
Abstract
Introduction
The recent advent of disease-modifying therapies (DMTs) has dramatically changed the treatment landscape of spinal muscular atrophy (SMA), and the multifaceted impact of this advancement has not been assessed thoroughly in the growing body of literature. We sought to summarize the literature on the natural history of SMA and the impact of SMA DMTs, including health-related quality of life (HRQOL) and utilities, clinical efficacy and safety, and economic impact.
Methods
Systematic literature reviews were conducted following PRISMA guidelines with no inclusive dates. Relevant studies were identified by searching full-text databases on November 12–13, 2020, including MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials, and EconLit, conference proceedings, health technology assessment databases, and clinical trial registries. All searches used a combination of MeSH and key terms. Studies were screened according to criteria based upon population, intervention, outcomes, and study design structure.
Results
Findings from 17, 23, 32, and 42 studies were included for the evaluation of natural history of SMA, HRQOL and utilities, clinical efficacy and safety, and economic impact of DMTs, respectively. Currently available data indicate that untreated SMA is associated with considerable humanistic and economic burden, with estimates of costs varying by treatment. While a variety of interventions have been evaluated in SMA clinical trials, quantitative synthesis of safety and efficacy findings was not feasible because of inconsistencies in reported outcomes. Data assessing impacts of DMTs on HRQOL were also lacking.
Conclusions
Overall, this systematic literature review highlights a clear need for up-to-date and methodologically rigorous clinical, HRQOL, and economic data to support unbiased assessments of the relative clinical and economic effectiveness of SMA treatments. More research is required to extend our understanding of the burden of SMA on HRQOL utility assessments and the impact of new DMTs on HRQOL and utilities for patients with SMA.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
The advent of disease-modifying therapies has transformed the treatment landscape for spinal muscular atrophy, which is reflected by the large volume of recent literature. |
We conducted a systematic literature review to summarize this material, focusing on the natural history of spinal muscular atrophy and the impact of disease-modifying therapies, including clinical efficacy and safety, health-related quality of life, and economic impact. |
What was learned from the study? |
Our literature review indicates substantial methodological heterogeneity between studies in the large volume of recent literature on spinal muscular atrophy and disease-modifying therapies for spinal muscular atrophy in particular. We conclude that opportunities for synthesis (and thus ability to reach overarching conclusions on the relative efficacies and safety results of different interventions) are limited. |
The variety of interventions evaluated in clinical trials reflects a changing therapeutic landscape in which disease-modifying therapies have recently been developed and approved. |
Overall, this review highlights a clear need for up-to-date and methodologically rigorous clinical, health-related quality of life, and economic data to support unbiased assessments of the relative clinical and economic effectiveness of spinal muscular atrophy treatments. |
Introduction
Spinal muscular atrophy (SMA) is a rare autosomal recessive disease that is caused by biallelic mutations in the survival motor neuron 1 (SMN1) gene [1, 2]. The most severe forms of SMA are characterized by motor neuron degeneration and progressive loss of muscle function that culminate in death or permanent ventilation early in childhood [3].
Before the development of disease-modifying therapies (DMTs), prognoses for patients with SMA were changing because of advances in nutritional and respiratory care, physiotherapy, and strategies to maintain independent living. While some improvements were achieved for even the most severely impacted patients, no clinical evidence confirmed that these strategies altered any neuropathologic process or neuromuscular function (i.e., mechanism of disease) [4].
Moreover, although several different compounds were investigated in randomized controlled trials (RCTs), including treatments intended to increase muscle function and strength (e.g., hyperacetylation agents, anabolics, thyrotropin-releasing hormone, growth hormone, neuroprotective agents such as gabapentin, riluzole, and olesoxime), all produced negative results for their respective primary endpoints, and none were approved [5]. However, with the advent of DMTs (e.g., nusinersen, risdiplam, and onasemnogene abeparvovec), the prognosis for patients with SMA has significantly improved. Prior to these discoveries, SMA was the leading genetic cause of infant mortality [1, 6]. Adherence to the recommendations put forth in the 2007 Consensus Statement for the Standard of Care in Spinal Muscular Atrophy, which includes early assessments of respiratory, feeding, and nutritional needs, may help reduce the severity of SMA and improve health-related quality of life (HRQOL) for patients with SMA [7].
Nusinersen is an antisense oligonucleotide that modifies pre-messenger RNA splicing of the survival motor neuron 2 (SMN2) gene to promote increased production of full-length, functional SMN protein. Treatment is initiated with four loading doses followed by maintenance dosage once every 4 months [8, 9]. In a sham-controlled RCT (ENDEAR; NCT02193074) [10], patients with nusinersen-treated SMA type 1 experienced a significantly greater likelihood of event-free survival (P = 0.005) and motor milestone response (51% vs. 0) compared with the control group [10]. Overall survival was significantly greater in the nusinersen group versus the control group (P = 0.004).
Onasemnogene abeparvovec is a gene replacement therapy that delivers a functional human SMN transgene to motor neurons via one-time intravenous infusion [11]. In the Phase I START study (NCT02122952; n = 15), treatment of symptomatic SMA with onasemnogene abeparvovec resulted in significant improvements in survival, motor milestones, and function without the need for permanent ventilation [12]. STR1VE-US (NCT03306277) [13], a completed Phase III study, demonstrated that the favorable risk-benefit profile first observed in START [12] was confirmed for a larger group of patients (n = 22 vs. n = 15). In STR1VE-US, 59% of patients receiving onasemnogene abeparvovec achieved functional independent sitting for 30 s or longer at the 18-months-of-age study visit (vs. 0 in the untreated cohort; P < 0.0001) and 91% survived free from permanent ventilation at age 14 months (vs. 26% in the untreated cohort; P < 0.0001).
Risdiplam is a SMN2 splicing modifier designed to treat patients with SMA that is caused by mutations in chromosome 5q that lead to SMN protein deficiency [14]. In FIREFISH, 41% (7/17) of infants treated with the therapeutic dosage achieved the ability to sit without support for at least 5 s as measured by the Bayley Scales of Infant and Toddler Development Third Edition (BSID-III) [15]. In addition, 90% (19/21) of infants were alive without permanent ventilation at 12 months of treatment and reached 15 months of age or older [16]. In SUNFISH, children and adults treated with risdiplam experienced a clinically meaningful and statistically significant improvement in motor function at 12 months (1.55 point mean difference; P = 0.0156) compared with placebo (1.36 points [95% CI 0.61, 2.11]; –0.19 points [95% CI –1.22, 0.84], respectively), as measured by a change from baseline in the Motor Function Measure-32 total score [17].
Based upon these trial results, nusinersen has been approved for use in the United States, Europe, Canada, Japan, and several other countries in Asia and the Middle East. Onasemnogene abeparvovec has been approved for use in the United States, Europe, Japan, and many other countries in South America and Asia. Risdiplam has been approved in the United States and European Union [14, 18]. Nusinersen and onasemnogene abeparvovec are also recommended by the National Institute for Health and Care Excellence (NICE) in the United Kingdom [19].
While the advent of DMTs has clearly and dramatically improved prognoses for patients with SMA, their full impact is unquestionably multifactorial and not completely understood. Therefore, we conducted systematic literature reviews (SLRs) to summarize and provide a landscape synthesis of the current published literature on the natural history of SMA, the HRQOL and utilities, the impact of recent DMTs (including efficacy and safety), and the economic burden of SMA.
Methods
Literature reviews were performed on November 12–13, 2020, and were designed, completed, and reported following PRISMA guidelines [20]. Full-text studies were identified by searching the following databases: MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials, and EconLit. Inclusive dates were not used for this SLR. Full methodology for searches for all four SLRs can be found in the Supplementary Material.
Study Selection and Eligibility Criteria
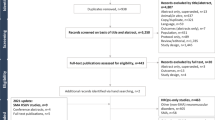
Study eligibility criteria were defined based on the population, interventions, comparators, outcomes, and study design structure outlined in Tables 1, 2, 3, and 4, which guided the identification and selection of studies related to each of the four SLRs, respectively. Only prospective studies with at least 12 months of follow-up were included in our analysis. Further information regarding the review and data selection process can be found in the Supplementary Material. Two reviewers (RG, AK), working independently, reviewed all materials identified by the search according to the selection criteria, with the exception of outcome criteria, which were only applied during the screening of full-text publications. All studies identified as eligible during abstract screening were then screened at a full-text stage by the same two reviewers. The full-text studies identified at this stage were included for the data extraction. Following reconciliation between the two investigators, a third reviewer (YZ) was added to reach consensus for any remaining discrepancies. The process of study identification and selection for each SLR is summarized with PRISMA flow diagrams (Figs. 1, 2, 3, 4) [20]. For RCTs with a placebo arm, data from the placebo arm were included in the review of natural history.

Study selection flow diagram for natural history review

Study selection flow diagram for health-related quality of life review

Study selection flow diagram for clinical review

Study selection flow diagram for economic review
The endpoints considered in the included studies are all objective clinical outcomes, including survival outcomes, motor functionality, and ventilation support, which are not likely to be exposed to bias from the placebo effect. The double-blind study design also minimizes the risk of the placebo effect.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Results
Systematic Literature Review of Natural History
Study Selection and Overview
Figure 1 presents the PRISMA flow diagram of the study selection process for the search to identify RCTs and prospective cohort studies of interest for the SLR of the natural history of SMA types 1, 2, and 3. Of the 17 natural history studies identified by this SLR, one (ENDEAR [10, 21,22,23,24,25]) was an RCT, and those remaining were either prospective or longitudinal cohort studies. The ENDEAR RCT was conducted internationally across centers in Europe, North America, and Asia Pacific. Three other studies were conducted internationally in North America and Europe. Among the included studies, three were conducted at multiple centers in North America, six at multiple centers in Europe, three at single centers in the United States, Chile, and Spain, and one in The Netherlands. Of these observational studies, only one (NeuroNEXT [26]) was comparative, assessing individuals with SMA type 1 versus matched healthy control infants. Each study had a planned follow-up duration of ≥12 months. A summary of study characteristics of the included studies is given in Table 5 [10, 21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41].
Receipt of no intervention, best supportive care (BSC), or palliative care was of interest in this natural history review of patients with SMA types 1, 2, and 3. Although the ENDEAR clinical trial compared nusinersen with a sham procedure that consisted of a small needle prick on the lower back at the location at which the intrathecal injection of nusinersen is normally made, only data from the sham-controlled arm were extracted and reported for the natural history review [10, 21,22,23,24,25]. The remaining 16 natural history studies were non-interventional and did not report details of any background treatment or supportive care that patients received.
SMA Disease Type
Five studies reported patient characteristics for patients with SMA type 1 (Table 6) [10, 26,27,28,29]. Nine studies in the review reported patient characteristics for those with SMA types 2 and 3 (Table 7) [29, 31,32,33,34,35,36,37,38,39,40, 42]. Finkel et al. [27] evaluated both SMA types 1 and 2, reporting data separately for SMA type 1 and for subgroups of SMA type 1: type 1B (symptom onset at <3 months of age) and type 1C (symptom onset at >3 months of age). These categories were then further broken down by “recent” (enrolled within 3 months of diagnosis) or “chronic” (enrolled beyond 3 months of diagnosis) SMA. For SMA type 1, the average age of patients at the time of study enrollment ranged from 131 days to 59 months, whereas for SMA types 2 and 3, the average age of patients ranged from 4.6 to 35.57 years. Piepers et al. [41] assessed SMA type 3B (symptom onset at >3 years of age) and type 4 (symptom onset at >19 years of age). For SMA type 3B, the age at onset ranged from 10–16 years, and the age at onset for SMA type 4 ranged from 27–34 years [41]. Finally, Wijngaarde et al. [43] assessed SMA types 1, 2, 3, and 4 and separately reported data by SMA subtypes 1A, 1B, 1C, 2A, 2B, 3A, and 3B. The classification of SMA type and subtype in this study was based on age at symptom onset and highest acquired motor developmental milestones.
Outcome Reporting
Survival, including overall and event-free survival, was assessed in five studies, motor function in 15 studies, ventilation support in seven studies, and nutritional support in two studies (Table 8) [10, 26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41, 43]. Five studies (ENDEAR [10], Finkel et al. [27], Finkel et al. [28], NeuroNEXT [26], and Wijngaarde et al. [43]) reported some form of overall survival or event-free survival outcome, as summarized in Table 8. Overall survival was defined as the percentage of the population alive at the study’s last follow-up endpoint. Event-free survival was defined as the percentage of patients who had not reached the combined endpoint of death or need for a minimum of 16 h/day of permanent ventilation support. Wijngaarde et al. [43] also assessed the combined endpoints of death or the need for a minimum of 12 h/day of permanent ventilation support and death or the need for nocturnal ventilation. Event-free survival was generally not reported in the analysis populations for natural history studies during the time points measured, except for two studies. Finkel et al. [27] reported 14 months of event-free survival for patients with SMA type 1C. Wijngaarde et al. [43] reported a median event-free survival of 9 days for patients with SMA type 1A, 7.7 months for patients with SMA type 1B, and 17 years for patients with SMA type 1C. Median event-free survival was not achieved for patients with SMA types 2, 3, and 4 in Wijngaarde et al. [43]. Overall survival for patients with SMA type 1 ranged from 5.3–8 months, 6–12 months for patients with type 1B (177 months for chronic type 1B), and 11.5–32 months for patients with type 1C [10, 26,27,28, 43].
Motor function assessments (summarized in Table 9) were conducted in 15 of 17 studies [10, 26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41, 43]. The most commonly reported motor function measurements included Children’s Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP INTEND), Hammersmith Functional Motor Scale (HFMS), HFMS expanded, the Revised Upper Limb Module, Motor Function Measure (MFM), Gross MFM, and the 6-min walk test.
Ventilation support was captured by seven studies [10, 24, 26,27,28,29, 33, 43], but they varied in definition. The ENDEAR trial [10, 21,22,23,24,25] captured the use of ventilator support at baseline and reported use of permanent assisted ventilation at the end of the study’s follow-up. Finkel et al. [27] reported the percentage of patients who received ventilation support (non-invasive ventilation or intubation), Finkel et al. [28] reported the percentage of patients who required >16 h of mechanical ventilator support, and NeuroNEXT [26] reported the percentage of patients who needed intubation during the study’s follow-up. Alvarez et al. [29] summarized ventilator support outcomes during the study, whereas NatHis-SMA [33, 34] reported these outcomes at baseline. Finally, Wijngaarde et al. [43] reported the percentage of patients who depended on at least ≥8–12 h of mechanical ventilation or nocturnal mechanical ventilation. This study also reported the ventilator dependency rate at various time points during the follow-up [43]. Only two studies captured information on nutritional support (Table 8).
Finkel et al. [27] and ENDEAR [10, 21,22,23,24,25] reported on the use of the gastrointestinal tube, with the latter revealing this outcome at baseline only. Quality assessments of the studies are covered in the Supplementary Material.
Systematic Literature Review of HRQOL and Utilities
Study Selection and Overview
Figure 2 presents the PRISMA flow diagram of the study selection process for the original and updated search to identify studies that described the humanistic burden of SMA. A total of 23 unique studies were included in the review, which corresponded to 27 publications (Fig. 2; Table 10) [44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70]. These publications included two SLRs (Landfeldt et al. [56], Wadman et al. [67]). Wadman et al. [67] reviewed trials that evaluated the safety and efficacy of drug treatments for SMA types 2 and 3 and reported a change in HRQOL as a secondary outcome, whereas Landfeldt et al. [56] conducted a systematic review of studies reporting HRQOL outcomes for all SMA types. Of the remaining unique 21 studies, 12 used the Pediatric Quality of Life Inventory (PedsQL) as an HRQOL measure. Other study characteristics of the included studies are described in Table 11 [44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69]. Eight studies assessed the impact of DMTs on the HRQOL of patients with SMA, and these are summarized below. Overall, there was limited evidence available on the impact of DMTs on HRQOL.
Outcome Reporting
In an abstract presented at the American Academy of Neurology in 2020, Belter et al. [44] reported HRQOL among patients with SMA types 1 to 3 based on 281 responses collected in the Cure SMA community update survey in 2019. The HRQOL measures included Health Utilities Index Mark 2 (HUI2) and HUI3, which were described for patients with treatment versus patients without treatment by SMA type. Patients with treatment had greater HRQOL scores across all SMA types compared with patients not receiving treatment, although treatment information was not disclosed in the abstract.
Bertini et al. [46] examined HRQOL among patients with SMA types 2 and 3 as part of a multicenter Phase II RCT that studied the effects of olesoxime versus placebo. Participants had to have been between 3 and 25 years of age, had type 2 or non-ambulatory type 3 SMA, and had an MFM relative score of ≥15% and an HFMS score between 3 and 38, with onset of SMA symptoms at 3 years of age or younger. HRQOL was measured using the PedsQL Neuromuscular Module, including both patient- and parent-reported assessments. Of 158 included patients, 136 completed at least a baseline rating and one follow-up HRQOL rating. The difference in change in HRQOL from baseline between the olesoxime and placebo groups was not statistically significant for any subpopulation by age or subscore by PedsQL module. However, because scores were reported as differences in change from baseline between treatment groups, there is no indication whether HRQOL improved or declined in either group, respectively. Study authors concluded that no clear benefit of olesoxime treatment was observed regarding HRQOL outcomes. However, the authors also asserted that the validity and sensitivity of the PedsQL had not been fully established in patients with SMA.
Johnson et al. [50, 51] examined the impact on caregivers through Assessment of Caregiver Experience with Neuromuscular Disease (ACEND) scores and changes in HRQOL through the parent version of PedsQL using data from the CHERISH trial, which randomized children aged 2 to 12 years of age with SMA types 2 and 3 to nusinersen or control (sham procedure). The change in ACEND (least squares mean difference) was measured in seven subdomains at 6 and 15 months. HRQOL was measured using the PedsQL Generic Core Scale and Neuromuscular Module through parent-reported assessments. A reduced impact on caregivers in the nusinersen arm was reported over time in three ACEND subdomains: feeding/grooming/dressing, transfer, and mobility. The decline in PedsQL scores for the nusinersen arm was reported to be less than the decline in scores in the sham control arm from baseline to month 15.
Montes et al. [63] examined change in HRQOL for patients with later-onset SMA and the impact on caregivers based on data from SHINE and CHERISH. SHINE is an open-label extension study that enrolled patients from multiple completed clinical trials, including CHERISH, EMBRACE, and ENDEAR. HRQOL was measured using the caregiver-reported PedsQL Generic Core Scale and Neuromuscular Module for patients from the nusinersen-treated group in CHERISH. Impact on caregivers was measured using ACEND scores among parents of the same patient population. Both PedsQL and ACEND scores were compared between baseline and day 1170 of CHERISH. For ACEND, only five out of seven subdomain scores were reported. This study also stated that greater benefits in caregiver impact were observed among patients who initiated nusinersen earlier (aged ≥2 and <3.5 years) than later (aged ≥3.5 and <5 years) in six out of seven ACEND subdomains. However, the corresponding ACEND scores were not reported. Quality assessments of the studies are contained in the Supplementary Material.
Swoboda et al. [48] examined HRQOL among patients with SMA types 2 and 3 in Part 1 of SMA CARNI-VAL, a multicenter Phase II RCT that examined the effects of valproic acid (VPA) and levocarnitine (l-carnitine) versus placebo in non-ambulatory pediatric patients with SMA types 2 or 3 who were aged 2 to 8 years and had Modified HFMS (MHFMS) scores between 2 and 37. HRQOL was measured using the PedsQL, including both patient-reported and parent-reported assessments at baseline, but just parent-reported assessments at 6 months of follow-up. The number of patients completing HRQOL assessments varied across PedsQL subscales. Overall, the change from baseline in parent-reported PedsQL scores was not significantly different between treatment groups (VPA + l-carnitine and placebo). No clear benefit of VPA + l-carnitine was observed with regard to HRQOL. Although PedsQL total HRQOL ratings did not improve as MHFMS improved, there was evidence of deterioration of HRQOL as MHFMS declined over time.
Kissel et al. [49] examined HRQOL in Part 2 of SMA CARNI-VAL, an open-label trial conducted in parallel with Part 1, in which all patients received a VPA and l-carnitine combination regimen. Eligible participants had SMA type 2 or 3, were 3 to 17 years of age, and were capable of standing independently for at least 2 s. HRQOL was assessed using the PedsQL, including both patient- and parent-reported assessments. Data were provided only for patient-reported PedsQL ratings, but the authors noted that there was no associated change in any domain of HRQOL by parental assessment. Of 33 included patients, 22 reported PedsQL values at baseline, 17 reported values at 6 months, and 16 reported values at 12 months. Patient-reported physical function demonstrated statistically significant deterioration at 12 months, with study authors concluding that VPA + l-carnitine failed to improve HRQOL.
Systematic Literature Review of Clinical Efficacy and Safety
Study Selection and Overview
Figure 3 presents the PRISMA flow diagram of the study selection process for the search to identify RCTs and single-arm trials of interest for the SLR of clinical efficacy and safety. This review identified 16 single-arm studies, 11 RCT studies, and five dose-escalation studies (Table 12) [10, 46, 48,49,50, 52, 63, 71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97], which assessed a variety of therapies for SMA. Patient characteristics across the 32 included studies are summarized in Table 13 [10, 46, 48,49,50, 52, 63, 71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97]. Among the 13 included studies with exclusively presymptomatic patients or those with SMA type 1, age at study onset ranged from a median of 19 days in NURTURE [84, 85] to a mean of 9.3 months in Russman et al. [87]. For the 14 included studies with patients with exclusively SMA types 2 and 3, median age at study onset ranged from approximately 4.4 months in Darras et al. [73] to 16.6 years in Chen et al. [71].
Treatments
The therapeutic interventions evaluated in published literature have changed over time with the advent of new treatments such as nusinersen, onasemnogene abeparvovec, and risdiplam. Of the included studies, nine reported nusinersen regimens, six investigated onasemnogene abeparvovec, four assessed VPA, three evaluated risdiplam, and two evaluated olesoxime and salbutamol; hydroxyurea, riluzole, branaplam, somatropin, 4-aminopyridine, and reldesemtiv were each evaluated in one study. Interventions evaluated in trials published in the last 2 years include gene therapy, antisense oligonucleotides, small-molecule therapies, and neuroprotective therapies [98].
Outcome Reporting
The outcomes reported were broadly consistent for SMA types across the included studies. However, scales and measures used to assess these outcomes varied across studies. Motor function was assessed in patients with SMA type 1 using measures explicitly indicated for infants, such as the CHOP INTEND, Hammersmith Infant Neurological Examination-Part 2 (HINE-2), and Test of Infant Motor Performance Screening Items. Ventilator use was only measured in studies of patients with SMA type 1, and forced vital capacity was only measured for patients with SMA types 2, 3, or 4. Quality assessments of the studies are contained in the Supplementary Material.
Systematic Literature Review of Economic Burden
Study Selection and Overview
Figure 4 presents the PRISMA flow diagram of the study selection process for the search to identify studies of interest in the SLR of economic burden. The final list of included studies and publications is presented in Table 14 [55, 59, 61, 62, 65, 69, 99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134]. Among the 42 included studies on economic burden, 20 were cost analyses that reported on the cost of illness. In addition, 20 were full economic evaluations that modeled the cost-effectiveness or cost utility of treatments for SMA; of these, seven were reported in documentation supporting either submissions to or recommendations from health technology assessment (HTA) organizations. Finally, among the remaining two studies, one was a clinical trial that reported health care resource utilization outcomes, whereas another was an SLR of economic burden and economic evaluations in SMA (Dangouloff et al. [133]). A systematic review of the literature identified 13 published full economic evaluations of SMA therapy. Six evaluations compared nusinersen with onasemnogene abeparvovec, five compared nusinersen with the standard of care or BSC, one compared onasemnogene abeparvovec versus BSC, and one compared both onasemnogene abeparvovec and nusinersen with BSC.
Cost Outcomes
Dangouloff et al. [133] reviewed studies evaluating the cost of SMA and economic evaluations of SMA therapies, including original articles published between January 1, 1998, and March 2020. Seven cost analyses and five economic evaluations were included. Cost outcomes reported by economic burden studies were adjusted to 2021 US dollars. The reported annual burden associated with untreated SMA type 1 ranged from $106,000 to $140,000 ($108,704–$143,571 2021 USD) versus $23,000 to $115,000 ($23,587–$117,933 2021 USD) for SMA types 2 to 4. In addition, the reported incremental cost-effectiveness ratios (ICERs) associated with novel therapies (i.e., nusinersen and onasemnogene abeparvovec) were generally > $200,000 versus no treatment. Because Dangouloff et al. [133] was a conference abstract, the list of included studies was not provided.
Costs
The literature review identified 20 published cost analyses. Ten studies were conducted in the United States, two in Canada, three in Spain, one in Australia, one in Germany, one in Turkey, one in the United Kingdom, and one in Europe (United Kingdom, France, and Germany). The year of costing to address inflation was reported by most of the studies. In general, studies did not clearly state whether costing was based on top-down or micro-costing, except for Chambers et al. [102].
In cost-effectiveness analyses, treatment with onasemnogene abeparvovec and nusinersen produced greater improvements in terms of quality-adjusted life-years (QALYs) compared with BSC, but these improved outcomes were also associated with greater total cost [65, 119]. Moreover, onasemnogene abeparvovec was cost-effective versus nusinersen in all included studies comparing these two treatments [62, 131].
Ali et al. [99] conducted a single-center retrospective analysis based on medical records of all children within the West Midlands, UK. Patients with SMA type 1 who were treated with nusinersen at the Royal Stoke University Hospital were observed to investigate the respiratory care, hospital utilization, and costs associated with newly treated SMA type 1 [99]. Eleven children who received nusinersen between May 2017 and April 2019 were enrolled in this study. The total number of hospital days since diagnosis was 1101, with a median of 118 (range 7–235) days per child, which included general pediatric ward days (median 0, range 0–63), more dependency unit days (median 79, range 7–173), and pediatric intensive care unit days (median 13, range 0–109) per child. This equated to a median of 20% (range 2–72) of their lives in the hospital, and the total cost of the hospital days for these 11 children was £2.2 M ($2.9 M 2021 USD).
Patients with SMA type 1 who were treated with nusinersen initially spend a considerable percentage of their early life in a hospital and have significant ongoing medical costs in addition to the cost of treatment received. Limitations of Ali et al. [99] are that the study includes only 11 patients treated at one center, which questions its representativeness; the retrospective nature of the study may have introduced bias; and the author did not adjust for such potential confounding factors as socioeconomic status and comorbidities.
All other cost-effectiveness data were extracted from seven HTAs: three from HTA agencies in the United Kingdom (one each from the UK’s NICE [19], the National Centre for Pharmacoeconomics Ireland [130], and the Scottish Medicines Consortium [126]), one from the Canadian Agency for Drugs and Technologies in Health [127], one from Croatia’s Agency for the Quality and Accreditation in Health Care and Social Welfare [128], one from the Swedish Dental and Pharmaceutical Benefits Agency [129], and one from the Institute for Clinical and Economic Review [131].
Malone et al. [61] developed a multi-state survival Markov model over a lifetime to assess the ICER of onasemnogene abeparvovec versus nusinersen in patients with SMA type 1 in the United States. Undiscounted total QALYs per patient were 30.3 for onasemnogene abeparvovec and 7.2 for nusinersen, whereas the discounted (at 3%) QALYs were 15.9 and 5.3, respectively. The estimated discounted lifetime costs were $6.33 M for nusinersen, while the lifetime discounted costs for onasemnogene abeparvovec at hypothetical price points from $2 M to $3 M per dose ranged from $3.7 M to $4.7 M per patient, resulting in cost savings and QALY gains compared with nusinersen. In a scenario analysis in which sitting patients who received gene therapy experienced the survival trajectory of walking patients, onasemnogene abeparvovec undiscounted QALYs were 57.5 (if discounted at 3%: 21.9) and onasemnogene abeparvovec again overshadowed nusinersen at a price of $3 M. The author further suggested that US-based decision-makers should also consider undiscounted QALY gain when assessing the value of innovative therapies because discounting QALYs at the US standard rate of 3% results in a substantial underestimate of health benefits. Reporting of study methods and results was limited to a single meeting abstract and key information, such as cost year, which was not always provided.
In the same year, Malone et al. [62] revised the Markov model and added more details in this full-text publication. Similar to the above, the objective was to investigate the cost-effectiveness of onasemnogene abeparvovec gene replacement therapy for SMA type 1 compared with nusinersen from the perspective of a commercial insurer in the United States. All costs were reported in 2018 USD based on a lifetime horizon. Survival, health care costs, and QALYs were estimated using natural history data for patients with SMA who achieved motor milestones, whereas health utility weights were obtained from the CHERISH trial [2, 51].
In the base case scenario [61], expected survival (undiscounted) over a lifetime predicted by the model was 37.20 life years for onasemnogene abeparvovec and 9.68 for nusinersen (undiscounted QALYs were 29.86 and 7.21, whereas discounted QALYs were 15.65 and 5.29, respectively). Using a potential onasemnogene abeparvovec price range ($2.5–5.0 M per treatment) and a discount rate of 3%, the estimated mean lifetime cost per patient was $4.2 M to 6.6 M for onasemnogene abeparvovec and $6.3 M for nusinersen. These costs were primarily driven by therapy treatment costs (i.e., the percentage of total costs ranging from 57 to 73% for onasemnogene abeparvovec and 70.9% for nusinersen). The ICER range was –$203,072 to $31,379 per QALY gained for onasemnogene abeparvovec versus nusinersen, indicating that onasemnogene abeparvovec was cost-effective when treatment costs are ≤$5 M. If patients treated with onasemnogene abeparvovec experienced a treatment waning and subsequent loss of milestones at 10 and 25 years, there would be a substantial impact on the survival outcomes (discounted QALYs of 7.80 and 12.95, respectively) and a corresponding reduction in lifetime medical costs. At a price of $5 M for onasemnogene abeparvovec, the estimated lifetime payer cost would be $6.2 M, assuming a 10-year duration of effect and $6.6 M assuming a 25-year duration of effect. Given that the estimated cost of lifetime nusinersen treatment is $6.3 M, onasemnogene abeparvovec dominates nusinersen, assuming a 10-year duration of effect, and generates an ICER of $30,926, assuming a 25-year duration of effect.
With the assumption that treated patients who sit have a normal mortality trajectory, the optimistic survival scenario would be the ICER increased to $57,261 because sitting patients incurred costs of care for longer durations, while the total QALY gain by onasemnogene abeparvovec over nusinersen increased to 16.19. The undiscounted QALYs may be as great as 56.35 years, and the cost per QALY gain for onasemnogene abeparvovec versus nusinersen is $18,864 ($14,347 for base case) [61]. Quality assessments of the studies are given in the Supplementary Material.
Discussion
Natural History
To focus our natural history SLR on the high-quality evidence published to date, we limited the observational evidence base to prospective studies with at least 12 months of follow-up only. However, some studies excluded for retrospective study design or insufficient follow-up may have presented data that would also further our understanding of the natural history of SMA. Because of the heterogeneous nature of the disease, some important endpoints may not be prospectively and consistently collected in the real-world setting. For natural history studies, the majority of included studies focused on children with SMA. In addition, survival outcomes were prospectively reported for patients with SMA type 1 only. Natural history studies prospectively reporting survival outcomes for patients with other types of SMA are warranted. Event-free survival, ventilation support, and nutritional support were prospectively reported by a limited number of studies. More evidence is needed to better understand the clinical course of SMA for these measures.
HRQOL and Utilities
The systematic review of humanistic burden identified studies with authors who concluded that symptomatic SMA corresponded to a strong deterioration in HRQOL for both patients and caregivers. Lower HRQOL was generally associated with the worse clinical phenotype. With the exception of those in the nusinersen 9-mg treatment arm in Chiriboga et al. [52], none of the treatments evaluated in the included trials demonstrated a significant improvement in HRQOL.
Overall, there are limited studies assessing the impact on HRQOL of patients. Health-related quality of life for both patients and their caregivers could be substantially affected by the disease. However, only a small percentage of studies assessed both patients and caregivers, and the majority of the studies focused on patients only. Future studies assessing the impact on caregivers or both patients and caregivers are warranted.
Clinical Efficacy and Safety
The systematic review of clinical efficacy and safety found 32 studies that evaluated various interventions, including conventional treatments and, more recently, DMTs in SMA. The included studies had considerable heterogeneity with respect to baseline patient characteristics, particularly age at diagnosis and study onset. Reported outcomes were broadly consistent for studies, including different SMA types, however, with varied scales or measurement tools to assess these outcomes. Studies with patients who were exclusively presymptomatic or had SMA type 1 generally reported motor function, ventilator use, and survival. Included studies with only patients with SMA types 2 and 3 generally reported motor function. Some of the included studies also evaluated muscle strength and respiratory outcomes, with most reporting adverse events. Varied scales and measures used to assess the outcomes across studies preclude a quantitative synthesis of existing evidence.
Humanistic and Economic Burden
Based on the available data, SMA is associated with substantial humanistic and economic burden. SMA cost data are plentiful, in both magnitude and treatments or resources for which they are available. However, comparisons of cost estimates across studies were hindered by differences in study methodology, choice of the associated time frame, and limitations inherent in the data. We observed large variations in attributable costs as well as in the drivers of costs. The economic costs of SMA are greater for direct medical costs to health care providers, non-medical costs incurred by patients and their caregivers, and indirect costs through productivity losses among informal caregivers. Costs also vary over the trajectory of the condition and are dependent on disease manifestation, progression, and duration of survival. To date, however, a limited number of economic evaluations of interventions for SMA have been published, and the cost-effectiveness of novel SMA therapies has not been conclusively established. Existing literature reported heterogeneous cost-effectiveness ratios and interpreted these ratios based upon different willingness-to-pay thresholds of what constitutes an acceptable threshold in varied settings. However, treatment with both onasemnogene abeparvovec and nusinersen produced larger QALY gains compared with BSC, but these improved outcomes were also associated with greater total costs. In addition, onasemnogene abeparvovec was cost-effective compared with nusinersen in all studies that evaluated these two treatments.
Although the literature suggests that the greater economic costs of SMA are consistent across different health care systems, the economic burden could be reduced by expanding newborn screening and early treatment for SMA [135]. In the future, broader elements of value beyond health gains directly related to treatment should be considered by using QALYs or greater cost-effectiveness thresholds. The use of cost-benefit analyses and saved young life equivalents could be used as an alternative to QALYs for the valuation of outcomes of gene replacement therapies because they use broader elements of value and avoid the challenges of eliciting utilities for pediatric diseases [136].
Additional Studies
Although this SLR captured a large volume of published literature on SMA treatments, there are some additional studies that should be acknowledged, many of which were published after the completion of our literature searches and some that were not returned in the search results, particularly studies related to DMTs.
In the NICE report published in July 2021 [137], after the SLR search was completed, the committee recommended onasemnogene abeparvovec as an option for treating 5q SMA with a biallelic mutation in the SMN1 gene and a clinical diagnosis of SMA type 1 in infants ≤6 months of age or 7–12 months of age. Because of the limited trial data for infants aged 7–12 months, their treatment should be discussed by a national multidisciplinary team. The treatment was only recommended for these two groups when permanent ventilation >16 h per day or a tracheostomy was not needed. Onasemnogene abeparvovec was recommended by NICE as an option for treating presymptomatic 5q SMA with a biallelic mutation in the SMN1 gene and up to three copies of the SMN2 gene in infants [137].
In the EMBRACE study, which evaluated nusinersen in infants and children with infantile- or later-onset SMA (n = 20), motor-milestone responder rates were greater in those receiving nusinersen (93%) versus those receiving sham treatment (29%) [138]. In the NUTURE study, De Vivo et al. [84] found substantial clinical benefit as a result of early initiation of nusinersen treatment in infants with two or three copies of the SMN2 gene (n = 15; considered most likely to develop SMA type 1 or 2).
New data from RESTORE [135, 139], a comprehensive registry of patients with SMA, were recently presented. In a conference poster, older patients with SMA aged ≥6 months at onasemnogene abeparvovec infusion benefited from treatment as measured by CHOP INTEND and HINE-2 scores. Another poster on the RESTORE registry demonstrated that newborn screening for patients with SMA was associated with significantly earlier diagnosis and intervention and generally achieving motor milestones at earlier ages than clinically diagnosed patients. Compared with those clinically diagnosed, patients who were diagnosed via newborn screening were less likely to receive more than one treatment for SMA.
In the absence of RCTs and head-to-head comparisons, a recent matching-adjusted indirect comparison [140] of patients from START [12], STR1VE-US [13], and SHINE [63, 88] studies demonstrated that treatment with onasemnogene abeparvovec provided significantly greater event-free survival compared with nusinersen for patients with SMA type 1. Patients treated with onasemnogene abeparvovec had numerically longer overall survival compared with nusinersen, although this result was not significant.
Results from the SUNFISH part 2 [141] study, a Phase III, randomized, double-blind, placebo-controlled study, have been recently published. Patients (N = 180) aged 2–25 years with confirmed 5q autosomal recessive SMA type 2 or type 3 were stratified by age and randomly assigned (2:1) to receive either daily oral risdiplam, at a dosage of 5.00 mg (for individuals weighing ≥20 kg) or 0.25 mg/kg (for individuals weighing <20 kg), or daily oral placebo. Treatment with risdiplam resulted in a significant improvement in motor function compared with placebo for patients aged 2–25 years with type 2 or non-ambulant SMA type 3. The exploratory subgroup analyses demonstrated that motor function was generally improved for younger patients and stabilized for older ones. These data require confirmation in further studies.
Some limitations are applicable to all reviews and should be acknowledged. As with any SLR, the evidence base continues to evolve. As such, recently published clinical trials may not have been captured because the searches were conducted up to and including November 2020. Therefore, an update to these SLRs to avoid potential bias as the evidence base evolves would be beneficial. Retrospective analyses and/or prospective studies with cross-sectional data can be informative, and the exclusion of these studies is another limitation of this study.
There is a risk of publication bias as some clinical trials were published as full-text articles while others were not, presenting limited information. To mitigate the risk, the current study encompassed an extensive search of conference abstracts, gray literature, and clinical trial registries, although studies from these sources do not always provide complete information. As such, studies identified from these sources should be interpreted with caution as they do not undergo the same peer-review process as fully published studies.
Cost data included in the economic review were derived from a heterogeneous set of studies that used varied methodologies. This lack of a standard method for collecting the cost data may impact some of our findings. Also, the included studies were conducted in different countries with various health care systems, which may limit the transferability and comparability of results.
Conclusions
In conclusion, our SLRs demonstrate substantial methodological heterogeneity between studies in the large volume of recent literature on SMA and, in particular, DMTs for SMA. We conclude that opportunities for synthesis (and thus the ability to reach overarching conclusions on the relative efficacy and safety of different interventions) are limited. The various interventions evaluated in SMA clinical trials reflect a changing therapeutic landscape in which DMTs have only recently been developed and approved. Without conducting a quantitative synthesis, further conclusions cannot be drawn about the relative efficacy and safety of different interventions.
Overall, this review has highlighted a clear need for up-to-date and methodologically rigorous clinical, HRQOL, and economic data to support unbiased assessments of the cost-effectiveness of future SMA treatments. More research is required to extend our understanding of the impact of SMA on HRQOL utility assessments and the impact of new DMTs on HRQOL and utilities for patients with SMA.
References
Sugarman EA, Nagan N, Zhu H, et al. Pan-ethnic carrier screening and prenatal diagnosis for spinal muscular atrophy: clinical laboratory analysis of >72,400 specimens. Eur J Hum Genet. 2012;20:27–32.
Kolb S, Kissel JT. Spinal muscular atrophy. Neurol Clin. 2015;33:831–46.
Tisdale S, Pellizzoni L. Disease mechanisms and therapeutic approaches in spinal muscular atrophy. J Neurosci. 2015;35:8691–700.
Talbot K, Tizzano EF. The clinical landscape for SMA in a new therapeutic era. Gene Ther. 2017;24:529–33.
Schorling DC, Pechmann A, Kirschner J. Advances in treatment of spinal muscular atrophy: new phenotypes, new challenges, new implications for care. J Neuromuscul Dis. 2020;7:1–13.
Awano T, Kim J-K, Monani UR. Spinal muscular atrophy: journeying from bench to bedside. Neurotherapeutics. 2014;11:786–95.
Wang CH, Finkel RS, Bertini ES, et al. Consensus statement for standard of care in spinal muscular atrophy. J Child Neurol. 2007;22:1027–49.
Wurster CD, Ludolph AC. Nusinersen for spinal muscular atrophy. Ther Adv Neurol Disord. 2018;11:1756285618754459.
US Food & Drug Administration. SPINRAZA prescribing information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/209531s010lbl.pdf. Accessed 2 Mar 2022.
Finkel RS, Mercuri E, Darras BT, et al. Nusinersen versus sham control in infantile-onset spinal muscular atrophy. N Engl J Med. 2017;377:1723–32.
ZOLGENSMA prescribing information. Updated October 2021. https://www.novartis.us/sites/www.novartis.us/files/zolgensma.pdf. Accessed 29 Oct 2021.
Mendell JR, Al-Zaidy S, Shell R, et al. Single-dose gene-replacement therapy for spinal muscular atrophy. N Engl J Med. 2017;377:1713–22.
Day JW, Finkel RS, Chiriboga CA, et al. Onasemnogene abeparvovec gene therapy for symptomatic infantile-onset spinal muscular atrophy in patients with two copies of SMN2 (STR1VE): an open-label, single-arm, multicentre, phase 3 trial. Lancet Neurol. 2021;20:284–93.
Risdiplam prescribing information. Updated April 2021. https://www.gene.com/download/pdf/evrysdi_prescribing.pdf. Accessed 27 Oct 2021.
Bayley N. Bayley scales of infant and toddler development. 3rd ed. New York: Psychological Corporation; 2006.
Baranello G, Darras BT, Day JW, et al. Risdiplam in type 1 spinal muscular atrophy. N Engl J Med. 2021;384:915–23.
A study to investigate the safety, tolerability, pharmacokinetics, pharmacodynamics and efficacy of risdiplam (RO7034067) in type 2 and 3 spinal muscular atrophy (SMA) (SUNFISH). ClinicalTrials.gov identifier: NCT02908685. Updated December 28, 2021. https://clinicaltrials.gov/ct2/show/NCT02908685. Accessed 2 Mar 2022.
European Medicines Agency. Evrysdi (risdiplam). https://www.ema.europa.eu/en/medicines/human/EPAR/evrysdi. Accessed 28 Oct 2021.
National Institute for Health and Care Excellence (NICE). Single technology appraisal—nusinersen for treating spinal muscular atrophy [ID1069]—committee papers. London, England: NICE; 2019. https://www.nice.org.uk/guidance/ta588/documents/committee-papers-4. Accessed 15 Aug 2021.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009;62:1006–12.
Mercuri E, Darras BT, Chiriboga CA, et al. Nusinersen versus sham control in later-onset spinal muscular atrophy. N Engl J Med. 2018;378:625–35.
Finkel R, Kuntz N, Mercuri E, et al. Efficacy and safety of nusinersen in infants with spinal muscular atrophy (SMA): final results from the phase 3 ENDEAR study. Eur J Paediatr Neurol. 2017;21(Suppl 1):e14–5.
McNeil E, Finkel R, Darras B, et al. Nusinersen improves motor function in infants with and without permanent ventilation: results from the ENDEAR study in infantile-onset spinal muscular atrophy (SMA). Ann Neurol. 2017;82:S264–5.
Servais L, Farrar M, Finkel R, et al. Nusinersen demonstrates greater efficacy in infants with shorter disease duration: end of study results from the ENDEAR study in infants with spinal muscular atrophy (SMA). Dev Med Child Neurol. 2017;59:17–8.
Yan L, Kuntz N, Farwell W, et al. Nusinersen in infants with spinal muscular atrophy (SMA): design/interim results of the ENDEAR study. No To Hattatsu. 2017;49:S280.
Kolb SJ, Coffey CS, Yankey JW, et al. Baseline results of the NeuroNEXT spinal muscular atrophy infant biomarker study. Ann Clin Transl Neurol. 2016;3:132–45.
Finkel RS, McDermott MP, Kaufmann P, et al. Observational study of spinal muscular atrophy type I and implications for clinical trials. Neurology. 2014;83:810–7.
Finkel RS, Weiner DJ, Mayer OH, McDonough JM, Panitch HB. Respiratory muscle function in infants with spinal muscular atrophy type I. Pediatr Pulmonol. 2014;49:1234–42.
Alvarez K, Suarez B, Palomino MJ, et al. Observations from a nationwide vigilance program in medical care for spinal muscular atrophy patients in Chile. Arq Neuropsiquiatr. 2019;77:470–7.
Exposito J, Natera-de Benito D, Carrera L, et al. Longitudinal study of the natural history of spinal muscular atrophy type 2 and 3. Neuromuscul Disord. 2019;29(Suppl 1):S132.
Pera MC, Coratti G, Mazzone ES, et al. Revised upper limb module for spinal muscular atrophy: 12 month changes. Muscle Nerve. 2019;59:426–30.
Mercuri E, Coratti G, Pera M, et al. Trajectories of disease progression in ambulant and non ambulant SMA: 12 month follow-up. Neuromuscul Disord. 2019;29(Suppl 1):S131.
Chabanon A, Seferian AM, Daron A, et al. Prospective and longitudinal natural history study of patients with type 2 and 3 spinal muscular atrophy: baseline data NatHis-SMA study. PLoS ONE. 2018;13: e0201004.
Servais L, Mihaela Seferian A, Daron A, et al. Natural history of type 2 and 3 spinal muscular atrophy (SMA): longitudinal 2-year NatHis-SMA study. Neurology. 2020;94(15 Suppl):530.
Kaufmann P, McDermott MP, Darras BT, et al. Prospective cohort study of spinal muscular atrophy types 2 and 3. Neurology. 2012;79:1889–97.
Mazzone E, De Sanctis R, Fanelli L, et al. Hammersmith functional motor scale and motor function measure-20 in non ambulant SMA patients. Neuromuscul Disord. 2014;24:347–52.
Mazzone E, Bianco F, Main M, et al. Six minute walk test in type III spinal muscular atrophy: a 12 month longitudinal study. Neuromuscul Disord. 2013;23:624–8.
Seferian AM, Moraux A, Canal A, et al. Upper limb evaluation and one-year follow up of non-ambulant patients with spinal muscular atrophy: an observational multicenter trial. PLoS ONE. 2015;10: e0121799.
Sivo S, Mazzone E, Antonaci L, et al. Upper limb module in non-ambulant patients with spinal muscular atrophy: 12 month changes. Neuromuscul Disord. 2015;25:212–5.
Montes J, McDermott MP, Mirek E, et al. Ambulatory function in spinal muscular atrophy: age-related patterns of progression. PLoS ONE. 2018;13: e0199657.
Piepers S, Van Den Berg LH, Brugman F, et al. A natural history study of late onset spinal muscular atrophy types 3b and 4. J Neurol. 2008;255:1400–4.
Kaufmann P, McDermott MP, Darras BT, et al. Observational study of spinal muscular atrophy type 2 and 3: functional outcomes over 1 year. Arch Neurol. 2011;68:779–86.
Wijngaarde CA, Stam M, Otto LAM, et al. Population-based analysis of survival in spinal muscular atrophy. Neurology. 2020;94:E1634–44.
Belter L, Cruz R, Jarecki J. Health utility index scores in treated and untreated patients with spinal muscular atrophy: findings from the 2019 Cure SMA Community Update Survey. Neurology. 2020;94(15 Suppl):4564.
Bermudez CA, Frank S, Kolb SJ, et al. Quality of life in adults with spinal muscular atrophy. Neurology. 2020;94(15 Suppl):2716.
Bertini E, Dessaud E, Mercuri E, et al. Safety and efficacy of olesoxime in patients with type 2 or non-ambulatory type 3 spinal muscular atrophy: a randomised, double-blind, placebo-controlled phase 2 trial. Lancet Neurol. 2017;16:513–22.
Binz C, Schreiber-Katz O, Kumpe M, et al. An observational cohort study on impact, dimensions and outcome of perceived fatigue in adult 5q-spinal muscular atrophy patients receiving nusinersen treatment. J Neurol. 2021;268:950–62.
Swoboda KJ, Scott CB, Crawford TO, et al. SMA CARNI-VAL trial part I: double-blind, randomized, placebo-controlled trial of l-carnitine and valproic acid in spinal muscular atrophy. PLoS ONE. 2010;5: e12140.
Kissel JT, Scott CB, Reyna SP, et al. SMA CARNI-VAL TRIAL PART II: a prospective, single-armed trial of l-carnitine and valproic acid in ambulatory children with spinal muscular atrophy. PLoS ONE. 2011;6: e21296.
Johnson N, Paradis AD, Montes J, Krasinski DC. Impact of caregiver experience and HRQOL in later-onset spinal muscular atrophy (SMA): results from the phase 3 CHERISH trial. Value Health Reg Issues. 2019;19(Suppl S):S76.
Johnson NB, Paradis AD, Naoshy S, Wong J, Montes J, Krasinski DC. Evaluation of nusinersen on impact of caregiver experience and HRQOL in later-onset spinal muscular atrophy (SMA): results from the phase 3 CHERISH trial. Neurology. 2020;94(15 Suppl):1429.
Chiriboga CA, Swoboda KJ, Darras BT, et al. Results from a phase 1 study of nusinersen (ISIS-SMN(Rx)) in children with spinal muscular atrophy. Neurology. 2016;86:890–7.
Kirschner J, Swoboda KJ, Mercuri E, et al. Nusinersen experience in individuals with spinal muscular atrophy type III: a case series. J Neuromuscul Dis. 2018;5(Suppl 1):S366.
Hernandez-Rojo Claverie I, Rodríguez Álvarez-Cienfuegos J, Monton Alvarez F, Díez JA, Rodríguez CF. Impact of the disease on quality of life in patients with spinal muscular atrophy. Eur J Neurol. 2020;27(Suppl 1):872.
Klug C, Schreiber-Katz C, Thiele S, et al. Disease burden of spinal muscular atrophy in Germany. Orphanet J Rare Dis. 2016;11:58.
Landfeldt E, Edström J, Sejersen T, Tulinius M, Lochmüller H, Kirschner J. Quality of life of patients with spinal muscular atrophy: a systematic review. Eur J Paediatr Neurol. 2019;23:347–56.
Lloyd AJ, Thompson R, Gallop K, Teynor M. Estimation of the quality of life benefits associated with treatment for spinal muscular atrophy. Clinicoecon Outcomes Res. 2019;11:615–22.
Lloyd A, Gallop K, Thompson R, Vaidya S, Teynor M. Estimation of the health-related quality of life benefits of treatment for spinal muscular atropy (SMA). Value Health. 2017;20:A559.
López-Bastida J, Peña-Longobardo LM, Arando-Reneo I, Tizzano E, Sefton M, Oliva-Moreno J. Social/economic costs and health-related quality of life in patients with spinal muscular atrophy (SMA) in Spain. Orphanet J Rare Dis. 2017;12:141.
Love D, Hicks R, Wei Y, Zapata Aldana E, Almobarak S, Campbell C. Utility based health related quality of life in children and adolescents with spinal muscular atrophy. Neuromuscul Disord. 2019;29(Suppl 1):S130.
Malone D, Dean R, Miller B, et al. ND2 Cost-utility analysis of single dose gene-replacement therapy for spinal muscular atrophy type 1 compared to chronic nusinersen treatment. Value Health. 2019;22(Suppl 2):S42–3.
Malone DC, Dean R, Arjunji R, et al. Cost-effectiveness analysis of using onasemnogene abeparvocec (AVXS-101) in spinal muscular atrophy type 1 patients. J Mark Access Health Policy. 2019;7:1601484.
Montes J, Krasinski D, Foster R, et al. Impact of continued nusinersin treatment on caregiver experience and health-related quality of life in later-onset SMA: results from the SHINE study. Neuromuscul Disord. 2020;30(Suppl 1):S125.
Strauss KA, Carson VJ, Brigatti KW, et al. Preliminary safety and tolerability of a novel subcutaneous intrathecal catheter system for repeated outpatient dosing of nusinersen to children and adults with spinal muscular atrophy. J Pediatr Orthop. 2018;38:e610–7.
Thokala P, Stevenson M, Kumar VM, Ren S, Ellis AG, Chapman RH. Cost effectiveness of nusinersen for patients with infantile-onset spinal muscular atrophy in US. Cost Eff Resour Alloc. 2020;18:41.
Thompson R, Vaidya S, Teynor M. The utility of different approaches to developing health utilities data in childhood rare diseases-a case study in spinal muscular atrophy (SMA). Value Health. 2017;20:A725–6.
Wadman RI, van der Pol WL, Bosboom WM, et al. Drug treatment for spinal muscular atrophy types II and III. Cochrane Database Syst Rev. 2020;1:CD006282.
Weaver MS, Hanna R, Hetzel S, et al. A prospective, crossover survey study of child- and proxy-reported quality of life according to spinal muscular atrophy type and medical interventions. J Child Neurol. 2020;35:322–30.
Zuluaga-Sanchez S, Teynor M, Knight C, et al. Cost effectiveness of nusinersen in the treatment of patients with infantile-onset and later-onset spinal muscular atrophy in Sweden. Pharmacoeconomics. 2019;37:845–65.
Zuluaga S, Knight C, Thompson R, Teynor M. Adequately reflecting the clinical benefits in rare disease economic modeling using SMA type I as a case study. Value Health. 2017;20:A722.
Chen T-H, Chang J-G, Yang Y-H, et al. Randomized, double-blind, placebo-controlled trial of hydroxyurea in spinal muscular atrophy. Neurology. 2010;75:2190–7.
Chiriboga CA, Marra J, LaMarca NM, et al. Lack of effect on ambulation of dalfampridine-ER (4-AP) treatment in adult SMA patients. Neuromuscul Disord. 2020;30:693–700.
Darras BT, Chiriboga CA, Iannaccone ST, et al. Nusinersen in later-onset spinal muscular atrophy: long-term results from the phase 1/2 studies. Neurology. 2019;92:e2492–506.
Finkel RS, Chiriboga CA, Vajsar J, et al. Treatment of infantile-onset spinal muscular atrophy with nusinersen: a phase 2, open-label, dose-escalation study. Lancet. 2016;388:3017–26.
Cytokinetics. A study of CK-2127107 in patients with spinal muscular atrophy. Clinicaltrials.gov; 2020. https://clinicaltrials.gov/ct2/show/study/NCT02644668. Accessed 6 June 2021.
Shieh PB, Acsadi G, Mueller-Felber W, et al. Safety and efficacy of nusinersen in infants/children with spinal muscular atrophy (SMA): part 1 of the phase 2 EMBRACE study. Can J Neurol Sci. 2018;45(Suppl 2):S13.
Baranello G, Servais L, Day JW, et al. FIREFISH part 1: RG7916 significantly increases SMN protein in SMA type 1 babies. Acta Myol. 2018;37:61.
Frongia A, De Benito D, Alarcon-Cornejo M, et al. Salbutamol treatment in type 2 SMA patients: 18 months assessment. J Neuromuscul Dis. 2018;5(Suppl 1):S371–2.
Chiriboga C, Mercuri E, Fischer D, et al. PD and safety data from JEWELFISH, a study of RG7916 in SMA patients previously enrolled in a SMN2-splicing modifier study. J Neuromuscul Dis. 2018;5(Suppl 1):S356–7.
Kirschner J, Schorling D, Hauschke D, et al. Somatropin treatment of spinal muscular atrophy: a placebo-controlled, double-blind crossover pilot study. Neuromuscul Disord. 2014;24:134–42.
Krosschell KJ, Kissel JT, Townsend EL, et al. Clinical trial of l-Carnitine and valproic acid in spinal muscular atrophy type I. Muscle Nerve. 2018;57:193–9.
Deconinck N, Born A, Baranello G, et al. Branaplam in type 1 spinal muscular atrophy: respiratory support and feeding. J Neuromuscul Dis. 2018;5(Suppl 1):S361–2.
AveXis, Inc. 31 DEC 2019 Efficacy update Zolgensma®, onasemnogene abeparvovec. Bannockburn: AveXis, Inc.; 2019.
De Vivo DC, Bertini E, Swoboda KJ, et al. Nusinersen initiated in infants during the presymptomatic stage of spinal muscular atrophy: interim efficacy and safety results from the Phase 2 NURTURE study. Neuromuscul Disord. 2019;29:842–56.
De Vivo DC, Topaloglu H, Swoboda KJ, et al. Nusinersen in infants who initiate treatment in a presymptomatic stage of spinal muscular atrophy (SMA): interim efficacy and safety results from the phase 2 NURTURE study. Neurology. 2019;(15 Suppl):S25.001.
Muntoni F, Buchbjerg J, Bertini E, et al. A long-term, open-label follow-up study of olesoxime in patients with type 2 or non-ambulatory type 3 spinal muscular atrophy who participated in a placebo-controlled phase 2 trial. Neurology. 2018;90(15 Suppl):S46.002.
Russman BS, Iannaccone ST, Samaha FJ. A phase 1 trial of riluzole in spinal muscular atrophy. Arch Neurol. 2003;60:1601–3.
Finkel R, Castro D, Farrar MA, et al. Longer-term assessment of nusinersen safety/efficacy in infantile-onset spinal muscular atrophy: interim analysis of SHINE. J Neuromuscul Dis. 2018;5(Suppl 1):S377.
AveXis, Inc. SPR1NT 31 December 2019 data cut. Bannockburn: AveXis, Inc.; 2019.
Al-Zaidy S, Pickard AS, Kotha K, et al. Health outcomes in spinal muscular atrophy type 1 following AVXS-101 gene replacement therapy. Pediatr Pulmonol. 2019;54:179–85.
Mendell J, Al-Zaidy SA, Shell R, et al. AVXS-101 phase 1 gene therapy clinical trial in SMA type 1: event free survival and achievement of developmental milestones. Neurology. 2017;88(16 Suppl):CT.003.
AveXis, Inc. STR1VE-EU 31 December 2019 data cut. Bannockburn: AveXis, Inc.; 2020.
AveXis, Inc. STR1VE 31 December 2019 data cut. Bannockburn: AveXis, Inc.; 2019.
AveXis, Inc. STRONG (102) 31 December 2019 data cut. Bannockburn: AveXis, Inc.; 2019.
Mercuri E, Baranello G, Kirschner J, et al. Update from SUNFISH part 1: safety, tolerability and PK/PD from the dose-finding study, including exploratory efficacy data in patients with type 2 or 3 spinal muscular atrophy (SMA) treated with risdiplam. Neurology. 2019;92(15 Suppl):S25.007.
Swoboda KJ, Scott CB, Reyna SP, et al. Phase II open label study of valproic acid in spinal muscular atrophy. PLoS ONE. 2009;4: e5268.
Tiziano FSD, Lomastro R, Abiusi E, et al. Longitudinal evaluation of SMN levels as biomarker for spinal muscular atrophy: results of a phase IIb double-blind study of salbutamol. J Med Genet. 2019;56:293–300.
Groen E, Talbot K, Gillingwater T. Advances in therapy for spinal muscular atrophy: promises and challenges. Nat Rev Neurol. 2018;14:214–24.
Ali I, Gilchrist FJ, Carroll WD, et al. Healthcare utilisation in children with SMA type 1 treated with nusinersen: a single centre retrospective review. BMJ Paediatr Open. 2019;3: e000572.
Armstrong EP, Malone DC, Yeh W-S, Dahl GJ, Lee RL, Sicignano N. The economic burden of spinal muscular atrophy. J Med Econ. 2016;19:822–6.
Cardenas J, Menier M, Heitzer MD, Sproule DM. High healthcare resource use in hospitalized patients with a diagnosis of spinal muscular atrophy type 1 (SMA1): retrospective analysis of the Kids’ Inpatient Database (KID). Pharmacoecon Open. 2019;3:205–13.
Chambers GM, Setttumba SN, Carey KA, et al. Prenusinersen economic and health-related quality of life burden of spinal muscular atrophy. Neurology. 2020;95:e1-10.
Chen G, Sharif B, Gerber B, et al. A population-based study examining the epidemiologic burden, healthcare resource utilization and costs of spinal muscular atrophy in Alberta, Canada. Neuromuscul Disord. 2020;30(Suppl 1):S101.
Dabbous O, Seda J, Sproule DM. Economic burden of infant-onset (type 1) spinal muscular atrophy: a retrospective claims database analysis. Value Health. 2018;21(Suppl 1):S251.
Darbà J. Direct medical costs of spinal muscular atrophy in the Catalonia Region: a population-based analysis. Clin Drug Investig. 2020;40:335–41.
Droege M, Sproule D, Arjunji R, Gauthier-Loiselle M, Cloutier M, Dabbous O. Economic burden of spinal muscular atrophy in the United States: a contemporary assessment. J Med Econ. 2020;23:70–9.
Droege M, Dabbous O, Arjunji R, et al. Burden of illness of spinal muscular atrophy: an update. Value Health Reg Issues. 2020;22(Suppl):S76–7.
Goble J, Dai D, Boulos F, Weng A, Johnson K. The economic burden of spinal muscular atrophy patients in a commercially insured population in the United States. J Manag Care Spec Pharm. 2018;24(10-a Suppl):S49.
Hall E, Wells W, Teynor M, et al. Healthcare resource utilization and costs of spinal muscular atrophy care in the US Medicaid population. J Manag Care Spec Pharm. 2017;23(10-a Suppl):S50–1.
Koch SJ, Arego DE, Bowser B. Outpatient rehabilitation for chronic neuromuscular diseases. Am J Phys Med. 1986;65:245–57.
Kockaya G, Ergin GO, Çalışkan Z. Annual cost of treatment of spinal muscular atrophy patients in Turkey. Value Health. 2019;22(Suppl 3):S849–50.
Lee M Jr, França UL, Graham RJ, McManus ML. Pre-nusinersen hospitalization costs of children with spinal muscular atrophy. Pediatr Neurol. 2019;92:3–5.
McMillan H, Gerber B, Cowling T, et al. Disease and treatment burden of spinal muscular atrophy (SMA) on patients and caregivers in Canada. Neuromuscul Disord. 2020;30(Suppl):S100–1.
López-Bastida J, Peña-Longobardo LM, Aranda-Reneo I, et al. The economic impact and health-related quality of life of spinal muscular atrophy (SMA). An analysis across three European countries. Value Health. 2019;22(Suppl 3):S848–9.
Peña-Longobardo LM, Aranda-Reneo I, Oliva-Moreno J, et al. The economic impact and health-related quality of life of spinal muscular atrophy. An analysis across Europe. Int J Environ Res Public Health. 2020;17:5640.
Starner C, Gleason P. Spinal muscular atrophy: an integrated medical and pharmacy claims analysis of nusinersen uptake and gene therapy forecast among 15 million commercially insured. J Manag Care Spec Pharm. 2019;25(3-a Suppl):S54.
Arjunji R, Zhou J, Patel A, et al. Cost-effectiveness analysis of newborn screening for spinal muscular atrophy in the United States. Value Health Reg Issues. 2020;22(Suppl):S75.
Chen H, Hutton DW, Lavieri MS, et al. Cost-effectiveness analysis of newborn screening and treatment for spinal muscular atrophy. Value Health. 2020;23(Suppl):S2.
Connock M, Andronis L, Auguste P, Dussart C, Armoiry X. Will the US $5 million onasemnogene abeparvovec treatment for spinal muscular atrophy represent ‘value for money’ for the NHS? A rapid inquiry into suggestions that it may be cost-effective. Expert Opin Biol Ther. 2020;20:823–7.
Dabbous ON, Dean R, Arjunji R, Sproule DM, Feltner DE, Malone DC. Cost-effectiveness and budget impact of onasemnogene abeparvovec for spinal muscular atrophy type 1: post-hoc analysis of a model developed by ICER. Value Health. 2019;22(Suppl 3):S850.
Dean R, Miller B, Arjunji R, et al. Cost-utility analysis of single dose gene-replacement therapy for spinal muscular atrophy type 1 compared to chronic nusinersen treatment in Japan. Value Health. 2020;23(Suppl 1):S239.
Jalali A, Rothwell E, Botkin JR, Anderson RA, Butterfield RJ, Nelson RE. Cost-effectiveness of nusinersen and universal newborn screening for spinal muscular atrophy. J Pediatr. 2020;227:274-80.e2.
Thokala P, Stevenson M, Kumar VM, et al. Cost-effectiveness of nusinersen and onasemnogene abeparvovec for infantile-onset spinal muscular atrophy (type I SMA) in the US. Value Health. 2019;22(Suppl 2):S337–8.
Zuluaga Sanchez S, Purser M, Mader G, et al. Improved quality of life and life-years in patients with infantile-onset SMA following treatment with nusinersen. Value Health. 2019;22(Suppl 2):S337.
Zuluaga Sanchez S, Purser M, Mader G, et al. Improved quality of life for patients and caregivers among patients with later-onset SMA following treatment with nusinersen. Value Health. 2019;22(Suppl 2):S338.
Scottish Medicines Consortium. Nusinersen 12 mg solution for injection (Spinraza®) [SMC No 1318/18]. 2018. https://www.scottishmedicines.org.uk/media/3415/nusinersen-spinraza-final-april-2018-for-website.pdf. Accessed 6 June 2021.
Canadian Agency for Drugs and Technologies in Health (CADTH). CADTH Canadian Drug Expert Committee Recommendation—Nusinersen (Spinraza). Mississauga; Biogen Canada Inc.; 2017.
Agency for the Quality and Accreditation in Health Care and Social Welfare. Nusinersen (Spinraza) in the treatment of patients with spinal muscular atrophy (SMA) [Nusinersen (Spinraza) u liječenju bolesnika sa spinalnom mišićnom atrofijom (SMA)]. 2017. http://aaz.hr/sites/default/files/Nusinersen_Spinraza_Hitno_izvijesce_srpanj_2017_.pdf. Accessed 6 June 2021.
Swedish Dental and Pharmaceutical Benefits Agency. Spinraza (nusinersen). 2017.
National Centre for Pharmacoeconomics. Cost-effectiveness of nusinersen (Spinraza) for the treatment of 5q spinal muscular atrophy (SMA). 2017. http://www.ncpe.ie/wp-content/uploads/2017/08/Summary-Nusinersen.pdf. Accessed 6 June 2021.
Institute for Clinical and Economic Review. Spinraza® and Zolgensma® for spinal muscular atrophy: effectiveness and value. 2020. https://icer.org/wp-content/uploads/2020/10/ICER_SMA_Final_Evidence_Report_052419.pdf. Accessed 6 June 2021.
Dabbous O, Reyna S, Feltner D, et al. Value of onasemnogene abeparvovec in spinal muscular atrophy type 1: improvements in motor function, ventilation-free survival, and hospitalizations. Neuromuscul Disord. 2020;30(Suppl 1):S123.
Dangouloff T, Servais L, Hiligsmann M. Systematic literature review of the economic burden and economic evaluations in spinal muscular atrophy. Neuromuscul Disord. 2020;30(Suppl 1):S101–2.
Darbà J, Marsà A. Patient characteristics and hospitalisation costs of spinal muscular atrophy in Spain: a retrospective multicentre database analysis. BMJ Open. 2019;9:1–6.
Servais L, De Vivo DC, Kirschner J, et al. Newborn screening for spinal muscular atrophy in the United States: early findings from the RESTORE registry. In: Presented at MDA Clinical and Scientific Conference 2021; March 15–18, 2021.
Aballéa S, Thokagevistk K, Velikanova R, et al. Health economic evaluation of gene replacement therapies: methodological issues and recommendations. J Mark Access Health Policy. 2020;8:1822666.
National Institute for Health and Care Excellence (NICE). Onasemnogene abeparvovec for treating spinal muscular atrophy. Highly specialised technologies guidance. HST15. July 7, 2021. https://www.nice.org.uk/guidance/hst15. Accessed 12 Oct 2021.
Acsadi G, Crawford TO, Müller-Felber W, et al. Safety and efficacy of nusinersen in spinal muscular atrophy: the EMBRACE study. Muscle Nerve. 2021;63:668–77.
Servais L, De Vivo DC, Kirschner J, et al. Routine practices in use of onasemnogene abeparvovec in older patients with spinal muscular atrophy: early findings from RESTORE. In: Presented at MDA Clinical and Scientific Conference 2021; March 15–18, 2021.
Bischof M, Lorenzi M, Lee J, Druyts E, Balijepalli C, Dabbous O. Matching-adjusted indirect treatment comparison of onasemnogene abeparvovec and nusinersen for the treatment of symptomatic patients with spinal muscular atrophy type 1. Curr Med Res Opin. 2021;37:1719–30.
Mercuri E, Deconinck N, Mazzone ES, et al. Safety and efficacy of once-daily risdiplam in type 2 and non-ambulant type 3 spinal muscular atrophy (SUNFISH part 2): a phase 3, double-blind, randomised, placebo-controlled trial. Lancet Neurol. 2022;21:42–52.
Acknowledgements
The authors thank Roksana Ghanbariamin, Aidai Kozubekova, and Yi Zhong, employees of Analysis Group, Inc., for their support in conducting literature review, data extraction, and analysis.
Funding
This analysis was funded by Novartis Gene Therapies, Inc. Novartis Gene Therapies, Inc., also funded the journal’s Rapid Service and Open Access fees.
Medical Writing and Editorial Assistance
Medical writing assistance and editorial support were provided by Leonard Lionnet, PhD, of Kay Square Scientific, LLC, Newtown Square, PA, USA. This support was funded by Novartis Gene Therapies, Inc., Bannockburn, IL, USA.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
Min Yang and Su Zhang contributed to all aspects of this study, including study design, data extraction, analysis, visualization, and critical review, editing, and approval of the draft manuscript. Satoru Tanaka, Omar Dabbous, and Walter Toro participated in conception and design of the study, interpretation of data, and critical review, revision, and approval of the draft manuscript. Hiroyuki Awano participated in the critical review, editing, and approval of the draft manuscript. Ataru Igarashi participated in the critical review, editing, and approval of the draft manuscript. All authors have reviewed and approved the final version of this manuscript for submission.
Prior Presentation
This manuscript contains content from an oral presentation that was given at the 66th Annual Meeting of the Japan Society of Human Genetics and the 28th Annual Meeting of the Japanese Society for Gene Diagnosis and Therapy-Joint Conference 2021, held in Yokohama, Japan, on October 13–16, 2021.
Disclosures
Min Yang and Su Zhang are employees of the Analysis Group, Inc., and consultants to Novartis Gene Therapies, Inc. Satoru Tanaka is an employee of Novartis Pharma K.K. Walter Toro and Omar Dabbous are employees of Novartis Gene Therapies, Inc., and own stock options. Hiroyuki Awano reports payment for lectures from Novartis Pharma Japan Inc., and Biogen Japan Ltd. Ataru Igarashi reports personal fees from Novartis Pharma Japan Inc., during the conduct of the study. Ataru Igarashi also reports grants and other from Gilead Sciences KK.; grants from Intuitive Surgical GK., Boston Scientific Japan Inc., Beckton Dickinson and Company, and Milliman Inc.; grants and personal fees from Pfizer Japan Inc.; personal fees and other from Terumo Corporation, personal fees from Chugai Pharmaceuticals Inc., Sanofi Japan Inc., Takeda Pharmaceutical Inc., Nippon Boehringer Ingelheim Inc., Ono Pharmaceutical Inc., Novartis Pharma Japan Inc., Eisai Inc., AbbVie GK, Sumitomo Dainippon Pharma Inc., AYUMI Pharmaceutical Inc., Medilead Inc., Astellas Pharma Inc., Novo Nordisk Japan Inc., and Taiho Pharmaceutical Inc., outside the submitted work; and other from Fuji Film Inc., and CSL Behring Japan Inc.
Compliance with Ethics Guidelines
This article is based upon previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Yang, M., Awano, H., Tanaka, S. et al. Systematic Literature Review of Clinical and Economic Evidence for Spinal Muscular Atrophy. Adv Ther 39, 1915–1958 (2022). https://doi.org/10.1007/s12325-022-02089-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-022-02089-2