
Abstract
Background
The purpose of this study was investigate the dose proportionality of a novel, once-daily, controlled-release formulation of hydromorphone that utilizes the OROS® Push-Pull™ osmotic pump technology.
Methods
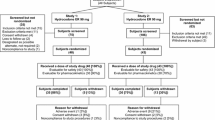
In an open-label, four-way, crossover study, 32 healthy volunteers were randomized to receive a single dose of OROS® hydromorphone 8, 16, 32, and 64 mg, with a 7-day washout period between treatments. Opioid antagonism was provided by three or four doses of naltrexone 50 mg, given at 12-hour intervals pre- and post-OROS® hydromorphone dosing. Plasma samples for pharmacokinetic analysis were collected pre-dose and at regular intervals up to 48 hours post-dose (72 hours for the 64-mg dose), and were assayed for hydromorphone concentration to determine peak plasma concentration (Cmax), time at which peak plasma concentration was observed (Tmax), terminal half-life (t1/2), and area under the concentration-time curve for zero to time t (AUC0-t) and zero to infinity (AUC0–∞). An analysis of variance (ANOVA) model on untransformed and dose-normalized data for AUC0-t, AUC0–∞, and Cmax was used to establish dose linearity and proportionality.
Results
The study was completed by 31 of 32 subjects. Median Tmax (12.0–16.0 hours) and mean t1/2 (10.6–11.0 hours) were found to be independent of dose. Regression analyses of Cmax, AUC0–48, and AUC0–∞ by dose indicated that the relationship was linear (slope, P ≤ 0.05) and that the intercept did not differ significantly from zero (P > 0.05). Similar analyses with dose-normalized parameters also indicated that the slope did not differ significantly from zero (P > 0.05).
Conclusion
The pharmacokinetics of OROS® hydromorphone are linear and dose proportional for the 8, 16, 32, and 64 mg doses.
Trial Registration
Clinical Trials.gov NCT00398957
Similar content being viewed by others


Background
Hydromorphone hydrochloride (HCl), which is available in immediate- and extended-release formulations, is a semi-synthetic opioid agonist that has been used widely for many years in the treatment of acute and chronic pain. A number of studies have demonstrated the efficacy and tolerability of hydromorphone in comparison with morphine and other opioid analgesic agents [1]. When formulated as an immediate-release preparation, hydromorphone has an elimination half-life of approximately 2 to 3 hours [2–4]. As a consequence, doses must be administered every 4 to 6 hours to ensure continuous analgesia for the patient [5].
To improve pain relief and provide convenient dosing for patients with severe chronic cancer and non-cancer pain, a novel 24-hour controlled-release formulation of hydromorphone is currently being investigated. This formulation uses the patented OROS® Push-Pull™ osmotic pump delivery system developed by ALZA Corporation (Palo Alto, CA) [6–8], and a consistent release of hydromorphone over 24 hours has been demonstrated in healthy volunteers [9]. Moreover, steady-state plasma concentrations for OROS® hydromorphone (Jurnista™, Janssen Pharmaceutica, N.V., Beerse, Belgium) are achieved after 48 hours (i.e., after two doses or by the third dose) and are maintained throughout the 24-hour dosing interval [10]. An initial study also has shown that the pharmacokinetics of hydromorphone are not substantially affected when OROS® hydromorphone is taken immediately after a high-fat meal [11].
Co-administration of OROS® hydromorphone with naltrexone, an opioid antagonist, under fasting conditions resulted in a 39% increase in Cmax, but there was no significant change in Tmax, AUC0-t, or AUC0–∞ [11]. These results indicate that blockade of opioid effects by naltrexone is useful in comparative bioavailability studies of high-dose opioids in healthy volunteers, with the assumption that all treatments are affected similarly. The objective of the present study was to evaluate the dose proportionality and linearity of OROS® hydromorphone at daily doses of 8, 16, 32, and 64 mg.
Methods
Subjects
Study volunteers were non-smoking, healthy male and female adults between 19 and 50 years of age. Their body weight was required to be between 61 and 100 kg and within ± 10% of the recommended weight range for height and body frame (1984 Metropolitan Height and Weight Tables). Results of the baseline screen were required to be negative for drugs of abuse (cannabinoids, opiates, cocaine, ethanol, and barbiturates). Subjects were required to have no clinically significant deviations from normal in laboratory results. All participants provided written informed consent. The study was approved by the Institutional Review Board and was carried out according to the Declaration of Helsinki and subsequent revisions.
Subjects who were intolerant of, or hypersensitive to, opioid agonists or antagonists were excluded, as were those with opioid dependency. Other exclusion criteria included gastrointestinal disorders; compromised cardiac, respiratory, renal, or hepatic function; psychiatric abnormalities; and significant hematologic, metabolic, or central nervous system disorders. Study participation did not permit any subject to take any long-term medication, enzyme-altering agents, recreational drugs, or an investigational agent within 30 days of beginning the study.
Study design and interventions
This was an open-label, randomized, four-way crossover study designed to examine the pharmacokinetic profile of once-daily OROS® hydromorphone for dose proportionality after administration of a single oral dose of 8, 16, 32, and 64 mg.
Based on the assumption that the within-subject variability is less than 20% (value guided by variability in exposure following immediate-release hydromorphone) and that there is a 5% difference between treatments, a sample size of 30 subjects was estimated to provide 80% power to demonstrate equivalence at the 0.05 level of significance.
Subjects received each of the four treatments (OROS® hydromorphone 8, 16, 32, and 64 mg, given after a 10-hour overnight fast), with a 7-day washout period between treatments. The order in which treatments were received was determined according to the predetermined randomization schedule. Naltrexone 50 mg was administered 12 hours before, with, and 12 hours after OROS® hydromorphone in all groups, with an additional 50-mg dose of naltrexone administered 24 hours after the 64-mg dose of OROS® hydromorphone. Naltrexone was administered to minimize adverse events following the higher doses of OROS® hydromorphone in these opioid-naïve subjects, and was given concomitantly with each dose level of OROS® hydromorphone to facilitate dose-proportionality comparisons.
Plasma sampling
Plasma samples for pharmacokinetic analysis were collected pre-dose (time 0) and at 2, 4, 6, 8, 10, 12, 16, 20, 24, 30, 36, 42, and 48 hours post-dose. Additional samples were taken at 56, 64 and 72 hours after the 64-mg dose. Plasma hydromorphone concentrations were measured using a validated LC/MS/MS method (CEDRA Corporation, Austin, TX) covering a range of 0.05 to 10 ng/mL. Calibration standards prepared for each of the sample sets were used to calculate the inter-day precision of the assay. The coefficients of variation for the standards ranged from 1.7% to 9.9%. The absolute deviations ranged from 0.05% to 2.6%.
Based on the measured hydromorphone concentration, the following parameters were calculated: peak plasma concentration (Cmax), time at which peak plasma concentration was observed (Tmax), terminal half-life (t1/2), and the area under the concentration-time curve from time 0 to time t (AUC0-t) and from time zero to infinity (AUC0–∞). The non-compartmental pharmacokinetic parameters described above were estimated using macros built in Excel (Microsoft, Redmond, WA).
Statistical analysis
Untransformed and log-transformed (ln) data for Cmax, AUC0-t and AUC0–∞ were analyzed using an appropriate analysis of variance (ANOVA) regression model to establish dose linearity and dose proportionality. All tests were two-sided at the 0.05 level of significance. Tmax was analyzed non-parametrically, without dose-normalization, using the Wilcoxon matched-pairs test for each pairwise comparison; the 95% confidence interval (CI) for the difference in treatment medians was constructed. Data for t1/2 were summarized using descriptive statistics. The apparent elimination-rate constant (K) for each subject was estimated by linear regression of the log-transformed concentration during the terminal log-linear decline phase of the curve. Terminal half-life was estimated as 0.693/K.
Results
Subjects
Thirty-two healthy volunteers were enrolled in the study, 8 in each of four treatments, with at least 24 subjects expected to complete the study. They were primarily male (63%) and Caucasian (81%), with a mean age of 33 years (Table 1). The study was completed by 31 subjects; one subject discontinued for personal reasons, after completing the first phase of treatment (64-mg dose).
Pharmacokinetics
The plasma concentration-time profiles of the four OROS® hydromorphone doses tested are shown in Figure 1. Following a single oral dose of OROS® hydromorphone, plasma mean concentrations gradually increase over 6 to 8 hours, and thereafter are sustained at or near maximum levels up to approximately 30 hours post-dose. The means of untransformed pharmacokinetic parameters and the medians of Tmax are shown in Table 2. Maximum plasma hydromorphone concentrations were achieved approximately 12 to 16 hours after administration, with no significant dose effect observed. Mean values for t1/2 were similar for the various doses (10.6–11.0 hours). Analysis of Cmax, AUC0-t, and AUC0–∞ by dose indicated that the relationship was linear (P ≤ 0.05) and that the intercept did not differ significantly from zero (P > 0.05; Figure 2).

Mean plasma hydromorphone concentrations over time after administration of single-dose OROS® hydromorphone.

Analyses of dose linearity with OROS® hydromorphone: (A) Cmax/dose; (B) AUC0–48/dose. Dashed lines represent 95% CI.
Mean dose-normalized pharmacokinetic parameters for OROS® hydromorphone after administration of 8, 16, 32, and 64 mg doses are shown in Table 3. Cmax and AUC increased linearly and in a manner proportional to the dose of OROS® hydromorphone. The slopes of dose-normalized Cmax and AUC vs. dose did not differ significantly from zero (P > 0.05; Figure 3). Inter-subject variability in pharmacokinetic parameters was similar across the doses except for high variability of Cmax following the 8-mg dose. This was mainly due to one subject with a high concentration (>5 times the mean). When this subject was excluded, Cmax variability for the 8-mg dose was similar to the other doses. No significant gender-by-treatment interactions were observed (ANOVA model; data not shown).

Analyses of dose proportionality with OROS® hydromorphone: (A) Cmax/dose; (B) AUC0–48/dose. Dashed lines represent 95% CI.
Safety
At least one adverse event was experienced by 21 of the 32 subjects (66%). All events were of mild or moderate intensity, and none were considered serious. Headache, asthenia, and nausea were the most common adverse events, occurring in 31%, 28%, and 28% of patients, respectively, during one or more of the treatment periods. The adverse events for each dose group are shown in Table 4. No treatment-related trends were noted with regard to vital signs, electrocardiogram results, or clinical laboratory data.
Discussion
The results of this study indicate that plasma hydromorphone concentrations and overall exposure to hydromorphone are proportional to the administered dose (over the 8- to 64-mg dose range) with OROS® hydromorphone. The time to achieve maximum plasma concentration was independent of dose. Near-maximum plasma concentrations were reached approximately 6 hours after dosing, and plasma concentrations were maintained at or near maximum levels throughout a 30-hour period, consistent with once-daily dosing. Beginning 24 to 30 hours post-dose, plasma hydromorphone concentrations declined slowly, with an apparent terminal half-life of approximately 10 hours. This is longer than the half-life of immediate-release hydromorphone (2–3 hours), which has been determined from studies with intravenous formulations [2–4]. The present study included plasma sampling for up to 72 hours post-dose, and it was designed to characterize both the controlled-release and the post-absorptive elimination phases of the drug. The apparent terminal half-life observed in this study is similar to that seen in a study designed to assess the effects of food intake on the pharmacokinetics of OROS® hydromorphone [11]. The observed plasma profile with concentration maintained over 24 hours supports the proposed once-daily administration of OROS® hydromorphone.
An exploratory analysis suggested no influence of gender on the pharmacokinetics of OROS® hydromorphone for the dose range studied. Although limited, these data do suggest that there are no clinically relevant differences between males and females with respect to the pharmacokinetics of OROS® hydromorphone.
Safety results were consistent for all four OROS® hydromorphone doses, indicating no dose relationship with the incidence of adverse events. Adverse events were consistent with those expected for an opioid agonist and antagonist and primarily affected the digestive and central nervous systems. No serious adverse events were reported during the study.
Conclusion
Plasma concentrations of OROS® hydromorphone and its pharmacokinetic parameters were found to be proportional to the orally administered dose over the dose range studied (8 mg to 64 mg). Plasma concentrations achieved the maximal level by approximately 16 hours after single administration, independently of dose, and remained near that level for up to 30 hours. Adverse events were consistent with those expected for an opioid agonist and antagonist.
References
Quigley C, Wiffen P: A systematic review of hydromorphone in acute and chronic pain. J Pain Symptom Manage. 2003, 25: 169-178. 10.1016/S0885-3924(02)00643-7.
Hill HF, Coda BA, Tanaka A, Schaffer R: Multiple-dose evaluation of intravenous hydromorphone pharmacokinetics in normal human subjects. Anesth Analg. 1991, 72: 330-336. 10.1213/00000539-199103000-00009.
Vallner JJ, Stewart JT, Kotzan JA, Kirsten EB, Honigberg IL: Pharmacokinetics and bioavailability of hydromorphone following intravenous and oral administration to human subjects. J Clin Pharmacol. 1981, 21: 152-156.
Parab PV, Ritschel WA, Coyle DE, Gregg RV, Denson DD: Pharmacokinetics of hydromorphone after intravenous, peroral and rectal administration to human subjects. Biopharm Drug Dispos. 1988, 9: 187-199. 10.1002/bod.2510090207.
Murray A, Hagen NA: Hydromorphone. J Pain Symptom Manage. 2005, 29 (5S): S57-S66. 10.1016/j.jpainsymman.2005.01.007.
Theeuwes F: Elementary osmotic pump. J Pharm Sci. 1975, 64: 1987-1991. 10.1002/jps.2600641218.
Palangio M, Northfelt DW, Portenoy RK, Brookoff D, Doyle RT, Dornseif BE, Damask MC: Dose conversion and titration with a novel, once-daily, OROS osmotic technology, extended-release hydromorphone formulation in the treatment of chronic malignant or nonmalignant pain. J Pain Symptom Manage. 2002, 23: 355-368. 10.1016/S0885-3924(02)00390-1.
Bass DM, Prevo M, Waxman DS: Gastrointestinal safety of an extended-releasenondeformable, oral dosage form (OROS®). A retrospective study. Drug Saf. 2002, 25: 1021-1033. 10.2165/00002018-200225140-00004.
Drover DR, Angst MS, Valle M, Ramaswamy B, Naidu S, Stanski DR, Verotta D: Input characteristics and bioavailability after administration of immediate and a new extended-release formulation of hydromorphone in healthy volunteers. Anesthesiology. 2002, 97: 827-836. 10.1097/00000542-200210000-00013.
Summary of Product Characteristics for JURNISTA. ALZA Corporation,Mountain View, CA., May 2006,
Sathyan G, Xu E, Gupta S: Effect of food on the pharmacokinetic profile of OROS hydromorphone [abstract]. IASP Press. 2005, 632: Abstract 1796-P299
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1472-6904/7/3/prepub
Acknowledgements
This study was supported by Alza Corporation, Mountain View, CA, USA.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Financial Competing Interests
In the past five years none of the authors of this manuscript have received reimbursements, fees, funding, or salary from an organization that may in any way gain or lose financially from publication of this manuscript, either now or in the future.
The authors of this manuscript do hold stock in ALZA Corporation but the stock price is not affected by the product alone or the publication.
There are no patents filed based on the data disclosed in this publication. The authors have not received reimbursements, fees, funding, or salary from an organization that holds or has applied for patents relating to the content of the manuscript.
The authors do not have any other financial competing interests.
The authors do not have any non-financial competing interests (political, personal, religious, academic, ideological, intellectual, commercial or any other) to declare in relation to this manuscript.
Authors' contributions
GS reviewed the pharmacokinetic and statistical results and authored the related sections. EX performed all the pharmacokinetic and statistical analysis. SKG participated in the conception of OROS hydromorphone product and contributed to the design of the study. JT reviewed the safety results and authored the related sections. All authors read and approved the final manuscript. All authors wish to acknowledge Philip Sjostedt and PharmaGenesis, Inc., in preparation of this manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
{kind=link}
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Sathyan, G., Xu, E., Thipphawong, J. et al. Pharmacokinetic investigation of dose proportionality with a 24-hour controlled-release formulation of hydromorphone. BMC Clin Pharmacol 7, 3 (2007). https://doi.org/10.1186/1472-6904-7-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1472-6904-7-3