
Abstract
Objective
To study the influence of glazing on strength repair of lithium disilicate glass–ceramics after defect incorporation in different production processing phases.
Materials and methods
Bar-shaped specimens (1 × 1 × 12 mm, n = 280; 20/group) made from different lithium disilicate ceramics (IPS e.max CAD, Ivoclar, “LD” or advanced lithium disilicate CEREC Tessera, Dentsply Sirona, “ALD”) were exposed to 7 different protocols: crystallized without (c) and with glaze layer (cg), with a defect incorporated before crystallization without (ic) and with glaze layer (icg), with a defect after crystallization without (ci) or with glaze layer (cig), and defect incorporated after the glaze layer (cgi). The flexural strength was determined using the three-point bending test. Analysis of indented areas and fractured specimens was performed by scanning electron microscopy. Flexural strength data were evaluated by two-way ANOVA followed by Tukey tests (α = 5%).
Results
Two-way ANOVA revealed a significant influence of ceramic (p < 0.001; F = 55.45), protocol (p < 0.001; F = 56.94), and the interaction protocol*ceramic (p < 0.001; F = 13.86). Regardless of ceramics, defect incorporation as final step resulted in the worst strength, while defects introduced before crystallization did not reduce strength. Glaze firing after defect incorporation led to strength repair for ALD, whereas such an effect was not evident for LD.
Conclusions
The advanced lithium disilicate must receive a glaze layer to achieve its highest strength. Defects incorporated in the pre-crystallized stage can be healed during crystallization. Defects should not be incorporated after glazing.
Clinical relevance
Clinical adjustments should be performed on pre-crystallized or crystalized restorations that receive a glazer layer afterwards.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Reinforced glass–ceramics have passed through improvements leading to materials that combine sufficient strength and esthetics. These biomimetic characteristics have been missed for a long time in the first generation of zirconia and glass–ceramics, respectively. However, with the contemporary processing methods and material composition, it is possible to successfully rehabilitate damaged teeth using these synthetic materials. In addition, glass–ceramics present a high amount of glassy phase that allows its surface conditioning with acid etching promoting suitable bond strength to different substrates [1].
One of the most common reinforced glass–ceramic materials available for dental application is lithium disilicate reinforced glass–ceramic (LD). LD can be milled or heat-pressed in different restoration designs, making it widely popular for many dental applications, e.g., anterior and posterior crowns, implant-supported prosthesis, abutments, inlays, onlays, occlusal veneers, veneers, and ultrathin veneers [2]. LD restoration showed a high success rate of more than 90% in short- and mid-term observation [3,4,5]. However, long-term studies of 15 years reveal lower survival rates regarding single crown (81.9%) [6], posterior three-unit fixed prostheses (48.6%) [7], and posterior inlay-retained prostheses (22%) [8]. Specifically, fracture emerged as the main cause of failure at the later stage, according to studies on lithium disilicate restorations manufactured from IPS e.max Press developed by Ivoclar [7, 8].
Every clinician aims for a restorative material that combines suitable mechanical and optical properties to mimic the natural teeth. This is possible for LD that is available in different translucencies and has the indication to rehabilitate innumerous clinical situations. However, during the oral try-in of the restoration, adjustments are sometimes necessary [9]. For LD, this procedure can be done before [10] and after [3] final crystallization, including internal and marginal adaptation, proximal contact, and occlusion. Usually, diamond burs are indicated to adjust the restoration, while silicone diamond burs can be used as the following step to polish the adjusted area, since it is well-known that the surface roughness is directly related to biofilm formation [11] and slow crack growth when the ceramic is submitted to fatigue in the oral medium [12]. Other clinicians opt to prove the restoration and perform grinding adjustments and the cementation procedure in a single-time visit [13]. However, it is not well-known if there is any deleterious effect in performing the adjustments after crystallization or glazing, which raises the question of which moment the restoration adjustment procedure should be performed when necessary not to decrease the material’s strength. In addition to the clinical adjustment by dentists, there are other possible situations in which defects can be incorporated in the ceramic surface, e.g., the milling process (before crystallization) [14] and support removal after milling (before crystallization) [15], as well as chewing and biting during a long period of service (after the glaze firing) [16]. Therefore, it is worthwhile to understand the effect of defect incorporation moment on the mechanical behavior of restorations.
To overcome the deleterious effect of surface defects, an advanced lithium disilicate (ALD) has been developed with the claim that possible surface defects or hairline fractures could be healed after a short crystallization firing [17]. Compared with conventional LD, ALD shows a different phase composition after mandatory firing, including 40% less Li2Si2O5, approximately twice as much residual glass and the presence of quartz-like phases (3.7 vol%) [18]. In addition, a smaller microstructural size was observed for ALD after acid etching [19], indicating a potentially significant difference in their mechanical performance. However, the relevant literature on the properties of this new material in comparison with conventional LD is currently limited. Moreover, according to the manufacturer, a glaze layer is necessary for the firing process to achieve its final strength. As a consequence, clinical adjustments are recommended to be performed after glazing.
Flexural strength is an essential mechanical property for dental ceramic materials. It determines whether the restoration can withstand occlusal forces and plays a critical role in the survival of restorations. Based on the strength test, indentation strength is another important technique to understand the mechanical properties of ceramic materials [10]. It incorporates controlled flaws with standardized shape and size and eliminates the influence of other defects on the results [20]. In this study, a Vickers indenter was used to introduce the flaw and simulate the surface damage in the restoration at various moments simulating different situations: before crystallization, after crystallization and before the glaze firing, and after the glaze firing. Therefore, this study was aimed at assessing the influence of defect incorporation and glazing on the flexural strength of two lithium disilicates. The null hypothesis is that the moment of defect incorporation would not affect the flexural strength of LD and ALD regardless of glaze firing.
Materials and methods
Specimen’s preparation
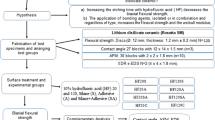
One hundred and forty bar-shaped specimens (1 × 1 × 12 mm ± 0.2) [21,22,23] were obtained from each lithium disilicate glass–ceramic: “IPS e.max CAD” (LD; batch number: Y52153; Ivoclar, Lichtenstein) and “CEREC Tessera” (ALD; batch number: 16011535; Dentsply Sirona, Germany) using a diamond-coated saw in a precision cutting machine (IsoMet 1000; Buehler, Lake Bluff, IL). All specimens were polished until the final dimension using SiC abrasive papers (Ecomet; Buehler Ltd., Evanston, IL) with grit sizes of P800 and P1200. Then, the specimens were submitted to different clinical simulations summarized in Fig. 1. The brand names of all the materials and their compositions are presented in Table 1, and the firing protocols including mandatory firing of the evaluated CAD/CAM lithium disilicate glass–ceramics as well as the glazing procedure are shown in Table 2.

The study’s design of five protocols to simulate different moments for defect incorporation (before or after crystallization and/or glaze firing) compared to two situations without defect incorporation. The 1st and 2nd protocols were respectively conventional crystallization firing without (c) and with a glaze layer (cg) without defect incorporation. In the 3rd and 4th protocols, the defect was incorporated before crystallization firing, while one group did not receive a glaze layer (ic) and the other received (icg). The 5th and 6th groups received a defect after crystallization firing, without (ci) or with a glaze layer (cig) in sequence. Finally, the latest condition is simulated defects incorporated after the glaze layer application (cgi). All protocols have been simulated for both materials (LD and ALD)
To simulate the incorporation of a defect, an indentation was performed in the middle of the tensile side of each specimen, using a Vickers indenter with a 19.6 N load for 15 s (HM-124 Hardness Testing Machine, Mitutoyo Corp., Kanagawa, Japan). Considering the length of the generated damage, the defect length and depth had an average size of 73 µm and 14 µm, respectively.
Flexural strength
Twenty specimens (n = 20) from each group were submitted to a 3-point bending test with a universal testing machine (Instron 6022; Instron Limited, High Wycombe, UK). The load was applied on the middle of the surface using a load cell (1000 N) with a crosshead speed of 0.5 mm/min. Flexural strength (MPa) was calculated according to the following equation based on ISO 6872–2015:
where P is the maximum load (in N), l is the distance between the two supports (in mm), b represents the specimen width (in mm), and h is the specimen thickness (in mm).
Scanning electron microscopy (SEM)
All the fractured specimens were submitted to the fractographic analysis. The fractured surfaces were examined under SEM (EVO LS15; Carl Zeiss, Oberkochen, Germany) at × 165 and × 500 magnifications to identify the fracture origin. In addition, representative specimen per group was also evaluated under SEM at × 1000 magnification for the indented area. All the specimens received a gold coat in a low-pressure atmosphere using an ion sputter coater.
Data analysis
Flexural strength data were submitted to one- and two-way analyses of variance (ANOVA) followed by Tukey tests (α = 5%). One-way ANOVA was applied to compare the mean values of all subgroups within each material. Two-way ANOVA was used to evaluate the effect of materials and protocols on strength as well as the interaction between factors. In addition, the strength data were also used to identify the Weibull distribution for each group using maximum likelihood method with 95% confidence interval.
Results
Flexural strength
Table 3 and Fig. 2 present the mean flexural strength value and standard deviation of each group according to each material. Two-way ANOVA revealed a significant influence caused by ceramic (p < 0.001; F = 55.45) and protocol (p < 0.001; F = 56.94) ceramics. In addition, the grouping comparing all groups is presented since the interaction protocol*ceramic has also presented statistical significance (p < 0.001; F = 13.86).

Mean flexural strength and standard deviation according to the ceramic material and moment of defect incorporation
Based on Tukey results, considering the strength of unaffected materials during production phases, crystallized LD is stronger than ALD (p < 0.001). After glazing, LD became weaker (p < 0.001) while ALD strength increases (p < 0.001). There was no significant difference between ALDcg and LDcg (p = 0.154). Regarding the influence of the defect incorporation moment in the production process, the defect incorporation as the final step (ci, cgi) resulted in the worst strength for both ceramics. However, no difference was found between ALDcgi and LDcgi (p = 0.057). In addition, defects introduced before crystallization (ic) did not reduce the crystallized materials’ strength for LD (p = 0.290) and ALD (p = 1.000). Observing the glaze effect, ALDcig was stronger than the corresponding groups without glaze firing (ALDci, p < 0.001) and similar to ALDcg (p = 0.282); ALDicg was also stronger than ALDic (p = 0.011) and similar to ALDcg (p = 1.000). For LDcg, the similarity was found with ic and icg (p = 0.396).
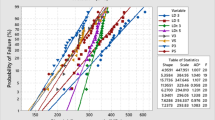
According to Weibull 95% CI (Fig. 3), it was possible to observe that LD groups were more sensitive to the simulated protocols when compared to ALD groups since the Weibull modulus of LD ranged from 3.6 to 5.5 while that of ALD ranges from 3.8 to 7.7. The probability plot revealed that ALDcg and LDic presented the highest reliability for flexural strength values, while icg protocol showed the lowest reliability for both materials.

Weibull 95% confidence interval (CI) plots for LD (A) and ALD (B) groups
Fractography
According to the fractographic analysis, the defects were not visible when the indentation was performed before crystallization (ic) or crystallization and glaze layer application (icg and cig), while in groups in which the defect was incorporated as the last step, the defect was clearly visible (ci and cgi). Finally, the analysis revealed that all specimens failed from the tensile side (Fig. 4).

Fractographic analysis of representative failed specimens. The images on the left (× 165) show the complete view of the failed specimen, indicating the failure origin on the tensile side (positioned as the top side in the figures). The figures on the right (× 600) show an approximated view of the failure origin. The black arrows indicate the direction of crack propagation (dcp), the asterisks indicate the compression curl, and the hands indicate the fracture origins
Indented areas
Figure 5 exhibits the five protocols for defect incorporation. According to the non-indented areas of ic and ci, ALD showed a smoother surface than LD after crystallization. Protocols cgi, icg, and cig showed the glossy surface effect of glazing. The defect incorporation, directly after crystallization or after applying a glaze layer, promoted flaw formation. For protocol ci, the indentations showed similar diagonal lengths but different radial crack lengths. For group cgi, since the same glaze layer was applied for both materials, the indentations of ALD and LD presented similar diagonal and radial crack lengths. These images of ci and cgi also revealed a comparison between the mechanical properties of ALD and LD after glaze firing. For both materials, the indentation from group ic had vague boundaries with fewer/shorter cracks, revealing that the damage caused by the indentation is minimized/healed after the crystallization firing. However, the indentations of icg and cig were covered by the glaze layer.

SEM image (× 1000) of the indented areas according to the moment of defect incorporation
Discussion
The aim of this study was to characterize the flexural strength of two lithium disilicates and assess the effect of defect incorporation moments and glaze firing. Based on the results, LD and ALD showed different flexural strengths, which are affected by the moment of defect incorporation as well as glaze firing. Therefore, the null hypothesis was rejected. In this study, a Vickers indentation with a load of 19.6 N was used to simulate damage by clinical adjustments, which consists of brittle fracture and plastic deformation [14]. Only a small defect caused an approximately 50% decrease of the average flexural strength for both LD and ALD, which indicates the sensitivity of ceramics to such type of defects, as well as the effectiveness of the defect incorporation method for evaluating the influence of incorporation moment and glazing firing.
The lithium disilicates evaluated in this study presented different flexural strength under as-crystallized condition (ALDc and LDc). The mean initial strength of ALD was calculated as 195.9 MPa, which is close to another study also adopting the 3-point bending [15] but much lower than a biaxial test [16]. Since the effective volume/area of uniaxial tests like 3-point bending is smaller than that of biaxial tests, the former usually obtains higher flexural strength values than the latter [24]. The explanation could be that the uniaxial tests are more susceptible to edge defects incorporated during specimen preparation, while such edge damage is also common in restorations by milling. Additionally, it can be seen in Fig. 5 that the Vickers indenter generated similar indentations on both materials but shorter crack lengths for LDc, revealing that both materials might have similar hardness but different capabilities against crack propagation. This is consistent with another study [25] that LD has a higher fracture toughness of 2.04 MPam1/2 in comparison with ALD (1.45 MPam1/2), which also contributes to the higher flexural strength of LD.
According to the results, defect incorporation moment had a significant influence on flexural strength. For both materials, group cgi and ci produced the worst strength. This is consistent with the finding in Fig. 4 that the fracture origins of ci and cgi were the introduced defects located in the middle of the tensile surface, while for other groups, the failure started from the flaws in the tensile surface within both materials and glaze layer. For both ceramics, group ic generated similar strength as group c, indicating that the defect incorporation before crystallization did not influence the strength. This is in agreement with fractography that the incorporated defects failed to dominate the fracture initiation. It is possible that the crystallization process can heal the flaws so that the incorporated defect size was reduced. Evidence can be found in Fig. 4, that the defects showed vague boundaries, and the radial cracks were reduced or shortened. Such a phenomenon where the induced pre-crack on pre-crystallized LD failed to control the fracture after fully crystallization has also been previously reported [26].
The effect of glaze on strength recovery varies between the evaluated materials. For ALD, groups cg, icg, and cig were significantly stronger than groups c, ic, and ci respectively, and both icg and cig even generated similar strength as cg. This indicates that glaze firing after defect incorporation either before or after crystallization led to full strength recovery for ALD, while it did not have the same repair effect on LD. As a result, the flexural strength of both lithium disilicates after the glaze firing (LDcg, ALDcg) was similar. A possible explanation is that the incorporated defects and other surface flaws of ALD might be healed after the glaze firing, whereas this did not happen to LD. Glass–ceramics can benefit from auto-glaze to obtain a smooth surface and improve its mechanical properties when getting refired, during which the glass component filled the surface flaws and reduced their depth and sharpness [27]. A recent study [22] found that even an additional firing cycle without glaze material (same protocol as normal glaze firing) can also generate a higher flexural strength of ALD than a single mandatory firing, although this improvement is not as great as mandatory firing followed by glazing, indicating that a healing effect of glaze firing on ALD is attributed to both the glaze material and the refiring process. However, such a glaze firing cycle is not sufficient to heal the defects in LD [28, 29], and the application of glaze material even generates additional defects within the glaze layer that have a larger size than the defects within LD [22].
This study showed that both materials had similar strength after glazing and surface damage by clinical adjustment, despite the difference in their initial strength; glazing of ALD can improve material strength and eliminate the influence of the incorporated defect, but this is not the case for LD. Therefore, our recommended moment for ALD defect incorporation is after crystallization and before the glaze firing (cig); while for LD, defect incorporations before crystallization (ic, icg) are also acceptable; though glazing after defect incorporation can lead to an intra-oral start of the restoration at the highest strength, such initial strength of the restoration will decrease if a necessary adjustment has to be performed after the glaze firing. Further studies are needed to reveal the effect of surface treatments after necessary clinical adjustment, such as polishing and reglazing, on the flexural strength of ALD restorations. Another limitation of this study is that the defects incorporated do not completely simulate the real defects introduced on ceramic restorations in the clinical situation, because the shape and size of the defects and location of the adjustments for each case can be distinct from the others. When the size of the introduced flaw is too small or located in a low stress region, it may not have a noticeable effect on strength. However, in this study, only one defect was already sufficient to promote significant differences in the results. Future studies should be performed to investigate damages caused by the milling burs, as well as two- and three-body wear to investigate the influence of defect incorporation in simulated function with other mechanical properties for reinforced glass–ceramic restorations.
Conclusions
According to the limitations of this study, it was possible to draw the following conclusions:
-
1.
Advanced lithium disilicate showed lower flexural strength compared to a well-known lithium disilicate.
-
2.
Considering the finishing technique, different from lithium disilicate, the advanced lithium disilicate must be crystallized and receive a glaze layer to achieve its highest flexural strength
-
3.
Defects should not be incorporated after glaze firing. The less critical moment when a defect is incorporated occurs on crystalized restorations that will receive a glazer layer after
-
4.
Defects incorporated in pre-crystallized advanced lithium disilicate and lithium disilicate can be healed during crystallization firing.
Data Availability
The data will be available when requested to the corresponding author.
References
Giordano R (2022) Ceramics overview. Br Dent J 232:658–663. https://doi.org/10.1038/S41415-022-4242-6
Chen Y, Yeung AWK, Pow EHN, Tsoi JKH (2021) Current status and research trends of lithium disilicate in dentistry: a bibliometric analysis. J Prosthet Dent 126:512–522. https://doi.org/10.1016/J.PROSDENT.2020.08.012
Saavedra GDSFA, Tribst JPM, De Carvalho RN et al (2021) Feldspathic and lithium disilicate onlays with a 2-year follow-up: split-mouth randomized clinical trial. Braz Dent J 32:53–63. https://doi.org/10.1590/0103-6440202104080
Zarone F, Di Mauro MI, Ausiello P et al (2019) Current status on lithium disilicate and zirconia: a narrative review. BMC Oral Health 19:1–14. https://doi.org/10.1186/s12903-019-0838-x
Malament KA, Margvelashvili-Malament M, Natto ZS et al (2021) 10.9-year survival of pressed acid etched monolithic e.max lithium disilicate glass-ceramic partial coverage restorations: performance and outcomes as a function of tooth position, age, sex, and the type of partial coverage restoration (inlay or onlay). J Prosthet Dent 126:523–532. https://doi.org/10.1016/J.PROSDENT.2020.07.015
van den Breemer C, Vinkenborg C, van Pelt H et al (2017) The clinical performance of monolithic lithium disilicate posterior restorations after 5, 10, and 15 years: a retrospective case series. Int J Prosthodont 30(1):62–65. https://doi.org/10.11607/ijp.4997
Garling A, Sasse M, Becker MEE, Kern M (2019) Fifteen-year outcome of three-unit fixed dental prostheses made from monolithic lithium disilicate ceramic. J Dent 89:103178. https://doi.org/10.1016/J.JDENT.2019.08.001
Becker M, Chaar MS, Garling A, Kern M (2019) Fifteen-year outcome of posterior all-ceramic inlay-retained fixed dental prostheses. J Dent 89:103174. https://doi.org/10.1016/J.JDENT.2019.07.012
Son K, Yu BY, Lee JH et al (2021) Comparison of intaglio surface adjustment in the oral cavity for lithium disilicate crowns fabricated using different scanners. J Prosthodont 30:276–281. https://doi.org/10.1111/jopr.13259
Chantikul P, Anstis GR, Lawn BR, Marshall DB (1981) A critical evaluation of indentation techniques for measuring fracture toughness: II, strength method. J Am Ceram Soc 64(9):539–543. https://doi.org/10.1111/j.1151-2916.1981.tb10321.x
Dal Piva AMO, Contreras LPC, Ribeiro FC et al (2018) Monolithic ceramics: effect of finishing techniques on surface properties, bacterial adhesion and cell viability. Oper Dent 43:315–325. https://doi.org/10.2341/17-011-L
de Oliveira Dal Piva AM, JPM T, Venturini AB et al (2020) Survival probability of zirconia-reinforced lithium silicate ceramic: effect of surface condition and fatigue test load profile. Dent Mater 36(6):808–815. https://doi.org/10.1016/J.DENTAL.2020.03.029
Zandinejad A, Lin WS, Atarodi M et al (2015) Digital workflow for virtually designing and milling ceramic lithium disilicate veneers: a clinical report. Oper Dent 40:241–246. https://doi.org/10.2341/13-291-S
Song XF, Ren HT, Yin L (2016) Machinability of lithium disilicate glass ceramic in in vitro dental diamond bur adjusting process. J Mech Behav Biomed Mater 53:78–92. https://doi.org/10.1016/J.JMBBM.2015.08.003
Reid DA, Matis JI, Lien W et al (2023) Optical and mechanical properties of new ceramic CAD/CAM materials. Oper Dent 48:425–434. https://doi.org/10.2341/22-098-L
Demirel M, Diken Türksayar AA, Donmez MB (2023) Translucency, color stability, and biaxial flexural strength of advanced lithium disilicate ceramic after coffee thermocycling. J Esthet Restor Dent 35:390–396. https://doi.org/10.1111/JERD.12960
Rosentritt M, Schmid A, Huber C, Strasser T (2022) In vitro mastication simulation and wear test of virgilite and advanced lithium disilicate ceramics. Int J Prosthodont 35:770–776. https://doi.org/10.11607/ijp.7820
Hurle K, Lubauer J, Belli R, Lohbauer U (2022) On the assignment of quartz-like LiAlSi2O6 - SiO2 solid solutions in dental lithium silicate glass-ceramics: virgilite, high quartz, low quartz or stuffed quartz derivatives? Dent Mater 38(9):1558–1563. https://doi.org/10.1016/J.DENTAL.2022.07.009
Lubauer J, Lohbauer U, Belli R (2023) Fatigue threshold R-curves for dental lithium disilicate glass–ceramics. J Dent Res 102(10):1106–1113. https://doi.org/10.1177/00220345231180565
Marshall DB (1983) Controlled flaws in ceramics: a comparison of Knoop and Vickers indentation. J Am Ceram Soc 66(2):127–131. https://doi.org/10.1111/j.1151-2916.1983.tb09989.x
Lu Y, Wang L, Dal Piva AMO et al (2023) Influence of surface finishing and printing layer orientation on surface roughness and flexural strength of stereolithography-manufactured dental zirconia. J Mech Behav Biomed Mater 143:105944. https://doi.org/10.1016/J.JMBBM.2023.105944
Lu Y, Dal Piva AMO, Nedeljkovic I et al (2023) Effect of glazing technique and firing on surface roughness and flexural strength of an advanced lithium disilicate. Clin Oral Investig 27:3917–3926. https://doi.org/10.1007/S00784-023-05014-1/FIGURES/3
Machry RV, Dapieve KS, Cadore-Rodrigues AC et al (2022) Mechanical characterization of a multi-layered zirconia: flexural strength, hardness, and fracture toughness of the different layers. J Mech Behav Biomed Mater 135:105455. https://doi.org/10.1016/J.JMBBM.2022.105455
Lu Y, Mei Z, Zhang J et al (2020) Flexural strength and Weibull analysis of Y-TZP fabricated by stereolithographic additive manufacturing and subtractive manufacturing. J Eur Ceram Soc 40(3):826–834. https://doi.org/10.1016/j.jeurceramsoc.2019.10.058
Lubauer J, Belli R, Peterlik H et al (2022) Grasping the Lithium hype: insights into modern dental lithium silicate glass-ceramics. Dent Mater 38:318–332. https://doi.org/10.1016/J.DENTAL.2021.12.013
Belli R, Lohbauer U, Goetz-Neunhoeffer F, Hurle K (2019) Crack-healing during two-stage crystallization of biomedical lithium (di)silicate glass-ceramics. Dent Mater 35:1130–1145. https://doi.org/10.1016/j.dental.2019.05.013
Hirao K, Tomozawa M (1987) Dynamic fatigue of treated high-silica glass: explanation by crack tip blunting. J Am Ceram Soc 70(6):377–382. https://doi.org/10.1111/j.1151-2916.1987.tb05654.x
Aurélio IL, Fraga S, Dorneles LS et al (2015) Extended glaze firing improves flexural strength of a glass ceramic. Dent Mater 31:e316–e324. https://doi.org/10.1016/j.dental.2015.10.012
Aurélio IL, Dorneles LS, May LG (2017) Extended glaze firing on ceramics for hard machining: crack healing, residual stresses, optical and microstructural aspects. Dent Mater 33:226–240. https://doi.org/10.1016/j.dental.2016.12.002
Funding
This study was funded by China Scholarship Council (grant number: 202006240085).
Author information
Authors and Affiliations
Contributions
Yuqing Lu: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, validation, visualization, writing original draft, writing, review, and editing.
Amanda Maria de Oliveira Dal Piva: conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, supervision, validation, visualization, writing original draft, writing, review, and editing.
Joao Paulo Mendes Tribst: conceptualization, formal analysis, methodology, project administration, resources, software, validation visualization, writing, review, and editing.
Albert J. Feilzer: conceptualization, formal analysis, funding acquisition, project administration, resources, supervision, validation, visualization, writing, review, and editing.
Cornelis J. Kleverlaan: conceptualization, formal analysis, methodology, project administration, resources, software, supervision, validation, visualization, writing, review, and editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Conflict of interest
The authors declare no competing of interests.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lu, Y., de Oliveira Dal Piva, A.M., Tribst, J.P.M. et al. Does glaze firing affect the strength of advanced lithium disilicate after simulated defects?. Clin Oral Invest 27, 6429–6438 (2023). https://doi.org/10.1007/s00784-023-05246-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-023-05246-1