AJR Am J Roentgenol 196:W240–W246. doi:10.2214/AJR.09.4146
Reid LM (1950) Reduction in bronchial subdivision in bronchiectasis. Thorax 5(3):233–247
Tanaka N, Matsumoto T, Miura G et al (2003) Air trapping at CT: high prevalence in asymptomatic subjects with normal pulmonary function. Radiology 227:776–785
de Jong PA, Long FR, Nakano Y et al (2006 Oct) Computed tomography dose and variability of airway dimension measurements: how low can we go? Pediatr Radiol 36(10):1043–1047
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Ethical Approval
All procedures performed in this study were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was waived according to the institution ethics committee resolution.
Rights and permissions
About this article

Cite this article
do Amaral, R.H., Nin, C.S., de Souza, V.V.S. et al. Computed Tomography Findings of Bronchiectasis in Different Respiratory Phases Correlate with Pulmonary Function Test Data in Adults. Lung 195, 347–351 (2017). https://doi.org/10.1007/s00408-017-9995-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00408-017-9995-3