
Abstract
For many drugs administered per os, high variability in the concentration–time (C–T) values from first sampling to the phase of distribution may cause difficulty in pharmacokinetic analysis. Therefore, the aim of this study was to propose a method of transformation of C–T data, which would allow significantly reducing the standard deviation (SD) value of observed concentrations, without a statistically significant influence on the value of the mean for each sampling point in group. In the presented study, the lowest value of relative standard deviation of concentrations observed in the elimination phase and the value of precision of the used analytical method, were used to optimize the arithmetic, geometric means, median, and the value of SD obtained after single oral administration of itraconazole in human subjects. Non-compartmental modeling was used to estimate pharmacokinetic parameters. The analysis of SD pharmacokinetic parameters after C–T value optimization indicated more than twice the lower value of SD. After transforming the itraconazole data, lower variability of concentration data gives more selective pharmacokinetics profile in absorption and early distribution phase.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
The arithmetic, geometric and harmonic means, as well as the standard deviation (SD), as the measures of variability, are the ones most frequently used descriptive statistics in the calculation of pharmacokinetic (PK) (Cocchetto et al. 1980; Lam et al. 1985; Roe and Karol 1997; Griffin et al. 1999; Koch 1985; Julious and Debarnot 2000). A common problem in the analysis and interpretation of comparative pharmacokinetic parameters is the high value of SD (Davit et al. 2008; Haidar et al. 2008; Van Peer 2010). In extreme cases, the high value of SD makes it impossible to make the right decision as to the fate of the study. This problem concerns many types of studies, from preclinical studies, pilot pharmacokinetic studies to bioequivalence (BE) (Riley 2001; Chien et al. 2005). One way to solve the problem of comparative analysis of data burdened with high values of SD is to optimize the sample size of the group in the study, which consists of a precise determination of the number of subjects or animals on the basis of intrasubject variability (FDA 2006; Ramirez et al. 2008; EMA 2010). This is usually possible for BE studies. However, even in BE studies, in some cases, to determine the correct number of subjects, a pilot study is needed or even a two-stage study model (EMA 2010). A high value of variability (CV %) of observed concentrations or PK parameters, especially often makes it impossible to properly interpret the outcome of the study in case of research concerning new drugs, for which their value of variability of key PK parameters is unknown. This situation is further complicated by the fact that research in the early stages of drug discovery and pilot studies is usually conducted on a small number of subjects (for example first in man).
The scatter of results described by mean values and SD is the result of many factors. To a large extent it depends on the fate of the drug in the organism, such as absorption, distribution, re-distribution, metabolism and elimination. One of the factors standing “outside” of a living organism is the scatter of results, which comes from the precision of the used analytical method. Currently, the limit value for the CV % of precision for the calibration curve excluding the lower limit of quantitation point (LLOQ) is 15 %, while in the point equal to LLOQ, this value can be ≤20 % (FDA 2001). In relation to incurred sample analysis for classic drugs, as the acceptable range of differences for repeated analysis, the range 20 % is proposed (EMA 2009; Rozet et al. 2011; Yadav and Shrivastav 2011). This means that every bioanalytical result introduces an error to the pharmacokinetic calculations as well as the chosen research model—human, laboratory animal or cells in the in vitro studies (Jansen et al. 2002; Jones 2009).
For many drugs, the problem of analysis of PK after per os administration of the drug is high variability in the C–T values from first sampling to the phase of distribution. The common factor influencing maximum concentration (C max) and last concentration (C last) values is the spread of analysis result, which determines the precision of the analytical method. All three, absorption, distribution and elimination, processes which in point of time corresponding to C max occur simultaneously. In case of a single administration of the drug in the elimination phase, the values of the concentration can be observed, which illustrate almost exclusively elimination processes (excluding the redistribution phenomenon), until the interval between the end of the distribution phase and the value equal to \( t_{\hbox{max} } + t_{1/2kel} \times 3 \) (EMEA 2001; Veng-Pedersen 2001; FDA 2006; HC 2010). It can be assumed that the factors that affect the C max relative standard deviation (C max, CV %), resulting from simultaneously occurring elimination, are to some extend dependent on the value of last concentration relative standard deviation (Clast,CV %) minus the error resulting from the precision of the analytical method (CV %,an).
PK studies are usually conducted in the conditions of good laboratory practice and good clinical practice, or in accordance with the principles of these quality systems. It can be therefore assumed that the sum of errors connected to the subject, experimental animal, used formulation or bioanalytical method is constant, while keeping the experiment conditions, controlled by the quality system. It can also be assumed that in each PK study, a minimum range of SD for C–T is possible to achieve. In relation to a single administration, the closest value in many cases could be the lowest value of CV % for the last points of sampling in the elimination phase. In this phase of the study, the deviations from the mean are usually the lowest in the whole series, as the elimination phase is the dominant one and no other process, which is characterized by high variability (for example absorption) influences the SD of the analyzed concentrations. Taking the above into account, the aim of this study was to propose a method of transformation of C–T, which would allow significantly reducing the SD value of observed concentrations, without the statistically significant influence on the value of the mean and median for each sampling point.
2 Materials and methods
2.1 Pharmacokinetic data
In the presented study, the lowest value of relative standard deviation (RSD %) of concentrations observed in the elimination phase and the value of precision of the used analytical method were used to optimize the arithmetic and geometric mean and the value of SD obtained after single oral administration of itraconazole, which is characterized by high variability of pharmacokinetic parameters. A single dose of 100 mg of itraconazole was administered orally (Sporanox® 100 mg tab., Janssen Pharmaceuticals) for male subjects ≥20 to ≤40 years old, with a body mass index ≥20 to ≤25 kg/m2. Blood samples were collected just prior to administration and at 0.5, 1.0, 1.5, 2.0, 2.5, 3.0, 3.5, 4.0, 4.5, 5.0, 6.0, 8.0, 12.0, 24.0, 36.0, 48.0, and 72.0 h after the administration. The concentration analyses were performed using tandem mass spectrometry, using the method described previously (Grabowski et al. 2009). The study was approved by Independent Ethics Committee of District Council of Physicians, Baśniowa 3, Warsaw (Resolution No. 45/05). Itraconazole is a drug with high intrasubject variability, and the formulation belongs to the group of high variability drug product (HVDP). Therefore, the majority of pharmacokinetic profiles began and ended at different time points (different time of absorption delay and concentration with values <LLOQ in last sampling points). For the transformation of data, the only C–T profiles that were chosen were those which originated from different subjects and those having identical number of indicated concentrations in the same interval. Ten C–T profiles were obtained this way between 1.5 and 48 h after the drug administration (Table 1).
2.2 Assumptions
The source of variability in C max point and for concentrations illustrating C last are different and are the result of different processes, which are subject to the drug molecule in the two time points. Components that generate the C max,CV % value are inter alia: variability resulting from the absorption process (CV %,abs), variability resulting from the distribution process (CV %,dist), variability resulting from the elimination process (CV %el) and CV %an. CV %an which in this case is expressed by the precision of the method designated for the value equal to LLOQ. The main components that generate the C last,CV % value are CV %el and CV %an. Both CV %el and CV %an to a large extent influence the value of C max,CV %, as the drug elimination process is simultaneous to the processes of distribution and absorption. Therefore, it was assumed that
while in the case of a point in the elimination phase:
subtracting Eq. 2 from Eq. 1 the value
is obtained, which allows to observe the C max value, without the factors responsible for the variability of the qualifying process and the analytical method.
Adopting the above assumptions, a scheme of data transformation was proposed, which is illustrated by the following example: the arithmetic mean (M A ) for the sampling point equal to 1.5 h is 7.30 ng ml−1, concentration value (C n ) for one of the subjects in the analyzed series is before the transformation 8.77 ng ml−1 (\( C_{n} > M_{A} \)); the lowest value of variability in the elimination phase is the value obtained for the sampling point in the 48th hour and equals to 21.26 % (C last,CV %); CV %an for the LLOQ value is 7.06 %; C max,CV % in the analyzed group is 30.82 % therefore
which in the case of the analyzed point is 19.76 %,
which in the case of the analyzed point is 28.64 %,
represents the percentage of concentration value before the transformation (C n ) calculated with the value of the variability C max,CV % reduced with CV %an, which in the case of the analyzed point gives the value of 2.51 ng × ml−1.
represents the percentage of value Y 1 calculated with the value Clast,CV % reduced with CV %,an, which in the case of the analyzed point gives the value of 0.496 ng × ml−1.
The value of C n after the transformation of (C nT) is
if
if \( C_{n} > M_{A} \). In the case of the analyzed concentration point \( C_{n} > M_{A} \) therefore\( C_{{n{\text{T}}}} = 8.77 - (2.51 - 0.496) \, \), which after transformation gives the concentration equal to \( C_{{n{\text{T}}}} = 6.75 \) ng × ml−1. The transformation of all of the concentration points was made in an analogous way, excluding the series of concentration, which were the source for Clast,CV %.
In developed form, used formulas take the form:if \( C_{n} < M_{A} \), then C nT takes the value:
if \( C_{n} > M_{A} \), then C nT takes the value:
2.3 Pharmacokinetics and statistical analysis
Non-compartmental modeling was used to estimate pharmacokinetic parameters of itraconazole. Pharmacokinetic calculations were performed with the use of Phoenix™ WinNonlin® 6.3 (Certara L.P.). The area under the C–T curve (AUC) from time 0 to the last concentration time point and for infinity (AUC0-tlast; AUC0-inf) as well as area under first moment of concentration time curve (AUMC) from time 0 to the last concentration time point (AUMC0-tlast), were determined by the trapezoidal method. Mean residence time (MRT0-tlast) from time 0 to the last concentration time point was calculated using the standard formula \( {\text{MRT}}_{{ 0 {\text{ - tlast}}}} {\text{ = AUMC}}_{{ 0 {\text{ - tlast}}}} / {\text{AUC}}_{{ 0 {\text{ - tlast}}}} . \) The elimination rate constant (k el) was determined by linear regression of the last three points on the C–T curve. In relation to calculations of t 1/2kel in the specified population it is recommended to conduct the analysis with the harmonic mean and the proper value of pseudo SD (Lam et al. 1985). This is due to the fact that in the case of C–T data, the data distribution is inclined according to the log-normal model. Thus, the geometric mean (MG) and the corresponding coefficient of variation are the factors of descriptive statistics for t 1/2kel, which are considered to be more appropriate than the arithmetic mean (M A ) (Keene 1995; Senn 2002; Gad 2009). In relation to t 1/2kel, the harmonic mean and the value of pseudo SD were calculated. In relation to the other parameters M A and M G were calculated. As tool for measurement of central tendency, median (M) and his standard deviation (SD M ) were used. A statistical analysis of M A , M G , M and their SD (SD A ; SD G ; SD M ) was performed using Microsoft Office Excel® software. The percent of relative standard deviation (CV %) was calculated using formula \( {\text {CV\,\%}}\;=\;{\text{SD}}/{\text{M}}\times{100} \) Raw and transformed data correlations were confirmed by sign test and all pharmacokinetics correlations were confirmed by student-t test. Differences with P < 0.05 were regarded as statistically significant.
3 Results
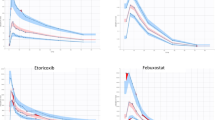
The lowest values of CV % for raw data (RD) were noted for the sampling point 48 h after the administration of the drug, and the value was 20.61 % (Table 1). It was used to transform data in the rest of the time points (1.5–35 h). The concentration values after the transformation (TD) are presented in the Table 1. Image of differences between RD and TD for the largest fluctuation of C–T curve is presented in Fig. 1. On the basis of RD and TD, CV % was calculated for M A , SD A , M G , SD G , M and SD M , which is presented in the Table 2. In relation to the value of M A , M G and M between the RD and TD data, there were no statistically significant differences (P > 0.05). No statistically significant differences (P > 0.05) were found between the mean values of individual points of concentration and the RD and TD data. The SD A value and SD G were significantly lower (P < 0.05) in relation to the RD group.

Concentration–time data of itraconazole administered orally at a single dose of 100 mg for 10 male subjects before (solid line) and after transformation (dashed line). a Represents arithmetic mean and standard deviation, b shows geometric mean and standard deviation and c shows median and standard deviation
The results of the key calculations of pharmacokinetic parameters are shown in Table 3. The analysis of SD G pharmacokinetic parameters in RD and TD groups indicated more than twice lower value of SD G in TD group. The CV % (\( {\text{SD}}_{A} /M_{A} \times 100 \)) of pharmacokinetic parameters, such as k el, t 1/2kel, t max, C max, AUC0-tlast, AUC0-inf, AUMC0-last and MRTinf calculated on the basis of TD was lower by 21.25, 15.44, 17.43, 9.47, 9.85, 1.59, 10.39 and 2.69 %, respectively, than CV % obtained for the PK parameters in RD group but not statistically significant (P > 0.05). The CV % (\( {\text{SD}}_{G} /M_{G} \times 100 \)) of pharmacokinetic parameters k el, t 1/2kel, t max, C max, AUC0-tlast, AUC0-inf, AUMC0-last, and MRTinf calculated on the basis of TD was significantly lower (P < 0.05) by 39.40, 30.75, 44.13, 59.42, 53.77, 51.82 and 38.83 %, respectively, from CV % obtained for the PK parameters in RD group. The ratio of M G in the RD group to MG in the TD group ranged between 0.935 and 1.041 and was not statistically significant (P > 0.05).
4 Discussion
This manuscript presents the method of data transformation calculated on the basis of PK parameters expressed as M A , M G and M. Until now, only a few methods of transforming the values of PK parameters were proposed (Abdallah 1998; Fujita et al. 2006). Frequently, these methods were based on data transformation through the normalization of pharmacokinetic parameters, value of the dose or physiological parameters (body weight, dose, body surface, normalization etc.), (Sathirakul et al. 2003; Sathyan et al. 2007; Staatz and Tett 2007). Normalization and scaling of pharmacokinetic data are also used in the allometric analysis, in scaling either concentrations, time or pharmacokinetic parameters (Mahmood 2005). The purpose of these methods is to facilitate comparative analysis in pharmacokinetics. These methods, however, do not use the variation values obtained in the study to transform data. In the C–T data sequences standard deviation in individual time points within the population is different and ranges from low to high. This is true for both, the analysis of the variability within and between subjects. In the analyzed case, the phase of itraconazole absorption is a subject of large fluctuations. After a single administration of the drug, the low values of deviation for individual C–T points usually fall at the last sampling points. In these points, usually equal to or a bit higher than the LLOQ value, the variability of the SD value often does not exceed 10 %. This occurs because these are the concentrations which usually represent only the process of elimination that is not affected by the factors responsible for the variability of the kinetics of absorption and distribution of the drug. In relation to a single administration, the exceptions are the cases of redistribution of the drug in the late elimination phase (Davis et al. 2000; Coldham et al. 2002; Chrenova et al. 2010). Also, in the analyzed case the volatility calculated for each sampling point was the lowest at a point closest to the LLOQ value of the analytical method. It happens differently in the case of concentrations analyzed in relation to oral administration, while the drug is still present in the stomach or the process of absorption has begun in the intestines. Depending on many factors, the variability in this phase can be very high (Duquesnoy et al. 1998; Tubic et al. 2006). After transforming the itraconazole data, lower variability of concentration data gives more selective pharmacokinetics profile in absorption and early distribution phase.
In summary, the proposed method allows to achieve a reliable picture of the pharmacokinetic profile, free of substantial interference in the average values of obtained concentrations and in the values of pharmacokinetic parameters with a simultaneous decrease in the value of SD. This makes it easier to evaluate the C–T data at points, in which the SD is particularly high. Reducing the value of SD for studies such as first in man, pilot or the rare ones, due to the difficulty of collecting sufficient number of subjects, can help to make a decision about the further direction of the research.
References
Abdallah HY (1998) An area correction method to reduce intrasubject variability in bioequivalence studies. J Pharm Pharm Sci 1:60–65
Chien JY, Friedrich S, Heathman MA, de Alwis DP, Sinha V (2005) Pharmacokinetics/pharmacodynamics and the stages of drug development: role of modeling and simulation. AAPS J 7:E544–E559
Chrenova J, Durisova M, Mircioiu C, Dedik L (2010) Effect of gastric emptying and entero-hepatic circulation on bioequivalence assessment of ranitidine. Methods Find Exp Clin Pharmacol 32:413–419
Cocchetto DM, Wargin WA, Crow JW (1980) Pitfalls and valid approaches to pharmacokinetic analysis of mean concentration data following intravenous administration. J Pharmacokinet Biopharm 6:539–552
Coldham NG, Zhang AQ, Key P, Sauer MJ (2002) Absolute bioavailability of [14C] genistein in the rat; plasma pharmacokinetics of parent compound, genistein glucuronide and total radioactivity. Eur J Drug Metab Pharmacokinet 27:249–258
Davis TM, Daly F, Walsh JP, Ilett KF, Beilby JP, Dusci LJ, Barrett PH (2000) Pharmacokinetics and pharmacodynamics of gliclazide in Caucasians and Australian Aborigines with type 2 diabetes. Br J Clin Pharmacol 49:223–230
Davit BM, Conner DP, Fabian-Fritsch B, Haidar SH, Jiang X, Patel DT, Seo PR, Suh K, Thompson CL, Yu LX (2008) Highly variable drugs: observations from bioequivalence data submitted to the FDA for new generic drug applications. AAPS J 10:148–156
Duquesnoy C, Lacey LF, Keene ON, Bye A (1998) Evaluation of different partial AUCs as indirect measures of rate of drug absorption in comparative pharmacokinetic studies. Eur J Pharm Sci 6:259–264
EMA (2009) Guideline on validation of bioanalytical methods. 1–17
EMA (2010) Guideline on the investigation of bioequivalence. 1–27
EMEA (2001) Guidelines for the conduct of bioequivalence studies for veterinary medicinal products. 1–11
FDA (2001) Guidance for industry bioanalytical method validation. 1–25
FDA (2006) Bioequivalence guidance. 1–28
Fujita T, Matsumoto Y, Ozaki M, Majima M, Kumagai Y, Ohtani Y (2006) Comparison of maximum drug concentration and area under the time-concentration curve between humans and animals for oral and intravenous investigational drugs. J Clin Pharmacol 46:674–692
Gad SC (2009) Clinical trials handbook. John Wiley & Sons, p 905
Grabowski T, Świerczewska A, Borucka B, Sawicka R, Sasinowska-Motyl M, Gumułka SW (2009) Chromatographic/mass spectrometric method for the estimation of itraconazole and its metabolite in human plasma. Application to a bioequivalence study. Arzneimittelforschung 8:422–428
Griffin S, Marcus A, Schulz T, Walker S (1999) Calculating the interindividual geometric standard deviation for use in the integrated exposure uptake biokinetic model for lead in children. Environ Health Perspect 107:481–487
Haidar SH, Davit B, Chen ML, Conner D, Lee L, Li QH, Lionberger R, Makhlouf F, Patel D, Schuirmann DJ, Yu LX (2008) Bioequivalence approaches for highly variable drugs and drug products. Pharm Res 25:237–241
HC (2010) Guidance for industry preparation of veterinary abbreviated new drug submissions—generic drugs. 1–71
Jansen RT, Laeven M, Kardol W (2002) Internal quality control system for non-stationary, non-ergodic analytical processes based upon exponentially weighted estimation of process means and process standard deviation. Clin Chem Lab Med 40:616–624
Jones GR (2009) Critical difference calculations revised: inclusion of variation in standard deviation with analyte concentration. Ann Clin Biochem 46:517–519
Julious SA, Debarnot CA (2000) Why are pharmacokinetic data summarized by arithmetic means? J Biopharm Stat 1:55–71
Keene ON (1995) The log transformation is special. Stat Med 14:811–819
Koch HJ (1985) On the relation between standard deviation and arithmetic mean in pharmacokinetic studies. Eur J Clin Pharmacol 46:573–574
Lam FC, Hung CT, Perrier DG (1985) Estimation of variance for harmonic mean half-lives. J Pharm Sci 74:229–231
Mahmood I (2005) Interspecies pharmacokinetic scaling: principles and application of allometric scaling. Pine 1st edn. House Publishers, pp 1–390
Ramirez E, Guerra P, Laosa O, Duque B, Tabares B, Lei SH, Carcas AJ, Frias J (2008) The importance of sample size, log-mean ratios, and intrasubject variability in the acceptance criteria of 108 bioequivalence studies. Eur J Clin Pharmacol 64:783–793
Riley RJ (2001) The potential pharmacological and toxicological impact of P450 screening. Curr Opin Drug Discov Dev 4:45–54
Roe DJ, Karol MD (1997) Averaging pharmacokinetic parameter estimates from experimental studies: statistical theory and application. J Pharm Sci 86:621–624
Rozet E, Marini RD, Ziemons E, Boulanger B, Hubert P (2011) Advances in validation, risk and uncertainty assessment of bioanalytical methods. J Pharm Biomed Anal 55:848–858
Sathirakul K, Chan C, Teng L, Bergstrom RF, Yeo KP, Wise SD (2003) Olanzapine pharmacokinetics are similar in Chinese and Caucasian subjects. Br J Clin Pharmacol 56:184–187
Sathyan G, Xu E, Thipphawong J, Gupta SK (2007) Pharmacokinetic investigation of dose proportionality with a 24-hour controlled-release formulation of hydromorphone. BMC Clin Pharmacol 7:3. doi:10.1186/1472-6904-7-3
Senn S (2002) Pharmaceutical statistics. John Wiley & Sons, p 95
Staatz CE, Tett SE (2007) Clinical pharmacokinetics and pharmacodynamics of mycophenolate in solid organ transplant recipients. Clin Pharmacokinet 46:13–58
Tubic M, Wagner D, Spahn-Langguth H, Weiler C, Wanitschke R, Böcher WO, Langguth P (2006) Effects of controlled-release on the pharmacokinetics and absorption characteristics of a compound undergoing intestinal efflux in humans. Eur J Pharm Sci 29:231–239
Van Peer A (2010) Variability and impact on design of bioequivalence studies. Basic Clin Pharmacol Toxicol 106:146–153
Veng-Pedersen P (2001) Noncompartmentally-based pharmacokinetic modelling. Adv Drug Deliv Rev 48:265–300
Yadav M, Shrivastav PS (2011) Incurred sample reanalysis (ISR): a decisive tool in bioanalytical research. Bioanalysis 3:1007–1024
Acknowledgments
The authors thank Professor Witold Gumułka for valuable comments and the critical reading of the manuscript. Special thanks are expressed to Karolina Flejszman for correcting grammar and language of the manuscript.
Conflict of interest
The authors declare that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article
Cite this article
Grabowski, T., Jaroszewski, J.J., Piotrowski, W. et al. Method of variability optimization in pharmacokinetic data analysis. Eur J Drug Metab Pharmacokinet 39, 111–119 (2014). https://doi.org/10.1007/s13318-013-0145-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13318-013-0145-x