
Abstract
Cardiac stress can induce morphological, structural and functional changes of the heart, referred to as cardiac remodeling. Myocardial infarction or sustained overload as a result of pathological causes such as hypertension or valve insufficiency may result in progressive remodeling and finally lead to heart failure (HF). Whereas pathological and physiological (exercise, pregnancy) overload both stimulate cardiomyocyte growth (hypertrophy), only pathological remodeling is characterized by increased deposition of extracellular matrix proteins, termed fibrosis, and loss of cardiomyocytes by necrosis, apoptosis and/or phagocytosis. HF is strongly associated with age, and cardiomyocyte loss and fibrosis are typical signs of the aging heart. Fibrosis results in stiffening of the heart, conductivity problems and reduced oxygen diffusion, and is associated with diminished ventricular function and arrhythmias. As a consequence, the workload of cardiomyocytes in the fibrotic heart is further augmented, whereas the physiological environment is becoming less favorable. This causes additional cardiomyocyte death and replacement of lost cardiomyocytes by fibrotic material, generating a vicious cycle of further decline of cardiac function. Breaking this fibrosis-cell death axis could halt further pathological and age-related cardiac regression and potentially reverse remodeling. In this review, we will describe the interaction between cardiac fibrosis, cardiomyocyte hypertrophy and cell death, and discuss potential strategies for tackling progressive cardiac remodeling and HF.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Heart failure and cardiac remodeling
Fibrosis is the excessive deposition of extracellular matrix (ECM), such as collagens and fibronectin, resulting in the excessive accumulation of fibrous connective tissue [1, 2]. Fibrosis is an essential process in the repair of damaged tissues and wounds, but its accumulation in organs and tissues can lead to scarring, organ dysfunction and, ultimately, failure. In many chronic diseases, sustained progressive fibrosis can be very detrimental, like in fibrotic kidney and liver disease, and this is also true for chronic heart failure [3]. Heart failure (HF) is a complex clinical syndrome in which reduced cardiac function results in insufficient perfusion of peripheral tissues [4, 5]. HF is an enormous health problem in the Western society, in which more than 8 % of the population aged 75 years and older are diagnosed with HF, and prevalence and incidence rates are not expected to decline in the upcoming decade [6]. Cardiac remodeling, which can be described as any structural and functional change of the heart, underlies HF development. Cardiac remodeling is a reaction of the heart to reduce ventricular wall stress in response to changes in after load (pressure load), preload (volume overload) or myocardial injury [7]. Amongst others, main risk factors for HF include coronary artery disease and hypertension [6]. A recent study of a community-based cohort revealed that more than 70 % of new HF patients had a history of hypertension and more than 25 % have had a preceding myocardial infarction (MI) [8]. Regardless of the initiating events, cardiac hypertrophy, cardiomyocyte cell death and fibrosis constitute key features of pathological cardiac remodeling.
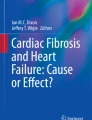
Fibrosis is a hallmark of pathological cardiac remodeling and is absent under physiological stress conditions, such as exercise and pregnancy [9–11]. Cardiac fibrosis appears to be an irreversible process [12] and is increasingly recognized as a major cause of morbidity and mortality in many chronic diseases. In the myocardium, fibrosis can be divided into interstitial fibrosis, replacement fibrosis and perivascular fibrosis, which all have their characteristics (Fig. 1). The distinction between different types of fibrosis is made based on cause and anatomical localization [13]. As a response to increased wall stress generated by a cardiac stressor, like hypertension, interstitial reactive fibrosis is developed in the myocardium [14, 15]. Reactive interstitial fibrosis is located in the ECM surrounding cells and is defined as the expansion of ECM without cardiomyocyte loss and is characterized by a widespread deposition of collagens throughout the myocardium [13, 14]. In perivascular fibrosis, which is also associated with hypertension, fibrillar collagens accumulate in the adventitia of intramural coronary arteries [14, 16, 17]. With ongoing hypertension, the accumulation of collagens progresses [17].

Different types of fibrosis. Mouse cardiac tissue was stained with Masson’s trichrome stain to visualize cardiomyocytes in red and fibrotic fibers in blue. Pictures with interstitial and perivascular fibrosis are from pressure overload (TAC) mouse hearts and replacement fibrosis from mouse hearts with a myocardial infarction. Bar indicates 50 µm
Replacement fibrosis occurs in the myocardium to replace dead tissue and is an essential repair process after myocardial infarction [13, 14, 16, 18]. Since cardiomyocytes have no or only very limited proliferative capacity, cardiomyocyte replacement does not occur in the damaged heart and scar formation is the only reparative mechanism to prevent cardiac rupture. Replacement fibrosis does also occur under other pathological conditions that will ultimately affect cardiomyocyte viability, like in sustained hypertension, cardiomyopathies and valve insufficiencies. This may result in a more dispersed fibrosis throughout the myocardium.
Thus, fibrosis may initially have cardiac preserving functions, but a sustained fibrotic response, as observed under pathological conditions, may negatively impact on cardiac function and finally exacerbate cardiac functional decline. Persistent accumulation of collagens disturbs tissue architecture, stiffens the heart and can affect both systolic and diastolic function and contribute to arrhythmias [17]. In agreement with this hypothesis, Hein et al. [19] observed in aortic stenosis patients with HF an increase in fibrosis and cell death. This was strongly increased in decompensated patients in whom fibrosis and myocyte degeneration was strongly accelerated [19]. These observations support the view that an apparent vicious cycle of impaired cardiac function, fibrogenesis and cell death exists and if not properly treated this cycle will accelerate and result in cardiac failure [19]. Not surprisingly, fibrosis-associated proteins, including soluble suppression of tumorigenicity 2 (sST2) and galectin-3 (Gal-3), which can be detected in blood plasma, are increasingly recognized as markers for poor prognosis of HF patients [20–23]. These biomarkers have recently been included in the AHA/ACC clinical guidelines for potential additive risk stratification of patients with established HF [5]. Nevertheless, additional research will be required to prove that circulating biomarkers properly reflect histological myocardial fibrosis [24].
In contrast to cardiac fibrosis, hypertrophy is generally believed to be an adaptive and protective mechanism since it also occurs in athletes and pregnant women [9–11]. This physiological hypertrophy is reversible and does not decompensate to HF. Sustained wall stress associated with cardiovascular diseases generates, however, a pathological form of hypertrophy, which is associated with reduced cardiomyocyte function. Among others, pathological hypertrophy involves alterations in Ca2+ handling, increased oxidative stress, changes in excitation–contraction coupling, sarcomere dysfunction and metabolic and energetic remodeling [9–11]. These cellular and molecular changes finally culminate into cardiomyocyte death caused by necrosis, apoptosis and/or phagocytosis [9, 25, 26]. Importantly, myofibroblasts, which are the main producers of ECM components, also secrete numerous factors with inflammatory and paracrine functions and play an essential role in hypertrophy development under pathological conditions. The contribution of myofibroblasts toward cardiac dysfunction is therefore twofold, namely via connective tissue formation and via production of paracrine and inflammatory molecules [27, 28]. Together, this will promote pathological cardiomyocyte hypertrophy and may finally lead to cardiomyocyte death and progressive deterioration of cardiac function. Excellent reviews have been published on apoptosis (programmed cell death), necrosis and phagocytosis, and we will not elaborate on these and other modes of cell death [26, 29–31]. Here, we will review the deleterious effects of activated (myo)fibroblast on cardiac function and postulate an apparent vicious cycle of fibrogenesis, impaired cardiac function and cardiomyocyte cell death (Fig. 2).

A simplified depiction of the vicious cycle of myofibroblast activation, impaired cardiac function and cardiomyocyte cell death. This simplified scheme shows in the outer circle (black) the role of myofibroblasts in fibrogenesis and cardiac impairment, whereas the inner processes predominantly reflect paracrine signaling effects. Together, this generates a sustained response of progressive cardiac deterioration. FMT fibroblasts to myofibroblasts transition, IL-6 interleukin-6, IL-33 interleukin-33, FGF2 fibroblast growth factor 2, TGFβ transforming growth factor beta. Lightning symbols indicate stressors acting on the cells
Cardiac fibroblasts and myofibroblasts
In the healthy heart, normal amounts of fibrillar collagens form a network between different cell types within the myocardium and are essential to provide a scaffold for myofiber alignment and to maintain cardiac geometry during systole and diastole of the heart. Collagen I and III are the main collagens in the heart and constitute about 85 and 10 % of collagen, respectively [16]. Fibroblasts, which constitute the majority of the large (40–70 %) non-myocyte population in the heart [32–34] are responsible for the turnover of ECM proteins and play an essential role in maintaining the integrity of connective tissue. It is generally believed that most cardiac fibroblasts in the myocardium are derived from the pericardium during development, but proper fait mapping is still lacking [34]. Fibroblasts are a heterogeneous group of cells, and so far no specific markers have been identified for fibroblasts. Discoidin domain receptor 2 (DDR2), a tyrosine kinase cell surface receptor for collagen [35], has been predominantly used to define fibroblast in the heart [33]. DDR2 is also expressed in other cells outside the heart, and among others, it is important for chondrocyte proliferation [36]. Thus, although it may specify fibroblasts in the heart, it is not a specific fibroblast marker in general.
A common feature to fibrotic diseases is the activation of fibroblasts and their differentiation into myofibroblasts, which express and secrete much higher levels of ECM proteins. Myofibroblasts are not usually present in healthy cardiac tissue, with the exception of heart valve leaflets. Fibroblasts to myofibroblasts transition (FMT) can be induced by mechanical stress, cytokines, growth factors and ECM components [37]. Transforming growth factor β (TGFβ) is the most potent activator of FMT. Three homologues of TGFβ isoforms exist (TGFβ1, TGFβ2, TGFβ3) in mammalians that are produced as latent precursors bound to latency-associated peptide (LAP), which can interact with latent TGFβ-binding proteins (LTBP1–4) to form a large latent complex (LLC) that is effectively secreted into the extracellular space. Only after cleavage of this complex by extracellular proteases, TGFβ becomes liberated and can bind to its cellular receptor [38, 39]. TGFβ signals via a heteromeric tyrosine kinase complex of TGFβ type I receptor (TGFBR1, also termed Alk5) and type II receptor (TGFBR2), in which TGFBR2 phosphorylates TGFBR1, which propagates the signal via activation of SMAD transcription factors. This results in relocalization of the SMAD2/SMAD3 to the nucleus and the expression of ECM matrix proteins and alpha-smooth muscle actin (αSMA) [40]. The latter is used as a marker to identify myofibroblasts, although it is not specific and is also strongly expressed in smooth muscle cells [41]. αSMA allows contraction of myofibroblasts [42], and this is important during wound closure, but in the heart it can affect cardiac function and contribute to arrhythmogenicity [43]. Importantly, inhibition of TGFβ signaling has been shown to reduce fibrosis in animal models of cardiac remodeling and to preserve cardiac function [44, 45].
Besides FMT, TGFβ also stimulates epithelial mesenchymal transition (EMT) and endothelial mesenchymal transition (EndoMT) [46, 47]. It has been reported that approximately 27–35 % of all cardiac fibroblasts in the pressure-overloaded mouse heart (aortic banding) were derived from endothelial cells via EndoMT [48]. Inhibition of EndoMT by infusion of recombinant bone morphogenic protein-7 (BMP-7) reduced fibrosis in the mouse pressure-overloaded heart by almost 50 % [48]. Recent cell lineage tracking studies in mice reported much lower levels of EndoMT-derived fibroblasts and, moreover, did not provide a role for enhanced EndoMT during cardiac pressure overload [49, 50]. Thus, although EndoMT plays an important role during development of HF [51, 52], the role for EndoMT in the stressed heart is still controversial. Circulating bone marrow-derived cells have also been proposed to be a source of myofibroblasts in the diseased heart [53, 54], but cell lineage tracking has also disputed these results [49, 50].
Recently, Kramann et al. [55] identified glioma-associated oncogene family zinc finger 1 (Gli1) positive perivascular mesenchymal stem cells (MSCs) as a source of myofibroblast cells in mouse tissue after induction of organ damage, including the pressure-overloaded heart (aortic banding). Interestingly, ablation of these Gli1+ cells reduced cardiac fibrosis by almost 50 %, but also reduced cardiac hypertrophy and preserved left ventricular ejection fraction. This nicely exemplifies the importance of myofibroblasts in the fibrotic process and in the induction of pathological hypertrophy. The role of TGFβ in the transition of these Gli1+ cells is so far not known.
Thus, although the exact nature of myofibroblasts in the heart remains obscure, these cells are most likely generated from resident cell types in the heart. Inhibition of the formation of these myofibroblast populations reduces fibrosis and improves cardiac function.
Fibrosis impairs cardiac function
Myofibroblast-mediated fibrosis in the myocardium is the hallmark of pathophysiological cardiac remodeling [13, 14, 18]. In addition to collagens, fibronectin and other structural ECM proteins, myofibroblasts also express a large number of matrix remodeling proteins and together determine the functionality of the ECM. Matrix metalloproteases (MMPs) are produced by myofibroblasts and are secreted as inactive zymogens that can be activated by cleavage of the propeptide, resulting in active proteases that can cleave collagens and other ECM proteins [2, 56]. These MMPs are negatively regulated by tissue inhibitors of metalloproteases (TIMPs), which are also secreted by myofibroblasts. TIMP1 is the major TIMP in the heart and is strongly induced in the failing heart [57]. Other matrix remodeling proteins that are strongly induced in the failing heart include, among others, lysyl oxidase-like 1 (LOXL1), latent-transforming growth factor beta-binding protein 2 (LTBP2), Gal-3, connective tissue growth factor (CTGF), periostin (POSTN), and Serpine2 [58]. Dysregulation of the proper balance between the different ECM and ECM-modulating proteins will affect the amount of connective tissue, its composition and quality, and will affect cardiac function. Recently, the plasma membrane glycoprotein syndecan-4 was identified to influence the degree of collagen cross-linking, which ultimately determined the degree of myocardial stiffness [59]. Syndecan-4 induces collagen, osteopontin (OPN) and lysyl oxidase (LOX) expression in cardiac fibroblasts and promotes LOX-dependent cross-linking of collagen fibers [59–61]. Thus, besides the amount of ECM, the level of collagen cross-linking also strongly determines the development of diastolic and systolic dysfunction [9, 16–18, 25, 56, 62].
Fibrosis also disturbs cardiac electrophysiology and induces rhythm disturbances. In mice, TGFβ1 overexpression resulted in atrial fibrosis, without ventricular involvement, and these mice developed inducible atrial fibrillation (AF) [63, 64]. Also in patients, AF is strongly associated with atrial fibrosis, [65] and it is now generally accepted that atrial fibrosis creates a substrate for AF [66, 67]. The mechanism by which myocardial scarring promotes rhythm disturbances is by creating reentry circuits [9, 16, 18, 62, 68, 69]. Furthermore, function of ion channels, ion pumps and gap junction proteins is also disturbed by cardiac remodeling [70]. Thereby, action potential conduction velocity is reduced which promotes susceptibility to reentry [70].
Finally, fibrosis limits nutrient supply toward the myocardium by limiting cardiac function and myocardial blood flow [9]. Perivascular fibrosis in coronary arteries reduces oxygen delivery toward myocardial tissue, reduces coronary reserves and promotes myocardial ischemia [16, 62]. Moreover, increased ECM deposition, which occurs often in association with hypertension and thus myocardial hypertrophy, results in diffusion problems in a situation in which demand for oxygen and nutrients is increased [14]. As discussed below, (myo)fibroblast also play an important role in cardiomyocyte hypertrophy development, and increased cardiomyocyte cell size will reduce oxygen diffusion in the cell interior. Decreased capillary density, as observed in heart failure tissue, will further contribute to cardiomyocyte dysfunction and finally cell death [71, 72].
Thus, fibrosis impairs cardiac function by at least three mechanisms, namely induction of myocardial stiffness, induction of AF and limiting oxygen and nutrient supply to the stressed myocardium. This will promote cardiomyocyte hypertrophy and cell death as schematically depicted in Fig. 2.
Myofibroblasts and cardiomyocyte hypertrophy and cell death
Within the myocardium, extensive cross talk between cardiac fibroblast and cardiomyocytes via soluble factors and direct cell–cell interactions occurs [27]. Fibroblast–cardiomyocyte co-cultures and experiments with conditioned medium have shown that paracrine signaling from fibroblasts induces cardiomyocyte hypertrophy. A number of cytokines and growth factors, including TGFβ, interleukin-33 (IL-33), fibroblast growth factor 2 (FGF2), tumor necrosis factor alpha (TNFα), insulin growth factor (IGF1) and endothelin-1 (ET-1), are produced by (myo)fibroblast, which directly affect cardiomyocyte function in vitro and/or in vivo [27, 73–79]. Myofibroblasts contribute to the pathological hypertrophic response in cardiomyocytes via paracrine signaling, which ultimately can culminate in cardiomyocyte cell death. In mice with a fibroblast-specific knockout of Krüppel-like factor 5 (Klf5), a transcription factor required for the fibrotic response, both fibrosis and cardiomyocyte hypertrophy were strongly ameliorated in the pressure-overloaded heart. Moreover, pathological cardiomyocyte gene expression, as exemplified by Nppa expression, was strongly reduced in these mice [80].
In the last decade, a number of microRNAs (miRs) have been identified that are increased selectively in fibroblasts of the failing heart [15, 81]. The TGFβ-induced miR-21 inhibits sprouty homologue 1 (Spry1) expression, an endogenous inhibitor of the ERK-MAPK signaling pathway. This mechanism is important for fibroblast survival and for growth factor secretion and controls both the extend of interstitial fibrosis and cardiomyocyte hypertrophy. Silencing of miR-21 by a specific antagomir inhibited interstitial fibrosis and attenuated cardiomyocyte hypertrophy and cardiac dysfunction in a mouse pressure overload (transverse aortic constriction, TAC) model [82]. Surprisingly, a miR-21 knockout mouse model did not show diminished cardiac hypertrophy or fibrosis in response to pressure overload or angiotensin-2 (AngII) infusion [83]. This might be explained by compensatory mechanisms that are activated in the persistent absence of miR-21, and since HF is a chronic disease, this will likely limit therapeutic applications targeting miR-21 [83]. Another miR, miR-29, was found to be downregulated in fibroblasts after MI and controls expression of ECM genes [84]. Overexpression of miR-29b in the mouse heart prevented AngII-mediated cardiac fibrosis, cardiomyocyte hypertrophy and cardiac dysfunction [85]. As described above, myofibroblast depletion, by Gli1 cell ablation, also attenuated both fibrosis and cardiomyocyte hypertrophy after aortic banding, resulting in improved cardiac function [55].
Together these studies provide clear evidence that myofibroblasts are important drivers of pathological cardiomyocyte hypertrophy. Hypertrophic stimuli activate apoptosis signal-regulating kinase 1 (ASK1) in cardiomyocytes in vitro and in vivo, which induces both apoptotic and necrotic cell death [86, 87]. In ASK1 transgenic mice, induction of the pro-apoptotic protein Bax was reported [88]. In a hamster cardiomyopathy model, ASK1 inhibition by gene transfer of a dominant negative kinase into cardiomyocytes not only prevented apoptosis, but also chamber dilation and preserved left ventricular (LV) systolic and diastolic function. Moreover, cardiac interstitial fibrosis was significantly inhibited [89]. Cathepsin B (CTSB), a lysosomal cysteine protease, participates in apoptosis and autophagy and is expressed in murine and human hearts and induced by hypertrophic stimuli [90]. Not surprisingly, knockout of CTSB in mice attenuated pressure-overload-induced apoptosis, cardiac hypertrophy, fibrosis and cardiac dysfunction. Deletion of CTSB also prevented the activation of ASK1 and attenuated the release of cytochrome c from mitochondria, which has pro-apoptotic actions in the cytosol [90]. Interestingly, a direct role for CTSB in matrix remodeling in the eye has been described via the upregulation and/or proteolytic activation of ECM-remodeling enzymes [91]. Whether this is also true in the heart is not known, but it is tempting to speculate that certain proteins may directly link and coordinate fibrogenic and cell death processes. Nix, another factor with pro-apoptotic and necrotic actions in the heart, is induced by Gαq-mediated hypertrophic stimuli [92, 93]. Cardiac-specific Nix ablation prevented cardiomyocyte apoptosis and myocardial fibrosis and cardiac decompensation after TAC [94]. A recent co-culture study using adult rat fibroblasts, myofibroblasts and cardiomyocytes showed that both fibroblasts and myofibroblasts directly affect cardiomyocyte cell viability [95]. The TGFBR1 inhibitor SB341542 prevented this loss of cardiomyocyte viability, although this was most likely not a direct effect of TGFβ. It has been suggested that this might be mediated via TGFβ-dependent upregulation of ET1 in (myo)fibroblasts. The latter has been shown to stimulate cardiomyocyte apoptosis [96]. Thus, myofibroblasts are essential to induce pathological cardiomyocyte hypertrophy that may culminate in cardiomyocyte cell death via specific cell death signaling pathways, and, at least in vitro, myofibroblasts can directly promote cardiomyocyte cell death.
The sustained fibrotic response
In normal wound healing, concomitant disappearance of myofibroblasts from the tissue marks the termination of the reparative response [97–100]. In many chronic diseases, including HF, a sustained fibrotic response is observed that further culminates in organ damage and finally organ failure. Apparently, at a certain stage of disease progression, a point of no return is reached and the fibrotic response cannot be downregulated anymore by the endogenous biological systems. The mechanisms behind this sustained response in the heart are multitude and include a positive feedback loop of fibroblast proliferation and FMT, inhibition of myofibroblast apoptosis, cardiomyocyte-mediated activation of fibroblasts and the presence of sustained low-grade systemic inflammation, as outlined below.
TGFβ plays an important role in fibroblast proliferation and FMT, and is produced in high amounts by myofibroblasts themselves resulting in a positive feedback loop. TGFβ therefore plays a central role in the sustained fibrotic response in the failing heart. TGFβ stimulates growth factor (EGF, IGF1)-mediated proliferation of fibroblast, and this probably also involves autocrine signaling via FGF2 and/or connective tissue growth factor (CTGF) [101, 102]. Inhibition of FGF2-induced fibroblast proliferation by TGFβ has also been described [103], indicating that this response is strongly dependent on the exact environmental factors. The increase in fibroblast numbers in the stressed heart indicates that in vivo this balance is shifted toward TGFβ-mediated fibroblast proliferation [49, 50].
TGFβ also prevents myofibroblast apoptosis via stimulation of PI3K/AKT pro-survival signaling pathway, and this is at least partly mediated via TGFβ-mediated secretion of ET1 [104]. The persistence of myofibroblasts can lead to nonresolving and progressive fibrosis, as exemplified by human idiopathic pulmonary fibrosis (IPF) [105, 106]. In pathological cardiac remodeling, persistent activation of the TGFβ pathway may therefore prevent myofibroblast apoptosis. This is consistent with the observation that myofibroblast can have very long life spans and continue secretion of pro-fibrotic factors and ECM proteins [107]. In vitro experiments using drugs targeting the TGFβ and MAPK pathways indicate that the myofibroblast phenotype can be reversed, but whether this also occurs in vivo and whether it can be stimulated in vivo is so far not known [108, 109].
In the heart, stressed cardiomyocytes themselves are important triggers of the fibrotic response of fibroblasts. Conditional, cardiomyocyte-specific knockout of Krüppel-like factor 6 (Klf6) in mice resulted in an attenuated fibrotic response after AngII infusion [110]. Surprisingly, a fibroblast-specific Klf6 knockout did not show this response. It was shown that Klf6 in cardiomyocytes controlled the expression of the ECM protein thrombospondin 4 (TSP4), which modulated activation of cardiac fibroblasts. This effect was specific for the AngII response and was not observed after aortic banding, indicating that under those conditions other factors are involved. Nevertheless, it indicates that as long as cardiomyocytes experience stress, these cells are able to produce factors that can induce and maintain a fibrotic response.
Inflammation is one of the main drivers of fibrosis and low-grade but persistent systemic inflammation is present in HF [111, 112]. Increased levels of cytokines and inflammatory biomarkers are present in patients, including TNFα, C-reactive protein (CRP), interleukin-6 (IL-6) and myeloid peroxidase (MPO), among others [113–117]. The precise mechanism of systemic inflammation in HF is unknown, but a growing body of evidence indicates that inflammation plays a role in the development and progression of HF and contributes to fibrosis. Cytokines, such as TNFα and interleukin-1β (IL-1β), are important activators of a variety of fibrotic diseases including cardiovascular diseases [118, 119]. TGFβ produced by myofibroblast may also play a role in cardiac inflammation. TGFβ has pleiotropic effects on the immune system and has both immunosuppressive and pro-inflammatory functions [120]. TGFβ can polarize macrophages and neutrophils toward a type II phenotype, which produces large quantities of inflammatory cytokines, including IL-6 and TGFβ. Inflammatory cytokines can activate cell death pathways and stimulate production of toxic reactive oxygen radicals (ROS) that can further exacerbate cardiac function. Moreover, systemic inflammation will not only affect myocardial function, but also other organs and therefore participate in the full manifestation of the complex HF syndrome [111].
Targeting fibrosis
The above data show that (myo)fibroblasts and fibrosis adversely affect cardiac function and directly and indirectly contribute to cardiomyocyte death. This will further amplify this adverse cycle, leading to more fibrosis and cardiomyocyte death hereby contributing to HF development. Animal studies have shown that cardiac fibrosis appears not to be an essential stress response under many circumstances, but does impair cardiac function. Removal of the fibrotic trigger(s) would therefore constitute a potential way to halt the progression of cardiac remodeling and hence provide a cardiac sparing effect and promote cardiac function. This begs the question whether inhibitors of fibroblast activation or fibrosis can interfere with the fibrosis-cell death axis and thereby stop the vicious cycle which eventually leads to HF. Components of the cycle that are potential targets to interrupt the fibrosis-cell death axis are ECM proteins, paracrine and inflammatory signals, and fibroblasts/myofibroblasts.
By targeting ECM proteins and enzymes, such as MMPs, LoxL and Gal-3, the production and processing of collagen can be influenced. Several studies revealed that MMP inhibition results in less myocardial fibrosis and improves diastolic function [56, 121]. MMP inhibition results in less LV dilatation, while collagen accumulation does not occur [56]. Inhibition of LoxL reduces both the degree of myocardial collagen buildup and collagen cross-linking and is associated with less LV dilatation and preserved cardiac function in a mouse model of MI [122]. Inhibition of Gal-3, a fibrotic HF marker and a component of the ECM, resulted in less fibrosis and preserved cardiac function in animal models of HF [123]. These studies indicate that targeting ECM proteins holds promise to modulate the fibrotic response and HF progression.
Blocking paracrine and inflammatory signals can break the fibrosis-cell death axis as well. Several studies have investigated the effects of TGFβ pathway inhibition on fibrosis formation. In animal models of MI, early TGFβ receptor inhibition resulted in increased mortality, whereas late inhibition resulted in reduced fibrosis, improved contraction in the infarct zone and improved survival [44]. In pressure overload models, TGFβ receptor inhibition attenuated cardiac fibrosis and also preserved cardiac function [44]. However, TGFβ receptor inhibitors also induced valve lesions in animal studies and increased aortic rupture in a mouse pressure overload model [124, 125]. These TGFβ receptor inhibitors may therefore have limited clinical use for the treatment of chronic diseases. Treatment with pirfenidone, an anti-fibrotic drug for the treatment of IPF, also reduced fibrosis in a pressure overload mouse model of HF and preserved LV function [45]. The exact mode of action of pirfenidone is not known, but most likely interferes with TGFβ-induced fibrogenesis [45]. As revealed from animal studies, interleukin-1 (IL-1) is a mediator of fibrosis, by recruiting myofibroblasts and induction of MMP expression [126]. Clinical trials with IL-1 receptor antagonist treatments in MI patients did, however, not show beneficial effects on cardiac function [126]. The latter illustrates that, due to the complexity of cytokine actions and differences in the exact mechanisms between species, extrapolation to the human situation is not so simple.
The discovery of fibroblast-specific microRNAs that control the fibrotic response opens new avenues to directly target (myo)fibroblasts [15, 81]. Although constitutive downregulation of the fibroblast-specific miR-21 resulted in apparent fibrotic compensatory mechanisms [83], investigating other miRs could be more rewarding. A recent study showed that miR-125b is another critical regulator of cardiac fibrosis [127]. These authors showed that miR-125b is both necessary and sufficient for the induction of FMT via targeting of apelin, a critical repressor of fibrogenesis. In addition, miR-125b inhibited p53 expression, allowing induction of fibroblast proliferation. The clinical inhibition of miR-125b may therefore represent a novel therapeutic approach for the treatment of human cardiac fibrosis. Rather than downregulating miR expression using antagomirs or locked nucleic acid (LNA) oligonucleotides, overexpression of particular miRs should also be considered. Overexpression of the fibroblast miR-29b in the mouse heart prevented cardiac fibrosis [85]. Thus, clinical strategies to enhance miR-29b levels in patients could provide a promising strategy.
Another innovative strategy that holds great promise is the reprogramming of cardiac myofibroblasts into cardiomyocytes [128]. The regenerative capacity of the heart is thought to be minimal, but by reprogramming myofibroblasts into cardiomyocytes, the effects of the fibrosis-cell death axis could be reversed, thereby offering a curative approach for HF. Song et al. [128] showed that adult mice fibroblasts could be directly reprogrammed into cardiac-like myocytes in vitro and in vivo, using the transcription factors GATA4, HAND2, MEF2C and TBX5 (GHMT). Novel cardiomyocytes were indentified in infarcted areas of mice treated with intramyocardial injections of GHMT, and preservation of cardiac function was observed. This same group showed that human fibroblasts can similarly be reprogrammed in vitro toward a cardiomyocyte-like fate [129]. Generation of induced cardiac-like myocytes (iCLMs) could potentially be a promising new approach to regenerate lost cardiomyocytes [130]. Nevertheless, numerous technical and biological hurdles, including efficiency issues and the immature cardiomyocyte phenotype, need to be overcome.
Discussion
HF is a major health problem in the Western world. Currently, the therapeutic approach toward HF mainly focuses on controlling symptoms and unloading the heart by reducing preload and afterload by treating HF patients with beta-blockers, angiotensin converting enzyme inhibitors (ACE-inhibitors), diuretics and aldosterone receptor antagonists [4, 5]. Although these drugs have shown beneficial effects in terms of relieving symptoms and reducing mortality [4, 5], prognosis for HF patients remains poor, with 5- and 10-year mortality rates of 50 and 90 %, respectively [131]. Current therapy reduces cardiac stress, but cardiac fibrosis is already present when most patients present themselves with symptoms at the clinic for the first time. Targeting the initial triggers, by unloading the heart, will slow down the vicious fibrosis-cell death cycle. However, it cannot eliminate the sustained fibrotic response present in the heart. Therefore, besides targeting the initial triggers, HF treatment should also focus on interrupting the fibrosis-cell death axis. As outlined in Fig. 3, we therefore believe that three pillars are important in HF therapy, namely unloading the heart, repressing fibrotic processes and improving cardiomyocyte function. Several ways to target myofibroblasts and fibrosis have been discussed above. We did not discuss the numerous studies that are aimed to improve cardiomyocyte function or limit cardiomyocyte death. Some interesting approaches that are under clinical investigation include the upregulation of the sarcoplasmatic reticulum calcium ATPase (SERCA2a) using gene therapy [132–134] and the use of myosin activators like omecamtiv mecarbil [135–137]. Whether apoptosis of cardiomyocytes can be inhibited at a clinical level, using caspase inhibitors or other cell death inhibitors needs to be awaited [138].

Suggested three pillars of heart failure treatment. Current standard heart failure (HF) therapy is focused at relief of the initial problem and aims at unloading the heart. Upon detection of HF, the sustained process of cardiac hypertrophy, fibrosis and cardiomyocyte cell death is already ongoing in most patients and cannot be stopped without additional treatment. We therefore suggest that to halt this sustained process, additional therapy will be required that blocks fibrotic processes and improves cardiomyocyte function. FMT fibroblasts to myofibroblasts transition, ECM extracellular matrix
It is difficult to elucidate whether fibrosis or cardiac cell death should be marked as the driver of the fibrosis-cell death axis, but it seems likely that both are important players. However, what can be concluded is that myofibroblasts plays a central role in the fibrotic-cell death axis, by secreting ECM components and autocrine and paracrine signaling molecules that drive sustained fibrosis, cardiomyocyte hypertrophy and inflammation. More research will be needed to identify and test clinical approaches that can halt this vicious cycle of cardiac fibrosis and cell death in HF.
References
Mouw JK, Ou G, Weaver VM (2014) Extracellular matrix assembly: a multiscale deconstruction. Nat Rev Mol Cell Biol 12:771–785
Bonnans C, Chou J, Werb Z (2014) Remodelling the extracellular matrix in development and disease. Nat Rev Mol Cell Biol 12:786–801
Rockey DC, Bell PD, Hill JA (2015) Fibrosis: a common pathway to organ injury and failure. N Engl J Med 12:1138–1149
McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Bohm M, Dickstein K, Falk V, Filippatos G, Fonseca C, Gomez-Sanchez MA et al (2012) ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 8:803–869
Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL et al (2013) 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 16:e147–e239
Mosterd A, Hoes AW (2007) Clinical epidemiology of heart failure. Heart 9:1137–1146
Sabbah HN, Goldstein S (1993) Ventricular remodelling: consequences and therapy. Eur Heart J 14:24–29
Brouwers FP, de Boer RA, van der Harst P, Voors AA, Gansevoort RT, Bakker SJ, Hillege HL, van Veldhuisen DJ, van Gilst WH (2013) Incidence and epidemiology of new onset heart failure with preserved vs. reduced ejection fraction in a community-based cohort: 11-year follow-up of PREVEND. Eur Heart J 19:1424–1431
Bernardo BC, Weeks KL, Pretorius L, McMullen JR (2010) Molecular distinction between physiological and pathological cardiac hypertrophy: experimental findings and therapeutic strategies. Pharmacol Ther 1:191–227
Weeks KL, McMullen JR (2011) The athlete’s heart vs. the failing heart: can signaling explain the two distinct outcomes? Physiology (Bethesda) 2:97–105
Maillet M, van Berlo JH, Molkentin JD (2013) Molecular basis of physiological heart growth: fundamental concepts and new players. Nat Rev Mol Cell Biol 1:38–48
Milting H, Jacob M, Kassner A, Heimann P, Mannherz HG, Becker G, Meyer HE, Bothig D, Arusoglu L, Morshuis M et al (2004) The structural examination of myocardial samples from patients with end-stage heart failure supported by ventricular assist devices using electron microscopy and amino acid analysis reveals low degree of reverse remodeling. J Heart Lung Transplant 4:396–404
Zeisberg M, Kalluri R (2013) Cellular mechanisms of tissue fibrosis. 1. Common and organ-specific mechanisms associated with tissue fibrosis. Am J Physiol Cell Physiol 3:C216–C225
n A, Frangogiannis NG (2011) Aging and cardiac fibrosis. Aging Dis 2:158–173
Creemers EE, Pinto YM (2011) Molecular mechanisms that control interstitial fibrosis in the pressure-overloaded heart. Cardiovasc Res 2:265–272
Segura AM, Frazier OH, Buja LM (2014) Fibrosis and heart failure. Heart Fail Rev 2:173–185
Weber KT, Brilla CG (1991) Pathological hypertrophy and cardiac interstitium. Fibrosis and renin-angiotensin-aldosterone system. Circulation 6:1849–1865
Kong P, Christia P, Frangogiannis NG (2014) The pathogenesis of cardiac fibrosis. Cell Mol Life Sci 4:549–574
Hein S, Arnon E, Kostin S, Schonburg M, Elsasser A, Polyakova V, Bauer EP, Klovekorn WP, Schaper J (2003) Progression from compensated hypertrophy to failure in the pressure-overloaded human heart: structural deterioration and compensatory mechanisms. Circulation 7:984–991
Ky B, French B, McCloskey K, Rame JE, McIntosh E, Shahi P, Dries DL, Tang WH, Wu AH, Fang JC et al (2011) High-sensitivity ST2 for prediction of adverse outcomes in chronic heart failure. Circ Heart Fail 2:180–187
de Boer RA, Lok DJ, Jaarsma T, van der Meer P, Voors AA, Hillege HL, van Veldhuisen DJ (2011) Predictive value of plasma galectin-3 levels in heart failure with reduced and preserved ejection fraction. Ann Med 1:60–68
Gaggin HK, Januzzi JL Jr (2013) Biomarkers and diagnostics in heart failure. Biochim Biophys Acta 12:2442–2450
Edelmann F, Holzendorf V, Wachter R, Nolte K, Schmidt AG, Kraigher-Krainer E, Duvinage A, Unkelbach I, Dungen HD, Tschope C et al (2015) Galectin-3 in patients with heart failure with preserved ejection fraction: results from the Aldo-DHF trial. Eur J Heart Fail 2:214–223
Lopez B, Gonzalez A, Ravassa S, Beaumont J, Moreno MU, San Jose G, Querejeta R, Diez J (2015) Circulating biomarkers of myocardial fibrosis: the need for a reappraisal. J Am Coll Cardiol 22:2449–2456
Kehat I, Molkentin JD (2010) Molecular pathways underlying cardiac remodeling during pathophysiological stimulation. Circulation 25:2727–2735
Chiong M, Wang ZV, Pedrozo Z, Cao DJ, Troncoso R, Ibacache M, Criollo A, Nemchenko A, Hill JA, Lavandero S (2011) Cardiomyocyte death: mechanisms and translational implications. Cell Death Dis 2:e244
Kakkar R, Lee RT (2010) Intramyocardial fibroblast myocyte communication. Circ Res 1:47–57
Weber KT, Sun Y, Bhattacharya SK, Ahokas RA, Gerling IC (2013) Myofibroblast-mediated mechanisms of pathological remodelling of the heart. Nat Rev Cardiol 1:15–26
Elmore S (2007) Apoptosis: a review of programmed cell death. Toxicol Pathol 4:495–516
van Empel VP, Bertrand AT, Hofstra L, Crijns HJ, Doevendans PA, De Windt LJ (2005) Myocyte apoptosis in heart failure. Cardiovasc Res 1:21–29
Kung G, Konstantinidis K, Kitsis RN (2011) Programmed necrosis, not apoptosis, in the heart. Circ Res 8:1017–1036
Nag AC (1980) Study of non-muscle cells of the adult mammalian heart: a fine structural analysis and distribution. Cytobios 109:41–61
Camelliti P, Borg TK, Kohl P (2005) Structural and functional characterisation of cardiac fibroblasts. Cardiovasc Res 1:40–51
Souders CA, Bowers SL, Baudino TA (2009) Cardiac fibroblast: the renaissance cell. Circ Res 12:1164–1176
Fu HL, Valiathan RR, Arkwright R, Sohail A, Mihai C, Kumarasiri M, Mahasenan KV, Mobashery S, Huang P, Agarwal G et al (2013) Discoidin domain receptors: unique receptor tyrosine kinases in collagen-mediated signaling. J Biol Chem 11:7430–7437
Labrador JP, Azcoitia V, Tuckermann J, Lin C, Olaso E, Manes S, Bruckner K, Goergen JL, Lemke G, Yancopoulos G et al (2001) The collagen receptor DDR2 regulates proliferation and its elimination leads to dwarfism. EMBO Rep 5:446–452
Tomasek JJ, Gabbiani G, Hinz B, Chaponnier C, Brown RA (2002) Myofibroblasts and mechano-regulation of connective tissue remodelling. Nat Rev Mol Cell Biol 5:349–363
Rifkin DB (2005) Latent transforming growth factor-beta (TGF-beta) binding proteins: orchestrators of TGF-beta availability. J Biol Chem 9:7409–7412
ten Dijke P, Arthur HM (2007) Extracellular control of TGFbeta signalling in vascular development and disease. Nat Rev Mol Cell Biol 11:857–869
Desmouliere A, Geinoz A, Gabbiani F, Gabbiani G (1993) Transforming growth factor-beta 1 induces alpha-smooth muscle actin expression in granulation tissue myofibroblasts and in quiescent and growing cultured fibroblasts. J Cell Biol 1:103–111
Hinz B (2007) Formation and function of the myofibroblast during tissue repair. J Investig Dermatol 3:526–537
Hinz B, Celetta G, Tomasek JJ, Gabbiani G, Chaponnier C (2001) Alpha-smooth muscle actin expression upregulates fibroblast contractile activity. Mol Biol Cell 9:2730–2741
Rosker C, Salvarani N, Schmutz S, Grand T, Rohr S (2011) Abolishing myofibroblast arrhythmogenicity by pharmacological ablation of alpha-smooth muscle actin containing stress fibers. Circ Res 10:1120–1131
Kapur NK (2011) Transforming growth factor-beta: governing the transition from inflammation to fibrosis in heart failure with preserved left ventricular function. Circ Heart Fail 1:5–7
Yamagami K, Oka T, Wang Q, Ishizu T, Lee JK, Miwa K, Akazawa H, Naito AT, Sakata Y, Komuro I (2015) Pirfenidone exhibits cardioprotective effects by regulating myocardial fibrosis and vascular permeability in pressure-overloaded hearts. Am J Physiol Heart Circ Physiol 3:H512–H522
Piera-Velazquez S, Li Z, Jimenez SA (2011) Role of endothelial-mesenchymal transition (EndoMT) in the pathogenesis of fibrotic disorders. Am J Pathol 3:1074–1080
van Meeteren LA, ten Dijke P (2012) Regulation of endothelial cell plasticity by TGF-beta. Cell Tissue Res 1:177–186
Zeisberg EM, Tarnavski O, Zeisberg M, Dorfman AL, McMullen JR, Gustafsson E, Chandraker A, Yuan X, Pu WT, Roberts AB et al (2007) Endothelial-to-mesenchymal transition contributes to cardiac fibrosis. Nat Med 8:952–961
Moore-Morris T, Guimaraes-Camboa N, Banerjee I, Zambon AC, Kisseleva T, Velayoudon A, Stallcup WB, Gu Y, Dalton ND, Cedenilla M et al (2014) Resident fibroblast lineages mediate pressure overload-induced cardiac fibrosis. J Clin Investig 7:2921–2934
Ali SR, Ranjbarvaziri S, Talkhabi M, Zhao P, Subat A, Hojjat A, Kamran P, Muller AM, Volz KS, Tang Z et al (2014) Developmental heterogeneity of cardiac fibroblasts does not predict pathological proliferation and activation. Circ Res 7:625–635
de Lange FJ, Moorman AF, Anderson RH, Manner J, Soufan AT, de Gier-de Vries C, Schneider MD, Webb S, van den Hoff MJ, Christoffels VM (2004) Lineage and morphogenetic analysis of the cardiac valves. Circ Res 6:645–654
Lincoln J, Alfieri CM, Yutzey KE (2004) Development of heart valve leaflets and supporting apparatus in chicken and mouse embryos. Dev Dyn 2:239–250
Ogawa M, LaRue AC, Drake CJ (2006) Hematopoietic origin of fibroblasts/myofibroblasts: its pathophysiologic implications. Blood 9:2893–2896
van Amerongen MJ, Bou-Gharios G, Popa E, van Ark J, Petersen AH, van Dam GM, van Luyn MJ, Harmsen MC (2008) Bone marrow-derived myofibroblasts contribute functionally to scar formation after myocardial infarction. J Pathol 3:377–386
Kramann R, Schneider RK, DiRocco DP, Machado F, Fleig S, Bondzie PA, Henderson JM, Ebert BL, Humphreys BD (2015) Perivascular Gli1 + progenitors are key contributors to injury-induced organ fibrosis. Cell Stem Cell 1:51–66
Spinale FG (2007) Myocardial matrix remodeling and the matrix metalloproteinases: influence on cardiac form and function. Physiol Rev 4:1285–1342
Barton PJ, Birks EJ, Felkin LE, Cullen ME, Koban MU, Yacoub MH (2003) Increased expression of extracellular matrix regulators TIMP1 and MMP1 in deteriorating heart failure. J Heart Lung Transplant 7:738–744
Lu B, Yu H, Zwartbol M, Ruifrok WP, van Gilst WH, de Boer RA, Sillje HH (2012) Identification of hypertrophy-and heart failure-associated genes by combining in vitro and in vivo models. Physiol Genom 8:443–454
Herum KM, Lunde IG, Skrbic B, Louch WE, Hasic A, Boye S, Unger A, Brorson SH, Sjaastad I, Tonnessen T et al (2015) Syndecan-4 is a key determinant of collagen cross-linking and passive myocardial stiffness in the pressure-overloaded heart. Cardiovasc Res 2:217–226
Lopez B, Gonzalez A, Lindner D, Westermann D, Ravassa S, Beaumont J, Gallego I, Zudaire A, Brugnolaro C, Querejeta R et al (2013) Osteopontin-mediated myocardial fibrosis in heart failure: a role for lysyl oxidase? Cardiovasc Res 1:111–120
Lu P, Takai K, Weaver VM, Werb Z (2011) Extracellular matrix degradation and remodeling in development and disease. Cold Spring Harb Perspect Biol. doi:10.1101/cshperspect.a005058
Brown RD, Ambler SK, Mitchell MD, Long CS (2005) The cardiac fibroblast: therapeutic target in myocardial remodeling and failure. Annu Rev Pharmacol Toxicol 45:657–687
Verheule S, Sato T, Everett T 4th, Engle SK, Otten D, Rubart-von der Lohe M, Nakajima HO, Nakajima H, Field LJ, Olgin JE (2004) Increased vulnerability to atrial fibrillation in transgenic mice with selective atrial fibrosis caused by overexpression of TGF-beta1. Circ Res 11:1458–1465
Everett TH 4th, Olgin JE (2007) Atrial fibrosis and the mechanisms of atrial fibrillation. Heart Rhythm 3(Suppl):S24–S27
Kostin S, Klein G, Szalay Z, Hein S, Bauer EP, Schaper J (2002) Structural correlate of atrial fibrillation in human patients. Cardiovasc Res 2:361–379
Burstein B, Nattel S (2008) Atrial fibrosis: mechanisms and clinical relevance in atrial fibrillation. J Am Coll Cardiol 8:802–809
De Jong AM, Maass AH, Oberdorf-Maass SU, Van Veldhuisen DJ, Van Gilst WH, Van Gelder IC (2011) Mechanisms of atrial structural changes caused by stretch occurring before and during early atrial fibrillation. Cardiovasc Res 4:754–765
Burchfield JS, Xie M, Hill JA (2013) Pathological ventricular remodeling: mechanisms: part 1 of 2. Circulation 4:388–400
Rudolph V, Andrie RP, Rudolph TK, Friedrichs K, Klinke A, Hirsch-Hoffmann B, Schwoerer AP, Lau D, Fu X, Klingel K et al (2010) Myeloperoxidase acts as a profibrotic mediator of atrial fibrillation. Nat Med 4:470–474
Heijman J, Voigt N, Nattel S, Dobrev D (2014) Cellular and molecular electrophysiology of atrial fibrillation initiation, maintenance, and progression. Circ Res 9:1483–1499
Tsagalou EP, Anastasiou-Nana M, Agapitos E, Gika A, Drakos SG, Terrovitis JV, Ntalianis A, Nanas JN (2008) Depressed coronary flow reserve is associated with decreased myocardial capillary density in patients with heart failure due to idiopathic dilated cardiomyopathy. J Am Coll Cardiol 17:1391–1398
De Boer MP, Meijer RI, Wijnstok NJ, Jonk AM, Houben AJ, Stehouwer CD, Smulders YM, Eringa EC, Serne EH (2012) Microvascular dysfunction: a potential mechanism in the pathogenesis of obesity-associated insulin resistance and hypertension. Microcirculation 1:5–18
Bogoyevitch MA, Glennon PE, Andersson MB, Clerk A, Lazou A, Marshall CJ, Parker PJ, Sugden PH (1994) Endothelin-1 and fibroblast growth factors stimulate the mitogen-activated protein kinase signaling cascade in cardiac myocytes. The potential role of the cascade in the integration of two signaling pathways leading to myocyte hypertrophy. J Biol Chem 2:1110–1119
Kaye D, Pimental D, Prasad S, Maki T, Berger HJ, McNeil PL, Smith TW, Kelly RA (1996) Role of transiently altered sarcolemmal membrane permeability and basic fibroblast growth factor release in the hypertrophic response of adult rat ventricular myocytes to increased mechanical activity in vitro. J Clin Investig 2:281–291
Pellieux C, Foletti A, Peduto G, Aubert JF, Nussberger J, Beermann F, Brunner HR, Pedrazzini T (2001) Dilated cardiomyopathy and impaired cardiac hypertrophic response to angiotensin II in mice lacking FGF-2. J Clin Investig 12:1843–1851
Virag JA, Rolle ML, Reece J, Hardouin S, Feigl EO, Murry CE (2007) Fibroblast growth factor-2 regulates myocardial infarct repair: effects on cell proliferation, scar contraction, and ventricular function. Am J Pathol 5:1431–1440
House SL, House BE, Glascock B, Kimball T, Nusayr E, Schultz JE, Doetschman T (2010) Fibroblast growth factor 2 mediates isoproterenol-induced cardiac hypertrophy through activation of the extracellular regulated kinase. Mol Cell Pharmacol 4:143–154
Ma F, Li Y, Jia L, Han Y, Cheng J, Li H, Qi Y, Du J (2012) Macrophage-stimulated cardiac fibroblast production of IL-6 is essential for TGF beta/Smad activation and cardiac fibrosis induced by angiotensin II. PLoS ONE 5:e35144
Melendez GC, McLarty JL, Levick SP, Du Y, Janicki JS, Brower GL (2010) Interleukin 6 mediates myocardial fibrosis, concentric hypertrophy, and diastolic dysfunction in rats. Hypertension 2:225–231
Takeda N, Manabe I, Uchino Y, Eguchi K, Matsumoto S, Nishimura S, Shindo T, Sano M, Otsu K, Snider P et al (2010) Cardiac fibroblasts are essential for the adaptive response of the murine heart to pressure overload. J Clin Investig 1:254–265
Thum T (2014) Noncoding RNAs and myocardial fibrosis. Nat Rev Cardiol 11:655–663
Thum T, Gross C, Fiedler J, Fischer T, Kissler S, Bussen M, Galuppo P, Just S, Rottbauer W, Frantz S et al (2008) MicroRNA-21 contributes to myocardial disease by stimulating MAP kinase signalling in fibroblasts. Nature 7224:980–984
Patrick DM, Montgomery RL, Qi X, Obad S, Kauppinen S, Hill JA, van Rooij E, Olson EN (2010) Stress-dependent cardiac remodeling occurs in the absence of microRNA-21 in mice. J Clin Investig 11:3912–3916
van Rooij E, Sutherland LB, Thatcher JE, DiMaio JM, Naseem RH, Marshall WS, Hill JA, Olson EN (2008) Dysregulation of microRNAs after myocardial infarction reveals a role of miR-29 in cardiac fibrosis. Proc Natl Acad Sci USA 35:13027–13032
Zhang Y, Huang XR, Wei LH, Chung AC, Yu CM, Lan HY (2014) miR-29b as a therapeutic agent for angiotensin II-induced cardiac fibrosis by targeting TGF-beta/Smad3 signaling. Mol Ther 5:974–985
Yamaguchi O, Higuchi Y, Hirotani S, Kashiwase K, Nakayama H, Hikoso S, Takeda T, Watanabe T, Asahi M, Taniike M et al (2003) Targeted deletion of apoptosis signal-regulating kinase 1 attenuates left ventricular remodeling. Proc Natl Acad Sci USA 26:15883–15888
Watanabe T, Otsu K, Takeda T, Yamaguchi O, Hikoso S, Kashiwase K, Higuchi Y, Taniike M, Nakai A, Matsumura Y et al (2005) Apoptosis signal-regulating kinase 1 is involved not only in apoptosis but also in non-apoptotic cardiomyocyte death. Biochem Biophys Res Commun 2:562–567
Liu Q, Sargent MA, York AJ, Molkentin JD (2009) ASK1 regulates cardiomyocyte death but not hypertrophy in transgenic mice. Circ Res 11:1110–1117
Hikoso S, Ikeda Y, Yamaguchi O, Takeda T, Higuchi Y, Hirotani S, Kashiwase K, Yamada M, Asahi M, Matsumura Y et al (2007) Progression of heart failure was suppressed by inhibition of apoptosis signal-regulating kinase 1 via transcoronary gene transfer. J Am Coll Cardiol 5:453–462
Wu QQ, Xu M, Yuan Y, Li FF, Yang Z, Liu Y, Zhou MQ, Bian ZY, Deng W, Gao L et al (2015) Cathepsin B deficiency attenuates cardiac remodeling in response to pressure overload via TNF-alpha/ASK1/JNK pathway. Am J Physiol Heart Circ Physiol 9:H1143–H1154
Porter K, Lin Y, Liton PB (2013) Cathepsin B is up-regulated and mediates extracellular matrix degradation in trabecular meshwork cells following phagocytic challenge. PLoS ONE 7:e68668
Galvez AS, Brunskill EW, Marreez Y, Benner BJ, Regula KM, Kirschenbaum LA, Dorn GW 2nd (2006) Distinct pathways regulate proapoptotic Nix and BNip3 in cardiac stress. J Biol Chem 3:1442–1448
Dorn GW 2nd (2011) Nix Nought Nothing: fairy tale or real deal. J Mol Cell Cardiol 4:497–500
Diwan A, Wansapura J, Syed FM, Matkovich SJ, Lorenz JN, Dorn GW 2nd (2008) Nix-mediated apoptosis links myocardial fibrosis, cardiac remodeling, and hypertrophy decompensation. Circulation 3:396–404
Cartledge JE, Kane C, Dias P, Tesfom M, Clarke L, Mckee B, Al Ayoubi S, Chester A, Yacoub MH, Camelliti P et al (2015) Functional crosstalk between cardiac fibroblasts and adult cardiomyocytes by soluble mediators. Cardiovasc Res 3:260–270
Ren A, Yan X, Lu H, Shi J, Yin Y, Bai J, Yuan W, Lin L (2008) Antagonism of endothelin-1 inhibits hypoxia-induced apoptosis in cardiomyocytes. Can J Physiol Pharmacol 8:536–540
Desmouliere A, Redard M, Darby I, Gabbiani G (1995) Apoptosis mediates the decrease in cellularity during the transition between granulation tissue and scar. Am J Pathol 1:56–66
Hinz B, Phan SH, Thannickal VJ, Prunotto M, Desmouliere A, Varga J, De Wever O, Mareel M, Gabbiani G (2012) Recent developments in myofibroblast biology: paradigms for connective tissue remodeling. Am J Pathol 4:1340–1355
Gabbiani G (2003) The myofibroblast in wound healing and fibrocontractive diseases. J Pathol 4:500–503
Iredale JP, Benyon RC, Pickering J, McCullen M, Northrop M, Pawley S, Hovell C, Arthur MJ (1998) Mechanisms of spontaneous resolution of rat liver fibrosis. Hepatic stellate cell apoptosis and reduced hepatic expression of metalloproteinase inhibitors. J Clin Investig 3:538–549
Strutz F, Zeisberg M, Renziehausen A, Raschke B, Becker V, van Kooten C, Muller G (2001) TGF-beta 1 induces proliferation in human renal fibroblasts via induction of basic fibroblast growth factor (FGF-2). Kidney Int 2:579–592
Grotendorst GR, Rahmanie H, Duncan MR (2004) Combinatorial signaling pathways determine fibroblast proliferation and myofibroblast differentiation. FASEB J 3:469–479
Sigel AV, Centrella M, Eghbali-Webb M (1996) Regulation of proliferative response of cardiac fibroblasts by transforming growth factor-beta 1. J Mol Cell Cardiol 9:1921–1929
Kulasekaran P, Scavone CA, Rogers DS, Arenberg DA, Thannickal VJ, Horowitz JC (2009) Endothelin-1 and transforming growth factor-beta1 independently induce fibroblast resistance to apoptosis via AKT activation. Am J Respir Cell Mol Biol 4:484–493
Thannickal VJ, Horowitz JC (2006) Evolving concepts of apoptosis in idiopathic pulmonary fibrosis. Proc Am Thorac Soc 4:350–356
Ding Q, Luckhardt T, Hecker L, Zhou Y, Liu G, Antony VB, deAndrade J, Thannickal VJ (2011) New insights into the pathogenesis and treatment of idiopathic pulmonary fibrosis. Drugs 8:981–1001
Gabbiani G (1996) The cellular derivation and the life span of the myofibroblast. Pathol Res Pract 7:708–711
Driesen RB, Nagaraju CK, Abi-Char J, Coenen T, Lijnen PJ, Fagard RH, Sipido KR, Petrov VV (2014) Reversible and irreversible differentiation of cardiac fibroblasts. Cardiovasc Res 3:411–422
Kosla J, Dvorakova M, Dvorak M, Cermak V (2013) Effective myofibroblast dedifferentiation by concomitant inhibition of TGF-beta signaling and perturbation of MAPK signaling. Eur J Cell Biol 12:363–373
Sawaki D, Hou L, Tomida S, Sun J, Zhan H, Aizawa K, Son BK, Kariya T, Takimoto E, Otsu K et al (2015) Modulation of cardiac fibrosis by Kruppel-like factor 6 through transcriptional control of thrombospondin 4 in cardiomyocytes. Cardiovasc Res 4:420–430
Oikonomou E, Tousoulis D, Siasos G, Zaromitidou M, Papavassiliou AG, Stefanadis C (2011) The role of inflammation in heart failure: new therapeutic approaches. Hell J Cardiol 1:30–40
Anker SD, von Haehling S (2004) Inflammatory mediators in chronic heart failure: an overview. Heart 4:464–470
Seta Y, Shan K, Bozkurt B, Oral H, Mann DL (1996) Basic mechanisms in heart failure: the cytokine hypothesis. J Card Fail 3:243–249
Anand IS, Latini R, Florea VG, Kuskowski MA, Rector T, Masson S, Signorini S, Mocarelli P, Hester A, Glazer R et al (2005) C-reactive protein in heart failure: prognostic value and the effect of valsartan. Circulation 10:1428–1434
Tsutamoto T, Hisanaga T, Wada A, Maeda K, Ohnishi M, Fukai D, Mabuchi N, Sawaki M, Kinoshita M (1998) Interleukin-6 spillover in the peripheral circulation increases with the severity of heart failure, and the high plasma level of interleukin-6 is an important prognostic predictor in patients with congestive heart failure. J Am Coll Cardiol 2:391–398
Levine B, Kalman J, Mayer L, Fillit HM, Packer M (1990) Elevated circulating levels of tumor necrosis factor in severe chronic heart failure. N Engl J Med 4:236–241
Tang WH, Brennan ML, Philip K, Tong W, Mann S, Van Lente F, Hazen SL (2006) Plasma myeloperoxidase levels in patients with chronic heart failure. Am J Cardiol 6:796–799
Ferrari R (1999) The role of TNF in cardiovascular disease. Pharmacol Res 2:97–105
Bujak M, Frangogiannis NG (2009) The role of IL-1 in the pathogenesis of heart disease. Arch Immunol Ther Exp (Warsz) 3:165–176
Travis MA, Sheppard D (2014) TGF-beta activation and function in immunity. Annu Rev Immunol 32:51–82
Jayasankar V, Woo YJ, Bish LT, Pirolli TJ, Berry MF, Burdick J, Bhalla RC, Sharma RV, Gardner TJ, Sweeney HL (2004) Inhibition of matrix metalloproteinase activity by TIMP-1 gene transfer effectively treats ischemic cardiomyopathy. Circulation 110(11 Suppl 1):II-180
González-Santamaría J, Villalba M, Busnadiego O, López-Olañeta MM, Sandoval P, Snabel J, López-Cabrera M, Erler JT, Hanemaaijer R, Lara-Pezzi E, Rodríguez-Pascual F (2016) Matrix cross-linking lysyl oxidases are induced in response to myocardial infarction and promote cardiac dysfunction. Cardiovasc Res 109(1):67–78
Yu L, Ruifrok WP, Meissner M, Bos EM, van Goor H, Sanjabi B, van der Harst P, Pitt B, Goldstein IJ, Koerts JA et al (2013) Genetic and pharmacological inhibition of galectin-3 prevents cardiac remodeling by interfering with myocardial fibrogenesis. Circ Heart Fail 1:107–117
Anderton MJ, Mellor HR, Bell A, Sadler C, Pass M, Powell S, Steele SJ, Roberts RR, Heier A (2011) Induction of heart valve lesions by small-molecule ALK5 inhibitors. Toxicol Pathol 6:916–924
Engebretsen KV, Skardal K, Bjornstad S, Marstein HS, Skrbic B, Sjaastad I, Christensen G, Bjornstad JL, Tonnessen T (2014) Attenuated development of cardiac fibrosis in left ventricular pressure overload by SM16, an orally active inhibitor of ALK5. J Mol Cell Cardiol 76:148–157
Turner NA (2014) Effects of interleukin-1 on cardiac fibroblast function: relevance to post-myocardial infarction remodelling. Vasc Pharmacol 1:1–7
Nagpal V, Rai R, Place AT, Murphy SB, Verma SK, Ghosh AK, Vaughan DE (2015) MiR-125b is critical for fibroblast-to-myofibroblast transition and cardiac fibrosis. Circulation 133(3):291–301
Song K, Nam YJ, Luo X, Qi X, Tan W, Huang GN, Acharya A, Smith CL, Tallquist MD, Neilson EG et al (2012) Heart repair by reprogramming non-myocytes with cardiac transcription factors. Nature 7400:599–604
Nam YJ, Song K, Luo X, Daniel E, Lambeth K, West K, Hill JA, DiMaio JM, Baker LA, Bassel-Duby R et al (2013) Reprogramming of human fibroblasts toward a cardiac fate. Proc Natl Acad Sci USA 14:5588–5593
Nam YJ, Song K, Olson EN (2013) Heart repair by cardiac reprogramming. Nat Med 4:413–415
Roger VL (2013) Epidemiology of heart failure. Circ Res 6:646–659
Gwathmey JK, Yerevanian A, Hajjar RJ (2013) Targeting sarcoplasmic reticulum calcium ATPase by gene therapy. Hum Gene Ther 11:937–947
Miyamoto MI, del Monte F, Schmidt U, DiSalvo TS, Kang ZB, Matsui T, Guerrero JL, Gwathmey JK, Rosenzweig A, Hajjar RJ (2000) Adenoviral gene transfer of SERCA2a improves left-ventricular function in aortic-banded rats in transition to heart failure. Proc Natl Acad Sci USA 2:793–798
Jessup M, Greenberg B, Mancini D, Cappola T, Pauly DF, Jaski B, Yaroshinsky A, Zsebo KM, Dittrich H, Hajjar RJ et al (2011) Calcium Upregulation by Percutaneous Administration of Gene Therapy in Cardiac Disease (CUPID): a phase 2 trial of intracoronary gene therapy of sarcoplasmic reticulum Ca2+-ATPase in patients with advanced heart failure. Circulation 3:304–313
Teerlink JR (2009) A novel approach to improve cardiac performance: cardiac myosin activators. Heart Fail Rev 4:289–298
Malik FI, Morgan BP (2011) Cardiac myosin activation part 1: from concept to clinic. J Mol Cell Cardiol 4:454–461
Liu LC, Dorhout B, van der Meer P, Teerlink JR, Voors AA (2016) Omecamtiv mecarbil: a novel cardiac myosin activator for the treatment of heart failure. Expert Opin Investig Drugs 25:117–127
Park M, Vatner SF, Yan L, Gao S, Yoon S, Lee GJ, Xie LH, Kitsis RN, Vatner DE (2013) Novel mechanisms for caspase inhibition protecting cardiac function with chronic pressure overload. Basic Res Cardiol 108:324
Acknowledgments
We like to thank Weijie Du for providing pictures of Masson trichrome-stained cardiac tissue.
Funding
R. A. de Boer was supported by the Innovational Research Incentives Scheme program of the Netherlands Organization for Scientific Research [Vidi grant 917.13.350].
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
A. Piek, R. A. de Boer and H. H. W. Silljé declare that they have no conflict of interest.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Piek, A., de Boer, R.A. & Silljé, H.H.W. The fibrosis-cell death axis in heart failure. Heart Fail Rev 21, 199–211 (2016). https://doi.org/10.1007/s10741-016-9536-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10741-016-9536-9