
Abstract
To systematically review the literature regarding the effect of air pollutants on the excess mortality risk among the elderly Chinese. PubMed, Scopus, Web of Science (WOS), and Chinese National Knowledge Infrastructure (CNKI) electronic databases were searched. A standardized data extraction form was used to collect methodological and outcome variables from each eligible study. The effect value was combined with a fixed- or random-effect model, and sensitivity analysis and publication bias test were performed. A total of 26 articles on air pollutants and excess risk (ER) of mortality in the Chinese elderly were identified. Among them, 16, 14, 8, and 8 articles contained PM2.5, PM10, SO2, and NO2 data, respectively. The meta-analysis results showed that the excess risk of mortality in the Chinese elderly associated with per 10 µg/m3 increase in PM2.5, PM10, SO2, and NO2 concentrations was 1.01%, 0.54%, 1.06%and 1.35%, respectively. Sufficient evidence supports that the increase in air pollutants (PM2.5, PM10, SO2, and NO2) will escalate the mortality of the elderly in China. Future research can study two or more air pollution models and the impact of air pollution on elderly mortality rates under different temperatures, duration of exposure, seasons and regions.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
1 Introduction
Air pollution is one of the greatest environmental risks to health. More than 90% of the global population 2019 lived in areas where concentrations exceeded the 2005 WHO air quality guideline of 10 µg/m3 (World Health Organization, 2021). The combined effects of ambient and household air pollution are associated with 7 million premature deaths annually (World Health Organization, 2023). From a health perspective, outdoor air pollution is a complex mixture of components that include airborne particulate matter (PM) and gaseous pollutants such as sulfur dioxide (SO2) and nitrogen dioxide (NO2), named primary pollutants (Camacho et al., 2020; Sun et al., 2010). Air pollution is widely recognized as an important causative agent of many non-communicable diseases, including diabetes mellitus, cardiovascular disease, Parkinson’s disease, neurological disorders, cancer, etc. (Meo et al., 2015; Cosselman et al., 2015; Chen et al., 2017; Heusinkveld et al., 2016; Turner et al., 2020). Moreover, air pollution contributes substantially to premature mortality and the disease burden of different populations (Cohen et al., 2017; Lelieveld et al., 2015; Yin, 2023).
Most research on air pollution and health is conducted in North America and Europe, while there needs to be more research on health effects in parts of Africa and Asia (Badida et al., 2023; Zhang et al., 2014). However, the negative impact of air pollution is more massive in low—and middle-income countries (World Health Organization, 2021). As the largest developing country, China has experienced severe ambient air pollution for a long time (Zhang et al., 2019a, b; Wei et al., 2023). Inhalable particles with aerodynamic diameters less than 10 and 2.5 um (PM10 and PM2.5), sulfur dioxide (SO2) and nitrogen dioxide (NO2) are important pollutants of concern to China (Chen et al., 2013; Tian et al., 2019). According to the bulletin on China's ecological environment in 2022, 126 out of 339 cities in China do not fulfill the Chinese air quality standards (Ministry of Ecology and Environment of the People’s Republic of China, 2022). Meanwhile, China is facing a severe challenge of aging. The 2020 Chinese census data showed that the proportion of people aged over 65 had reached 13.5% (Zheng, 2021). They indicate that China will soon transition from an aging into an aged society (Luo et al., 2021).
Aging is a continuous process of progressive decline of the body’s function leading to increased vulnerability, frailty or sensitivity in older people (Poland et al., 2014; Simoni et al., 2015). Previous studies have shown that older people are more vulnerable to air pollution than younger people (Lu et al., 2022; Luo et al., 2017; Qian et al., 2013). It is reported that increased pollution exposures have been associated with increased mortality and hospital admissions/emergency-room visits of the elderly, mainly due to exacerbations of chronic diseases or respiratory tract infections (Simoni et al., 2015). Several studies have shown a statistically significant correlation between air pollution and mortality among the elderly in China (Yang et al., 2012; Cai et al., 2019; Zeng et al., 2017). A study in Shenzhen found that with an increase of 10 µ g/m3 in PM2.5 concentration, the excess risk (ER) of mortality in the elderly is 1.32% (Cai et al., 2019). In Shenyang, a time-stratified case cross-analysis report states that with an increase in PM2.5 per 10 µg/m3 in the air, the excess risk of non-accidental death for elderly people aged 65–74 and ≥ 75 is 0.51% and 0.58%, respectively (Ma et al., 2011). Furthermore, a study in Baotou found that for every 10 µg/m3 increase in PM2.5 and PM10 in the air, the excess risk of non-accidental mortality among people aged 65 and above was 0.104% and 0.045%, respectively (Lu et al., 2022).
However, no previous meta-analyses focus on the effect of different air pollutants on elderly mortality. Only reviews and meta-analyses have demonstrated the acute effects of PM2.5 (Shang et al., 2013; Xia et al., 2019), PM10 (Jin et al., 2016; Shang et al., 2013), SO2 (Shang et al., 2013), and NO2 (Shang et al., 2013) on mortality rates for all age groups. Shang et al. (2013) showed that with 10 µg/m3 increases in gaseous pollutants PM2.5, PM10, SO2 and NO2, the total mortality risk in China were 0.38%, 0.32%, 0.81% and 1.30%. Xia et al. (2019) found that with an increase of PM2.5 in the air by 10 µg/m3, the excess risk of non-accidental death in the whole population in China will increase by 0.73%. Jin et al. (2016) concluded that with the increase of PM10 in the atmosphere by 10 µg/m3, the excess mortality of the whole population in China was 0.29%.
To our knowledge, this study is the first to systematically review existing literature regarding the impact of short-term exposure ambient to environmental air pollution on mortality among elderly adults in China. It synthesized scientific evidence examining the relationship between PM2.5, PM10, SO2, NO2 and excess mortality risk of the elderly in China. This study's findings help to provide theoretical evidence for the health risk assessment of air pollution of the elderly in China and other low- and middle-income countries. It also identified the limitations and gaps in this field that warranted future research.
2 Methods
Systematic review and meta-analysis procedures were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA, 2020).
2.1 Study Selection Criteria
Studies that met all of the following criteria were included in the review: (1) study designs: observational studies, such as time series or case-crossover studies; (2) exposures: specific air pollutants (PM2.5, PM10, SO2, NO2); (3) population: People aged only 65 and above; (4) outcome: mortality excess risk; (5) pollution model: single pollution model; (6) statistic methods: generalized linear model (GLM) or generalized additive model (GAM); (7) article types: peer-reviewed publications.
Studies that met any of the following criteria were excluded from the review: (1) no accurate data or the data cannot be converted to an excess risk (ER) value with a 95% CI; (2) no data for elderly individuals; (3) articles not written in Chinese or English; (4) death caused by disease, such as respiratory system disease; (5) study samples enrolled from a specific setting, for example, hospitals and nursing homes, etc.
2.2 Search of the Literature
Keywords and abstracts were searched in English databases of PubMed, Scopus, Web of Science (WOS) and the Chinese database of China National Knowledge Infrastructure (CNKI). The time window of search is from the inception of an electronic bibliographic database to 10th June 2023. The search algorithm includes all possible combinations of the following keywords: (1) PM2.5, PM10, SO2, NO2, ambient particulate matter, air pollutant, air quality and air pollution, (2) mortality, death or die, (3) elderly, old adults or older people, and (4) China or Chinese. Titles and abstracts of the articles identified through the keyword search were screened against the study selection criteria. Potentially relevant articles were retrieved for evaluation of the full text.
A reference list search (i.e., backward reference search) and cited reference search (i.e., forward reference search) were conducted based on the full-text articles meeting the study selection criteria that were identified from the keyword search. Articles identified from the backward and forward reference search were further screened and evaluated using the same study selection criteria. Reference searches were repeated on all newly identified articles until no additional relevant article was found.
2.3 Data Extraction
Standard data extraction tables were used to collect the following data for each included study: (1) first author and year of publication; (2) research time; (3) research area; (4) concentration of air pollutants; (5) statistical methods; (6) experimental design; (7) ER value and 95% confidence interval.
2.4 Study Quality Assessment
Quality assessment was performed to analyze the quality and risk of bias of the literature included in our review since no recognized quality assessment tools for time series and case cross study exists. We drew on the New Castle Ottawa Scale (Peterson et al., 2011) and the Cochrane risk of bias tool (Higgins et al., 2011), as applied in previous studies (Mustafic et al., 2012; Zhang et al., 2021). The quality of each study was evaluated on the basis of three aspects (the quality of air pollution data [0–1 point], the quality of mortality data [0–1 point], and the extent of adjustment for potential confounders [0–3 points]). For the quality of air pollution data, 1 point was awarded if ≤ 25% of daily pollutant data was missing, and 0 points were awarded if > 25% of daily pollutant data was missing. For the quality of mortality data, 1 point was awarded to studies with causes of mortality coded according to the International Classification of Disease, Revision 9 (ICD-9) or Revision 10 (ICD-10), whereas studies that did not meet this criterion were scored 0. For the adjustments for potential confounders, 3 points were awarded to studies that simultaneously considered meteorological factors, day of week and time trend, holiday effects or influenza epidemics. 2 points were awarded to studies that considered meteorological factors, day of the week and time trends effects, but did not consider holiday effects or influenza epidemics. 1 point were awarded to studies that only considered time trends effects. 0 points were given to studies that did not consider any of the confounders as mentioned above.
Studies that obtained the entire score in all three aspects were considered of high quality, studies that did not score in any of these aspects were considered of low quality, and studies in between were considered to be of intermediate quality.
2.5 Statistical Analysis
Meta-analysis was performed to estimate the effect of pollutants (PM2.5, PM10, SO2, NO2) and mortality excess risk among elderly Chinese individuals (age ≧65). The level of heterogeneity represented by the I2 index was interpreted as modest (I2 ≤ 25%), moderate (25% < I2 ≤ 50%), or considerable (I2 > 75%) (An et al., 2018; Higgins et al., 2003). Sensitivity analyses were assessed by repeating meta-analysis, removing one by one; that is, each study was excluded to test if individual studies had an effect on the pooled estimates (Deng et al., 2021). Publication bias was assessed by the funnel plots with Begg’s and Egger’s tests (Egger et al., 1997; Sterne & Egger, 2001; Racine et al., 2021).
All statistical analyses were conducted using the Stata 14.2 SE version (StataCorp, College Station, TX). Specific STATA commands included “metan” and “meta bias.” All analyses used two-sided tests; p-values less than 0.05 were considered statistically significant.
3 Results
3.1 Study Selection
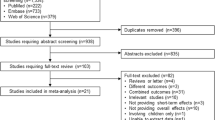
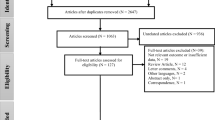
Figure 1 shows the study selection flow chart. We identified 1722 articles through keyword and reference searches, including 513 articles written in Chinese from CNKI and 1209 articles written in English from PubMed, Scopus and WOS. After removing duplicates, 1449 unique articles entered title and abstract screening, by which 1308 articles were excluded. The full texts of the remaining 141 articles were reviewed against the study selection criteria. Of these, 115 articles were excluded. Reasons for exclusion included: 54 articles did not have original data, 32 studies did not have data on the elderly, and 29 studies only did not have mortality data of non-accident. In total, 26 articles were included in the review, including 18 studies written in English and 8 in Chinese.

Flow chart of literature screening
3.2 Basic Characteristics of the Selected Studies
Table 1 summarizes the essential characteristics of the 26 studies included in the review. Twenty-one articles included other age groups and elderly individuals; only 5 (Chen et al., 2019; Huang et al., 2020; Qu et al., 2018; Zeng et al., 2019) articles exclusively examined older adults. All studies were published in the past twenty years, and the study areas included multiple cities in the north and south in China. Among these studies, there are 16, 14, 8 and 8 studies, including PM2.5, PM10, SO2 and NO2, respectively. Four studies adopted a time-stratified case-crossover study design, and others adopted a time-series design. The statistical models applied included the generalized additive model (GAM) and generalized linear model (GLM).
3.3 Meta-Analysis of the Impact of Four Pollutants on Elderly Mortality
Meta-analysis was conducted to estimate the correlation of four pollutants on mortality among the elderly in China. The analysis used excess risk included in each study. When the heterogeneity of literature in different pollution groups is greater than 75%, the data analysis adopts a random effect model. Figure 2 show the forest map generated by the meta-analysis of different pollutants. Table 2 show that the I2 values of PM2.5, PM10, SO2, and NO2 are 95.5%, 96.6%, 91.5%, and 82.6%. The combined ER values of PM2.5, PM10, SO2, and NO2 were 0.96 (95%CI: 0.63–1.28; p < 0.01), 0.53 (95%CI: 0.29–0.77; p < 0.01), 0.92 (95%CI: 0.44–1.41; p < 0.01) and 1.43 (95%CI: 0.92–1.94; p < 0.01), respectively. These findings indicate that for every 10 µg/m3 increase in the concentration of PM2.5, PM10, SO2, and NO2 in the atmosphere, the excess risk of mortality among the elderly was 0.96%, 0.53%, 0.92% and 1.43%, respectively.


Forest plot of the effect of air pollutants on the excess risk of elderly mortality in China
3.4 Subgroup Analysis
The included articles were grouped according to the concentration of air pollution for subgroup analysis. The GB3095-2012 standard annual average first level concentration limits NO2 (40 µg/m3) of the ministry of Ecology and Environment of the People's Republic of China were used as segmentation points for NO2 (Ministry of Ecology & Environment of the People's Republic of China, 2012). Moreover, since the average concentrations of PM2.5, PM10 and SO2 included in the literature are almost all higher than the annual average first-level concentration limits (PM2.5: 15 µg/m3, PM10: 40 µg/m3, and SO2: 20 µg/m3), the World Health Organization's 24-h second level concentration limit for PM2.5 (50 µg/m3) and PM10 (100 µg/m3) and the Air Quality Guidelines (AQG) level value for SO2 (40 µg/m3) were selected as the segmentation point (World Health Organization, 2021).
Table 3 shows the results of the subgroup analysis of the correlation of different concentrations of pollutants on elderly mortality. Under different concentrations of PM2.5, PM10, and NO2, an increase of 10 µg/m3 in PM2.5, PM10, and NO2 was significantly correlated with an increase in elderly mortality. Meanwhile, compared to the higher concentration group, in the lower concentration group, with each increase of 10 µg/m3 in PM2.5, PM10, and NO2, the excess risk mortality rate of the elderly is higher. Moreover, subgroup analysis of SO2 shows that in a low-concentration environment, the increase of SO2 concentration by 10 µg/m3 is not significantly related to elderly mortality, while in high concentration environment, the increase of SO2 concentration is significantly related to elderly mortality.
3.5 Publication Bias Test
Begg and Egger's methods were used in this study, and the results are shown in Table 4. The publication bias of air pollutants were not significant (P > 0.05). In addition, the funnel plot was drawn with logER as the abscissa and its standard error as the ordinate. It is found that the funnel plot is roughly symmetrical, indicating that there is no publication bias (Fig. 3). Therefore, there was no evidence of publication bias in the included literature.


Funnel chart of pollutants associated with air pollutants on the mortality of elderly individuals in China
3.6 Sensitivity Analysis
A sensitivity analysis was performed by repeating the meta-analysis to check the robustness of the combined results. Each of the initial studies was excluded, and the impact on the overall results was investigated according to the difference between the new and the initial effect values. Figure 4 shows that in the analysis of PM2.5, PM10, SO2, and NO2, the estimates obtained were essentially consistent with the initial results when any study was excluded, and changes only occurred in a narrow interval.


Sensitivity analysis of air pollutants on the mortality of elderly individuals in China
3.7 Study Quality Assessment
Table 5 reports the quality assessment of the included 26 studies. Five studies were classified as high quality, 21 were classified as medium quality, and none were classified as low quality. Overall, the quality of these studies was good, with high and intermediate quality accounting for 86.2%.
4 Discussion
This study is the first attempt to systematically review the correlation of air pollution on mortality among Chinese elderly. The results showed that with the increase of PM2.5, PM10, SO2 and NO2 concentrations by 10 µg/m3, the excess risk mortality of the elderly was 0.96%, 0.53%, 0.92% and 1.43%, respectively. There is no meta-analysis specifically targeting the elderly group in previous studies, but some surveys conducted in other countries have obtained similar results. A study in California shows that the excess risk mortality of the elderly was 0.6%, with an increase in PM2.5 concentration per 10 µg/m3 (Ostro et al., 2006). A study conducted in Seoul analyzed the health burden of related mortality caused by PM2.5 and concluded that PM2.5 contributed as much as 0.62% to the total mortality of the elderly (Jung et al., 2019). In a study in Singapore, the impact of air particles on the health of the population aged 65 years old and above was assessed. It was found that the risk of non-accidental death increased by 0.771% and 0.955%, respectively, in 0–5 days for every 10 µg/m3 increase in the concentration of PM10 and PM2.5 (Yap et al., 2019). Furthermore, A study observed that the percent increase in daily non-accidental mortality on each additional consecutive day with PM10 was 0.77% in Japan (Kim et al., 2019). Although the regions and air concentrations of the above studies varied, they all obtained relatively consistent results.
We found a more considerable negative correlation between air pollution and mortality among the elderly compared with the previous meta-analysis of ambient air pollutants and all-age mortality in China. Previous meta-analyses have found that as PM2.5, PM10, SO2, and NO2 in the air increase by 10 µ g/m3, the excess risk of non-accidental mortality for all age groups in China will increase by 0.73% (Xia et al., 2019), 0.29% (Jin et al., 2016), 0.81%, and 1.30% (Shang et al., 2013). These data are lower than the results of this study on older adults.
The subgroup analysis found that the influence of air pollution concentration on the excess risk mortality of the elderly is not a simple linear relationship. This is consistent with the conclusions of many previous studies (Burnett et al., 2014; Pope et al., 2011; Xia et al., 2019). In a meta-regression study, Burnett et al. (2014) found a more significant correlation at lower concentrations, and the PM2.5-mortality association was non-linear and more complex than described by a single unknown parameter. This may be the influence of other relevant factors in addition to air pollution concentration. In an integrated evaluation study of the impact of ambient air pollution on the risk of cardiovascular death, Pope et al. (2011) found that both exposure duration and intensity of air pollution impacted the risk of death. When the population is exposed to low to moderate pollution, a very steep and almost linear exposure–response relationship is observed, while at very high exposure, the exposure–response function is flat or stable, and there are likely essential risk trade-offs between duration and intensity of exposure. Moreover, a meta-analysis in China shows that the effect of daily average concentration has great regional differences (Xia et al., 2019). These studies provide a new perspective on the relationship between air pollution and mortality. Although the current linearity and nonlinearity have yet to be thoroughly examined or supported, more reasonable methods should be used to analyze the excess risk mortality of air pollution.
In addition, this study still has some limitations. First, other air pollutants such as CO and O3 may also affect the death of the elderly. However, due to a lack of research literature and inconsistent data, the analysis of the impact of increased CO and O3 on elderly mortality was not included. Second, this study only includes the effect estimates of the single pollutant model without considering the potential joint effects and collinearity among multiple pollutants. Moreover, in addition to air pollutants' concentration, the impact of temperature, duration of exposure, season and region on elderly mortality has also been put forward in previous studies. However, due to the limitations of the research scope, these contents were not analyzed.
5 Conclusion
This study synthesized scientific evidence examining the correlation of air pollutants on the excess risk of mortality among the elderly in China. The meta-analysis found that with the increase of PM2.5, PM10, SO2, and NO2 concentration by 10 µg/m3, the excess risk of death of the elderly was 0.96%, 0.53%, 0.92% and 1.43%, respectively. At different concentrations, the impact of air pollutants on the excess risk of death of the elderly is different. Future studies can also examine two or more air pollution models and the impact of air pollution on mortality in the elderly under different temperatures, duration of exposure, seasons and regions.
Data Availability
All the data and materials related to the manuscript are published with the paper and available from the corresponding author upon request.
References
An, R., Zhang, S., Ji, M., & Guan, C. (2018). Impact of ambient air pollution on physical activity among adults: A systematic review and meta-analysis. Perspectives in Public Health, 138(2), 111–121. https://doi.org/10.1177/1757913917726
Badida, P., Krishnamurthy, A., & Jayaprakash, J. (2023). Meta analysis of health effects of ambient air pollution exposure in low-and middle-income countries. Environmental Research, 216, 114604. https://doi.org/10.1016/j.envres.2022.114604
Burnett, R. T., Pope, C. A., III., Ezzati, M., Olives, C., Lim, S. S., Mehta, S., Shin, H. H., Singh, G., Hubbell, B., Brauer, M., Anderson, H. R., Smith, K. R., Balmes, J. R., Bruce, N. G., Kan, H., Laden, F., Prüss-Ustün, A., Turner, M. C., Gapstur, S. M., … Cohen, A. (2014). An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environmental Health Perspectives, 122(4), 397–403. https://doi.org/10.1289/ehp.1307049
Cai, J., Peng, C., Yu, S., Pei, Y., Liu, N., Wu, Y., ... & Cheng, J. (2019). Association between PM2.5 exposure and all-cause, non-accidental, accidental, different respiratory diseases, sex and age mortality in Shenzhen, China. International Journal of Environmental Research and Public Health, 16(3), 401. https://doi.org/10.3390/ijerph16030401
Camacho, I., Camacho, J., Camacho, R., Góis, A., & Nóbrega, V. (2020). Influence of outdoor air pollution on cardiovascular diseases in Madeira (Portugal). Water, Air, & Soil Pollution, 231, 1–15. https://doi.org/10.1007/s11270-020-4430-4
Chen, R., Pan, G., Kan, H., Tan, J., Song, W., Wu, Z., ... & Chen, B. (2010). Ambient air pollution and daily mortality in Anshan, China: a time-stratified case-crossover analysis. Science of the Total Environment, 408(24), 6086–6091. https://doi.org/10.1016/j.scitotenv.2010.09.018
Chen, R., Zhao, Z., & Kan, H. (2013). Heavy smog and hospital visits in Beijing, China. American Journal of Respiratory and Critical Care Medicine, 188(9), 1170–1171. https://doi.org/10.1164/rccm.201304-0678LE
Chen, H., Kwong, J. C., Copes, R., Tu, K., Villeneuve, P. J., Van Donkelaar, A., Hystad, P., Martin, R. V., Murray, B. J., Barry, J., Wilton, A. S., Kopp, A., & Burnett, R. T. (2017). Living near major roads and the incidence of dementia, Parkinson’s disease, and multiple sclerosis: A population-based cohort study. The Lancet, 389(10070), 718–726. https://doi.org/10.1016/S0140-6736(16)32399-6
Chen, R., Yin, P., Meng, X., Wang, L., Liu, C., Niu, Y., ... & Zhou, M. (2018a). Associations between ambient nitrogen dioxide and daily cause-specific mortality: evidence from 272 Chinese cities. Epidemiology, 29(4), 482–489. https://doi.org/10.1097/EDE.0000000000000829
Chen, C., Xu, D., He, M. Z., Wang, Y., Du, Z., Du, Y., Qian, Y., Ji, D., & Li, T. (2018b). Fine particle constituents and mortality: A time-series study in Beijing, China. Environmental Science & Technology, 52(19), 11378–11386. https://doi.org/10.1021/acs.est.8b00424
Chen, L., Zhao, C., Guan, M.-Y., Liu, Y., Xu, D.-Q., & Song, J. (2018c). Time-series analysis of the relationship between particulate matter and mortality in Shijiazhuang. Chinese Journal of Disease Control & Prevention, 22(3), 272–277. https://doi.org/10.16462/j.cnki.zhjbkz.2018.03.014
Chen, R., Yin, P., Meng, X., Wang, L., Liu, C., Niu, Y., Liu, Y., Liu, J., Qi, J., You, J., Kan, H., & Zhou, M. (2019a). Associations between coarse particulate matter air pollution and cause-specific mortality: A nationwide analysis in 272 Chinese cities. Environmental Health Perspectives, 127(1), 17008–17008. https://doi.org/10.1289/EHP2711
Chen, Z., Chen, X., Dong, H., & Wang, K. (2019b). Effect of fine particulate matter on daily mortality in the aged people in Changzhou City: A time-series study. Modern Preventive Medicine, 46(7), 1181–1185.
Chen, Y., Jiang, F., & Jiang, Z. (2020). Time-series analysis on the acute mortality affected by ambient particulate matter in Zhenjiang between 2015 and 2018. Modern Preventive Medicine, 47(14), 2550–2554.
Chen, Y., Jiao, Z., Chen, P., Fan, L., Zhou, X., Pu, Y., ... & Yin, L. (2021). Short-term effect of fine particulate matter and ozone on non-accidental mortality and respiratory mortality in Lishui district, China. BMC Public Health, 21(1), 1–11. https://doi.org/10.1186/s12889-021-11713-9
Cohen, A. J., Brauer, M., Burnett, R., Anderson, H. R., Frostad, J., Estep, K., ... & Forouzanfar, M. H. (2017). Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. The Lancet, 389(10082), 1907–1918. https://doi.org/10.1016/S0140-6736(17)30505-6
Cosselman, K. E., Navas-Acien, A., & Kaufman, J. D. (2015). Environmental factors in cardiovascular disease. Nature Reviews Cardiology, 12(11), 627–642. https://doi.org/10.1038/nrcardio.2015.152
Deng, J., Zhou, F., Hou, W., Silver, Z., Wong, C. Y., Chang, O., ... & Zuo, Q. K. (2021). The prevalence of depression, anxiety, and sleep disturbances in COVID‐19 patients: a meta‐analysis. Annals of the New York Academy of Sciences, 1486(1), 90–111. https://doi.org/10.1111/nyas.14506
Egger, M., Smith, G. D., Schneider, M., & Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test. BMJ, 315(7109), 629–634.
He, T., Yang, Z., Liu, T., Shen, Y., Fu, X., Qian, X., ... & Tang, J. (2016). Ambient air pollution and years of life lost in Ningbo, China. Scientific Reports, 6(1), 1–10. https://doi.org/10.1038/srep22485
Heusinkveld, H. J., Wahle, T., Campbell, A., Westerink, R. H., Tran, L., Johnston, H., ... & Schins, R. P. (2016). Neurodegenerative and neurological disorders by small inhaled particles. Neurotoxicology, 56, 94–106. https://doi.org/10.1016/j.neuro.2016.07.007
Higgins, J. P., Thompson, S. G., Deeks, J. J., & Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ, 327(7414), 557–560.
Higgins, J. P., Altman, D. G., Gøtzsche, P. C., Jüni, P., Moher, D., Oxman, A. D., ... & Sterne, J. A. (2011). The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ, 343. https://doi.org/10.1136/bmj.d5928
Hou, B., Dai, L., Wang, Z., et al. (2011). Time-series analysis of acute mortality effects of air pollution in Xi’an. Huan Jing Yu Jian Kang Za Zhi, 28(12), 1039–1043.
Hu, K., Guo, Y., Hu, D., Du, R., Yang, X., Zhong, J., ... & Qi, J. (2018). Mortality burden attributable to PM1 in Zhejiang province, China. Environment International, 121, 515–522. https://doi.org/10.1016/j.envint.2018.09.033
Huang, S., Zhong, W., Lin, L., Lin, X., & Yin, Y. (2020). Relationship between the elderly death counts and atmospheric fine particulates in Fuzhou City by time series study. Journal of Strait Preventive Medicine, 26(6), 11–13.
Jin, M., Tian, L., & Tong, J. (2016). Association between air inhalable particles and mortality in China: A meta-analysis. Journal of Environmental Health, 33(08), 725–729. https://doi.org/10.16241/j.cnki.1001-5914.2016.08.018
Jung, E. J., Na, W., Lee, K. E., & Jang, J. Y. (2019). Elderly mortality and exposure to fine particulate matter and ozone. Journal of Korean Medical Science, 34(48), e311. https://doi.org/10.3346/jkms.2019.34.e311
Kan, H., London, S. J., Chen, G., Zhang, Y., Song, G., Zhao, N., ... & Chen, B. (2008). Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: The Public Health and Air Pollution in Asia (PAPA) Study. Environmental Health Perspectives, 116(9), 1183–1188. https://doi.org/10.1289/ehp.10851
Kim, H., Kim, H., & Lee, J. T. (2019). Spatial variation in lag structure in the short-term effects of air pollution on mortality in seven major South Korean cities, 2006–2013. Environment International, 125, 595–605. https://doi.org/10.1016/j.envint.2018.09.004
Lelieveld, J., Evans, J. S., Fnais, M., Giannadaki, D., & Pozzer, A. (2015). The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature, 525(7569), 367–371. https://doi.org/10.1038/nature15371
Lin, H., Liu, T., Xiao, J., Zeng, W., Li, X., Guo, L., ... & Ma, W. (2016). Mortality burden of ambient fine particulate air pollution in six Chinese cities: results from the Pearl River Delta study. Environment International, 96, 91–97. https://doi.org/10.1016/j.envint.2016.09.007
Lu, Y. K., Liu, X. L., Liu, Y. H., Chen, N., Gao, H. Y., Jin, Y. H., & Yan, Y. X. (2022). The effects of short-term exposure to air pollution on mortality in Baotou, China, during 2015–2019. Environmental Geochemistry and Health, 1–18. https://doi.org/10.1007/s10653-022-01419-1
Luo, L., Jiang, J., Zhang, G., Wang, L., Wang, Z., Yang, J., & Yu, C. (2017). Stroke mortality attributable to ambient particulate matter pollution from 1990 to 2015 in China: An age-period-cohort and spatial autocorrelation analysis. International Journal of Environmental Research and Public Health, 14(7), 772. https://doi.org/10.3390/ijerph14070772
Luo, Y., Su, B., & Zheng, X. (2021). Trends and challenges for population and health during population aging—China, 2015–2050. China CDC Weekly, 3(28), 593. https://doi.org/10.46234/ccdcw2021.158
Ma, Y., Chen, R., Pan, G., Xu, X., Song, W., Chen, B., & Kan, H. (2011). Fine particulate air pollution and daily mortality in Shenyang, China. Science of the Total Environment, 409(13), 2473–2477. https://doi.org/10.1016/j.scitotenv.2011.03.017
Meo, S. A., Memon, A. N., Sheikh, S. A., Rouq, F. A., Usmani, A. M., Hassan, A., & Arian, S. A. (2015). Effect of environmental air pollution on type 2 diabetes mellitus. European Review for Medical and Pharmacological Sciences, 19(1), 123–128.
Ministry of Ecology and Environment of the People’s Republic of China. (2012). GB3095—2012Ambient air quality standards. China Environmental Science Press.
Ministry of Ecology and Environment of the People’s Republic of China. (2022). The bulletin of China’s ecological environment.
Mustafić, H., Jabre, P., Caussin, C., Murad, M. H., Escolano, S., Tafflet, M., ... & Jouven, X. (2012). Main air pollutants and myocardial infarction: A systematic review and meta-analysis. JAMA, 307(7), 713–721. https://doi.org/10.1001/jama.2012.126
Ostro, B., Broadwin, R., Green, S., Feng, W. Y., & Lipsett, M. (2006). Fine particulate air pollution and mortality in nine California counties: Results from CALFINE. Environmental Health Perspectives, 114(1), 29–33. https://doi.org/10.1289/ehp.8335
Peterson, J., Welch, V., Losos, M., & Tugwell, P. J. O. O. H. R. I. (2011). The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa: Ottawa Hospital Research Institute, 2(1), 1–12.
Poland, G. A., Ovsyannikova, I. G., Kennedy, R. B., et al. (2014). A systems biology approach to the effect of aging, immunosenescence and vaccine response. Current Opinion in Immunology, 29, 62–68. https://doi.org/10.1016/j.coi.2014.04.005
Pope, C. A., Brook, R. D., Burnett, R. T., & Dockery, D. W. (2011). How is cardiovascular disease mortality risk affected by duration and intensity of fine particulate matter exposure? An integration of the epidemiologic evidence. Air Quality, Atmosphere & Health, 4(1), 5–14. https://doi.org/10.1007/s11869-010-0082-7
PRISMA (2020) Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Available online at: http://www.prisma-statement.org/ (Last accessed 4th June 2023).
Qian, Z., He, Q., Lin, H. M., Kong, L., Liao, D., Dan, J., ... & Wang, B. (2007). Association of daily cause-specific mortality with ambient particle air pollution in Wuhan, China. Environmental Research, 105(3), 380–389. https://doi.org/10.1016/j.envres.2007.05.007
Qian, Y., Zhu, M., Cai, B., Yang, Q., Kan, H., Song, G., ... & Wang, C. (2013). Epidemiological evidence on association between ambient air pollution and stroke mortality. Journal of Epidemiology and Community Health, 67(8), 635–640. https://doi.org/10.1136/jech-2012-201096
Qu, Y., Pan, Y., Niu, H., He, Y., Li, M., Li, L., ... & Li, B. (2018). Short-term effects of fine particulate matter on non-accidental and circulatory diseases mortality: a time series study among the elder in Changchun. PLoS One, 13(12), e0209793. https://doi.org/10.1371/journal.pone.0209793
Qu, Y., Zhou, Q., Chen, Y., Yang, Y., Kang, S., He, C., Jiang, Y., Wu, C., Liu, B., & Xiang, J. (2022). The relationship between atmospheric particulate pollution and non accidental death of residents in Fuzhou urban area around COVID-19. Carcinogenesis, Teratogenesis & Mutagenesis, 34(2), 98–104. https://doi.org/10.3969/j.issn.1004-616x,2022.02.004
Racine, N., McArthur, B. A., Cooke, J. E., Eirich, R., Zhu, J., & Madigan, S. (2021). Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19: A meta-analysis. JAMA Pediatrics, 175(11), 1142–1150.
Shang, Y., Sun, Z., Cao, J., Wang, X., Zhong, L., Bi, X., ... & Huang, W. (2013). Systematic review of Chinese studies of short-term exposure to air pollution and daily mortality. Environment International, 54, 100–111. https://doi.org/10.1016/j.envint.2013.01.010
Simoni, M., Baldacci, S., Maio, S., Cerrai, S., Sarno, G., & Viegi, G. (2015). Adverse effects of outdoor pollution in the elderly. Journal of Thoracic Disease, 7(1), 34. https://doi.org/10.3978/j.issn.2072-1439.2014.12.10
Sterne, J. A., & Egger, M. (2001). Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. Journal of Clinical Epidemiology, 54(10), 1046–1055. https://doi.org/10.1016/S0895-4356(01)00377-8
Sun, Q., Hong, X., & Wold, L. E. (2010). Cardiovascular effects of ambient particulate air pollution exposure. Circulation, 121(25), 2755–2765. https://doi.org/10.1161/CIRCULATIONAHA.109.893461
Tian, L., Yang, C., Zhou, Z., Wu, Z., Pan, X., & Clements, A. C. (2019). Spatial patterns and effects of air pollution and meteorological factors on hospitalization for chronic lung diseases in Beijing, China. Science China Life Sciences, 62, 1381–1388. https://doi.org/10.1007/s11427-018-9413-y
Turner, M. C., Andersen, Z. J., Baccarelli, A., Diver, W. R., Gapstur, S. M., Pope III, C. A., ... & Cohen, A. (2020). Outdoor air pollution and cancer: An overview of the current evidence and public health recommendations. CA: A Cancer Journal for Clinicians, 70(6), 460–479. https://doi.org/10.3322/caac.21632
Wei, J., Li, Z., Wang, J., Li, C., Gupta, P., & Cribb, M. (2023). Ground-level gaseous pollutants (NO 2, SO 2, and CO) in China: Daily seamless mapping and spatiotemporal variations. Atmospheric Chemistry and Physics, 23(2), 1511–1532.
World Health Organization. (2021). WHO global air quality guidelines: particulate matter (PM2.5 and PM10), ozone, nitrogen dioxide, sulfur dioxide and carbon monoxide. https://apps.who.int/iris/handle/10665/345329 (Last accessed 8th June 2023)
World Health Organization. (2023). Air pollution. https://www.who.int/health-topics/air-pollution#tab=tab_2 (Last accessed 8th June 2023)
Wu, Y., Zhang, F., Shi, Y., Pilot, E., Lin, L., Fu, Y., ... & Wang, W. (2016). Spatiotemporal characteristics and health effects of air pollutants in Shenzhen. Atmospheric Pollution Research, 7(1), 58–65. https://doi.org/10.1016/j.apr.2015.07.005
Xia, Z., Wang, X., Yu, S., & Qian, Y. (2019). Meta-analysis of the association between PM2.5 pollution and total non-accidental mortality of residents in different regions in China. Environmental Pollution and Prevention, 41(08), 891–895. https://doi.org/10.15985/j.cnki.1001-3865.2019.08.005
Xu, Z., Xiong, L., Jin, D., & Tan, J. (2021). Association between short-term exposure to sulfur dioxide and carbon monoxide and ischemic heart disease and non-accidental death in Changsha city, China. PloS One, 16(5), e0251108. https://doi.org/10.1371/journal.pone.0251108
Yang, C., Peng, X., Huang, W., Chen, R., Xu, Z., Chen, B., & Kan, H. (2012). A time-stratified case-crossover study of fine particulate matter air pollution and mortality in Guangzhou, China. International Archives of Occupational and Environmental Health, 85, 579–585. https://doi.org/10.1007/s00420-011-0707-7
Yap, J., Ng, Y., Yeo, K. K., Sahlén, A., Lam, C. S. P., Lee, V., & Ma, S. (2019). Particulate air pollution on cardiovascular mortality in the tropics: Impact on the elderly. Environmental Health, 18(1), 1–9. https://doi.org/10.1186/s12940-019-0476-4
Yin, S. (2023). Decadal changes in premature mortality associated with exposure to outdoor PM2.5 in mainland Southeast Asia and the impacts of biomass burning and anthropogenic emissions. Science of The Total Environment, 854, 158775. https://doi.org/10.1016/j.scitotenv.2022.158775
Yu, I. T. S., Hui Zhang, Y., San Tam, W. W., Yan, Q. H., Jun Xu, Y., Jun Xun, X., ... & Lao, X. Q. (2012). Effect of ambient air pollution on daily mortality rates in Guangzhou, China. Atmospheric Environment, 46, 528-535. https://doi.org/10.1016/j.atmosenv.2011.07.055
Zeng, Q., Ni, Y., Jiang, G., Li, G., & Pan, X. (2017). The short term burden of ambient particulate matters on non-accidental mortality and years of life lost: A ten-year multi-district study in Tianjin, China. Environmental Pollution, 220, 713–719. https://doi.org/10.1016/j.envpol.2016.10.036
Zeng, J., Chen, J., Zhou, L., Jiang, X., & Zhang, L. (2019). Air pollution PM2.5 related excess mortality risk assessment among elderly residents in Chendu, Jiangsu. Journal of Preventive Medicine, 30(02), 147–149+162. https://doi.org/10.13668/j.issn.1006-9070.2019.02.011
Zhang, Y., Li, M., Bravo, M. A., Jin, L., Nori-Sarma, A., Xu, Y., ... & Bell, M. L. (2014). Air quality in Lanzhou, a major industrial city in China: characteristics of air pollution and review of existing evidence from air pollution and health studies. Water, Air, & Soil Pollution, 225, 1–17. https://doi.org/10.1007/s11270-014-2187-3
Zhang, K., Chen, X., Zhou, L., Li, T., & Sun, Q. (2015). Time-series analysis of association between inhalable particulate matter and daily mortality in Nanjing. Huan jing yu jian kang za zhi, 32(6), 485–488. https://doi.org/10.16241/j.cnki.1001-5914.2015.06.004
Zhang, F., Liu, X., Zhou, L., Yu, Y., Wang, L., Lu, J., & Krafft, T. (2016). Spatiotemporal patterns of particulate matter (PM) and associations between PM and mortality in Shenzhen, China. BMC Public Health, 16(1), 1–11. https://doi.org/10.1186/s12889-016-2725-6
Zhang, J., Chen, Q., Wang, Q., Ding, Z., Sun, H., & Xu, Y. (2019a). The acute health effects of ozone and PM2. 5 on daily cardiovascular disease mortality: A multi-center time series study in China. Ecotoxicology and Environmental Safety, 174, 218–223. https://doi.org/10.1016/j.ecoenv.2019.02.085
Zhang, J., McLaughlin, S. J., & Li, L. W. (2019b). Cumulative exposure to air pollution and subsequent mortality among older adults in China. Journal of Public Health, 41(3), 518–526. https://doi.org/10.1093/pubmed/fdy154
Zhang, H., Zhang, X., Wang, Q., Xu, Y., Feng, Y., Yu, Z., & Huang, C. (2021). Ambient air pollution and stillbirth: An updated systematic review and meta-analysis of epidemiological studies. Environmental Pollution, 278, 116752. https://doi.org/10.1016/j.envpol.2021.116752
Zheng, Z. (2021). From the past to the future: What we learn from China’s 2020 Census. China Population and Development Studies, 5(2), 101–106. https://doi.org/10.1007/s42379-021-00084-8
Acknowledgements
We thank the anonymous reviewers for their valuable suggestions.
Author information
Authors and Affiliations
Contributions
Cong Liu, Andiara Schwingel and Rong Gao participated in the study design and protocol and wrote the manuscript; Fengwei Jia and Mengmeng Ji sorted out the research process and analyzed the data; Guofeng Qu, Chunping Ye and Jiali Cheng screened the literature and drafted the manuscript. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Informed Consent Statement
Not applicable.
Institutional Review Board Statement
Not applicable.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Liu, C., Jia, F., Ji, M. et al. The Effect of Short-Term Air Pollutants Exposure on Daily Mortality Among Elderly Individuals in China: A Systematic Review and Meta-Analysis. Water Air Soil Pollut 234, 541 (2023). https://doi.org/10.1007/s11270-023-06566-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11270-023-06566-4