
Abstract
Background
Intrahospital transport is associated with a high rate of complications. Investigations of this problem using neuromonitoring remain scarce.
Methods
This is a monocentric, prospective observational study. Patients with severe brain diseases and intracranial pressure (ICP) monitoring were included. Continuous monitoring of ICP, cerebral perfusion pressure (CPP), oxygen saturation (SpO2), heart rate, and mean arterial pressure was measured during seven different periods of intrahospital transport (baseline for 30 min, I = preparation, II = transport I, III = CT scan, IV = transport II, V = postprocessing, and follow-up for another 30 min). All complications were documented.
Results
Between July 2013 and December 2013, a total number of 56 intrahospital transports of 43 patients were performed from ICU to CT. Data recording was incomplete in six cases. Fifty transports have been taken into account for statistical analysis. Forty-two percent were emergency transports. Mean duration of the procedure was 17′ (preparation), 6′ (transport I), 9′ (CT scan), 6′ (transport II), and 15′ (postprocessing), respectively. Mean ICP at baseline was 8.53 mmHg. Comparing all periods of intrahospital transport and the follow-up period to the baseline showed a significant increase of ICP only during CT scan (15.83 mmHg, p < 0.01), not during the transport to and from the radiology department. An overall complication rate of 36 % (n = 18) was observed. In 26 % (n = 13), additional ICP therapy was necessary due to an elevation of ICP above 20 mmHg.
Conclusion
There is a considerable rate of complications during intrahospital transport of critically ill patients with severe brain diseases, with a significant increase of ICP during transport and CT scan. In one-fifth of all patients, additional therapy was necessary. From our point of view, transport of critically ill patients should only be performed by trained staff and under monitoring of ICP and CPP.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Increased intracranial pressure (ICP) has been observed during several procedures in the management of critical ill patients with severe brain diseases, such as tracheostomy or prone positioning [1–3]. Transport of critically ill patients is a daily routine in intensive care units. However, intrahospital transport is associated with an increased risk for patients [4–6]. Studies report incidents in 4.2–70 % of critically ill patients during intrahospital transport [7]. Possible complications known to occur include airway management issues, extravasation, infiltration or displacement of peripheral arterial or venous lines, and cardiovascular alterations [8]. In addition, therapeutic intervention possibilities are limited during such transports compared to those of an intensive care unit with its infrastructural setting. Patients of a neurological/neurosurgical intensive care unit differ from those of a surgical- or internal medicine-dominated critical care unit in many factors, especially in the higher number of patient transports involved in neuroradiologic diagnostic procedures [9]. Cranial computer tomography (cCT) is a frequently performed and repeated procedure, especially in patients with severe cerebral diseases, and is required for diagnosis and decision-making during the critical phases of the underlying condition.
Besides the general risk factors mentioned above, the transport could per se determine an increase in the ICP value (e.g., through respiratory complications leading to an increased pCO2 and a consecutive ICP rise). ICP could increase due to the transport itself or could be evoked during placement of the patient on the CT table. Up until now, only a few studies have investigated complications of intrahospital transport of patients of a neurointensive care unit, especially with regard to the development of ICP and cerebral perfusion pressure (CPP) [9–12].
Methods
Study Design and Setting
We performed a monocentric, prospective observational study on the 12 beds in our neurointensive care unit (NICU) in a tertiary hospital in Germany (Department of Neurology and Department of Neurosurgery at Klinikum Kassel) between July 2013 and December 2013.
Study Population
Cases were considered eligible for analysis if patients had severe intracranial pathologies, presence of ICP monitoring, and need of intrahospital transport (CT scan). [We also perform MRI investigation; however, patients with ICP devices are not suited to undergo MRI, and therefore such patients were not included in the study.] ICP monitoring was performed due to the necessity of monitoring patients with reduced consciousness. Indication for monitoring ICP and indication for intrahospital transport was made by the senior neurointensivist on duty, and this study had no influence on this decision. All patients were ventilated mechanically in a pressure-controlled mode (BiPAP mode, EVITA®, Dräger, Lübeck, Germany). A team of at least two staff members of the NICU, including one physician, made intrahospital transport. After preparing the patient for transport, the ventilator was switched to a mobile device by the physician (OXYLOG® 3000 plus, Dräger, Lübeck, Germany). The ventilation parameters were adapted, and FiO2 was elevated to 1 for preoxygenation (Phase I, “Preparation”). The team always carried an emergency backpack with them including relevant drugs and emergency tools such as resuscitator bag, laryngoscope, or a manual suction pump. Both the NICU and the CT suite are located on the ground floor of our hospital, but in neighboring buildings. The patients were transported in their own beds. Motor vehicles were not used (Phases II and IV “Transport”). Repositioning of the patients was necessary only to transfer the patient onto the CT table, with additional help from the radiological staff members (Phase III “CT scan”).
Variables and Measurements
Due to treatment algorithms for certain diseases in the Department of Neurology and the Department of Neurosurgery, CT scans are scheduled for certain days. For instance, all patients receive CT scan 6 h after intradural surgery. These transports were labeled “elective.” Transports due to an acute clinical deterioration that was not predictable, such as occurrence of an anisocoria, were categorized as “emergency” transports. Continuous monitoring (minute-to-minute measurement) of ICP, CPP, oxygen saturation (SpO2), and mean arterial pressure (MAP) was performed in all patients. Data recording started 30 min before the procedure and was continued for another 30 min after the end of the procedure (Infinity® Delta, Dräger, Lübeck, Germany). ICP measurement was performed using intraparenchymal cerebral pressure measurement (NEUROVENT-P, Raumedic AG, Münchberg, Germany). The minute-to-minute individual measurements were compiled as mean values for the individual phases of the transport (I = preparation, II = transport to the radiology department, III = CT scan, IV = transport back to our critical care unit, and V = post-transport monitoring). Primary endpoints were change in ICP and CPP in comparison with the initial baseline-levels. Secondarily evaluated parameters were MAP, SpO2, and descriptive data (the presence of external ventricular drainage and/or decompressive hemicraniectomy, need for additional ICP therapy during transport). Depth of sedation was measured before each transport using the Ramsay Score (RS). Possible complications occurring during transport, such as respiratory disturbances or displacements of peripheral catheters, were documented separately.
Ethical Considerations
The study was approved by the local ethics committee review at Philipps University of Marburg (ID 67/13). We have prepared our publication according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement [13].
Statistical Methods
The median values were calculated for ICP, CPP, and MAP in all five phases of the transport and subsequently compared to baseline. To detect differences between the phases, we used pairwise Wilcoxon Test with Bonferroni–Holm correction for multiple testing. A probability value of p < 0.05 was considered significant. The analysis was done with R (version 2.14.1, The R Foundation for statistical computing).
Results
Between July 2013 and December 2013, a total number of 367 patients were treated on our NICU. Fifty-two of these required ICP monitoring. We collected data prospectively from 56 intrahospital transports involving 43 patients (2 transports in 5 patients, 3 transports in 1 patient, 4 transports in 2 patients). The mean age was 58 years, with a range from 23 to 76 years [female n = 28 (56 %), male n = 22 (44 %)].
Descriptive data of the patients are shown in Table 1. Data recording was incomplete in six cases due to technical hazards such as failure of the recording system. Fifty transports have been taken into account for statistical analysis. Forty-two percent were emergency transports.
Outcome Data
Mean duration of the procedure was 17′ (I = preparation), 6′ (II = transport I), 9′ (III = CT scan), 6′ (IV = transport II), and 15′ (V = postprocessing), respectively. The process of the procedure is illustrated in Fig. 1. Mean ICP before beginning the transport was 8.53 mmHg. Comparing all five phases of intrahospital transport and the follow-up period to baseline revealed a significant increase of ICP only during CT scan (15.83 mmHg, p < 0.01) (Fig. 2).

Flow-chart study protocol

Boxplot development ICP
Corresponding to changes of ICP, there was a significant decrease of CPP compared to baseline (82 mmHg) during CT scan (72 mmHg, p < 0.01) (Fig. 3). Development of MAP is illustrated in Fig. 4. SpO2 did not show any significant changes compared to the baseline value of 99 %.

Boxplot development CPP

Boxplot development mean arterial pressure (MAP)
Complications
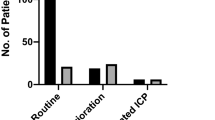
There were two pulmonary complications that exceeded the upper ventilation pressure of 30 mbar. Three additional patients were agitated, with the need for deepening analgosedation in order to perform the CT scan. Forty-two percent (n = 21) were emergency transports. Complications were observed in 36 % (n = 18). Unexpectedly, the complication rate was lower in the “emergency” group (33 %, n = 7/21) than in the “elective” group (38 %, n = 11/29). This difference was not statistically significant. In 13 cases (26 %), ICP therapy with osmotherapy or additional analgosedation was necessary. There is no statistically significant difference between patients with and without hemicraniectomy in terms of additional ICP therapy during the transport. All of these patients had a RS of 5 or 6 before transport. This is not surprising since all patients in the critical phase of raised ICP are kept under sedation on our ICU (64 % of all patients had a RS of 5 or 6). In case of raised ICP, we checked the measuring system to exclude inaccurate measurements (due to replugging the cables for the transport, incorrect values sometimes occur). In cases of truly elevated ICP (>20 mmHg), we started treatment immediately.
There were no catheter dislocations or severe hemodynamic or respiratory complications in any of the 50 transports.
Discussion
We investigated ICP and CPP development during intrahospital transport of critically ill patients. The wide range of patients with different underlying diseases represents the typical collective of patients treated on our neurosurgical and neurological ICU. Our results show a significant rise of ICP with a corresponding drop of CPP during the phase of CT scan compared to the baseline period. The overall rate of complications during intrahospital transport was 32 % and was, therefore, substantially elevated. This rate of general complications is comparable to that seen in other studies [8, 14, 15]. There are several recommendations for lowering patient risk during intrahospital transport [7, 16, 17]. However, these studies and recommendations do not focus on neurological intensive care patients. We observed two kinds of complications in our study: (1) extracerebral pulmonary complications exceeding the upper ventilation pressure were very low; and (2) a group of patients were anxious, restless, and agitated. Both complications were easily managed by deepening analgosedation. In some patients, only increased sedation was necessary because they were agitated, suggesting that deepening sedation before transport could have prevented this. Therefore, this cannot be regarded as a real critical complication in the narrow sense. Catheter dislocations [18] were not observed in our study.
The number of complications was due to therapy-relevant ICP elevation. It is of note that the mean baseline ICP was very low in our cohort, increasing from 8 to 16 mmHg during CT scan, thus not exceeding the dangerous mean ICP of 20 mmHg. In some cases, however, ICP increased substantially. Furthermore, ICP-reducing therapy was necessary in 13 cases (26 %) of all investigations. We believe that this was due to the transfer of the patient from their own bed to the CT table itself and the fact that a 30°–45° head-up positioning could no longer be maintained during CT scan. Median CPP during CT was 72.25 mmHg with a mean CPP of 75.46 mmHg, respectively. This might lead to the incorrect interpretation that CT scan can be performed without additional endangerment of the patients in any case. However, there was a statistically significant decrease of CPP during the CT scan compared to baseline. Furthermore, the minimum was 41 mmHg in one case, although the majority of patients does not reach a CPP level <60 mmHg during the phase of the CT scan, and the minimum reached is 41.25 mmHg in one case.
ICP fortunately decreased again within a few minutes after the end of the procedure, and this was accompanied with an adequate increase of CPP. Furthermore, the duration of the CT period, including transferring the patients from bed to the CT table and back again after the investigation, was manageable and lasted only for a mean of 9 min.
Whether or not the performed CT scan had immediate clinical consequences was not part of this study. In order to reevaluate the necessity of performed scans, this would have been an interesting aspect to analyze, especially in consideration of the (statistically not significant) higher complication rate in the elective group. This will be taken into account for future studies.
Transport by motor vehicles or use of elevators is not necessary in our hospital. The CT suite can be reached easily within a few minutes. This is only a single-center study, and the conditions for intrahospital transport may differ and even be more complex in other intensive care units. There was no significant increase of mean ICP or decrease of mean CPP during all other investigated periods of intrahospital transport. However, transfer from bed to the CT table is always necessary. This should be done with utmost caution. During CT scan, the patient’s head should be positioned into correct axial alignment. Compression of the jugular veins should be avoided. Even a short-lasting elevation of ICP might harm patients during the critical phases of severe brain diseases. The indication for intrahospital transport should always be critically questioned, and other diagnostic methods such as transcranial ultrasound or a portable CT scan are possible alternatives [19]. In our opinion, a conservative attitude regarding avoidable intrahospital transports for CT scans in critically ill patients is needed. In our clinic, alternative procedures such as transcranial ultrasound, for example, in patients who had undergone hemicraniectomy are increasingly being put to use before CT scans are performed.
Some departments have outsourced intrahospital transport to low-skilled staff and physicians who are not involved in the routine therapy of the patients [20, 21]. In our view, this is a worrying development. With regard to the possible complications, especially ICP elevation and CPP lowering, which often requires a therapeutic intervention, we suggest that critical care unit personnel, who are directly involved in the treatment of the patient, should carry out such transports. In particular, it is plausible that the lack of field-specific personnel resources and the increase in outsourcing of certain activities lead to an increased risk of harming patients.
From our point of view, transport of critically ill patients should be performed only by trained staff and under monitoring of ICP and CPP. In order to further analyze subgroups (hemicraniectomy vs. no hemicraniectomy, young vs. old, etc.), a continuation of the data collection is needed. One may consider prophylactic ICP therapy immediately before CT scan, for example by deepening sedation, but this must be proven by further prospective studies.
References
Roth C, Ferbert A, Deinsberger W, et al. Does prone positioning increase intracranial pressure? A retrospective analysis of patients with acute brain injury and acute respiratory failure. Neurocrit Care. 2014;21:186–91.
Kleffmann J, Pahl R, Deinsberger W, et al. Effect of percutaneous tracheostomy on intracerebral pressure and perfusion pressure in patients with acute cerebral dysfunction (TIP Trial): an observational study. Neurocrit Care. 2012;17:85–9.
Roth C, Stitz H, Kalhout A, et al. Effect of early physiotherapy on intracranial pressure and cerebral perfusion pressure. Neurocrit Care. 2013;18:33–8.
Braman SS, Dunn SM, Amico CA, et al. Complications of intrahospital transport in critically ill patients. Ann Intern Med. 1987;107:469–73.
Bercault N, Wolf M, Runge I, et al. Intrahospital transport of critically ill ventilated patients: a risk factor for ventilator-associated pneumonia—a matched cohort study. Crit Care Med. 2005;33:2471–8.
Papson JPN, Russell KL, Taylor DM. Unexpected events during the intrahospital transport of critically ill patients. Acad Emerg Med. 2007;14:574–7.
Brunsveld-Reinders AH, Arbous MS, Kuiper SG, et al. A comprehensive method to develop a checklist to increase safety of intra-hospital transport of critically ill patients. Crit Care. 2015;19:214.
Schwebel C, Clec’h C, Magne S, et al. Safety of intrahospital transport in ventilated critically ill patients: a multicenter cohort study. Crit Care Med. 2013;41:1919–28.
Kalisch BJ, Kalisch PA, Burns SM, et al. Intrahospital transport of neuro ICU patients. J Neurosci Nurses. 1995;27:69–77.
Picetti E, Antonini MV, Lucchetti MC, et al. Intra-hospital Transport of brain-injured patients: a prospective, observational study. Neurocrit Care. 2013;18:298–304.
Andrews PJ, Piper IR, Dearden NM, et al. Secondary insults during intrahospital transport of head-injured patients. Lancet. 1990;335:327–30.
Swanson EW, Mascitelli J, Stiefel M, et al. Patient transport and brain oxygen in comatose patients. Neurosurgery. 2010;66:925–31.
von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370:1453–7.
Nuckols TK. Reducing the risks of intrahospital transport among critically ill patients. Crit Care Med. 2013;41:2044–5.
Kue R, Brown P, Ness C, et al. Adverse clinical events during intrahospital transport by a specialized team: a preliminary report. Am J Crit Care. 2011;20:153–61 (quiz 162).
Fanara B, Manzon C, Barbot O, et al. Recommendations for the intra-hospital transport of critically ill patients. Crit Care. 2010;14:R87.
Quenot J-P, Milési C, Cravoisy A, et al. Intrahospital transport of critically ill patients (excluding newborns) recommendations of the Société de Réanimation de Langue Française (SRLF), the Société Française d“Anesthésie et de Réanimation (SFAR), and the Société Française de Médecine d”Urgence (SFMU). Ann Intensive Care. 2012;2:1.
Doring BL, Kerr ME, Lovasik DA, et al. Factors that contribute to complications during intrahospital transport of the critically ill. J Neurosci Nurses. 1999;31:80–6.
Gunnarsson T, Theodorsson A, Karlsson P, et al. Mobile computerized tomography scanning in the neurosurgery intensive care unit: increase in patient safety and reduction of staff workload. J Neurosurg. 2000;93:432–6.
Stearley HE. Patients’ outcomes: intrahospital transportation and monitoring of critically ill patients by a specially trained ICU nursing staff. Am J Crit Care. 1998;7:282–7.
Stubbs CR, Crogan KJ, Pierson DJ. Interruption of oxygen therapy during intrahospital transport of non-ICU patients: elimination of a common problem through caregiver education. Respir Care. 1994;39:968–72.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Kleffmann, J., Pahl, R., Deinsberger, W. et al. Intracranial Pressure Changes During Intrahospital Transports of Neurocritically Ill Patients. Neurocrit Care 25, 440–445 (2016). https://doi.org/10.1007/s12028-016-0274-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-016-0274-6