
Abstract
Guidance for medical staff reminds employees of the responsibility to deliver spiritual care in its broadest sense, respecting the dignity, humanity, individuality and diversity of the people whose cultures, faiths and beliefs coexist in society. This is no small or simple task, and although GPs (family practitioners) have been encouraged to deliver spiritual care, we suggest this is proving to be challenging and needs further careful debate. This literature review critiques and analyses existing studies and points to four categories of attitude to spiritual care, and two related but distinct concepts of spirituality in use by GPs. Our aims were to search for, summarise and critique the qualitative literature regarding general practitioners’ views on spirituality and their role in relation to spiritual care. An integrative review was made by a multidisciplinary team using a critical realism framework. We searched seven databases and completed thematic and matrix analyses of the qualitative literature. A number of good-quality studies exist and show that some but not all GPs are willing to offer spiritual care. Four patterns of attitude towards delivering spiritual care emerge from the studies which indicate different levels of engagement with spiritual care: embracing, pragmatic, guarded and rejecting. Further research is needed to identify whether these four views are fixed or fluid, whether training in spiritual care modifies these and whether they relate to patterns of care in practice, or patient outcomes. The authors suggest that some of the difference in viewpoint relate to the lack of clear philosophical framework. The authors suggest critical realism as having potential to facilitate interdisciplinary research and create clearer concepts of spiritual care for GPs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Qualitative and quantitative research studies have demonstrated that there are likely to be associations between certain religious and spiritual variables and health outcomes (Ellison and Levin 1998; Koenig 2011). These relationships may not be simple, and many of the studies are methodologically imperfect, but as more sophisticated research proceeds, these associations have persisted though there is some discussion about causality (Sloan 2006).
General practitioners in the UK more widely have been encouraged to think about incorporating spiritual care into their provision for patients (NHS Education for Scotland 2009). This advice to attend to a spiritual dimension of care specifically includes but is not confined to circumstances that include palliative care (Puchalski et al. 2009) and mental health care (Cook 2013). Interest in spirituality and health may reflect a wider discussion about the role of the biomedical model, and in examining what the humanities can bring to complex patient care problems (Misselbrook 2015). However, there is limited evidence that GPs are delivering effective spiritual care in any explicit way, or in one that effects outcomes.
Research to date has concluded that while in general most GPs see a role for themselves in spiritual care (Murray et al. 2003), this is not universal (Vermandere et al. 2011). The reservations of those who have not embraced this concept may contain insights that need to be more fully understood. We sought to clarify this situation via an integrative review: a form of research that reviews, critiques, and synthesises representative literature in an integrated way such that new frameworks and perspectives on the topic are generated (Torraco 2005).
We referred to a consensus definition of spirituality (Puchalski et al. 2009). This is thought to provide a set of parameters which has clinical usefulness in discussions around spirituality:
Spirituality The aspect of humanity that refers to the way individuals seek and express meaning and purpose and the way they experience their connectedness to the moment, to self, to others, to nature, and to the significant or sacred.
Religion We formed a definition of religion with reference to NHS spiritual care documentation (NHS Education for Scotland 2009) and by discussion to consensus. The definition adopted was “The characteristic beliefs and practices of a community of faith with particular reference to the worship of a divine being”.
Aims of the Study
-
1.
To summarise existing research related to general practitioners’ perceptions of spirituality, religion and spiritual care.
-
2.
To explore whether a robust and useful concept of spirituality exists in primary care.
-
3.
To identify gaps in the current literature and to suggest future research agendas.
Methods
Our interdisciplinary team included academic staff of the University of Aberdeen’s rural health and theology departments and included researchers with both theist and atheist belief. We used basic critical realism as the philosophical framework for the study. Critical realism has the advantage of being able to hold the weight of discussion between the humanities and sciences without diminishing either (Roberts 2014). Critical realism views science neither purely within the limitations of Popper/Hempel terms, where knowledge can only be gained by experiment, nor in relativist constructivist terms where nothing can be absolutely true or real except in relation to the experience of a particular observer. Critical realism describes an objective reality, but one which can only be understood incompletely due to the limitations of the human processes by which it can be investigated (Bhaskar 2008). It has proven usefulness in social science research (Danermark et al. 1997).
We made reference to the PRISMA guidelines (Moher et al. 2009) and to the HTA guidance (Murphy et al. 1998) in creating a framework for the search strategy. We used PRISMA to create a clear rationale for the study, defining eligibility criteria, information sources and study selection. We followed the HTA guidance on synthesising qualitative data at this stage of the review, and we used three methods of study identification:
-
1.
Formal electronic database search—2001 studies.
-
2.
Cross-referencing to bibliographies of key papers—2 studies.
-
3.
Expert peer review to ensure no papers were missed. No studies.
References and papers were sought from seven databases, using MESH headings and expanded terms and included both clinical scientific and social science/religion databases (e.g. ATLA). Each database was individually searched using a custom search, and all search results were available for inspection by the three reviewers.
Inclusion/Exclusion Criteria
Studies were included where they:
-
1.
Have a substantial focus on the research questions, i.e. investigated perceptions of spirituality as it related to the adopted definitions.
-
2.
Presented original data
-
3.
Related to general practitioners/primary care doctors
-
4.
Were published, in English, in the last 30 years
-
5.
Were published in peer review journals
Studies were excluded where they:
-
1.
Did not relate to the chosen definition of spirituality.
-
2.
Were individual case reports or studies involving the opinion of five, or fewer general practitioners.
After reading full manuscripts of the retrieved studies, and in accordance with the HTA standards for qualitative research review, we decided also to exclude papers which:
-
3.
Studied a heterogeneous group of carers or professionals, including but not confined to general practitioners, unless the views of the latter could be clearly differentiated.
-
4.
Papers where the focus was on complementary therapies, case reports, and reports and studies of “faith healing” (Table 1).
Table 1 Search strategy for Ovid-based Databases
Quality appraisal of studies:
We chose to qualitatively analyse the quality of studies to moderate the effect on our synthesis rather than to exclude certain studies (Gough et al. 2012).
Data extraction and analysis:
We performed a matrix analysis as described by Miles and Huberman (1994) as a way of highlighting and contrasting data from different studies to bring out unique insights and perspectives in relation to the way the data is configured.
In addition, we performed a formal grounded theory thematic analysis of participants’ views using QSR NVIVO 10 (Glaser and Strauss 1967). The research team assumed responsibility for the authenticity and validity of this process, which occurred through regular cross-disciplinary meetings.
Synthesis of the Data
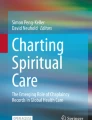
Experience and opinion from diverse cultures cannot simply be added together and merged conceptually (aggregation) without great care (Pope et al. 2007). In common with principles of ethnographic research, we chose only to perform limited aggregation and tried to preserve the context of the studies unless the concepts of spirituality were clearly analogous (Noblit and Hare 1988) (Fig. 1).

PRISMA-based flowchart shows inclusion and exclusion of studies at each stage
Results
All of the nine qualitative studies had robust methods of recording, transcribing and analysing. One study did not have a prospective design and relied on video initially and later on field notes (Saba 1999). Two studies explicitly stated an overall philosophical framework (phenomenology), and eight had a robust description of their methodology of analysing data, grounded theory being the most common. Most studies did not offer a concept of spirituality to its participants, probably legitimately because GPs’ own concepts were often sought.
A total of 294 GPs’ opinions were investigated. Three studies asked more fundamental questions about practice, and spirituality arose as a significant theme in participants’ responses. These three began their focus on: listening in primary care and awareness of personal boundaries to care (Cocksedge and May 2009), managing palliative patients (Kelly et al. 2008) and on what GPs believe and value in their work (Saba 1999).
No studies made specific attempts to investigate GPs’ perceptions of religion or its relation to health. However, respondents frequently made reference to religion in their answers, consistent with the idea that religious orientation and practice functionally and conceptually are an aspect of, but not necessarily mandatory for, GPs’ understandings of spirituality. A minority of researchers chose to ascertain or record religious affiliations of participants. There are some theoretical reasons why asking religious affiliation may detract from the validity of interviewees’ subsequent opinions: for example, participants may feel they are representing the views of their faith community rather than their private view. The failure to ascertain religious affiliation could also be seen as a weakness in ascertaining diversity of the sample. Where they were stated, participants’ affiliations included: Atheist, Agnostic, Muslim, Seventh Day Adventist, Christian, Jewish, Unitarian, “Universalist with Buddhist leanings” and “none”. The majority of participants whose beliefs could be identified were Christian (Table 2).
Thematic analysis of the studies showed several common themes emerging.
We identified four which related to GPs’ attitudes to being spiritual care providers. These were:
-
1.
Embracing—GPs who accept and approve a role for GPs in spiritual care.
“It’s an inherent part of the whole person, spirituality” GP 1. “If it’s unmet then that will impact on their overall health” GP 2 (Murray et al. 2003)
-
2.
Pragmatic—GPs who accept a role if it is deemed to help or be wished by the patient.
“Yes, I do see dealing with these as part of my role. But I generally consider that it would be up to him and his wife to raise them and they haven’t done so to date.”(Murray et al. 2003)
-
3.
Guarded—GPs who have reservations about the role and might consider providing spiritual care with some provisos or in some limited contexts.
“Everyone says ‘‘this only takes a few minutes.’’ If you keep adding that up it’s more than the 10 min that you have with a patient. It’s definitely important, but you can’t address it at every single visit.” (Olson et al. 2006)
-
4.
Rejecting—GPs who are fundamentally opposed to the role, regardless of circumstance.
“I think in the first place that it is not my personal responsibility to start up a conversation with the patient about ‘spiritual care’. So is that my role? Is that my task? Is that my duty? I don’t think so.” (Vermandere et al. 2012)
There are suggestions of a possible causal relationship of a GP’s attitude to providing spiritual care dependent on the personal belief of the GP.
“I do discuss it with some of my patients. I’ve got quite a lot of people from church who perhaps choose to see me rather than one of my partners. I would never push it down people’s throats, but if it’s obviously something they want to talk about, then I don’t feel uncomfortable because I have a faith of my own.” (Cocksedge and May 2009)
The author commented: “Of the three doctors who could not recall ever having had any consultations involving spiritual issues, two professed no personal faith”
There are also narratives that indicate that some GPs can, through awareness of their own personal assumptions and boundaries, modify and broaden their approach from their own beliefs or philosophical position to be more congruent with the patient or situation.
Two differently centred but overlapping concepts of spirituality were identified in the GP narratives.
-
1.
Exocentric: relating to connection with an ultimate spiritual reality which is independent of the individual. This concept expresses a recognition that spirituality transcends the individual towards an identifiable “Other” in its locus and intention. The commonest expression of exocentric spirituality in the literature is theocentric: relating to connection with the divine or to an ultimate being, usually through religious affiliation or commitment. One respondent put it in this form, although it arose in many other forms.
“Spirituality is seeing people as unique human beings whom God has created.” (Craigie et al. 1999)
-
2.
Anthropocentric: Centred on the individual’s needs. A quest for personal or individual meaning, human connectedness, the fulfilment of a deep existential need.
“[Spirituality is] a personal attitude to life, an outlook on life, … […] Spirituality is, to a certain extent, the time that you invest in the way you relate to things.” (Vermandere et al. 2012)
These concepts were not mutually exclusive, and participants often used theocentric and anthropocentric concepts of spirituality side by side. These concepts seem to be distinct in their focus, but used by many GPs without any sense of boundary between them.
“Religion is one of the forms, I think, in which spirituality can be expressed or defined. Thus I think it is a subset of the larger set we call “spirituality”. Uhh … beyond that, I don’t really see any other distinctions. But I think that you can perfectly well be spiritual in a non-religious way. That is also possible. And, yes, it seems to me that there are many different mixed forms of spirituality.” (Vermandere et al. 2012)
Another way of thinking about this would be to distinguish expressions of spirituality that have a concept of sacredness, (Pargament and Mahoney 2002) and those that do not.
Discussion
Most studies use convenience sampling, some used geographical sampling and a few use theoretical or intentional sampling. Few authors made more than a very superficial attempt to describe the belief demographic of the patient population. This knowledge forms an important context in which GPs deliver spiritual care. Critical realism states that cause and effect in society are, at least in part, local and contextual, e.g. positive associations between health and spirituality in one context may not operate in others.
In collating studies, it is important to recognise the significant cultural and religious differences which exist between study locations, for example between the UK and the USA. The cultural acceptability of religious belief and the prevalence of religious affiliation vary in these contexts (“Religion—Ipsos Global Trends,” n.d.). Similarly, the perceived role of GPs in society and understandings of appropriate professional behaviour are likely to vary. Terms like “spirituality” and “religious” may have different usage or connotations in different countries and these differences are likely to be reflected in GPs perceptions.
Study participants seem frequently to make assumptions about the correlation between religious service attendance and the beliefs of their patients. In patient populations, differences in belief, commitment and practice are known not to fit into simple categorisations (Aisthorpe 2016; Levin and Meador 2012). Likewise, few GPs comment on the diversity of religious affiliation in their populations. With some exceptions, we suggest that where affiliation could be ascertained there was generally a higher focus on a Judeo-Christian perspective of spirituality both from the point of view of authorship and participants.
Most research teams were composed of clinicians although three included psychiatry, nursing or social science departments. Concern has been expressed from more than one perspective that research which treats religious experience and belief purely as a health variable are limited as they rely on a reductionist position and in this respect there are no multidisciplinary studies which include the humanities. We argue this may be due to the difficulty that clinical sciences and the humanities experience in dialogue. We propose from both the practical experience of our research team and from the arguments of critical realism that this difficulty arises from the use of incompatible epistemologies, ways of discerning truth. Critical realism allows for a middle-ground approach using a more flexible and robust philosophical framework. We propose a critical realism approach may promote more effective dialogue and reflects a more current approach to science.
Implications for Future Research
Future studies which would be valuable might:
-
Be conducted in multiethnic and religiously diverse environments or among GPs with a wider range of religious affiliation. Have stronger sampling strategies to ensure better saturation of data.
-
Recognise that it may not be possible to easily aggregate research that is culturally diverse.
-
Be conducted with explicit philosophical frameworks which support interdisciplinary discussion and are consistent with current thinking on the philosophy of science. We offer critical realism as a possible framework.
-
Investigate GPs’ opinions regarding religion and spirituality as distinct, but related concepts.
-
Investigate any possible causal associations between GPs’ personal beliefs and their perceptions of spirituality, their willingness to offer spiritual care, or the type of spiritual care they offer. Investigate to what extent GPs can show pragmatism or flexibility in delivering spiritual care, despite their own beliefs.
-
Conduct research which tests the acceptability and outcomes of different models of spiritual care delivered in primary care
Conclusions
The concept of spiritual care in general practice suggests potential (Best et al. 2015) but needs more careful debate. Critical realism may provide an intellectually persuasive and practical framework for these discussions and avoid polarised arguments.
There is a good deal in common with the concept of spirituality which GPs use in practice but we argue that two differently focussed but not mutually exclusive concepts of spirituality are represented by GPs: exocentric and anthropocentric.
At least four different types of attitude to providing spiritual care exist in the literature: embracing, pragmatic, guarded and rejecting. Further research is needed to investigate whether these attitudes are fixed or fluid. There is some evidence in the literature that these attitudes influence both the likelihood and the nature of spiritual care being delivered by the GP. It may be worth investigating whether training, or other characteristics such as pragmatism or patient centeredness, may modify these views in terms of delivery of spiritual care.
If it is thought desirable to encourage spiritual care in general practice, we will need to find common frameworks for these discussions and recognise and learn from our current diversity of views. Perhaps that will allow us to neither rush in, nor fear to tread.
How this fits in: A modest number of studies from the USA, Europe, and Australia have described provisional but not universal acceptance of a spiritual care concept and role for GPs. This literature review critiques and analyses existing studies and points to four categories of attitude to spiritual care, and two related but distinct concepts of spirituality in use by GPs. The review recognises a need for further studies in a multi ethnic context and research with robust philosophical frameworks. The authors suggest critical realism as having potential to facilitate interdisciplinary research and create clearer concepts of spiritual care for GPs |
References
Aisthorpe, S. (2016). The invisible church (1st ed.). Edinburgh: St. Andrews Press.
Best, M., Butow, P., & Olver, I. (2015). Do patients want doctors to talk about spirituality? A systematic literature review. Patient Education and Counseling, 98(11), 1320–1328. https://doi.org/10.1016/j.pec.2015.04.017.
Bhaskar, R. (2008). A realist theory of science (1st ed.). Oxford: Routledge.
Cocksedge, S., & May, C. (2009). Doctors’ perceptions of personal boundaries to primary care interactions: A qualitative investigation. Communication and Medicine, 6(2), 109–116.
Colaizzi, P. F. (1978). Psychological research as the phenomenologist views it. In R. S. Valle & M. King (Eds.), Existential-phenomenological alternatives for psychology (pp. 48–71). New York: Oxford University Press.
Cook, C. C. H. (2013). Royal College of Psychiatrists position statement PS03/2013. London. https://www.rcpsych.ac.uk/pdf/PS03_2013.pdf. Accessed 19 Feb 2018.
Craigie, J., Frederic, C., & Hobbs, R. F., III. (1999). Spiritual perspectives and practices of family physicians with an expressed interest in spirituality. Family Medicine, 31(8), 578–585.
Danermark, B., Ekstrom, M., Jacobsen, L., & Karlsson, J. (1997). Explaining society: Critical realism and the social sciences (2nd ed.). Oxford: Routledge.
Ellis, M. R., Campbell, J. D., Detwiler-Breidenbach, A., & Hubbard, D. K. (2002). What do family physicians think about spirituality in clinical practice? Journal of Family Practice, 51(3), 249–254.
Ellison, C., & Levin, J. (1998). The religion-health connection: Evidence, theory, and future directions. Health Education and Behavior, 25(6), 700–720.
Glaser, B., & Strauss, A. (1967). The discovery of grounded theory, strategies for qualitative research (3rd ed.). New Jersey: Transaction Publishers.
Gough, D., Oliver, S., & Thomas, J. (2012). An introduction to systematic reviews (1st ed.). London: Sage.
Grant, E., Murray, S., Kendall, M., Boyd, K., Tilley, S., & Ryan, P. (2004). Spiritual issues and needs: Perspectives from patients with advanced cancer and nonmalignant disease. A qualitative study. Cambridge: Palliative and Supportive Care, Cambridge University Press.
Kelly, B., Varghese, F. T., Burnett, P., Turner, J., Robertson, M., Kelly, P., et al. (2008). General practitioners’ experiences of the psychological aspects in the care of a dying patient. Palliative and Supportive Care, 6(2), 125–131.
Koenig, H. (2011). Spirituality and health research (1st ed.). West Conshocken: Templeton Press.
Levin, J., & Meador, K. (2012). Healing to all their flesh (1st ed.). West Conshehocken: Templeton Press.
Mays, N., & Pope, C. (1996). Qualitative research in health care. London: BMJ Publishing Group.
Miles, M. B., & Huberman, A. M. (1994). Qualitative data analysis: An expanded sourcebook (2nd ed.). Thousand Oaks, CA: Sage Publications.
Misselbrook, D. (2015). An A to Z of medical philosophy. British Journal of General Practice, 65(631), 88.
Moher, David, Liberati, Alessandro, Tetzlaff, Jennifer, & Altman, Douglas G. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ. https://doi.org/10.1136/bmj.b2535.
Murphy, E., Dingwall, R., Greatbatch, D., Parker, S., & Watson, P. (1998). Qualitative research methods in health technology assessment: A review of the literature. Health Technol Assessment, 2(16), 1–276.
Murray, S. A., Kendall, M., Boyd, K., Worth, A., & Benton, T. F. (2003). General practitioners and their possible role in providing spiritual care: A qualitative study. British Journal of General Practice, 53(497), 957–959.
NHS Education for Scotland. (2009). www.nes.scot.nhs.uk. Spiritual Care Matters. Thistle House 91 Haymarket Terrace EDINBURGH EH12 5HE February 2009.
Noblit, G., & Hare, D. (1988). Meta—Ethnography: Synthesizing qualitative studies (1st ed.). Thousand Oaks, CA: Sage.
Olson, M. M., Sandor, M. K., Sierpina, V. S., Vanderpool, H. Y., & Dayao, P. (2006). Mind, body, and spirit: Family physicians’ beliefs, attitudes, and practices regarding the integration of patient spirituality into medical care. Journal of Religion and Health, 45(2), 234–247.
Pargament, K., & Mahoney, A. (2002). Sacred matters: Sanctification as a vital topic for the psychology of religion. Bowling State University Working Paper 02-17.
Pope, C., Mays, N., & Popay., J. (2007). Synthesizing qualitative and quantitative health evidence (1st ed.). Berkshire: Oxford University Press.
Puchalski, C., Ferrell, B., Virani, R., Otis-Green, S., Baird, P., Bull, J., et al. (2009). Improving the quality of spiritual care as a dimension of palliative care: The report of the Consensus Conference. Journal of Palliative Medicine, 12(10), 885–904(1).
Religion—Ipsos Global Trends. (n.d.). Retrieved October 23, 2017, from https://www.ipsosglobaltrends.com/religion/.
Roberts, J. M. (2014). Critical realism, dialectics, and qualitative research methods. Journal for the Theory of Social Behaviour, 44(1), 1–23. https://doi.org/10.1111/jtsb.12056.
Saba, G. W. (1999). What do family physicians believe and value in their work? The Journal of the American Board of Family Practice/American Board of Family Practice, 12(3), 206–213.
Sloan, R. P. (2006). Blind faith—The unholy alliance of religion and medicine (1st ed.). New York: St. Martins Press.
Strauss, A., & Corbin, J. (1990). Basics of qualitative research: Grounded theory procedures, techniques. Newbury Park, CA: Sage Publications.
Strauss, A., & Corbin, J. (1998). Basics of qualitative research techniques and procedures for developing grounded theory. London: Sage Publications.
Torraco, R. (2005). Writing integrative literature reviews: Guidelines and examples. Human Resources Development Review, 1(3), 356–367.
Vermandere, M., Choi, Y.-N., De Brabandere, H., Decouttere, R., De Meyere, E., Gheysens, E., et al. (2012). GPs’ views concerning spirituality and the use of the FICA tool in palliative care in Flanders: A qualitative study. British Journal of General Practice, 62(603), e718–e725. https://doi.org/10.3399/bjgp12X656865.
Vermandere, M., De Lepeleire, J., Smeets, L., Hannes, K., Van Mechelen, W., Warmenhoven, F., et al. (2011). Spirituality in general practice: A qualitative evidence synthesis. British Journal of General Practice, 61(592), e749–e760.
Acknowledgements
Thanks to Jenny Jones, Stirling University, Rod Sampson and Melanie Bickerton, and Nicola Ring, University of Stirling.
Funding
A bursary from the University of Aberdeen was awarded. Ethical approval is not required.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Appleby, A., Wilson, P. & Swinton, J. Spiritual Care in General Practice: Rushing in or Fearing to Tread? An Integrative Review of Qualitative Literature. J Relig Health 57, 1108–1124 (2018). https://doi.org/10.1007/s10943-018-0581-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10943-018-0581-7