
Abstract
Background
Bedside percutaneous tracheostomy (PT) is very commonly used for patients who require prolonged mechanical ventilation. The effect of tracheostomy on intracranial pressure (ICP) is currently a subject of controversy. The aim of our study is to clarify the relation between PT and its effect on ICP and cerebral perfusion pressure.
Methods
38 patients on our intensive care unit were included prospectively in an observational study. We examined mean values of HF, SpO2, ICP, CPP, and MAP for changes over five different phases of the procedure using paired Mann–Whitney U tests. A p value of <0.05 was considered significant. p values were Bonferroni corrected for multiple testing.
Results
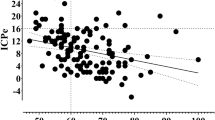
PT was performed on 38 patients (f = 19, m = 19; mean = 56 years). Median ICP before intervention was 9 mmHg. During positioning of the patient, ICP had risen to 14, during bronchoscopy to 16, and during tracheostomy to 18 mmHg, all being significantly higher than baseline level. Monitoring of MAP showed a significant increase to 101 mmHg only during tracheostomy. SpO2 and HF did not show any significant changes. Mean duration of positioning, bronchoscopy and tracheostomy was 19, 10, and 17 min. 8 patients received osmotherapy due to a rise of ICP of more than 30 mmHg.
Conclusion
PT only leads to a significant rise of ICP during the procedure. Nevertheless, therapy of ICP is necessary in some patients. From our point of view, therefore, tracheostomy should only be performed under continuous monitoring of ICP and CPP in patients with severe cerebral dysfunctions and critically elevated ICP.




Similar content being viewed by others

References
Rana S, Pendem S, Pogodzinski S, et al. Tracheostomy in critically ill patients. Mayo Clin Proc. 2005;80:1632–8.
Nieszkowska A, Combes A, Luyt C, et al. Impact of tracheotomy on sedative administration, sedation level, and comfort of mechanically ventilated intensive care unit patients. Crit Care Med. 2005;33:2527–33.
Durbin CG, Perkins MP, Moores LK. Should tracheostomy be performed as early as 72 hours in patients requiring prolonged mechanical ventilation? Respir Care. 2010;55:76–83.
Scales DC, Ferguson ND. Tracheostomy: it’s time to move from art to science. Crit Care Med. 2006;34:3039–40.
Kilner AJ. Another death after percutaneous dilational tracheostomy. Br J Anaesth. 2003;91:925–6.
Rosseland LA, Laake JH, Stubhaug A. Percutaneous dilatational tracheotomy in intensive care unit patients with increased bleeding risk or obesity. A prospective analysis of, procedures. Acta Anaesthesiol Scand. 1000;2011(55):835–41.
Freeman BD, Isabella K, Lin N, et al. A meta-analysis of prospective trials comparing percutaneous and surgical tracheostomy in critically ill patients. Chest. 2000;118:1412–8.
Kocaeli H, Korfali E, Taşkapilioğlu O, et al. Analysis of intracranial pressure changes during early versus late percutaneous tracheostomy in a neuro-intensive care unit. Acta Neurochir (Wien). 2008;150:1263–7. (discussion 1267).
Stocchetti N, Parma A, Songa V, et al. Early translaryngeal tracheostomy in patients with severe brain damage. Intensive Care Med. 2000;26:1101–7.
Imperiale C, Magni G, Favaro R, et al. Intracranial pressure monitoring during percutaneous tracheostomy “Percutwist” in critically ill neurosurgery patients. Anesth Analg. 2009;108:588–92.
Pryor JP, Reilly PM, Shapiro MB. Surgical airway management in the intensive care unit. Crit Care Clin. 2000;16:473–88.
Ciaglia P, Firsching R, Syniec C. Elective percutaneous dilatational tracheostomy. A new simple bedside procedure; preliminary report. Chest. 1985;87:715–9.
Frova G, Quintel M. A new simple method for percutaneous tracheostomy: controlled rotating dilation. A preliminary report. 2002;28(3):299–303.
Terragni PP, Antonelli M, Fumagalli R, et al. Early vs late tracheotomy for prevention of pneumonia in mechanically ventilated adult ICU patients. J Am Med Assoc. 2010;303:1483–9.
Funk GC, Anders S, Breyer MK, et al. Incidence and outcome of weaning from mechanical ventilation according to new categories. Eur Respir. 2010;35:88–94.
Griggs WM, Worthley LI, Gilligan JE, et al. A simple percutaneous tracheostomy technique. Surgery. 1990;170:543–5.
Fantoni A, Ripamonti D. A non-derivative, non-surgical tracheostomy: the translaryngeal method. Intensive Care Med. 1997;23:386–92.
Ng I, Lim J, Wong HB. Effects of head posture on cerebral hemodynamics: its influences on intracranial pressure, cerebral perfusion pressure, and cerebral oxygenation. Neurosurgery. 2004;54:593–8.
Reilly PM, Anderson HL, Sing R, et al. Occult hypercarbia: An unrecognized phenomenon during percutaneous endoscopic tracheostomy. Chest. 1995;107:1760–3.
Peerless JR, Snow N, Likave M, et al. The effect of fiberoptic bronchoscopy on cerebral hemodynamics in patients with severe head injury. Chest. 1995;108:962–5.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kleffmann, J., Pahl, R., Deinsberger, W. et al. Effect of Percutaneous Tracheostomy on Intracerebral Pressure and Perfusion Pressure in Patients with Acute Cerebral Dysfunction (TIP Trial): An Observational Study. Neurocrit Care 17, 85–89 (2012). https://doi.org/10.1007/s12028-012-9709-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-012-9709-x