
Abstract
Introduction
There are limited data on the burden of newly diagnosed patients with heart failure (HF) in Thailand. Thus, this study aimed to fully understand the hospitalization, rehospitalization, mortality rates, demographics and characteristics, and quality of care in these patients.
Method
A retrospective review of all eligible adult patients' medical records from 2018 and 2019 was conducted at five hospitals. The patients were newly diagnosed with HF, as indicated by the International Classification of Diseases (ICD)-10 code “I50.” Descriptive statistics was used to investigate patients' hospital burden and clinical outcome data.
Results
There were 1134 patients newly diagnosed with HF, classified as HF with reduced ejection fraction (HFrEF), HF with preserved ejection fraction (HFpEF), and HF with mildly reduced ejection fraction (HFmrEF) (44.0, 40.0, and 16.0%, respectively). The male-to-female ratios in HFmrEF and HFpEF were similar. In contrast, the proportion of men with HFrEF was greater. The mean age of all patients was 66.0 years. The hospitalization rate was 1.3. Rehospitalization rates for HF-related issues were 0.1, 0.2, 0.4, and 0.5 at 30 days, 60 days, 180 days, and 1 year, respectively. The percentage of deaths from all causes among these patients was 9.8%, while the percentage of deaths from cardiovascular-related causes was 8.5%. Only a small proportion of patients received a target dose of guideline-directed medical therapy (GDMT).
Conclusions
The study revealed that the characteristics, hospitalization rate for HF, and in-hospital mortality rate among newly diagnosed patients with HF were higher compared to similar studies conducted in Thailand and other countries. Moreover, a high quality of care is needed to improve the morbidity and mortality associated with HF in Thailand.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Why carry out the study? | |
The burden of newly diagnosed patients with heart failure (HF) in Thailand is not well understood, and there is concern regarding the appropriateness of care and treatment received by these patients. It has been found that less than half of patients with HF in Thailand receive the HF medications recommended by the national guideline. | |
To address this issue, a study was conducted to assess patient outcomes and evaluate the quality of care among newly diagnosed patients with HF in five hospitals across different regions in Thailand. | |
What was learned from the study? | |
The hospitalization rate for heart failure and the in-hospital mortality rate among newly diagnosed patients with HF were higher in comparison to studies conducted in Thailand and other countries. | |
Improving treatment and care for patients newly diagnosed with heart failure (HF) is crucial to reduce the morbidity and mortality rates associated with this condition in Thailand. |
Introduction
Heart failure (HF) is a significant global public health concern, impacting a considerable number of individuals across the world [1]. However, the occurrence of this condition varies from one region to another. The prevalence of HF in Western nations is normally between 1.0 and 2.0%, but it is between 5.0 and 7.0% in Southeast Asia [2]. The prevalence of HF in Thailand remains unknown. Nevertheless, there is a growing belief that the burden of HF in Thailand is steadily increasing. This upward trend is attributed to several factors, including heart failure being the ultimate consequence of cardiovascular disease (CVD) [3] and the rising number of elderly individuals in Thailand [4].
Heart failure ranks among the leading causes of hospital admissions worldwide. In developed countries, heart failure accounts for 1.0–4.0% of all hospital admissions [5], while in Asian countries, the percentage of hospitalizations due to heart failure ranges from 3.4 to 6.7% [6]. Additionally, the in-hospital mortality rate related to heart failure is notably elevated, with a range of 3.8–9.0% in Western countries and 2.0–6.0% in the Asian population. The initial data from the first heart failure registry in Thailand, known as the Thai Acute Decompensated Heart Failure Registry (Thai ADHERE), revealed an in-hospital mortality rate of 5.5% for patients with heart failure from 2006 to 2007 [7]. Furthermore, findings from a 10-year follow-up of the Thai ADHERE study showed that 28.0 and 58.2% of patients admitted for acute decompensated heart failure passed away within 1 and 5 years after their hospital admission, respectively [8].
Over the past three decades, significant advancements have been made in managing HF through the development of various medication classes like mineralocorticoid receptor antagonist (MRA) and interventions such as implantable cardioverter defibrillators and cardiac resynchronization therapy (CRT). These medical breakthroughs have contributed to a potential reduction in in-hospital mortality rates in Thailand, as evidenced by a decrease from 4.4% in 2008 to 4.1% in 2013 [9]. However, a contrasting trend emerges when examining HF hospitalization rates, which increased from 97 per 10,000 beneficiaries in 2008 to 117 per 10,000 beneficiaries in 2013 [9]. The elevated rate of HF hospitalizations imposes a significant economic burden, evidenced in healthcare expenditures. This burden accounts for a substantial portion of total healthcare spending in North America and Western Europe, typically ranging from 1.0 to 3.0% [10, 11].
Moreover, this rise in hospitalizations suggests a need for improved quality of care for patients with HF, particularly in the outpatient department. Supporting this hypothesis, a retrospective cohort study conducted in a tertiary care hospital in Thailand revealed that less than half of patients with HF received HF medications recommended by the national guideline, such as angiotensin-converting enzyme inhibitors/angiotensin receptor blockers (ACEI/ARB), beta-blockers, and MRA at the time of hospital admission [12]. Conducting a comprehensive study that evaluates the appropriateness of care and treatment received in patients with HF is crucial. It enhances the quality of care and reduces morbidity and mortality among patients with HF; it is crucial to conduct a comprehensive study that evaluates the appropriateness of care and treatment received in patients with HF. Thus, we performed a retrospective cohort study to assess patient outcomes, including hospitalization, rehospitalization, and mortality rates, and evaluate the quality of care by measuring the percentages of receiving appropriate care and treatments among newly diagnosed patients with HF in five hospitals across different regions in Thailand.
Methods
Study Settings and Participants
This retrospective cohort study was conducted between 2018 and 2019 across five hospitals in Thailand (i.e., Lampang, Chonburi, Udonthani, Bhumibol Adulyadej, and Queen Sirikit Heart Center of the Northeast, Khon Kaen University). These hospitals were chosen based on their diverse geographic locations and varying service levels including three advanced-level hospitals in the upcountry in the Ministry of Public Health (Lampang, Chonburi, and Udonthani; hospital size is 800, 850, and 300 beds, respectively), one medical school hospital in the upcountry (Queen Sirikit Heart Center of the Northeast; hospital size is 200 beds), and one military hospital in the center (Bhumibol Adulyadej; hospital size is 694 beds). The study's participants were adult patients with the diagnosis of HF.
The participants in this study consisted of adult patients who had received a new diagnosis of HF between January and December 2018. These individuals were identified using International Classification of Diseases (ICD)-10 codes “I50” (representing all cases of HF) and “I50.1” (indicating left ventricular HF) from the databases of the study's hospitals. Patients had to meet the following criteria: (1) newly diagnosed with HF, (2) aged between 18 and 99 years, and (3) had at least two hospital visits between 2018 and 2019. All participants were followed up until December 2019.
This study was conducted in accordance with the principles of the Declaration of Helsinki. The study’s protocol was approved by the Central Research Ethics Committee (CREC) (COA-CREC029/2022) and the local Institutional Review Board (IRB) of each participating institution (see supplementary material). Due to the study's retrospective nature, informed consent was exempted by the IRB.
Data Collection
The data collected in this study were categorized into three main parts as follows:
-
1.
Demographic data: This section encompassed information about age, gender, and the reimbursement scheme utilized.
-
2.
Co-morbidities: The participants' underlying health conditions included cardiovascular and metabolic diseases consisting of atrial fibrillation, diabetes mellitus, hypertension, hyperlipidemia, chronic obstructive pulmonary disease (COPD)/asthma, chronic kidney disease (CKD), myocardial infarction (MI), coronary artery disease (CAD), stroke, and obesity.
-
3.
Disease characteristics: This section included information about the etiology of heart failure, medication history, the New York Heart Association (NYHA) classification, and the left ventricular ejection fraction (LVEF).
The etiology of HF was classified into two primary types: (1) coronary artery disease and (2) cardiovascular abnormalities stemming from conditions such as hypertensive heart disease, dilated cardiomyopathy, hypertrophic cardiomyopathy, valvular heart disease, tachycardia-induced cardiomyopathy, and myocarditis. Medication history involved the medications administered to the participants for treatment of cardiovascular disease or diabetes mellitus before their enrollment in the study. This included medications such as ACEI or ARB, beta-blockers, MRA, diuretics, calcium channel blockers (CCBs), and antidiabetic drugs. Sodium glucose co-transporter subtype 2 (SGLT2) inhibitors data was not collected since the Heart Failure Council of Thailand (HFCT) 2019 Heart Failure Guidelines, which this research followed, did not include SGLT-2 inhibitors.
Demographic data, co-morbidities, the underlying causes of HF, and details about the NYHA functional class and LVEF (which includes results of 2D echocardiogram, where available) were all extracted from the medical records by the research physicians. At the same time, the medication history was retrieved directly from the hospital's database.
Outcomes of Interest
The main objective of this study was to assess the prognosis and disease journey of newly diagnosed patients with HF. The primary outcomes included their likelihood of hospitalization, rehospitalization, unscheduled hospital visits related to HF, as well as all-cause mortality and cardiovascular (CV) mortality.
Unscheduled hospital visits were defined as unplanned visits to either the outpatient department (OPD) or the emergency department (ED). Hospitalization was identified as an admission to an acute care facility for HF, which could include admissions in hospital wards, intensive care units (ICU), coronary care units (CCU), and cardiac intensive care units (ICCU). Rehospitalization was defined as an inpatient admission to an acute care facility for HF within specific timeframes: 30 days, 60 days, 180 days, and 1 year following discharge from a prior hospitalization. All-cause mortality was defined as any death due to any cause, whereas CV mortality specifically referred to deaths related to cardiovascular events. The outcomes were verified among the participants by accessing data from the hospital databases.
The secondary outcome was the quality of care for newly diagnosed patients with HF. Quality of care was measured by the proportion of newly diagnosed patients with HF successfully enrolled in an HF clinic. Additionally, we evaluated the extent to which these patients received guideline-directed medical therapy (GDMT). Furthermore, we investigated the proportion of patients with HF reduced ejection fraction (HFrEF) who achieved the recommended target dosage for each component of GDMT, as per the 2019 Heart Failure Guideline of the Heart Failure Council of Thailand (HFCT). The GDMT, as outlined in the guideline, comprises medications such as ACEI, ARB, angiotensin receptor neprilysin inhibitor (ARNI), beta-blockers, and MRA.
Statistical Analysis
Continuous data were reported using two different methods based on data distribution. When the data followed a normal distribution, the data were presented as the mean and standard deviation (SD). In cases where the data did not exhibit a normal distribution, the median and range were applied instead. Categorical data were presented in terms of frequency and percentage (%).
Calculating the hospitalization rate for heart failure, the number of hospitalizations was divided by the total count of newly diagnosed patients with HF. The rehospitalization rates were calculated at four different time points: 30 days, 60 days, 180 days, and 1 year. These rates were determined by dividing the number of patients with HF rehospitalized for all causes and CV-related causes at these specific time intervals by the total number of newly diagnosed patients with HF. The rate of unscheduled visits was estimated by dividing the number of ED visits or unplanned hospital visits at the OPD by the total number of newly diagnosed patients with HF.
All-cause mortality and CV mortality rates were estimated by dividing the number of deaths attributed to all causes and CV-related causes by the total number of newly diagnosed patients, respectively. To provide a measure of confidence in our findings, we estimated 95% confidence intervals (CI) for all proportions and rates. All data analyses were carried out using SAS program version 9.4.
Results
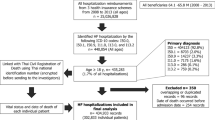
A total of 1134 newly diagnosed patients with HF met the inclusion criteria for this study. However, only 735 patients had available data on LVEF. Most of these patients (44.0%) were categorized as having HFrEF. Additionally, 40.0% were classified as having HF with preserved ejection fraction (HFpEF), while 16.0% were identified as having HF with mildly reduced ejection fraction (HFmrEF).
Characteristics of total participants and each type of HF were presented in Table 1. The male-to-female ratios were comparable for all participants and the patients with HFmrEF and HFpEF. However, there was a higher percentage of males than females among patients with HFrEF. The mean age of all participants was 66.0 years, which was consistent across all three types of HF. Most participants had Universal Coverage Scheme (UCS) health insurance (72.7%), followed by the Civil Service Medical Benefits Scheme (CSMBS) (20.6%) and Social Security Scheme (SSS) (5.1%). In terms of the etiology of HF, cardiovascular abnormalities were the leading cause of HF in all types. Moreover, ischemic heart disease was the most common cause of HF in HFmrEF (38.3%), followed by HFrmF and HFpEF (31.1 and 14.8%, respectively). Valvular heart disease was the etiology of HF in the remaining patients.
In terms of comorbidities, hypertension was the most common, affecting all types of heart failure, accounting for around 68.0% of all patients. Dyslipidemia, diabetes mellitus, atrial fibrillation, chronic kidney disease, and coronary artery disease were also commonly observed in patients with heart failure, with prevalence rates of 36.3, 34.6, 27.1, 22.1, and 15.8%, respectively.
Quality of Care
The quality of care of our participants is presented in Table 2. Most patients with HF were categorized as NYHA class II (62.2%). In comparison, roughly 35.0% of all HF types were categorized as NYHA class III or IV, but only 3.1, 5.0, and 6.6% of HFrEF, HFmrEF, and HFpEF patients were classified as NYHA class I. However, 3.2% of patients with HF were enrolled and treated at a specialized HF clinic. The proportion of patients treated at the HF clinic was highest for HFrEF (5.9%), followed by HFmrEF and HFpEF patients (1.7 and 1.0%, respectively). The median duration from diagnosis to first enrollment in HF care for all patients was 30 days, ranging from 1 to 640 days. Only 64.8% of patients underwent echocardiography and had LVEF data. Among these patients, the mean LVEF was 45.3%.
Regarding GDMT, 42.9, 20.6, 19.0, and 16.2% of patients with HF were given beta-blockers, ACEIs, MRAs, and ARBs, respectively. Only 1.0% received ARNI, mostly among HFrEF patients. Even among patients with HF who achieved the target dose of GDMTs, most fell short of the target doses for all GDMTs. ACEIs (14.1%) and MRAs (13.3%) had the greatest proportion of patients attaining the targeted dose. Furthermore, 5.9 and 1.3% of patients with HF received the recommended dose of beta-blockers and ARBs, respectively. With ARNI, no patients attained the targeted dose.
Burden of Heart Failure
Hospital Visits
A total of 4574 hospital visits were recorded. The median number of visits per patient was 3.0. Notably, the median number of hospital visits per patient was consistent across all types of heart failure, as detailed in Table 3. Most of these hospital visits were attributed to heart failure, with 85.0% having an ICD-10 code of I50 as the principal diagnosis. Further classifying the hospital visits, we discovered that approximately half were OPD visits, followed by IPD visits at 37.7% and ED visits at 5.0%. Regarding IPD visits, 92.5% of patients were admitted to the general hospital ward. In comparison, only 7.4, 5.5, and 4.8% were admitted to the intensive coronary care unit (ICCU), intensive care unit (ICU), and cardiac care unit (CCU), respectively. Hospital stays were constant among units, with median lengths ranging from 4 to 5 days. Most of these hospitalizations were primarily attributed to heart failure-related causes (83.6%). Other causes of hospitalization in patients with HF were usually acute myocardial infarction (4.5%) and infection (3.3%). The outcome of hospitalization was that 11.5% of the patients died during their hospital admission, and 85.7% of cases were classified as CV-related deaths. The mortality rate during hospital admission varied by heart failure type, with HFrEF patients having the highest rate (11.4%), followed by HFpEF (8.2%) and HFmrEF (6.8%). Regarding ED visits, the median length of stay was ten days, ranging from one to 99 days. The mortality rate among patients visiting the ED was 4.4%, with cardiovascular events causing all deaths.
Disease Prognosis
Hospitalization, Rehospitalization, and Unscheduled Visits
During a 2-year follow-up period comprising 1134 patients with HF, 1442 hospitalizations were due to HF-related causes, which equates to a hospitalization rate of 1.3 (95% CI 1.2–1.4); see Table 4. There was no significant difference in hospitalization rates across the different types of HF. The rates of rehospitalization for HF-related issues at 30 days, 60 days, 180 days, and 1 year were 0.1 (95% CI 0.1–0.2), 0.2 (95% CI 0.1–0.3), 0.4 (95% CI 0.3–0.5), and 0.5 (95% CI 0.4–0.6), respectively. Unscheduled visits to the ED and OPD were 332 among 1134 patients, indicating an unscheduled visit rate of 0.3 (95% CI 0.2–0.3). Unscheduled visits were relatively comparable across the three types of heart failure, with rates of 0.3 (95% CI 0.2–0.4) for HFrEF, 0.3 (95% CI 0.2–0.4) for HFmrEF, and 0.3 (95% CI 0.2–0.4) for HFpEF.
All-Cause and CV Mortality
All-cause and CV mortality rates in the study were presented in Table 4. Over the 2 years after the HF diagnosis, 111 patients died from any cause, with 96 from CV events. Consequently, among newly diagnosed patients with HF, the proportion of deaths from all causes was 9.8% (95% CI 8.1–11.5%), while the proportion of CV-related deaths was 8.5% (95% CI 6.9–10.1%). When evaluated by HF type, HFrEF had the highest rates of all-cause and CV mortality (9.5 and 7.7%, respectively), followed by HFpEF (7.6 and 6.9%) and HFmrEF (5.8 and 4.2%).
Cost of Heart Failure Utilization
The median cost of OPD visits for patients with a new diagnosis of HF was US $53.00. The median cost for IPD visits was US $460.30. In addition, the median total cost of ED visits was US $92.20.
Discussion
Our study found that approximately 35.0% of patients newly diagnosed with HF did not have information available regarding their LVEF. This was because these patients were initially diagnosed in primary care settings and did not have LVEF data at the time of referral to the tertiary hospital. In order to avoid potential delays in re-diagnosis and considering time limitations, it was decided that obtaining LVEF data for these patients would not be prioritized. Moreover, 80.0% of patients newly diagnosed with HF had at least one HF-related hospitalization during a 2-year follow-up period. This translated into an annual hospitalization rate of 63.0%, much higher than the rate in the 2013 Thai study (47.5%) [9]. Furthermore, our results showed a substantial difference from the Asian Sudden Cardiac Death in Heart Failure (ASIAN-HF) registry, which included data from 11 Asian regions, including Thailand. They reported an 11.0% hospitalization rate [13]. Our report's higher HF hospitalization rate might be related to differences in the study population and setting. Specifically, our study focused only on patients newly diagnosed with HF, while the previous studies included patients with chronic HF. Additionally, our data collection occurred at tertiary care and provincial hospitals, in contrast to the 2013 Thai study, which relied on claims data from patients admitted through Thailand's three major public health reimbursement systems. Consequently, the patients with HF in our study might exhibit a higher likelihood of experiencing severe symptoms and a less favorable prognosis compared to the prior study.
Furthermore, the quality of care provided to patients with HF may be a significant contributing factor to the high hospitalization rate observed in our study. Our findings show that less than half of our participants obtained the recommended medications for HF treatment, with only 43.0, 20.0, 18.0, and 16% receiving beta-blockers, ACEIs, MRAs, and ARBs, respectively. Additionally, fewer than 20% of patients receiving these recommended HF medications reached the target doses. In contrast, patients in the ASIAN-HF [13] registry had greater prescription rates for these medications, with 75.7, 73.7, and 52.1% obtaining beta-blockers, ACEI/ARB, and MRA, respectively. A study conducted in Singapore [14] and China [15] also reported more favorable percentages, with 70.0-80.0% of patients with HF receiving ACEI/ARB and beta-blockers. The difference in medication usage between our study and others highlights potential variations in the quality of care delivered to patients with HF in different settings. In addition to the risk of hospitalization, the usage of ACEI or ARB has been related to a better prognosis in patients with HF. The Thai ADHERE study indicated that patients receiving ACEI/ARB had a 37.0% lower risk of death compared to those not receiving these medications [8].
In terms of in-hospital mortality, our research found that 11.0% of patients died during their hospital admission. This percentage was much higher than previous research at a medical school hospital in Thailand, which showed an in-hospital mortality rate of 5.8% [12]. Furthermore, our study's in-hospital mortality rate exceeded the Thai ADHERE study [7]. In comparison to studies from other countries, our analysis found a higher in-hospital mortality rate than those done in South Korea [16], China [17], and Italy [18], which reported in-hospital mortality rates of 6.6, 4.1, and 2.9%, respectively. It is worth noting that about 93.0% of our patients were admitted to regular hospital wards, while previous studies reported that 19.0–62.0% of patients were admitted to the intensive care unit.
Consequently, the lower in-hospital mortality rate in the previous research might be attributed to differences in the quality of heart failure treatment and supportive care provided during hospitalization. This hypothesis is supported by the evidence that the in-hospital mortality rate was greatest among HFrEF patients, who had lower LVEF and more severe symptoms than other types of HF. Thus, admitting these patients to the ICU with comprehensive supporting care and HF management may reduce the risk of in-hospital mortality compared to admitting them to the general hospital wards. While our study observed a higher in-hospital mortality than prior studies, our all-cause mortality rate was comparable with other studies' findings. Similarly, the ASIAN-HF registry reported a 1-year all-cause mortality rate of 9.6% among symptomatic patients with HF [19], and the Korean Heart Registry found a 1-year mortality rate of 9.2% among HFrEF patients [16].
In comparison to countries in different regions, our study's mortality rate was lower than that of Africa (34.0%) and India (23.0%) [20]. Additionally, our research emphasized that the risk of mortality was highest after HF hospitalization, with cardiovascular events being the leading cause of death in HF. These results are consistent with studies conducted not just in Thailand [8, 12, 21] and other Asian countries [22, 23] but also in Western nations [18, 24, 25]. As a result, it emphasizes the significance of providing adequate treatment and preventative measures for cardiovascular events in patients with heart failure, particularly after hospitalization, to decrease morbidity and death.
Strengths and Limitations
This is the first study in Thailand to examine the disease characteristics and outcomes in patients newly diagnosed with HF. Additionally, our research collected data from five hospitals across various regions of Thailand. This comprehensive coverage allows for the generalizability of our findings to other newly diagnosed patients with HF in Thailand who receive care at hospitals of a similar standard. In addition, beyond the assessment of disease outcomes, our study evaluated the quality of care provided to newly diagnosed patients with HF. This important information raises awareness of the inadequacies in HF treatment in Thailand and is a valuable resource for healthcare professionals and policymakers. These insights can enhance care quality, ultimately reducing morbidity and mortality among patients with heart failure.
Nonetheless, it is essential to acknowledge certain limitations within our study. Firstly, the hospitals included in our research primarily comprised regional and university hospitals, potentially introducing a referral bias. Consequently, our study participants may have presented more severe disease profiles compared to a broader population of newly diagnosed patients with HF. Secondly, our study employed a retrospective study design, entailing data collection from medical records and hospital databases, which had inherent drawbacks leading to missing information in some instances, such as LVEF, NYHA, and drug prescriptions. Thirdly, our identification of newly diagnosed patients with HF relied solely on the ICD-10 coding system, which might have introduced a misclassification bias, potentially resulting in inaccuracies in the classification of newly diagnosed heart failure cases. Fourthly, some patients in this study were initially diagnosed in primary care settings and did not have LVEF) data available at the time of referral to the tertiary hospital. Due to time constraints and the potential for delays in re-diagnosis, the decision was made not to prioritize obtaining LVEF data for these patients. So, the absence of LVEF data for some patients is a limitation of the study. Fifthly, since the study was undertaken during the COVID-19 pandemic, it is possible that some patients had been admitted to another hospital in a different town or region. Lastly, our study did not include data on in-hospital treatment and management. Given that a significant proportion of deaths occurred after hospitalization, information concerning the quality of care during admission and post-hospital discharge is pivotal for improving the prognosis of patients with HF.
Conclusions
In summary, our study revealed that the hospitalization rate for heart failure and the in-hospital mortality rate among newly diagnosed patients with HF were higher in comparison to studies conducted in Thailand and other countries. Furthermore, a substantial proportion of newly diagnosed patients with HF did not receive the necessary treatments and comprehensive management for their condition. As a result, there is an urgent requirement for improved treatment and care for patients newly diagnosed with HF, both in inpatient and outpatient settings, to lower the morbidity and mortality associated with HF in Thailand.
Data Availability
All data generated or analyzed during this study are included in this published article.
References
Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, et al. Heart disease and stroke statistics-2018 update: a report from the American heart association. Circulation. 2018;137(12):e67-492.
Ponikowski P, Anker SD, AlHabib KF, Cowie MR, Force TL, Hu S, et al. Heart failure: preventing disease and death worldwide: addressing heart failure. ESC Heart Fail. 2014;1(1):4–25.
Global health estimates: leading causes of death [Internet]. Who.int. [cited 2024 Jan 19]. Available from: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-ofdeath
Mosterd A, Hoes AW. Clinical epidemiology of heart failure. Heart. 2007;93(9):1137–46.
Organisation for Economic Co-operation and Development. Health care quality indicators—primary care—congestive heart failure hospital admissions. [cited 2024 Jan 19]. Available from: https://stats.oecd.org/.
Shimokawa H, Miura M, Nochioka K, et al. Heart failure as a general pandemic in Asia. Eur J Heart Fail. 2015;17(9):884–92.
Laothavorn P, Hengrussamee K, Kanjanavanit R, et al. Thai acute decompensated heart failure registry (Thai ADHERE). CVD Prevent Control. 2010;5(3):89–95.
Krittayaphong R, Laothavorn P, Hengrussamee K, et al. Ten-year survival and factors associated with increased mortality in patients admitted for acute decompensated heart failure in Thailand. Singapore Med J. 2020;61(6):320–6.
Janwanishstaporn S, Karaketklang K, Krittayaphong R. National trend in heart failure hospitalization and outcome under public health insurance system in Thailand 2008–2013. BMC Cardiovasc Disord. 2022;22(1):203.
Lloyd-Jones D, Adams RJ, Brown TM, et al. Heart disease and stroke statistics–2010 update: a report from the American Heart Association. Circulation. 2010;121(7):e46–215.
Neumann T, Biermann J, Erbel R, et al. Heart failure: the commonest reason for hospital admission in Germany: medical and economic perspectives. Dtsch Arztebl Int. 2009;106(16):269–75.
Lorlowhakarn K, Arayakarnkul S, Trongtorsak A, et al. Outcomes and predictors of one-year mortality in patients hospitalized with acute heart failure. Int J Cardiol Heart Vasc. 2022;43:101159.
Tromp J, Tay WT, Ouwerkerk W, et al. Multimorbidity in patients with heart failure from 11 Asian regions: a prospective cohort study using the ASIAN-HF registry. PLOS Med. 2018;15(3):e1002541.
Hoong CW, Lim CP, Gao F, et al. Outcomes of heart failure with preserved ejection fraction in a Southeast Asian cohort. J Cardiovasc Med (Hagerstown). 2015;16(9):583–90.
Zhang Y, Gao C, Greene SJ, et al. Clinical performance and quality measures for heart failure management in China: the China-Heart Failure registry study. ESC Heart Fail. 2023;10(1):342–52.
Youn YJ, Yoo B-S, Lee J-W, et al. Treatment performance measures affect clinical outcomes in patients with acute systolic heart failure–Report From the Korean Heart Failure Registry–. Circul J. 2012;76(5):1151–8.
Zhang Y, Zhang J, Butler J, et al. Contemporary epidemiology, management, and outcomes of patients hospitalized for heart failure in China: results from the China Heart Failure (China-HF) Registry. J Card Fail. 2017;23(12):868–75.
Senni M, Gavazzi A, Oliva F, et al. In-hospital and 1-year outcomes of acute patients with heart failure according to presentation (de novo vs. worsening) and ejection fraction. Results from IN-HF Outcome Registry. Int J Cardiol. 2014;173(2):163–9.
MacDonald MR, Tay WT, Teng TK, et al. Regional variation of mortality in heart failure with reduced and preserved ejection fraction across Asia: outcomes in the ASIAN-HF registry. J Am Heart Assoc. 2020;9(1):e012199.
Dokainish H, Teo K, Zhu J, et al. Global mortality variations in patients with heart failure: results from the International Congestive Heart Failure (INTER-CHF) prospective cohort study. The Lancet Global Health. 2017;5(7):e665–72.
Krittayaphong R, Karaketklang K, Yindeengam A, et al. Heart failure mortality compared between elderly and non-elderly Thai patients. J Geriatr Cardiol. 2018;15(12):718–24.
Lee SE, Lee HY, Cho HJ, et al. Clinical characteristics and outcome of acute heart failure in Korea: results from the Korean Acute Heart Failure Registry (KorAHF). Korean Circ J. 2017;47(3):341–53.
Tsuchihashi-Makaya M, Hamaguchi S, Kinugawa S, et al. Characteristics and outcomes of hospitalized patients with heart failure and reduced vs preserved ejection fraction. Report from the Japanese Cardiac Registry of Heart Failure in Cardiology (JCARE-CARD). Circ J. 2009;73(10):1893–900.
Adams KF Jr, Fonarow GC, Emerman CL, et al. Characteristics and outcomes of patients hospitalized for heart failure in the United States: rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J. 2005;149(2):209–16.
Harjola VP, Follath F, Nieminen MS, et al. Characteristics, outcomes, and predictors of mortality at 3 months and 1 year in patients hospitalized for acute heart failure. Eur J Heart Fail. 2010;12(3):239–48.
Acknowledgements
All analyses were performed by a contracted research organization (CRO), the Center of Excellence for Biomedical and Public Health Informatics (BIOPHICS) of Mahidol University, and the authors confirmed the findings. The data were analyzed by Pathumwadee Meechok and funded by Novartis (Thailand) Limited. We thank the participants of the study.
Funding
This study was sponsored by Novartis (Thailand) Limited. Novartis also funded the journal’s publication fee.
Author information
Authors and Affiliations
Contributions
Thanita Boonyapiphat, Thidaporn Tangkittikasem, Artit Torpongpun, Vichai Senthong, and Panyapat Jiampo drafted, reviewed, and provided feedback on subsequent versions. Panyapat Jiampo and Thanita Boonyapiphat took the lead in the final revision of the manuscript before submitting it for publication.
Corresponding author
Ethics declarations
Conflict of Interest
Thanita Boonyapiphat, Thidaporn Tangkittikasem, Artit Torpongpun, Vichai Senthong, Panyapat Jiampo have nothing to disclose.
Ethical Approval
This study was conducted in accordance with the principles of the Declaration of Helsinki. The study’s protocol was approved by the Central Research Ethics Committee (CREC) (COA-CREC029/2022) and the local Institutional Review Board (IRB) of each participating institution (see supplementary material). Due to the study's retrospective nature, informed consent was exempted by the IRB.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Boonyapiphat, T., Tangkittikasem, T., Torpongpun, A. et al. Real-World Clinical Burden of Newly Diagnosed Heart failure in Thai Patients. Cardiol Ther 13, 415–430 (2024). https://doi.org/10.1007/s40119-024-00366-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40119-024-00366-5