
Abstract
Background
Ceramic-on-ceramic bearing couples are theoretically attractive in total hip arthroplasty (THA) because of low wear, but concerns regarding ceramic fracture and squeaking have arisen. Improved material properties of newer alumina matrix composite (AMC) materials, known as Delta ceramics, may reduce these risks. In addition, the use of thinner liners and larger femoral heads may be helpful clinically to lower the rate of dislocation. However, limited short-term clinical results are available and intermediate-term effects are unclear.
Questions/purposes
(1) What is the frequency of bearing-related complications (dissociation, fracture, and noise) with ceramic-on-ceramic AMC bearings in cementless THA? (2) What other complications arose in patients treated with these bearings? (3) What are the Harris hip scores (HHS) and survivorship free from reoperation and revision at a minimum of 5 years after cementless THA performed with AMC bearings?
Methods
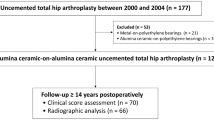
Over a 9-month period in 2009, one surgeon performed 125 THAs, of which 100 (80% of the total) were performed with cementless, AMC bearings. During the period in question, the exclusion criteria for this implant were primary THAs with severe acetabular or femoral bone defect and revision THAs. Of these, 94 hips (95%) in 91 patients were available for analysis at a minimum of 5 years (range, 5–6 years), because five patients (six hips) had died. Mean age at the time of arthroplasty was 55 ± 14 years. Prostheses with an identical design and Biolox® Delta ceramics were used in all patients. Noise was classified into squeaking, clicking, grinding, and popping. Ceramic fracture, dislocation, and any other complications associated with the use of AMC ceramics were also investigated. Clinical evaluation included the modified HHS preoperatively and at each followup. Survivorship free from reoperation and revision was calculated using the Kaplan-Meier method.
Results
Of 91 patients, four developed bearing-related complications, including one with liner dissociation despite initial square seating and three with clicking. No patients had ceramic fractures. A single event of perioperative dislocation occurred in one patient and postoperative periprosthetic fracture occurred in two hips. Mean HHS improved from 56 to 93 points at the final followup (p < 0.001). Survivorship at 5 years free from reoperation and revision was 96.8% and 97.9%, respectively.
Conclusions
Improved material properties combined with the possible use of larger diameter heads make AMC ceramics a promising alternative bearing option with seemingly comparable clinical outcomes reported by others with conventional ceramic bearings. Despite these encouraging results, however, meticulous technical precautions such as square seating and proper impaction in particular should be taken during liner insertion, because we did observe one liner dissociation and several patients with hip noises.
Level of Evidence
Level IV, therapeutic study.
Similar content being viewed by others

Introduction
Since polyethylene wear and osteolysis became recognized as a major problem affecting long-term survivorship of THA, efforts have been made to reduce wear and improve longevity. Although contemporary THAs with highly crosslinked polyethylene (HXLPE) or hard-on-hard bearings offer great hope for reducing wear, the reduction in wear observed in THAs with HXLPE appears to be not quite as dramatic as seen in those with hard-on-hard bearings [19, 32], and those with metal-on-metal bearings have problematic issues such as hypersensitivity and pseudotumors [34].
Alumina ceramic bearings have been reported to reduce wear [14]. Although the third-generation alumina ceramics have been shown to be superior to those with previous generations in terms of material properties and reducing risk of fractures [18], there still remains a number of concerns such as potential for ceramic fracture [13, 21], noise issues [20], fewer intraoperative options and impingement [3], and decreased positional range of error during liner insertion [22]. These limitations of pure alumina characteristics required the development of improved ceramic materials. The alumina matrix composite (AMC) material, Delta ceramics (CeramTec®, Plochingen, Germany), has been reported to increase ceramic strength with fracture toughness over previous pure alumina in the laboratory setting and thus to allow manufacturing thinner acetabular liners and consequent larger heads [1, 4]. Theoretically, these material improvements would be expected to decrease mentioned concerns associated with previous-generation alumina bearings. However, few short-term clinical results have been published [7, 15, 27] and several questions remain regarding longer term clinical outcomes after THAs using Delta ceramic bearings.
Therefore, we investigated: (1) What is the frequency of bearing-related complications (fracture, noise, and dissociation) with ceramic-on-ceramic AMC bearings in cementless THA? (2) What other complications arose in patients treated with these bearings? (3) What are the Harris hip scores (HHS) and survivorship free from reoperation and revision at a minimum of 5 years after cementless THA performed with AMC bearings?
Materials and Methods
The current retrospective study is a case series and we collected the data in a prospective manner. This study was approved by institutional review board and all patients provided informed consent.
Over a 9-month period in 2009, one surgeon (S-YK) performed 125 THAs, of which 100 (80% of the total) were performed with cementless, AMC bearings. During the period in question, the general indications for this implant were all primary THAs without severe acetabular or femoral bone defect and revision THAs were excluded. Of these, 94 hips (94%) in 91 patients were available for analysis at a minimum of 5 years (range, 5–6 years), because five patients (six hips) had died.
There were 47 male and 44 female patients with a mean age of 55 ± 14 years at the time of arthroplasty. The mean body mass index (BMI) was 23 ± 3 kg/m2. The mean followup was 5 ± 0.3 years (range, 5–6 years). The primary diagnosis for THA was osteonecrosis of the femoral head in 47 (50%), hip dysplasia in 16 (17%), primary osteoarthritis in 15 (16%), femoral neck fracture in eight (9%), posttraumatic osteoarthritis in four, ankylosing spondylitis in two, rheumatic arthritis in one, and sequela after pyogenic arthritis in one hip.
Prostheses with an identical design were implanted and so-called fourth-generation ceramics, Biolox® Delta (CeramTec®), without a metallic sleeve were coupled as the bearing surface in all patients (Fig. 1). Because 36-mm-sized femoral heads could be implanted only in cups larger than 50 mm according to the product specifications, the diameter of the femoral head was 32 mm in 19 (20%) and 36 mm in 75 hips (80%). The length of the femoral neck was short in 20 (21%), medium in 70 (75%), and long in four hips (4%). Biolox® Delta inserts have a Morse taper angle of 18.5° and were self-secured into cementless Bencox® Cups (CorenTec®, Cheon-An, Korea). Although the angled conical shape made it difficult to calculate the thickness of the liner, the mean thickness of outer conical fit according to the manufacturer was 3.9 ± 0.53 mm (range, 3.4–5.9 mm). The hemispheric titanium alloy cup was plasma-sprayed with microporous pure titanium with more than 30% porosity. The mean size of the acetabular cup was 53 ± 4 mm (range, 46–62 mm). The femoral component was a cementless Bencox® stem (CorenTec®), a grit-blasted tapered double-wedge stem with a rectangular cross-section.

Photograph demonstrates the Bencox® hip system with the Biolox® Delta ceramic head and liner.
We evaluated questionnaires on the history of ceramic fracture, dislocation, reoperation, and the noise around the hip, which was classified into squeaking, clicking, grinding, and popping [17] at each followup and snapping was excluded through physical examination or ultrasonography. These complications were investigated by routine radiographs as well. The serial radiographs were analyzed regarding component loosening [11, 33], osteolysis [24], periprosthetic fracture [6], and joint infection.
The modified HHS [16] was also evaluated at each followup and survivorship with any reoperation and revision as the endpoint at 5 years was calculated using the Kaplan-Meier method. Statistical analysis was conducted using the SAS (Version 9.3; SAS Institute Inc, Cary, NC, USA). Student’s/paired t-test and chi-square test were used to compare variables. A p value of < 0.05 was considered to be significant.
Results
Of 91 patients, four developed bearing-related complications, including one with liner dissociation and three with hip noises. No patients sustained ceramic fractures. The single liner dissociation without fracture was noted immediately after surgery and was revised with a new acetabular shell, Delta ceramic liner, and head. Three patients (three hips) reported subjective clicking, which was not associated with pain or functional limitation, and no patients reported squeaking. Noise occurred in younger age (p = 0.009), but was not associated with sex (p = 0.583), BMI (p = 0.334), head and cup size (p = 0.565 and p = 0.963, respectively), neck length (p = 0.832), inclination and anteversion angle of the cup (p = 0.338 and p = 0.661, respectively), and final HHS (p = 0.642) (Table 1).
One hip dislocated in a 61-year-old woman 9 days after surgery; after closed reduction, she has not experienced any further dislocations. When an intraoperative femoral fracture was suspected, simultaneous cerclage wiring was performed in seven hips (7%). In addition, postoperative periprosthetic fractures occurred in two hips (2%): one hip with type B2 fracture according to the Vancouver classification system underwent stem revision with an extensively porous-coated stem and plate fixation, whereas the other with Vancouver type AL was treated with cerclage wires. There was no loosening, osteolysis, or periprosthetic joint infection at the final followup.
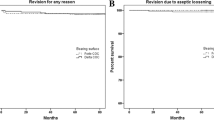
Mean HHS improved from 55.5 ± 16.3 to 93.2 ± 6.8 points at the final followup (p < 0.001). Two hips were revised as a result of liner dissociation and postoperative periprosthetic fracture, respectively. Survivorship with any reoperation and revision as the endpoint at a minimum of 5 years was 96.8% (95% confidence interval [CI], 90.45–98.96) and 97.9% (95% CI, 91.75–99.46), respectively (Fig. 2).

Survivorship with any reoperation and revision as the endpoint using the Kaplan-Meier method is shown.
Discussion
AMCs, also known as fourth-generation ceramics, provide superior strength with fracture toughness and allow manufacturing thinner liners with larger heads compared with earlier ceramic materials [1, 4]. Although these material improvements would be expected to decrease clinical concerns associated with previous-generation alumina bearings such as ceramic fracture and squeaking, little is known about this new bearing material and intermediate-term effects are unclear [7, 15, 27]. Therefore, we evaluated complications associated with the use of ceramic-on-ceramic AMC bearings and clinical outcomes including HHS and survivorship.
The present study has a number of limitations. First, this is not a comparative study. Comparison with those with different bearings would provide stronger evidence to our study. Second, it included a relatively small number of patients, which makes the statistical power of the study relatively weak. According to the manufacturer, fractures seen in third- and fourth-generation ceramics are as rare as 0.021% and 0.002% [25]. If the clinical performance of these bearings matches these laboratory findings, the number needed to treat to prevent a single ceramic fracture is as many as 4762 (range, 4351–5259) and 50,000 (range, 36,823–77,862), respectively. Nevertheless, as of the time of this writing, this is the first intermediate-term study after THA performed with AMC ceramic bearings conducted at a single institution by the same surgeon. We believe that our findings are valuable because, when new bearing materials are introduced, studies should be performed to look for unexpected complications unique to them. Third, we are unable to report long-term outcomes, because our study addresses intermediate-term outcomes with a minimum followup of 5 years. However, 90% of in vivo failures of AMC ceramics have been reported to occur within 24 months (80% at 12 months) after implantation [12]. Thus, different from third-generation ceramics, the fracture of fourth-generation ceramics appears to be rare after 5 years postoperatively. Fourth, average BMI is 23 ± 3 kg/m2; thus, we could not extend our conclusions to obese patients.
Liner dissociation is a concern. The rate of incorrect liner positioning has been reported as high as 16% in some studies and is thought to be the result of difficulty in seating along the axis of the Morse taper interior to the metal cups [15, 22]. As a result, instead of using a taper angle less than 10°, which generates a smaller window for engagement like in earlier designs, most manufacturers have adopted a taper of approximately 18°. Although increasing taper angle facilitates correct liner insertion into the shell, this change can complicate liner-cup engagement and lead to problems of secondary micromotion of the ceramic insert [18, 25]. Concerning the brittle nature of ceramics, we applied manual pressure with a plastic pusher on all ceramic liners and did not impact them after confirming square seating by tactile feeling with a finger [26]. A suction force acting at the instant of separation of the 28-mm-diameter head and liner was reported up to 30 N [10]. This force acts against the static friction between them and failure to impact the liner with sufficient force during assembly may contribute to liner dissociation [18]. Moreover, suction force between the head and liner and micromotion between the liner and cup secondary to joint torque force may increase as head size increases. Thus, a modular ceramic liner can introduce potential liner dissociation even after correct positioning. Indeed, special technical considerations, impacting the liner in particular, should be paid during the whole process of ceramic insertion [26]. We have not experienced ceramic bearing fracture. Although manufacturers reported a stable fracture rate of third- and fourth-generation ceramic liners going from 0.032% to 0.028% [25], this very low rate has not been supported by previous studies, which reported a higher rate of AMC ceramic liners ranging from 1.9% to 2% [7, 15] (Table 2). Most of those liner fractures were intraoperative insertional chipping [15] or postoperative fracture resulting from improper initial seating of the modular liner within the metal cup [7, 15]. Thus, liner fractures in vivo reported in earlier studies can be explained by technical errors rather than mechanical properties of the AMC ceramics. No patient reported squeaking, whereas three younger patients (3.2%) reported clicking in this study. Baek and Kim [2] reported squeaking in 1.4% and clicking in 18.3% after THAs using 28-mm-sized third-generation ceramic bearings at a mean followup of 7.1 years and attributed this to higher activity in younger patients and cultural habits like frequent squatting in Asian people. Hamilton et al. [15] hypothesized that absence of squeaking might result from smaller grain size in the AMC material leading to a lesser effect on the articular fluid film layer and avoidance of an elevated metallic rim. Other theoretical causes of squeaking include impingement, microseparation, or metal transfer. These might be reduced by the use of a larger head, but further comparative studies are necessary [12, 30].
In addition to the decrease in the risk of ceramic head fracture, another potential advantage of a larger head is that it may reduce the risk of dislocation and result in improved stable range of motion [21]. In THAs using AMC ceramics, when the acetabular cup size is large enough (> 50 mm in particular), a larger ceramic head (≥ 36 mm in particular) can be used. In our study, a 61-year-old woman with severe pelvic deformity by past trauma had a single event of perioperative dislocation. Although this result was comparable to those of previous intermediate-term studies using earlier generation ceramics ranging from 0% to 4% [9, 31, 35], dislocation is so multifactorial and the data available in this study are too small to draw any definite conclusions (Table 2). The risk of intraoperative femoral fractures has been shown as high as 5.4% during cementless primary THA [5]. Our rate appears higher than this. Because placement of a cerclage wire is a rapid procedure with little morbidity, when we suspected an intraoperative fracture, particularly in elderly females, we performed prophylactic cabling, which may account for this increase.
The HHS at the final followup in our study was 93.2 points, similar to those of previous studies ranging from 91 to 96 [8, 29] (Table 2). The 5-year survivorship free from revision was 97.9% and this result is also comparable to the survival rate of 95.9% to 96.0% in intermediate-term studies using third-generation ceramics [8, 23] and 97.6% in a short-term study using fourth-generation ceramics [15]. When new bearing materials are introduced, it is important to document patient-reported outcome and survivorship.
In conclusion, improved material properties combined with possible use of larger diameter heads make AMC ceramics a promising alternative bearing option with no evidence of increased early failure such as ceramic fracture, squeaking, and dislocation. Despite these encouraging midterm results, however, meticulous technical precautions such as square seating and proper impaction in particular should be taken during the whole process of liner insertion.
References
Al-Hajjar M, Fisher J, Tipper JL, Williams S, Jennings LM. Wear of 36-mm BIOLOX® delta ceramic-on-ceramic bearing in total hip replacements under edge loading conditions. Proc Inst Mech Eng H. 2013;227:535–542.
Baek SH, Kim SY. Cementless total hip arthroplasty with alumina bearings in patients younger than fifty with femoral head osteonecrosis. J Bone Joint Surg Am. 2008;90:1314–1320.
Barrack RL, Burak C, Skinner HB. Concerns about ceramics in THA. Clin Orthop Relat Res. 2004;429:73–79.
Benzaid R, Chevalier J, Saadaoui M, Fantozzi G, Nawa M, Diaz LA, Torrecillas R. Fracture toughness, strength and slow crack growth in a ceria stabilized zirconia-alumina nanocomposite for medical applications. Biomaterials. 2008;29:3636–3641.
Berry DJ. Epidemiology: hip and knee. Orthop Clin North Am. 1999;30:183–190.
Brady OH, Garbuz DS, Masri BA, Duncan CP. The reliability and validity of the Vancouver classification of femoral fractures after hip replacement. J Arthroplasty. 2000;15:59–62.
Cai P, Hu Y, Xie J. Large-diameter Delta ceramic-on-ceramic versus common-sized ceramic-on-polyethylene bearings in THA. Orthopedics. 2012;35:e1307–1313.
Capello WN, D’Antonio JA, Feinberg JR, Manley MT, Naughton M. Ceramic-on-ceramic total hip arthroplasty: update. J Arthroplasty. 2008;23:39–43.
Choi IY, Kim YS, Hwang KT, Kim YH. Incidence and factors associated with squeaking in alumina-on-alumina THA. Clin Orthop Relat Res. 2010;468:3234–3239.
Clarke MT, Lee PT, Villar RN. Dislocation after total hip replacement in relation to metal-on-metal bearing surfaces. J Bone Joint Surg Br. 2003;85:650–654.
Engh CA, Massin P, Suthers KE. Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop Relat Res. 1990;257:107–128.
Garino JP. The reliability of modern alumina bearings in total hip arthroplasty—update to a 2006 report. Semin Arthroplasty. 2013;24:193–201.
Ha YC, Kim SY, Kim HJ, Yoo JJ, Koo KH. Ceramic liner fracture after cementless alumina-on-alumina total hip arthroplasty. Clin Orthop Relat Res. 2007;458:106–110.
Hamadouche M, Boutin P, Daussange J, Bolander ME, Sedel L. Alumina-on-alumina total hip arthroplasty: a minimum 18.5-year follow-up study. J Bone Joint Surg Am. 2002;84:69–77.
Hamilton WG, McAuley JP, Dennis DA, Murphy JA, Blumenfeld TJ, Politi J. THA with Delta ceramic on ceramic: results of a multicenter investigational device exemption trial. Clin Orthop Relat Res. 2010;468:358–366.
Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am. 1969;51:737–755.
Jarrett CA, Ranawat AS, Bruzzone M, Blum YC, Rodriguez JA, Ranawat CS. The squeaking hip: a phenomenon of ceramic-on-ceramic total hip arthroplasty. J Bone Joint Surg Am. 2009;91:1344–1349.
Jeffers JR, Walter WL. Ceramic-on-ceramic bearings in hip arthroplasty: state of the art and the future. J Bone Joint Surg Br. 2012;94:735–745.
Johanson PE, Digas G, Herberts P, Thanner J, Karrholm J. Highly crosslinked polyethylene does not reduce aseptic loosening in cemented THA 10-year findings of a randomized study. Clin Orthop Relat Res. 2012;470:3083–3093.
Keurentjes JC, Kuipers RM, Wever DJ, Schreurs BW. High incidence of squeaking in THAs with alumina ceramic-on-ceramic bearings. Clin Orthop Relat Res. 2008;466:1438–1443.
Koo KH, Ha YC, Jung WH, Kim SR, Yoo JJ, Kim HJ. Isolated fracture of the ceramic head after third-generation alumina-on-alumina total hip arthroplasty. J Bone Joint Surg Am. 2008;90:329–336.
Langdown AJ, Pickard RJ, Hobbs CM, Clarke HJ, Dalton DJ, Grover ML. Incomplete seating of the liner with the Trident acetabular system: a cause for concern? J Bone Joint Surg Br. 2007;89:291–295.
Lusty PJ, Tai CC, Sew-Hoy RP, Walter WL, Walter WK, Zicat BA. Third-generation alumina-on-alumina ceramic bearings in cementless total hip arthroplasty. J Bone Joint Surg Am. 2007;89:2676–2683.
Maloney WJ, Jasty M, Harris WH, Galante JO, Callaghan JJ. Endosteal erosion in association with stable uncemented femoral components. J Bone Joint Surg Am. 1990;72:1025–1034.
Massin P, Lopes R, Masson B, Mainard D. Does Biolox Delta ceramic reduce the rate of component fractures in total hip replacement? Orthop Traumatol Surg Res. 2014;100:S317–321.
McAuley JP, Dennis DA, Grostefon J, Hamilton WG. Factors affecting modular acetabular ceramic liner insertion: a biomechanical analysis. Clin Orthop Relat Res. 2012;470:402–409.
McDonnell SM, Boyce G, Bare J, Young D, Shimmin AJ. The incidence of noise generation arising from the large-diameter Delta Motion ceramic total hip bearing. Bone Joint J. 2013;95:160–165.
Porat M, Parvizi J, Sharkey PF, Berend KR, Lombardi AV Jr, Barrack RL. Causes of failure of ceramic-on-ceramic and metal-on-metal hip arthroplasties. Clin Orthop Relat Res. 2012;470:382–387.
Restrepo C, Matar WY, Parvizi J, Rothman RH, Hozack WJ. Natural history of squeaking after total hip arthroplasty. Clin Orthop Relat Res. 2010;468:2340–2345.
Stanat SJ, Capozzi JD. Squeaking in third- and fourth-generation ceramic-on-ceramic total hip arthroplasty: meta-analysis and systematic review. J Arthroplasty. 2012;27:445–453.
Sugano N, Nishii T, Miki H, Yoshikawa H, Sato Y, Tamura S. Mid-term results of cementless total hip replacement using a ceramic-on-ceramic bearing with and without computer navigation. J Bone Joint Surg Br. 2007;89:455–460.
Tower SS, Currier JH, Currier BH, Lyford KA, Van Citters DW, Mayor MB. Rim cracking of the cross-linked longevity polyethylene acetabular liner after total hip arthroplasty. J Bone Joint Surg Am. 2007;89:2212–2217.
Udomkiat P, Wan Z, Dorr LD. Comparison of preoperative radiographs and intraoperative findings of fixation of hemispheric porous-coated sockets. J Bone Joint Surg Am. 2001;83:1865–1870.
Wiley KF, Ding K, Stoner JA, Teague DC, Yousuf KM. Incidence of pseudotumor and acute lymphocytic vasculitis associated lesion (ALVAL) reactions in metal-on-metal hip articulations: a meta-analysis. J Arthroplasty. 2013;28:1238–1245.
Yoo JJ, Kim YM, Yoon KS, Koo KH, Song WS, Kim HJ. Alumina-on-alumina total hip arthroplasty. A five-year minimum follow-up study. J Bone Joint Surg Am. 2005;87:530–535.
Acknowledgments
We thank Martin Zimmermann PhD, and Tae-Jin Shin PhD, for providing materials and information associated with Delta ceramics and professor Won Kee Lee for statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she, or a member of his or her immediate family, has no funding or commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research ® neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA-approval status, of any drug or device prior to clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
About this article

Cite this article
Baek, SH., Kim, W.K., Kim, J.Y. et al. Do Alumina Matrix Composite Bearings Decrease Hip Noises and Bearing Fractures at a Minimum of 5 Years After THA?. Clin Orthop Relat Res 473, 3796–3802 (2015). https://doi.org/10.1007/s11999-015-4428-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-015-4428-1