
Abstract
Background
MSdialog, a web- and mobile-based software application, captures data on self-administration of subcutaneous interferon β-1a, clinical outcomes, and patient-reported outcomes in patients with multiple sclerosis outside the clinic.
Methods
Patient and healthcare professional reactions to MSdialog were surveyed; participants rated benefits of MSdialog detailed in an explanatory video. A 6-week pilot study of patients with multiple sclerosis then assessed MSdialog usability. After participating in a training teleconference, patients completed weekly health reports via MSdialog, plus two usability surveys (weeks 3 and 6) and an exploratory follow-up telephone interview.
Results
Seventy-six patients, 92 neurologists and 40 multiple sclerosis nurses completed the MSdialog benefits survey. Highly motivating benefits for patients included sharing information with healthcare providers and capturing patient-reported outcomes data; healthcare providers were highly motivated by data availability on patient-reported outcomes and adherence. Thirty-nine of 42 enrolled patients completed the pilot study. Overall, 87 % of patients stated that completion of patient-reported outcomes with MSdialog fitted in “fairly well” to “extremely well” with their weekly routine. At week 6, 77 % of patients were “very satisfied” or “extremely satisfied” with their MSdialog experience; 82 % considered it better than previous methods for tracking their health and 95 % would recommend using MSdialog. Most patients were highly motivated to use MSdialog; reasons given included “helps me remember what to mention to my doctor”.
Conclusion
MSdialog was considered easy to use and superior to patients’ previous methods for tracking health. The ability to provide valuable data to healthcare providers offers the potential to improve patient–physician communication and engagement.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
MSdialog was considered to be easy to use and to provide valuable patient-reported outcome and adherence data to healthcare providers, offering the potential to improve the management of patients with MS. |
Highly motivating benefits for the use of MSdialog for both patients and healthcare providers included sharing information and capturing patient-reported outcomes and adherence data, enabling patients to actively engage in the management of their disease between consultations, as well as during consultations and decision making. |
Of 39 patients, 82 % considered MSdialog better than previous methods for tracking their health and 95 % would recommend its use. |
1 Introduction
Multiple sclerosis (MS) is a chronic, demyelinating disease associated with progressive neurodegeneration and neurological disability, affecting an estimated 2.5 million people worldwide [1]. Many patients with MS report a multitude of symptoms, including pain, fatigue, sleep disturbances, depression, and bladder/bowel dysfunction. These patient-reported outcomes (PROs) can have a negative effect on patients’ health-related quality of life (HRQoL) [2]. Objective measures of MS, such as the Expanded Disability Status Scale, which is biased towards the measurement of the patient’s locomotor function, do not always reflect the patient’s experience of the disease, sometimes leading to a lack of holistic care [2]. Furthermore, in the limited time that doctors and patients have together and because of ineffective communication [3], it is not always possible to identify all the issues that are important in the management of MS.
Effective management of MS-related symptoms such as pain, fatigue, and sleep disturbances requires patient-centered care [4] and effective communication between patients and their healthcare professionals (HCPs). Indeed, the relationship between patients and physicians is strongly associated with patient satisfaction and adherence to treatment [5, 6], and physician–patient communication has been shown to be central to improving adherence to long-term therapy and achieving optimal long-term treatment outcomes [7, 8]. However, approximately 50 % of patients with MS have been shown to discontinue treatment after 6 years [9]. Moreover, patients’ and physicians’ perceptions of the underlying reasons for nonadherence may differ; in the MS Choices Survey, 82 % of physicians cited side effects as the main reason for nonadherence, while only 42 % of patients gave the same reason [10]. Despite the importance of patient–physician communication, the Profile Project survey demonstrated that although 79 % of neurologists believe their communication is adequate and competent at the point of MS diagnosis, only 14 % believe they are able to manage all the needs and expectations of their patients [3]. This finding indicates that improving physician–patient communication, an important part of self-care, may enhance the long-term management of patients with MS should adequate resource and time be available.
Disease information materials, decision aids, and educational interventions, such as coaching and question prompts for patients and communication skills training for HCPs, have been shown to increase patient knowledge and empower patients to engage in their disease management [11, 12]. Patient support programs can improve patient adherence to treatment [13] and reduce hospitalization rates [14], and patients find these support programs highly valuable at all stages of their disease [15].
A number of tools have recently been developed to facilitate patient-centered care and PRO assessment, including Tecficare (Biogen Idec, Cambridge, MA, USA), an application (App) developed specifically for patients taking dimethyl fumarate; Betaconnect™ (Bayer HealthCare, Leverkusen, Germany; an electronic autoinjector device with Bluetooth and USB capabilities) and an associated software system, myBETAappTM (Bayer HealthCare, Leverkusen, Germany) for administering and monitoring interferon (IFN) β-1b; and MSdialog (Merck Serono, Darmstadt, Germany).
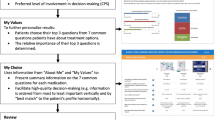
MSdialog is a web- and mobile (i.e., cell phone and tablet)-based software application that combines information from RebiSmart® (Merck Serono; a handheld electronic autoinjector for the subcutaneous [sc] administration of IFN β-1a with wireless data transmission capabilities) with health information recorded by patients via their personal computer or smartphone to collect and store real-time data regarding administration, clinical outcomes, and PROs (Fig. 1) [16]. There are also future plans to broaden the use of MSdialog to work with other devices (e.g., RebiDose® [Merck Serono]). MSdialog offers a practical means by which patients record and exchange information with their MS HCP (MS specialists/neurologists and nurses), with the aim of supporting the patient–physician relationship and offering patients a method of engaging in the management of their MS [16]. Haase et al. have shown that the majority of patients with MS use computers and mobile phones regularly, and approximately 90 % of patients are competent to use electronic health records and patient relationship management systems [17].

MSdialog graphs representing sample results for selected patient-reported outcomes (line chart in upper half of figure) and treatment adherence (bar chart in lower half of figure) in the healthcare professional view. Names and personal details in figure are fictitious and for illustrative purposes only. Displaying the EDSS score in the MSdialog graphs is optional and the EDSS score data are not included in the figure
MSdialog uses existing standardized and validated PRO instruments that have been used in previous research [16]. MSdialog was designed to be flexible regarding the number, type, and frequency of PRO questions in order to align clinical assessments with individual patient needs. PRO instruments were included in MSdialog to help patients with MS engage with their disease. PRO instruments for inclusion were identified through structured workshops with international representation from MS patients, clinical nurses, and neurologists from Sweden, the UK, and Canada [16].
Herein, we report the results of a survey assessing the most important product benefits of MSdialog from both the patients’ and physicians’ perspectives, and a subsequent pilot study exploring the usability of MSdialog in patients with MS.
2 Methods
2.1 Study Designs and Data Collection
2.1.1 MSdialog Benefits Survey
Patients with MS from the UK and Canada, and HCPs (MS specialists/neurologists [hereafter referred to as ‘neurologists’] and nurses) involved in the management and treatment of MS patients, were recruited to take part in an MSdialog survey between June and July 2013 (see electronic supplementary material). Patients were identified from an internally held database by EMD Serono, Inc., Rockland, MA, USA. Patients from the UK and Canada were sent a letter from MySupport (a service developed by Merck Serono to support patients who are prescribed sc IFN β-1a) and EMD Serono, respectively, outlining details of the study, and were asked to register their interest via a webpage. HCPs were recruited from an online panel, which they previously provided consent to join, and were asked to access a webpage to opt into the survey. HCPs who opted in were selected for relevance via initial screening questions. A small financial incentive was offered to participants to take part in and complete the survey. Participants viewed an MSdialog explanatory video and completed a 15-min online questionnaire on their overall reaction to MSdialog. Product benefits were ranked on a scale of 1–7, with 7 being the most positive response and 1 being the least positive.
2.1.2 Patient Usability Pilot Study
Patients with MS from the UK and Canada, who were current or previous RebiSmart users, and who had taken part in the MSdialog survey and provided permission for future follow-up, were invited to participate in the usability pilot study. An incentive was offered to patients to take part in and complete the study (UK, £215; Canada, $380).
The study consisted of the following stages: registration and setting up an MSdialog account; completion of a 5-min online survey entitled “Me and My MS” to gather contextual data around treatment and disease history and to ascertain early levels of interest in MSdialog; a short MSdialog training teleconference; weekly health reports for 6 weeks that were completed via MSdialog, which formed the basis of the usability pilot study; and completion of a 5-min usability survey at weeks 3 and 6. A 30-min exploratory follow-up telephone interview was completed in a subset of randomly selected patients; patients were not selected using patient characteristics or survey answers, and participation was based on the patient providing prior consent to participate and their availability to attend the telephone interview.
For the weekly health reports, patients were randomly assigned (i.e., independent of any patient factors) to complete either one MS quality-of-life (QoL) questionnaire consisting of 31 questions, or five short questionnaires on pain (6 questions), cognitive function (5 questions), fatigue (5 questions), mental health (5 questions), and social support (5 questions).
All patients who participated in the study were required to try to provide feedback on the MSdialog web-based software via the 5-min usability survey at weeks 3 and 6 and, in a subset of patients, a 30-min exploratory follow-up telephone interview. Testing and providing feedback on the mobile App was optional and the choice of the individual patient.
2.1.3 Ethics
Because of the non-experimental design of this study (a survey and telephone interview designed and conducted solely to judge benefits of the MSdialog software application among participants who use or deliver the application), ethics approval was not required, and no ethics committees were approached prior to beginning the study. All interactions with participants took place over the telephone. There was no change to the medical management of patients, and no randomization of participants to different groups. There were no specific questions relating to participants’ health other than the length of time since MS diagnosis and their method, attitudes, or satisfaction with tracking health status; MSdialog itself included approved health-related questions which participants completed as part of testing the usability of MSdialog, but this data was not captured and was not the focus of the study. All data and survey responses were anonymized before analysis, and contact details of patients participating in telephone interviews deleted. All patients provided written informed consent, and could opt out of the survey at any time.
3 Results
3.1 MSdialog Survey
3.1.1 Patient and HCP Demographics
In total, 76 patients (UK 35; Canada 41), 92 neurologists (UK 52; Canada 40), and 40 MS nurses (UK 20; Canada 20) completed the MSdialog benefits survey. Patient and HCP baseline demographics are shown in Tables 1 and 2, respectively.
3.1.2 Overall Reaction to MSdialog
Patients expressed a high interest in using MSdialog, with 94 % of patients rating “how would you describe your level of interest in using the MSdialog software tool” as 5–7 (where 7 is “very interested” and 1 is “not at all interested”). Patient quotes included “I think it is awesome and I would like to try it” and “I try to remember to write down how I’m feeling…but this is in a diary at home and I sometimes forget…if there was a tool available to do this on-the-go it would help”. HCPs also appreciated the ability of patients to record information, with one UK neurologist stating “This is an excellent tool, it engages patients more with their treatment and provides valuable sources of information for the treating neurologist”. HCP quotes also included “…it seems to be a good idea, it could save me time and help focus on patient needs” and “Great! Should decrease amount of time on asking questions. Will streamline appointments and make it easier to set realistic goals that are mutually acceptable to HCPs and patients”.
3.1.3 The Value of MSdialog—User-Reported Benefits
In general, user-reported benefits were highly motivating for patients, scoring 6.0–6.3 out of 7 on all but one benefit tested. The most motivating benefit related to sharing information with their doctor: 71 % of patients ranked this among their top three most motivating benefits. In total, over 80 % of patients agreed that MSdialog could deliver on each of the benefits listed in Fig. 2, with the exception of “MSdialog would keep me motivated to take my drug”. Ninety-six percent of patients agreed with the benefit “MSdialog would be an easy way to provide relevant information to my doctor”, rating this benefit 5–7 on the 7-point scale; and 92 % of patients agreed “MSdialog would be an easy way for me to engage in the management of my disease”, rating this statement 5–7 on the 7-point scale.

Percentage of patients who believe MSdialog would deliver benefits. Patients were asked: “Please indicate the extent to which you agree or disagree with the following statements”. Percentages do not always total 100 % due to rounding
In alignment with the views of the patients surveyed, >80 % of HCPs were highly motivated (i.e., recorded 5–7 on the 7-point scale) by the availability of PRO data, identifying areas to focus on during consultations and helping patients to engage with their disease. Neurologists were also particularly motivated by the availability of adherence data, with 48 % of neurologists most motivated by the statement “MSdialog would provide readily available, user-friendly patient treatment adherence data over time”. Over 80 % of HCPs agreed with the statements “MSdialog would provide readily available, user-friendly patient treatment adherence data over time” and “MSdialog would provide readily available, user-friendly, agreed upon patient-reported outcome data over time”, giving mean ± standard deviation (SD) scores of 5.7 ± 1.3 out of 7 ± 1.2 (with 7 being “completely agree” and 1 being “completely disagree”) for both statements. HCPs were least convinced by the benefit that MSdialog could save time during consultations, giving a mean ± SD score of 5.0 ± 1.5 out of 7.
3.1.4 The Value of MSdialog—Functionality Benefits
Overall, the functionality benefits of MSdialog were appealing to at least 80 % of patients, and a high proportion (≥54 %) found most benefits to be “extremely appealing” (Fig. 3). The most appealing benefit for patients was the ability to share how MS is impacting their life.

Percentage of patients that found each functional MSdialog benefit appealing. Patients were asked: “Please indicate how appealing you find each of the following statements”. Percentages do not always total 100 % due to rounding. PRO patient-reported outcome
Similar to the opinions of the patients, surveyed HCPs also found all functionality benefits appealing. All benefits appealed to ≥73 % of neurologists, ≥78 % of nurses, and ≥74 % of all HCPs, irrespective of role. Viewing adherence and PRO data was the most appealing function. The highest performing benefit for nurses related to MSdialog allowing patients to set reminders on their future appointments, medication and treatments, and the PRO questionnaires.
3.1.5 The Value of MSdialog—PROs
Patients felt that it was highly important to monitor and review PROs over time, with more than 90 % of patients scoring the following between 5 and 7 (with 7 being “extremely important” to monitor and 1 being “not important at all”): fatigue (99 %), fatigue impact (97 %), physical health (96 %), general health (95 %), cognitive deficits (93 %), pain (91 %), and sleep quality (91 %). Symptoms such as bowel control and sexual satisfaction were considered less important, with only 70 and 65 % of patients scoring them between 5 and 7, respectively.
HCP responses generally agreed with those of patients regarding the importance of monitoring PROs, but also placed higher emphasis on mental (92 % [HCP] vs 81 % [patient]), emotional (91 vs 80 %), and social (92 vs 73 %) well-being. When patients and HCPs were asked about other health considerations or PROs that they felt were important to monitor with MSdialog, both stated treatment side effects (e.g., injection-site reactions and flu-like symptoms); gait, balance, and mobility; work/employment capacity; dizziness/numbness; relationships; QoL; and relapses.
3.1.6 The Value of MSdialog—Clinical Benefits
The assessment of clinical benefits was carried out by HCPs only. Neurologists and nurses exhibited a high level of agreement regarding clinical benefits relating to treatment adherence. Ninety-three percent of HCPs agreed (i.e., recorded 5–7 on the 7-point scale) with the claim that engaged patients are more adherent (mean ± SD score: 6.0 ± 0.9 out of 7) and 91 % agreed that better adherence generally leads to better clinical outcomes (mean ± SD score: 5.9 ± 1.0 out of 7).
3.2 MSdialog Usability Pilot Survey
3.2.1 Patient Demographics and MS History
A total of 42 patients who completed the MSdialog survey were enrolled in the MSdialog usability pilot survey, of whom 39 completed the week 6 health report and feedback survey (UK 19 patients; Canada 20 patients) and 12 completed the exploratory follow-up telephone interview (six each from the UK and Canada). Two patients discontinued from the study because of illness and one patient discontinued for unknown reasons. Of the 39 patients who trialed and provided feedback on the MSdialog web-based software, 13 patients also chose to use the mobile App.
The mean ± SD age of patients taking part in the pilot study was 43.9 ± 7.6 years and 72 % of patients were women. Concerning disease and treatment history, the mean ± SD time since diagnosis was 7.0 ± 6.4 years and mean ± SD duration of drug treatment was 4.8 ± 4.5 years. Most patients (82 %) were currently receiving sc IFN β-1a; other current MS therapies were dimethyl fumarate (8 %), other (10 %), and none (10 %). Previous treatments included sc IFN β-1a (15 %) and intramuscular IFN β-1a (13 %).
3.2.2 Current and Previous MS Management
Overall, the mean ± SD frequency of interaction with a neurologist or nurse was 1.5 ± 0.7 and 1.6 ± 1.6 times per year, respectively. Patients reported moderate-to-high satisfaction with MS management (mean ± SD score: 5 ± 1.5 out of 7 on the 7-point scale).
Generally, motivation to track health status was high: 79 % of patients scored their motivation as 5–7, where 7 indicates “extremely motivated” and 1 “extremely unmotivated”. In total, 63 % of patients were dissatisfied with their current tracking tool, rating their current tool from 1–4, where 1 indicates “extremely dissatisfied” and 7 indicates “extremely satisfied”. Sixty-four percent of patients reported previously keeping a record of their health. Pen and paper was the most common previously used method to keep health records (92 %), followed by mobile phone Apps and other online tools (both 8 %), and blogs and other electronic formats (both 4 %). Most patients (64 %) stated that they often or always forget to mention something they intended to raise with their HCP during their consultation. Furthermore, 51 % of patients reported often or always feeling they could have made better use of their consultation time.
3.2.3 Patient Feedback on MSdialog Web and App Platforms
Usability (overall ease of use) of MSdialog increased from week 3 to week 6, with the percentage of patients finding the web-based software “easy” or “very easy” to use, increasing from 77 % at week 3 to 85 % at week 6. For the 13 patients who used the MSdialog App, 85 % found it “easy” or “very easy” to use at both week 3 and week 6. Sixty-four percent of patients found the overall intuitiveness of the web-based software “easy” or “very easy” at week 6, compared with 59 % at week 3; the corresponding values for the App were 85 and 69 %. Importantly, overall ease of PRO completion also improved over time. At week 6, 95 % of patients found PRO completion using the web-based software “easy” or “very easy”, compared with 85 % at week 3, while the same parameter increased from 92 to 100 % for the App.
Eighty-seven percent of patients stated that PRO completion fitted in “fairly well” to “extremely well” with their weekly routine, with 44 % able to complete the questionnaire within 6–10 min. The mean ± SD time spent completing the questionnaires was 11.3 ± 5.2 min per week. At week 3, 69 and 79 % of patients were either “extremely committed” or “committed” to completing health reports on a weekly or monthly basis, respectively. At week 6, this decreased to 64 and 74 %, respectively. Patients considered all six health reports completed in the study useful to monitor, with the longer MS QoL report rated as the most important (mean ± SD score: 6.1 ± 1.0 out of 7, where 7 is “most useful” and 1 is “least useful”), followed by pain (5.9 ± 1.2), cognitive function (5.9 ± 1.3), fatigue (5.8 ± 1.4), mental health (5.7 ± 1.2), and social support (5.2 ± 1.5). An exploratory follow-up of a small patient sample (n = 12) found that the utility of PRO health reports was dependent on the individual: patients placed highest value on the PROs that they experience. However, some patients considered certain PROs to be less relevant to their circumstances and thus challenging to answer questions on, while others considered it useful to highlight less recognized issues.
At week 6, 77 % of patients were “very satisfied” or “extremely satisfied” with their MSdialog experience so far, with 82 % considering it a better method for tracking their MS health compared with previously tried methods, and 95 % of patients stating that they would recommend MSdialog to another person with MS. At the start of the study (week 0), interest in MSdialog was high: 74 % of patients recorded scores of 6 or 7 (with 7 being “extremely interested” and 1 “extremely uninterested”). This high initial interest was sustained and increased slightly over the course of the pilot study, with 85 % of patients returning a score of 6 or 7 at week 6. Similarly, most patients were highly motivated to use MSdialog to track health: 95 % of patients recorded a score of 5–7 and 82 % a score of 6–7, with 7 being “extremely motivated”. The most important reasons for high motivation in over 50 % of patients at week 6 were “helps me remember what to mention to my doctor”, “easy way to engage in disease management”, and “easy way to provide relevant information to doctor”.
4 Discussion
The benefits survey and pilot study described herein were designed to assess patients’ and physicians’ perceptions of the potential value and usability of MSdialog. The MSdialog benefits survey highlighted the value that MSdialog may bring to the management and care of patients with MS. Both patients and physicians felt that MSdialog would improve the sharing of information. Physicians were highly motivated by the availability of PRO data and engaging patients with their disease. The MSdialog usability pilot study found the usability to be high. Patients reported both the MSdialog web-based software and the App to be easy to use, with ease of use increasing over 6 weeks. Patients were highly committed to reporting PROs on a weekly or monthly basis and most patients found MSdialog to be a better method of tracking their health than their current method.
The findings reported here demonstrate that MSdialog provides a user-friendly tool for patients to monitor their own health status, thus engaging with the management of their MS, and to share this information with their HCP. The inclusion of patient-centered care in routine MS assessments through a tool such as MSdialog provides physicians with information that they might not otherwise have access to, which may optimize HRQoL and overall outcomes. Indeed, optimizing use of time with HCPs was recognized as an area of need in the benefit testing survey. Considering that the usability pilot study found that >60 % of patients forget to tell their physician something regarding their health during consultations, there is a clear need for systems that facilitate the sharing of information between patients and their HCPs. It has previously been reported that the patients’ ability to effectively communicate with their HCPs is an essential part of self-care [8], yet our findings suggest that this remains a problem for many patients. In both the pilot study and the MSdialog benefit survey, patients identified the effective sharing of relevant data with their HCPs as a highly motivating/appealing benefit of MSdialog. Thus, a tool such as MSdialog that captures data on PROs between consultations has the potential to improve the flow of information from patients to their HCPs by identifying key areas to focus on during consultations. Providing HCPs with such data will allow them to consider PROs alongside clinical assessments, magnetic resonance imaging scans, and adherence data from injection devices when assessing the effectiveness of treatment, making treatment decisions, and identifying treatment problems and educational needs. In addition, both neurologists and nurses felt that the data obtained from MSdialog would provide a focus point for their consultations and could enhance patient participation in decision making.
The data from this pilot study and MSdialog benefit survey contribute to the understanding of the potential role of MSdialog in optimizing the management of MS; however, certain limitations should be acknowledged. Patients and physicians recruited to take part in both surveys were from the UK and Canada only, and this small pool of participants may not accurately represent patient and physician perspectives globally. Patients were offered a financial incentive to take part in the usability pilot study and the MSdialog benefit survey, and this small incentive may introduce a positive bias in terms of the survey answers and retention rates, which should be interpreted with caution. Furthermore, patients motivated to participate in this type of research include those who appreciate the use of computers, applications, and completing questionnaires, and our data may not represent the wider patient population as a whole; as such, patients with MS who did not participate in the survey may have responded differently. Concerning the usability study specifically, patients did not have access to the full functionality of MSdialog; although they could explore other features, the basis for participation in the study was completion of the health reports. Discontinuation rates were low in the 6-week usability pilot study, although it is not clear whether participation may decrease in studies with a longer duration. Importantly, in the benefit testing survey, HCPs and patients watched a video explaining MSdialog but did not have access to the tool and, therefore, were evaluating MSdialog without hands-on experience or the training they would have received in the clinical setting. Finally, patients were identified and approached from a list of RebiSmart users provided by EMD Serono (a subsidiary of Merck KGaA, Darmstadt, Germany); although there was no preselection of patients, this process may further limit the applicability of our findings to the wider MS population.
5 Conclusion
MSdialog was considered to be easy to use and to provide valuable PRO and adherence data to HCPs, offering the potential to improve the management of patients with MS. In addition, the findings suggest that patients felt MSdialog would help them to actively engage in the management of their disease between consultations, as well as during consultations and decision making, through improved communication with their healthcare team. MSdialog provides a good example of the potential development of healthcare by providing patients and physicians with a tool to enhance disease management.
References
Compston A, Confavreux C, Lassman H. McAlpine’s multiple sclerosis. 4th ed. Philadelphia: Churchill Livingstone; 2006.
Benito-Leon J, Morales JM, Rivera-Navarro J, Mitchell A. A review about the impact of multiple sclerosis on health-related quality of life. Disabil Rehabil. 2003;25(23):1291–303. doi:10.1080/09638280310001608591.
Martinelli V, Ghezzi A, Montanari E, Radaelli M, Comi G, Bossa R. Disclosing the diagnosis of multiple sclerosis: the Profile Project. J Neurol. 2012;259(12):2605–10. doi:10.1007/s00415-012-6548-9.
Miller D, Rudick RA, Hutchinson M. Patient-centered outcomes: translating clinical efficacy into benefits on health-related quality of life. Neurology. 2010;74(Suppl 3):S24–35. doi:10.1212/WNL.0b013e3181dbb884.
Fuertes JN, Boylan LS, Fontanella JA. Behavioral indices in medical care outcome: the working alliance, adherence, and related factors. J Gen Intern Med. 2009;24(1):80–5. doi:10.1007/s11606-008-0841-4.
Fuertes JN, Mislowack A, Bennett J, Paul L, Gilbert TC, Fontan G, et al. The physician-patient working alliance. Patient Educ Couns. 2007;66(1):29–36. doi:10.1016/j.pec.2006.09.013.
Koudriavtseva T, Onesti E, Pestalozza IF, Sperduti I, Jandolo B. The importance of physician-patient relationship for improvement of adherence to long-term therapy: data of survey in a cohort of multiple sclerosis patients with mild and moderate disability. Neurol Sci. 2012;33(3):575–84. doi:10.1007/s10072-011-0776-0.
Lugaresi A, Ziemssen T, Oreja-Guevara C, Thomas D, Verdun E. Improving patient-physician dialog: commentary on the results of the MS Choices survey. Patient Prefer Adherence. 2012;6:143–52. doi:10.2147/PPA.S27932.
Evans C, Tam J, Kingwell E, Oger J, University of British Columbia MSCN, Tremlett H. Long-term persistence with the immunomodulatory drugs for multiple sclerosis: a retrospective database study. Clin Ther. 2012;34(2):341–50. doi:10.1016/j.clinthera.2012.01.006.
Rinon A, Buch M, Holley D, Verdun E. The MS Choices Survey: findings of a study assessing physician and patient perspectives on living with and managing multiple sclerosis. Patient Prefer Adherence. 2011;5:629–43. doi:10.2147/PPA.S26479.
Coulter A, Ellins J. Effectiveness of strategies for informing, educating, and involving patients. BMJ. 2007;335(7609):24–7. doi:10.1136/bmj.39246.581169.80.
Heesen C, Solari A, Giordano A, Kasper J, Kopke S. Decisions on multiple sclerosis immunotherapy: new treatment complexities urge patient engagement. J Neurol Sci. 2011;306(1–2):192–7. doi:10.1016/j.jns.2010.09.012.
Jones JL, Scheidt DJ, Kaushal RS, Carroll CA. Assessing the role of patient support services on adherence rates in patients using glatiramer acetate for relapsing-remitting multiple sclerosis. J Med Econ. 2013;16(2):213–20. doi:10.3111/13696998.2012.744316.
Tan H, Yu J, Tabby D, Devries A, Singer J. Clinical and economic impact of a specialty care management program among patients with multiple sclerosis: a cohort study. Mult Scler. 2010;16(8):956–63. doi:10.1177/1352458510373487.
Kohlmann T, Wang C, Lipinski J, Hadker N, Caffrey E, Epstein M, et al. The impact of a patient support program for multiple sclerosis on patient satisfaction and subjective health status. J Neurosci Nurs. 2013;45(3):E3–14. doi:10.1097/JNN.0b013e31828a4161.
Exell S, Thristan M, Dangond F, Marhardt K, Charles-Krohe MS. A novel electronic application of patient-reported outcomes in multiple sclerosis—meeting the necessary challenges of assessing quality of life and outcomes in daily clinical practice. Eur Neurol Rev. 2014;9(1):49–55.
Haase R, Schultheiss T, Kempcke R, Thomas K, Ziemssen T. Modern communication technology skills of patients with multiple sclerosis. Mult Scler. 2013;19(9):1240–1. doi:10.1177/1352458512471882.
Acknowledgments
Conduct of the survey and pilot study was supported by EMD Serono, Inc., MA, USA. The authors thank Lara Miller of EMD Serono, Inc., Billerica, MA, USA (a subsidiary of Merck KGaA, Darmstadt, Germany), for support in the development of this manuscript. Writing support and editorial assistance was provided by Sarah Barnes and Andrea Plant of Caudex Medical, UK (supported by Merck Serono SA Geneva, Switzerland, a subsidiary of Merck KGaA, Darmstadt, Germany), as well as Shaun Foley of inScience Communications, Chester, UK (supported by Merck KGaA, Darmstadt, Germany).
Peter Greiner, Anna Sawka, and Emma Imison all contributed to data interpretation, and conceiving, writing, and revising the manuscript. Peter Greiner is the guarantor and takes responsibility for the integrity of the work as a whole.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
PG is an employee of Merck KGaA, Darmstadt, Germany, which is the developer of MSdialog.
AS and EI are employees of Simpson Carpenter Ltd and received funding from EMD Serono (a subsidiary of Merck KGaA, Darmstadt, Germany) to perform data collection and analyses.
Additional information
P. Greiner, A. Sawka and E. Imison contributed equally to this work.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Greiner, P., Sawka, A. & Imison, E. Patient and Physician Perspectives on MSdialog, an Electronic PRO Diary in Multiple Sclerosis. Patient 8, 541–550 (2015). https://doi.org/10.1007/s40271-015-0140-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40271-015-0140-1