
Abstract
Background
Chronic pancreatitis (CP) is defined according to the recently proposed mechanistic definition as a pathological fibro-inflammatory syndrome of the pancreas in individuals with genetic, environmental, and/or other risk factors who develop persistent pathological responses to parenchymal injury or stress.
Methods
The clinical practice guidelines for CP in Japan were revised in 2021 based on the 2019 Japanese clinical diagnostic criteria for CP, which incorporate the concept of a pathogenic fibro-inflammatory syndrome in the pancreas. In this third edition, clinical questions are reclassified into clinical questions, background questions, and future research questions.
Results
Based on analysis of newly accumulated evidence, the strength of evidence and recommendations for each clinical question is described in terms of treatment selection, lifestyle guidance, pain control, treatment of exocrine and endocrine insufficiency, and treatment of complications. A flowchart outlining indications, treatment selection, and policies for cases in which treatment is ineffective is provided. For pain control, pharmacological treatment and the indications and timing for endoscopic and surgical treatment have been updated in the revised edition.
Conclusions
These updated guidelines provide clinicians with useful information to assist in the diagnosis and treatment of CP.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The clinical practice guidelines for chronic pancreatitis (CP) have a history of being prepared in accordance with revisions to the clinical diagnostic criteria for CP. The first edition of the clinical practice guidelines for CP was created in 2009 based on the 2001 clinical diagnostic criteria, and the second edition [1] was published in 2015 with addition of new diagnostic criteria for early stage CP from the 2009 revision of the clinical diagnostic criteria [2]. This third edition, namely, the 2021 clinical practice guidelines for CP, is based on the 2019 revision of the clinical diagnostic criteria for CP [3, 4], which incorporate the concept of a pathogenic fibro-inflammatory syndrome, which involves persistent inflammation and fibrosis of the parenchyma.
The revision work was carried out in accordance with the Minds Guide for the Development of Clinical Practice Guidelines 2017 [5] and the JSGE Clinical Practice Guidelines [6]. The JSGE guidelines committee decided to reclassify the clinical questions into three categories: clinical questions (CQ), the answers to which are associated with important outcomes in the guidelines and were established by an exhaustive literature review; background questions (BQ), which generally have 100% consensus; and future research questions (FRQ) that do not have sufficient data available to be considered as CQ, but are important issues for the future. For CQ and FRQ, the literature search covered the period from 1989 to December 31, 2019, and included both English- and Japanese-language studies. Important new evidence that emerged between the end of the literature search period and June 2021 was added through a manual search. The level of evidence in general was evaluated using the GRADE (The Grading of Recommendations Assessment Development and Evaluation) system [7]. The strength of each recommendation was based on (1) certainty of evidence (strength), (2) patient preferences, (3) benefits and harms, and (4) cost evaluation. The quality of the evidence was graded as A (high), B (moderate), C (low), or D (very low).
Experts voted using a modified Delphi method and the nominal group technique, and consensus was deemed to have been reached when at least 70% of experts were in agreement.
Definition
The concept of a new international mechanistic definition of CP has been proposed [8]. According to this definition, CP is defined as a pathogenic fibro-inflammatory syndrome of the pancreas in which a persistent pathological response to pancreatic parenchymal injury or stress occurs in individuals with genetic, environmental, and/or other risk factors. In Japan, diagnosis of CP is based on the 2019 clinical diagnostic criteria [3, 4]. According to this new concept, patients with CP are considered to be at risk or to have acute pancreatitis-recurrent acute pancreatitis, early CP, established CP, or end-stage CP. Thus, CP based on the 2009 clinical diagnostic criteria [2] corresponds to established CP and end-stage CP in this conceptual model. Early CP has not reached established CP, and it is assumed that some biomarkers and pathological changes that reflect the pathophysiology of CP will be detected to distinguish it from acute pancreatitis-recurrent acute pancreatitis.
Diagnosis
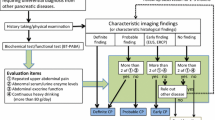
When CP is suspected, a diagnosis should be made according to the 2019 clinical diagnostic criteria for CP [3, 4]. The 2009 clinical diagnostic criteria for CP [2] introduced the concept of early CP for the first time, and were revised in 2019 with the intention of implementing diagnostic criteria with higher specificity based on the findings of a nationwide epidemiologic survey of early CP [9] and a prospective prognosis survey [10]. A flowchart showing the process for differential diagnosis of CP is provided in Fig. 1. Diagnostic elements consist of characteristic imaging findings, characteristic histological findings, and five evaluation elements. Patients are diagnosed as having early CP if they have three or more of the five evaluation items and findings characteristic of early CP on endoscopic ultrasound (EUS), endoscopic retrograde cholangiopancreatography (ERCP), or magnetic resonance cholangiopancreatography (MRCP).

Diagnostic pathway for chronic pancreatitis. *Careful follow-up is required for a suspected case of early CP when two items of (1) to (5) are positive and other diseases are excluded in cases showing imaging findings that suggest early CP. BT-PABA pancreatic function diagnostant test, CT computed tomography, CP chronic pancreatitis, ERCP endoscopic retrograde cholangiopancreatography, EUS endoscopic ultrasound, MRCP magnetic resonance cholangiopancreatography, US ultrasonography
Abdominal ultrasound is useful for diagnosis of stones, dilation of the pancreatic duct, and pancreatic atrophy, but these features are often difficult to observe if the patient is in poor physical condition. A systematic review [11] found that abdominal ultrasound had sensitivity of 67% [95% confidence interval (CI) 53–78%], which is clearly lower than that for other diagnostic imaging methods. A study in the United States found that when the findings in the pancreatic duct and parenchyma were assessed according to the Rosemont classification [12], which is a system of criteria for diagnosing CP by EUS, the sensitivity increased to 81% and the specificity increased to 97% [13].
Computed tomography (CT) is useful for diagnosing CP, but it is difficult to diagnose early CP using CT. Despite having inferior diagnostic ability to that of EUS, abdominal CT has been reported to be useful for diagnosis of CP [14,15,16]. In a systematic review of the various diagnostic imaging methods used for CP, abdominal CT had sensitivity of 75% and specificity of 91%, indicating excellent diagnostic ability [11]. When early stage CP is suspected, it is difficult to detect subtle changes in the pancreatic parenchyma by CT (9), and evaluation by EUS should be added [3, 4].
CQ: is abdominal magnetic resonance imaging/MRCP recommended for diagnosis of CP?
-
Abdominal magnetic resonance imaging/MRCP is useful for the diagnosis of CP, and we suggest that it be performed.
Strength of recommendation: weak, evidence level: B
MRCP has been shown to have high diagnostic ability for CP and a good diagnostic correlation with ERCP [17, 18]. In a recent meta-analysis, the diagnostic ability of MRCP for CP had sensitivity of 78% and specificity of 96%, which are almost the same as those of ERCP [11]. Recently, secretin-stimulated MRCP has been shown to have high diagnostic ability for early CP and evaluation of exocrine function [19,20,21]. Although ERCP is useful for diagnosing CP, it should be performed after carefully considering the indications.
CQ: is endoscopic ultrasound recommended for diagnosis of CP?
-
EUS is useful for diagnosing CP/early CP, because it allows detailed observation of the pancreatic parenchyma and the morphology of the pancreatic duct, and has been proposed as treatment.
Strength of recommendation: weak, evidence level: B
The 2009 clinical diagnostic criteria for CP [2] include seven EUS findings for diagnosis of early CP with reference to the Rosemont classification (12). The validity of each EUS diagnostic element in the examination has also been demonstrated from the standpoint of risk factors for CP [22, 23]. A multicenter prospective study that sought to confirm the validity of these diagnostic criteria found that about 5% of cases diagnosed as early CP by this criteria progressed to definite or probable CP [10]. In the 2019 clinical diagnostic criteria for CP [3], similar findings for early CP were integrated and the number of items was reduced from seven to four to increase the specificity of EUS diagnosis: (1) hyperechoic foci (non-shadowing) or strands, (2) lobularity, (3) a hyperechoic main pancreatic duct margin, and (4) dilated side branches. At least two of these four EUS findings, including (1) or (2), are required for a diagnosis of early CP. In recent years, pancreatic hardness measured by EUS elastography has been investigated for its ability to diagnose early stage CP [24].
Etiology
FRQ: which patients should be tested for pancreatitis-associated genetic abnormalities?
-
A search for PRSS1 and SPINK1 gene abnormalities should be considered in patients with juvenile pancreatitis or CP of unknown origin and a family history.
-
It is hoped that greater consensus will be reached on the genes to be analyzed, gene counseling for mutation-positive individuals, and pancreatic cancer screening methods in patients with hereditary pancreatitis.
Since the report identifying mutation of the cationic trypsinogen (PRSS1) gene as the cause of hereditary pancreatitis in 1996 [25], abnormalities in various pancreatitis-associated genes, including cystic fibrosis membrane conductance regulator (CFTR) [26, 27], pancreatic secretory trypsin inhibitor (SPINK1) [28], chymotrypsin C (CTRC) [29], carboxypeptidase A1 (CPA1) [30], and calcium ion channel TRPV6 [31], have been reported. In the Japan National Survey of Hereditary Pancreatitis [32], mutations in PRSS1 were found in 30 of 73 families (41.1%) and mutations in SPINK1 in 26 (35.6%). Genetic testing for PRSS1 and SPINK1 in patients with hereditary pancreatitis has been reported in Europe and the US [33, 34]. Furthermore, the American College of Gastroenterology guideline for CP [35] recommends that genetic tests for PRSS1, SPINK1, CFTR, and CTRC be performed for CP of unknown origin, especially in young patients. In the 2019 clinical diagnostic criteria for CP [3, 4], mutations in established pancreatitis-associated genes, such as PRSS1 and SPINK1, are included in the diagnostic items for early stage CP, and the role of genetic testing in daily clinical practice is increasing. However, pancreatitis-associated genetic tests are currently not covered by national health insurance in Japan, and it is still unclear how abnormalities in SPINK1 should be handled in the diagnostic criteria for hereditary pancreatitis. It is hoped that greater consensus will be reached by combining the genes to be analyzed in the same genetic test, genetic counseling for mutation-positive individuals, and improved screening methods for pancreatic cancer in patients with hereditary pancreatitis.
Staging
CP is classified into latent, compensatory, transitional, and decompensated stages according to the degree of pancreatic endocrine and exocrine dysfunction.
Abdominal pain is the main symptom during the latent to compensatory stage, when there is no obvious impairment of pancreatic endocrine and exocrine function. In the decompensated stage, pancreatic endocrine and exocrine dysfunction becomes the main symptom. Pancreatic exocrine dysfunction is caused by a deficiency in pancreatic enzymes and manifests as digestive and absorptive disorders. Patients with pancreatic exocrine dysfunction are susceptible to malnutrition because of impaired digestion and absorption of lipids and caloric loss as a result of increased fat excretion in the stool. Pancreatic exocrine dysfunction also causes various symptoms, including steatorrhea, abdominal distension, and deficiencies in fat-soluble vitamins (A, D, E, and K) and essential fatty acids, which reduce the patient’s quality of life [36, 37]. Moreover, pancreatic exocrine insufficiency has recently been reported to be associated with a decrease in muscle mass (sarcopenia), which leads to a decrease in muscle strength and impaired physical function [38]. There are two types of pancreatic exocrine function tests: a direct method for evaluating pancreatic exocrine function under secretin stimulation and an indirect method under non-stimulation. Indirect pancreatic exocrine function tests include measurement of fecal chymotrypsin activity, measurement of fecal elastase 1, the 13C-dipeptide (benzoyl-L-tyrosyl-[1-13C] alanine: Bz-Tyr-Ala) breath test, the BT-PABA (pancreatic function diagnostant) test, and cine-dynamic MRCP. A diagnosis of exocrine pancreatic insufficiency is based on clinical signs, nutritional index markers, and the BT-PABA test. The fecal elastase 1, the 13C-labeled breath tests, and cine-dynamic MRCP are currently not covered by national health insurance in Japan.
Pancreatic endocrine dysfunction is positioned as diabetes mellitus secondary to pancreatic disease, such as CP and pancreatic cancer, or following pancreatectomy. Glycemic control is often unstable in these patients because of reduced secretion of insulin and glucagon.
Treatment
Treatment strategies include pharmacological agents, nutritional therapy, lifestyle guidance, endoscopic treatment, and surgery depending on symptoms, pancreatic exocrine and endocrine function, and various complications. A flowchart summarizing the treatment options is shown in Fig. 2.

Therapeutic pathway for chronic pancreatitis. CP chronic pancreatitis, ESWL extracorporeal shock wave lithotripsy
Alcohol is a risk factor for progression from acute alcoholic pancreatitis to CP, and abstinence may prevent recurrent acute pancreatitis and progression to CP [39, 40]. According to a survey of the prognosis of acute pancreatitis in Japan, the percentage of patients who progressed to CP after acute alcoholic pancreatitis was 13.6% in cases of complete abstinence, 23.3% in cases of limited alcohol consumption but still drinking daily, and 40.9% when alcohol consumption remained unchanged [41]. Abstinence is important for improvement of the prognosis in patients with alcoholic CP. In a study of alcohol abstinence in patients with acute alcoholic pancreatitis, the recurrence rate was significantly lower in patients who were repeatedly instructed to abstain from alcohol after discharge than in those who were instructed to abstain from alcohol only once at the time of discharge [42]. In principle, patients with alcoholic pancreatitis should be instructed to refrain from alcohol, which means permanent abstinence. Abstinence from smoking may also prevent progression of CP; therefore, the recommendation is to provide guidance on smoking cessation.
In the compensated stage, prevention of repeated relapses and pain takes priority. Nutritional therapy appropriate to the disease stage is useful for patients with CP. A fat-restricted diet is effective for patients in the compensatory stage who have abdominal pain. Nonsteroidal anti-inflammatory drugs (NSAIDs) are the first choice for analgesia, and if inadequate, weak opioids are useful for both abdominal pain and back pain. If analgesia is still inadequate, strong opioids may be used (see Fig. 3). Endoscopic treatment is used in patients with abdominal pain resulting from obstruction of the pancreatic duct. Extracorporeal shock wave lithotripsy (ESWL), endoscopic treatment, and surgery are options for treatment of pancreatic stones. Endoscopic treatment includes endoscopic pancreatic duct incision, endoscopic stone removal, and endoscopic placement of a pancreatic duct stent. For stenosis/occlusion of the pancreatic duct, plastic stents, metallic stents, and dumbbell-type stents with a terminal shape that is less likely to cause stent invasion or stent-induced pancreatic duct stenosis can be placed. Transpapillary drainage or EUS (transgastrointestinal, antegrade, and rendezvous) drainage of pseudocysts due to CP is recommended. If endoscopic drainage is difficult, surgery should be considered. EUS/CT-guided celiac plexus block/neurolysis is effective in the short term for abdominal pain, but is less effective in the long term. Interventional radiology is useful for pseudoaneurysm and hemosuccus pancreaticus associated with CP.

Conservative medical treatment pathway for chronic pancreatitis. In cases of acute exacerbation, the severity of acute pancreatitis and the treatment strategy should be determined promptly. Treatment with an elemental diet may be considered. Choice of pharmacotherapy and selection of the dose should be decided in reference to this figure
In the decompensated stage, treatment is required for digestive malabsorption, nutritional disorders, and diabetes mellitus caused by decreased pancreatic endocrine and exocrine function. Patients with exocrine pancreatic insufficiency should receive pancreatic enzyme replacement therapy and adequate nutrition without fat restriction. Fat-soluble vitamin (A, D, E, and K) supplementation can be given after pancreatic enzyme replacement therapy depending on the degree of exocrine pancreatic insufficiency and nutritional status. Prospective observational studies have shown that patients with CP have decreased bone mineral density [43]. It has been reported that 23.4% (95% CI 16.6–32.0) of patients with CP have osteoporosis and 39.8% (95% CI 29.1–51.6) have osteopenia [44]. Cross-sectional observational studies have also found that bone mineral density decreases in patients with CP regardless of its cause and duration [45]. The decrease in bone density and bone disease caused by CP are now known as CP-associated osteopathy [44]. Sarcopenia has been reported to lead to a significantly increased hospitalization risk and mortality risk in patients with CP [46], and pancreatic exocrine dysfunction is an independent risk factor for sarcopenia [38, 46]. Although there is not a high level of evidence from studies of treatment methods for CP-associated sarcopenia, nutritional therapy, including appropriate pancreatic enzyme replacement therapy for pancreatic exocrine dysfunction, is presumed to be useful [47].
CQ: is smoking cessation guidance recommended for treatment of CP?
-
Smoking cessation guidance is recommended for treatment of CP.
Strength of recommendation: strong, evidence level: C
In a meta-analysis of 10 observational studies (n = 22,850), smoking significantly increased the risk of developing CP [relative risk (RR) 2.29, 95% CI 2.08–2.51; p < 0.00001] [48,49,50,51,52,53,54,55,56,57]. Furthermore, smoking was found to promote pancreatic calcification (RR 1.44, 95% CI 1.25–1.67; p < 0.00001) [58,59,60,61,62,63,64] and to increase the risk of developing pancreatic exocrine dysfunction (RR 1.62, 95% CI 1.29–2.04, p < 0.00001) and diabetes (RR 1.28, 95% CI 1.10–1.48; p = 0.001) in a meta-analysis of seven observational studies of pancreatic calcification (n = 2953), four observational studies of pancreatic exocrine dysfunction (n = 1331), and five observational studies of diabetes (n = 2254) [58,59,60,61,62,63,64,65]. In a meta-analysis of two observational studies, smoking also worsened the long-term prognosis after endoscopic treatment in patients with painful CP (RR 4.73, 95% CI 2.15–10.40; p = 0.0001) [66, 67]. In contrast, a meta-analysis of five observational studies showed that smoking cessation had the effect of suppressing the onset of CP (RR 0.58, 95% CI 0.51–0.67; p < 0.00001) [51,52,53,54,55]. A study in which 360 patients with CP underwent long-term follow-up (for a mean of 19 years) found that those who quit smoking within 5 years after onset of CP had a significantly reduced risk of pancreatic calcification in comparison with those who continued to smoke (RR 0.44, 95% CI 0.22–0.87; p = 0.02) [62]. A meta-analysis of two observational studies in which ESWL and endoscopic treatment were performed in patients with painful CP who underwent long-term follow-up found that relapse of pain was significantly less likely in those who stopping smoking than in those who continued smoking (RR 0.20, 95% CI 0.08–0.54; p = 0.001) [66, 68].
CQ: are nonopioid analgesics, opioids, and analgesic adjuvants recommended for treatment of pain?
-
Weak opioids are recommended if NSAIDs are ineffective.
Strength of recommendation: weak, evidence level: C
-
If adequate doses of NSAIDs or weak opioids are ineffective, consider endoscopic treatment or surgery. Strong opioids should be reserved for patients for whom these treatments are not indicated.
Strength of recommendation: weak, evidence level: D
NSAIDs and anticholinergic agents that suppress pancreatic exocrine stimulation via the vagus nerve have been widely used in CP. However, a weak opioid is recommended when NSAIDs are not sufficiently effective. Tramadol is a weak opioid that was demonstrated to have an analgesic effect equivalent to that of morphine in a randomized-controlled trial (RCT) that included patients whose pain did not improve after 2 weeks of an NSAID [69]. Furthermore, compared with morphine, tramadol has fewer psychological and gastrointestinal side effects [70]. A study of the pharmacokinetics of oral and intravenous administration of acetaminophen in patients with CP found a low concentration of acetaminophen in the blood and suggested that administration of additional analgesics should be considered in these patients [71]. The American Gastroenterological Society guidelines on the treatment of pain in CP [72] and the German guidelines for treatment of CP [73] recommend use of NSAIDs and non-narcotic analgesics in stages, and if they are not sufficiently effective, narcotic agents can be used. Recent reports suggest that the analgesic effect of oxycodone may be better than that of morphine because of its kappa agonist activity [71]. An RCT reported a few years ago found that pain associated with CP was alleviated by a combination of antioxidants and pregabalin [74].
CQ: is pancreatic enzyme replacement therapy recommended for treatment of pain?
-
Pancreatic enzyme replacement therapy should not be used to treat pain in patients with CP. However, it may be beneficial for abdominal symptoms, such as abdominal distention and flatulence, associated with pancreatic exocrine dysfunction.
Strength of recommendation: weak, evidence level: C
A meta-analysis [75], systematic review [76], and Cochrane review [77] could not demonstrate the efficacy of pancreatic enzyme replacement therapy for pain in CP. However, its effectiveness for abdominal pain and flatulence due to exocrine pancreatic insufficiency has been confirmed [78,79,80].
CQ: are proteolytic enzyme inhibitors recommended for treatment of pain?
-
We propose use of a proteolytic enzyme inhibitor as a treatment for pain.
Strength of recommendation: weak, evidence level: D
Proteolytic enzyme inhibitors have an inhibitory effect on trypsin activity and are thought to suppress the progression of pancreatitis by suppressing activation of pancreatic enzymes. Abdominal symptoms were reported to improve in patients with nonalcoholic CP who received proteolytic enzyme inhibitors if they had a higher number of positive EUS findings [81]. A combination of camostat mesilate, pancrelipase, and rabeprazole has been reported to achieve significant improvement in epigastric pain in patients with early stage CP [82].
CQ: is long-term repeated endoscopic treatment recommended for treatment of pain?
-
Long-term repeated endoscopic treatment (for more than 2–3 years) should not be used to treat pain in patients with CP.
Strength of recommendation: weak, evidence level: C
In randomized-controlled trials, pain scores were significantly improved in patients with CP-related pain who underwent surgery first in comparison with those who underwent endoscopic treatment first [83,84,85,86]. Furthermore, in one of these studies, the number of treatment procedures was significantly lower in the surgical treatment group [86]. Although the superiority of surgery is recognized, endoscopic treatment is currently positioned as first-line treatment in view of its minimal invasiveness and low complication rate. A systematic review reported that pain severity and reintervention and pancreatic insufficiency rates were lower after early surgical intervention (within 3 years) than after late surgery (3 years and beyond) [87]. Another study found no significant difference in the complete or partial pain disappearance rate between endoscopic treatment (+ ESWL) and surgery in patients with pancreatic stones in the head and body of the pancreas but no inflammatory mass, duodenal stenosis, or biliary stricture [88]. In summary, repeated endoscopic treatment should not be used over the long term (2–3 years) in patients with CP-related pain. However, given that endoscopic treatment is less invasive than surgery and is effective in some cases, endoscopic treatment (+ ESWL) can be performed over a period of 1–2 years. However, the evidence is still inadequate and more studies are needed to clarify the value of repeated endoscopic treatment in the long term.
CQ: is surgical treatment recommended for treatment of pain when endoscopic treatment is ineffective?
-
Surgical treatment is recommended for patients in whom endoscopic treatment has been ineffective for pain relief.
Strength of recommendation: strong, evidence level: B
Endoscopic treatment is unlikely to achieve long-term pain control. In a study of patients in whom pain relapsed during long-term follow-up after insertion of a pancreatic duct stent, the results in terms of severity of pain, weight gain, and reintegration were better in those who underwent surgery than in those who underwent stent reinsertion [89]. Pancreatectomy, pancreaticojejunostomy, and abscess drainage were reported to achieve complete resolution of pain in approximately 62.5% of cases in which pain resolution had been inadequate after endoscopic pancreatic stenting [90], suggesting that surgery can be helpful when endoscopic pancreatic stenting has been ineffective. Endoscopic stenting of the pancreatic duct was reported to have no adverse effects on the outcome of subsequent pancreaticojejunostomy in patients with CP [91]. Furthermore, according to three meta-analyses, the pain remission rate after surgical treatment was 80.4% and significantly higher than that after endoscopic treatment which was 72.6%, whereas the complication rate associated with surgical treatment was 12.7% and that associated with endoscopic treatment was 10.1%. These findings indicate that surgery is superior to endoscopic treatment in terms of pain relief. Furthermore, there is evidence, suggesting that there is no difference in the incidence of complications in patients with CP and pancreatic duct dilation [92,93,94]. Although endoscopic treatment is the first choice for pain control in patients with CP for whom conservative medical treatment is ineffective, surgical treatment is recommended for the cases in which endoscopic treatment is unsuccessful or ineffective (Fig. 4).

Surgical treatment pathway for chronic pancreatitis. If a malignant tumor cannot be ruled out, pancreaticoduodenectomy is performed for a lesion at the head of the pancreas and distal pancreatectomy with lymph-node dissection for a lesion at the tail of the pancreas. *Effective in the short term but not in the long term. CP chronic pancreatitis, ESWL extracorporeal shock wave lithotripsy
CQ: is a fat-restricted diet recommended for treatment of pancreatic exocrine insufficiency?
-
A uniform fat-restricted diet is not recommended in the decompensated stage of CP with exocrine pancreatic insufficiency.
Strength of recommendation: strong, evidence level: D
A short-term low-fat diet (fat 30–35 g/day; fat ≤ 10 g/meal) is recommended for patients with compensatory abdominal pain and back pain. However, in the decompensated stage with pancreatic exocrine insufficiency, a daily fat intake of 40–70 g or 30%–40% of total calories is recommended in combination with pancreatic enzyme replacement therapy to prevent malnutrition [95]. The basis of treatment in the decompensated phase is both administration of sufficient pancreatic enzyme replacement therapy and an appropriate energy intake. Excessive dietary restrictions, including fat restriction, must be avoided, because they worsen malnutrition [96].
CQ: is pancrelipase recommended for treatment of pancreatic exocrine insufficiency?
-
Pancrelipase is a high-titer pancreatic enzyme preparation that can be recommended for treatment of pancreatic exocrine insufficiency with steatorrhea and weight loss.
Strength of recommendation; strong, evidence level: A
Significant improvements in fat absorption, nitrogen absorption, and fecal fat content have been reported in multiple randomized-controlled trials of pancrelipase in patients with pancreatic insufficiency due to CP or following pancreatic surgery [79, 80, 97]. Furthermore, a multicenter questionnaire-based survey found that pancrelipase improved quality of life, for example, by improving weight loss and steatorrhea [98].
CQ: are agents that suppress gastric acid recommended for treatment of pancreatic exocrine insufficiency?
-
If the therapeutic effect of pancreatic enzyme replacement therapy is inadequate in patients with pancreatic exocrine insufficiency, an H2-receptor antagonist or proton pump inhibitor can be used.
Strength of recommendation: weak, evidence level: C
In cases of pancreatic exocrine insufficiency, the pH in the upper small intestine is lower because of a decreased bicarbonate concentration in pancreatic juice. A pH of < 4 in the small intestine inactivates pancreatic lipase, and precipitation of bile acid leads to poor formation of micelles. Furthermore, enteric-coated digestive enzyme preparations are not released at a pH < 5. Treatment with a proton pump inhibitor or H2-receptor antagonist has been shown to be effective when combined with a pancreatic digestive enzyme agent, whether enteric-coated or not, in patients with steatorrhea [99,100,101]. Combined use of a gastric acid-suppressing agent has been reported to be effective when the capacity to secrete gastric acid is normal or high [100, 101]. However, the additive effect of a gastric acid-suppressing agent was not confirmed in some studies [102, 103]. Therefore, it is not necessary to consider routine use of a combination of enteric-coated pancreatic digestive enzyme therapy and a gastric acid-suppressing agent. However, it is worth adding an agent that suppresses gastric acid secretion when pancreatic digestive enzyme replacement therapy is not sufficiently effective.
CQ: is calorie restriction similar to that used in primary diabetes recommended when pancreatic exocrine insufficiency is complicated by diabetes?
-
Uniform calorie restriction for pancreatogenic diabetes is not recommended in view of the risk of poor nutrition and hypoglycemia. Glycemic control should be performed in combination with treatment for pancreatic exocrine insufficiency with an appropriate energy intake.
Strength of recommendation: strong, evidence level: D
Pancreatogenic diabetes in the decompensated stage of CP is often associated with exocrine pancreatic insufficiency. It is necessary to evaluate the endocrine and exocrine function of the pancreas and manage nutrition from a long-term perspective. Although there is no explicit treatment policy for calorie intake in patients with diabetes secondary to CP, excessive calorie restriction is not recommended, because it results in poor nutritional status and hypoglycemia [96, 104]. Energy metabolism in patients with pancreatogenic diabetes may be higher than in healthy individuals and should be evaluated on a case-by-case basis. The dietary content, including the carbohydrate and fat intake, should be adjusted with the cooperation of a registered dietitian while monitoring the daily blood glucose level according to the needs of the individual patient [105]. In patients with diabetes secondary to CP and pancreatic exocrine insufficiency, it is important to control blood glucose levels after treating poor digestion and malabsorption and to maintain an appropriate energy intake.
CQ: are oral hypoglycemic agents recommended for treatment of diabetes secondary to CP?
-
Oral hypoglycemic agents are recommended for pancreatogenic diabetes whether the patient has insulin resistance or normal insulin secretory capacity.
Strength of recommendation: weak, evidence level: D
The main treatment for diabetes secondary to CP is insulin, given that the diabetes is caused by insulin deficiency due to depletion of pancreatic β-cells [106]. In the National Epidemiological Survey on Pancreatic Diabetes in Japan, 66.7% of patients with CP-associated diabetes were treated with insulin [107]. However, there are some cases in which the pathophysiology of type 2 diabetes is included as CP-associated diabetes [108]. Although there is not sufficient evidence supporting the efficacy of oral hypoglycemic agents for pancreatogenic diabetes, medication for insulin resistance and insulin secretagogues may be effective if insulin resistance is suspected or insulin secretory capacity is maintained. Metformin has been reported to reduce the risk of developing pancreatic cancer and to improve the prognosis. Although metformin is widely used first-line for CP-associated diabetes [109], there is a report, suggesting that it has no effect on the prognosis [110], and there is little clear evidence to warrant its recommendation at this time.
CQ: is insulin therapy recommended for treatment of pancreatogenic diabetes mellitus?
-
Insulin therapy is recommended for patients with insulin-dependent diabetes mellitus.
Strength of recommendation: strong, evidence level: C
In the National Epidemiological Survey on Pancreatic Diabetes in Japan (2005), 66.7% of respondents were receiving insulin. According to the 2019 diabetes practice guideline [111], insulin therapy is an absolute indication regardless of the type of diabetes if it is insulin-dependent. Considering that endocrine insufficiency in patients with CP is accompanied by deficient glucagon secretion and that hypoglycemia is likely to occur and be prolonged, insulin injections at a frequency close to that of the physiological secretion pattern of insulin are recommended [106, 112].
CQ: is drainage recommended for pseudocysts associated with CP?
-
Endoscopic drainage is recommended as the first choice for symptomatic pseudocysts.
Strength of recommendation: strong, evidence level: C
Pseudocysts measuring < 4 cm in size or confined to the pancreas may disappear and can be followed up without endoscopic drainage if asymptomatic [113, 114]. In symptomatic cases, drainage is indicated regardless of the size of the cyst. Endoscopic drainage is the first choice and surgery is performed in cases where endoscopic treatment is difficult. Percutaneous drainage takes a long time to perform, and should be considered as an emergency evacuation procedure for patients whose general condition is poor [113,114,115]. In a meta-analysis of studies comparing endoscopic treatment and surgery, the success rate was higher after surgical intervention but without any difference in the treatment-related complication rate or the pseudocyst recurrence rate. However, endoscopic treatment resulted in short hospital stays and low costs [116]. When endoscopic EUS drainage is performed, a double pigtail-type plastic stent is placed and not removed for at least 6 weeks [113]. Metal stents are not recommended as the first choice because of cost [117, 118]. Drainage is less invasive when performed laparoscopically than when performed via open surgery and may contribute to a lower complication rate and shorter hospital stays, but these benefits are yet to be determined [119]. Laparoscopic drainage of pseudocyst is currently not covered by national health insurance in Japan.
CQ: is a pancreatic duct stent recommended for internal pancreatic fistula?
-
Placement of a pancreatic duct stent is recommended as the initial treatment for internal pancreatic fistula.
Strength of recommendation: weak, evidence level: C
Endoscopic insertion of a pancreatic duct stent (± conventional conservative treatment) is recommended as the first choice for treatment of internal pancreatic fistula and surgery for nonresponsive cases after 3–6 weeks of follow-up [120,121,122]. The results of treatment are improved by inserting a stent beyond the site of disruption/stenosis in the pancreatic duct. Surgery is performed for patients in whom endoscopic and conservative treatment has been ineffective and for those with complications, such as intra-abdominal infection. The main surgical procedures performed for internal pancreatic fistula are pancreatojejunostomy and cystogastrostomy, with pancreatectomy performed in 10–50% of cases [123, 124].
CQ: is a bile duct stent recommended for biliary stricture associated with CP?
-
The recommendation is to insert multiple plastic stents or a fully covered self-expandable metallic stent (FCSEMS) for CP-associated biliary stricture.
Strength of recommendation: weak, evidence level: B
The 2012 European Society for Gastrointestinal Endoscopy (ESGE) guidelines recommended insertion of multiple plastic stents as first-line treatment [125]. However, there is no difference in results between FCSEMS and insertion of multiple plastic stents and few long-term complications [126, 127]. Therefore, the Asia–Pacific consensus guideline in 2017 recommended insertion of a FCSEMS as the first choice [128]. The 2017 ESGE guidelines also recommend insertion of multiple plastic stents and FCSEMS [129]. However, both procedures are difficult to perform, and it is permissible to insert a single plastic stent in an emergency or for a short period of time.
Prognosis
Causes of death in patients with CP include malignant tumors, pneumonia, infectious diseases, and diabetes and its complications. Long-term treatment and follow-up are needed according to age of onset and whether there are poor prognostic factors such as alcohol consumption and smoking. It is hoped that defining early CP will increase the likelihood of early intervention to prevent progression to irreversible definitive CP. However, there are no reports demonstrating the effectiveness of therapeutic interventions for early CP that target abstinence from alcohol or smoking cessation. Furthermore, there are no reports on medical intervention for early CP with a high level of evidence. A prospective study that includes a large number of cases is needed in the future to confirm the effect of early medical therapy in patients with early CP.
Although CP is a risk factor for pancreatic cancer, no screening test for pancreatic cancer has been established for patients with CP. In a study of 506 Japanese patients who had been diagnosed with CP more than 2 years earlier, 19 (3.7%) developed pancreatic cancer during a median follow-up of 5.6 years (standardized prevalence ratio 11.8). The risk of pancreatic cancer was 0.11 (95% CI 0.0014–0.80) in surgical cases compared with non-surgical cases [130]. Prevention of inflammation by early intervention may theoretically protect against development of pancreatic cancer; however, most of the relevant studies published to date have been retrospective, with variations in the time from the onset to the intervention and in the follow-up period thereafter. According to the international guidelines, prophylactic pancreatectomy can be considered for individuals with hereditary pancreatitis, who have a lifetime risk of developing pancreatic cancer of 40–55%, but is not recommended for patients without hereditary pancreatitis [131].
CQ: is endoscopic treatment (+ ESWL) recommended for patients with asymptomatic CP?
-
Endoscopic treatment (+ ESWL) is not recommended in patients with asymptomatic CP.
Strength of recommendation: weak, evidence level: C
The efficacy, safety, and cost of endoscopic treatment (+ ESWL) to preserve pancreatic function have not been adequately investigated in asymptomatic cases with pancreatic duct stenosis or pancreatic stones. In view of its invasiveness, uniform endoscopic treatment is not recommended for asymptomatic patients [113, 132]. However, when there is no atrophy of the pancreatic parenchyma and there is a disorder of pancreatic juice secretion caused by pancreatic stones, this treatment can be performed in a specialist facility with adequate informed consent.
CQ: is surgery recommended to prevent progression of CP?
-
Given that early surgery after onset of CP can delay progression, the surgical indications and procedures should be decided after a thorough evaluation of symptoms and complications.
Strength of recommendation: weak, evidence level: C
Surgery is performed for CP when non-surgical treatment is ineffective and when pancreatic cancer is suspected. Pancreatic duct drainage or pancreatectomy is selected according to the pathological condition. Furthermore, the course of subsequent pancreatic function differs depending on the stage of CP at which surgery was performed. Therefore, the effect of surgery on progression of CP cannot be described unequivocally. To date, there have been no studies of surgery performed primarily to prevent progression of a pathological condition. Therefore, the effect on progression must be inferred from long-term postoperative analysis of pancreatic endocrine and exocrine function in symptomatic cases.
A randomized-controlled trial in patients with mild-to-moderate CP found that significantly better pancreatic function was maintained in patients who underwent surgery than in those who did not [133]. Intervention within a period of 3 years has also been shown to reduce the risk of developing postoperative endocrine and exocrine dysfunction to a greater extent than interventions after 3 years or longer [87, 134, 135]. Pancreatic duct drainage (e.g., Frey’s procedure) may be effective from the standpoint of surgical invasion and prevention of pathophysiological progression of CP when performed at an early stage after onset [136]. However, prophylactic surgery is rarely performed to prevent progression in asymptomatic patients.
References
Ito T, Ishiguro H, Ohara H, et al. Evidence-based clinical practice guidelines for chronic pancreatitis 2015. J Gastroenterol. 2016;51:85–92.
Shimosegawa T, Kataoka K, Kamisawa T, et al. The revised Japanese clinical diagnostic criteria for chronic pancreatitis. J Gastroenterol. 2010;45:584–91.
Japan Pancreas Society. Clinical diagnostic criteria for chronic pancreatitis 2019. J Jpn Pancreas Soc (Suizou). 2019;34:279–81 (in Japanese).
Masamune A, Kikuta K, Kume K, et al. Nationwide epidemiological survey of chronic pancreatitis in Japan: introduction and validation of the new Japanese diagnostic criteria 2019. J Gastroenterol. 2020;55:1062–71.
Kojimahara N, Nakayama T, Morizane T, et al. Minds manual for guideline development 2017. Tokyo: Japan Council for Quality Health Care. 2017.
Yoshida M, Kinoshita Y, Watanabe M, et al. JSGE Clinical Practice Guidelines 2014: standards, methods, and process of developing the guidelines. J Gastroenterol. 2015;50:4–10.
Qaseem A, Kansagara D, Lin JS, et al. The development of clinical guidelines and guidance statements by the clinical guidelines committee of the American college of physicians: update of methods. Ann Intern Med. 2019;170:863–70.
Whitcomb DC, Frulloni L, Garg P, et al. Chronic pancreatitis: an international draft consensus proposal for a new mechanistic definition. Pancreatology. 2016;16:218–24.
Masamune A, Kikuta K, Nabeshima T, et al. Nationwide epidemiological survey of early chronic pancreatitis in Japan. J Gastroenterol. 2017;52:992–1000.
Masamune A, Nabeshima T, Kikuta K, et al. Prospective study of early chronic pancreatitis diagnosed based on the Japanese diagnostic criteria. J Gastroenterol. 2019;54:928–35.
Issa Y, Kempeneers MA, van Santvoort HC, et al. Diagnostic performance of imaging modalities in chronic pancreatitis: a systematic review and meta-analysis. Eur Radiol. 2017;27:3820–44.
Catalano MF, Sahai A, Levy M, et al. EUS-based criteria for the diagnosis of chronic pancreatitis: the Rosemont classification. Gastrointest Endosc. 2009;69:1251–61.
Engjom T, Sangnes DA, Havre RF, et al. Diagnostic accuracy of transabdominal ultrasound in chronic pancreatitis. Ultrasound Med Biol. 2017;43:735–43.
Buscail L, Escourrou J, Moreau J, et al. Endoscopic ultrasonography in chronic pancreatitis: a comparative prospective study with conventional ultrasonography, computed tomography, and ERCP. Pancreas. 1995;10:251–7.
Rösch T, Schusdziarra V, Born P, et al. Modern imaging methods versus clinical assessment in the evaluation of hospital in-patients with suspected pancreatic disease. Am J Gastroenterol. 2000;95:2261–70.
Manfredi R, Brizi MG, Masselli G, et al. Imaging of chronic pancreatitis. Rays. 2001;26:143–9.
Adamek HE, Albert J, Breer H, et al. Pancreatic cancer detection with magnetic resonance cholangiopancreatography and endoscopic retrograde cholangiopancreatography: a prospective controlled study. Lancet. 2000;356:190–3.
Pungpapong S, Wallace MB, Woodward TA, et al. Accuracy of endoscopic ultrasonography and magnetic resonance cholangiopancreatography for the diagnosis of chronic pancreatitis: a prospective comparison study. J Clin Gastroenterol. 2007;41:88–93.
Madzak A, Olesen SS, Wathle GK, et al. Secretin-stimulated magnetic resonance imaging assessment of the benign pancreatic disorders: systematic review and proposal for a standardized protocol. Pancreas. 2016;45:1092–103.
Trikudanathan G, Walker SP, Munigala S, et al. Diagnostic performance of contrast-enhanced MRI with secretin-stimulated MRCP for non-calcific chronic pancreatitis: a comparison with histopathology. Am J Gastroenterol. 2015;110:1598–606.
Sandrasegaran K, Tahir B, Barad U, et al. The value of secretin-enhanced MRCP in patients with recurrent acute pancreatitis. AJR Am J Roentgenol. 2017;208:315–21.
Irisawa A, Mishra G, Hernandez LV, et al. Quantitative analysis of endosonographic parenchymal echogenicity in patients with chronic pancreatitis. J Gastroenterol Hepatol. 2004;19:1199–205.
Yamabe A, Irisawa A, Bhutani MS, et al. Validity of endoscopic ultrasound findings of chronic pancreatitis: evaluation from the viewpoint of disease risk factors. Digestion. 2021;102:289–97.
Kuwahara T, Hirooka Y, Kawashima H, et al. Quantitative diagnosis of chronic pancreatitis using EUS elastography. J Gastroenterol. 2017;52:868–74.
Whitcomb DC, Gorry MC, Preston RA, et al. Hereditary pancreatitis is caused by a mutation in the cationic trypsinogen gene. Nat Genet. 1996;14:141–5.
Sharer N, Schwarz M, Malone G, et al. Mutations of the cystic fibrosis gene in patients with chronic pancreatitis. N Engl J Med. 1998;339:645–52.
Cohn JA, Friedman KJ, Noone PG, et al. Relation between mutations of the cystic fibrosis gene and idiopathic pancreatitis. N Engl J Med. 1998;339:653–8.
Witt H, Luck W, Hennies HC, et al. Mutations in the gene encoding the serine protease inhibitor, Kazal type 1 are associated with chronic pancreatitis. Nat Genet. 2000;25:213–6.
Rosendahl J, Witt H, Szmola R, et al. Chymotrypsin C (CTRC) variants that diminish activity or secretion are associated with chronic pancreatitis. Nat Genet. 2008;40:78–82.
Witt H, Beer S, Rosendahl J, et al. Variants in CPA1 are strongly associated with early onset chronic pancreatitis. Nat Genet. 2013;45:1216–20.
Masamune A, Kotani H, Sörgel FL, et al. Variants that affect function of calcium channel TRPV6 are associated with early-onset chronic pancreatitis. Gastroenterology. 2020;158:1626-1641.e8.
Masamune A, Kikuta K, Hamada S, et al. Nationwide survey of hereditary pancreatitis in Japan. J Gastroenterol. 2018;53:152–60.
Ellis I, Lerch MM, Whitcomb DC, et al. Genetic testing for hereditary pancreatitis: guidelines for indications, counselling, consent and privacy issues. Pancreatology. 2001;1:405–15.
Teich N, Mössner J. Hereditary chronic pancreatitis. Best Pract Res Clin Gastroenterol. 2008;22:115–30.
Gardner TB, Adler DG, Forsmark CE, et al. ACG clinical guideline: chronic pancreatitis. Am J Gastroenterol. 2020;115:322–39.
Hammer HF. Pancreatic exocrine insufficiency: diagnostic evaluation and replacement therapy with pancreatic enzymes. Dig Dis. 2010;28:339–43.
Domínguez-Muñoz JE. Pancreatic enzyme therapy for pancreatic exocrine insufficiency. Curr Gastroenterol Rep. 2007;9:116–22.
Shintakuya R, Uemura K, Murakami Y, et al. Sarcopenia is closely associated with pancreatic exocrine insufficiency in patients with pancreatic disease. Pancreatology. 2017;17:70–5.
Samokhvalov AV, Rehm J, Roerecke M. Alcohol consumption as a risk factor for acute and chronic pancreatitis: a systematic review and a series of meta-analysis. EBioMedicine. 2015;2:1996–2002.
Nikkola J, Räty S, Laukkarinen J, et al. Abstinence after first acute alcohol-associated pancreatitis protects against recurrent pancreatitis and minimizes the risk of pancreatic dysfunction. Alcohol Alcohol. 2013;48:483–6.
Takeyama Y. Long-term prognosis of acute pancreatitis in Japan. Clin Gastroenterol Hepatol. 2009;7(Suppl):S15–7.
Nordback I, Pelli H, Lappalainen-Lehto R, et al. The recurrence of acute alcohol-associated pancreatitis can be reduced: a randomized controlled trial. Gastroenterology. 2009;136:848–55.
Gupta N, Singh S, Vargas L, et al. Prevalence of low bone density and comorbid hypogonadism in patients with chronic pancreatitis. Pancreas. 2019;48:387–95.
Duggan SN, Smyth ND, Murphy A, et al. High prevalence of osteoporosis in patients with chronic pancreatitis: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2014;12:219–28.
Kumar KH, Sood AK, Manrai M. Occult metabolic bone disease in chronic pancreatitis. Niger J Clin Pract. 2017;20:1122–6.
Olesen SS, Büyükuslu A, Køhler M, et al. Sarcopenia associates with increased hospitalization rates and reduced survival in patients with chronic pancreatitis. Pancreatology. 2019;19:245–51.
Dominguez-Muñoz JE. Management of pancreatic exocrine insufficiency. Curr Opin Gastroenterol. 2019;35:455–9.
Bourliere M, Barthet M, Berthezene P, et al. Is tobacco a risk factor for chronic pancreatitis and alcoholic cirrhosis? Gut. 1991;32:1392–5.
Lévy P, Mathurin P, Roqueplo A, et al. A multidimensional case-control study of dietary, alcohol, and tobacco habits in alcoholic men with chronic pancreatitis. Pancreas. 1995;10:231–8.
Talamini G, Bassi C, Falconi M, et al. Alcohol and smoking as risk factors in chronic pancreatitis and pancreatic cancer. Dig Dis Sci. 1999;44:1303–11.
Lin Y, Tamakoshi A, Hayakawa T, et al. Cigarette smoking as a risk factor for chronic pancreatitis: a case-control study in Japan. Research Committee on intractable pancreatic diseases. Pancreas. 2000;21:109–14.
Rothenbacher D, Löw M, Hardt PD, et al. Prevalence and determinants of exocrine pancreatic insufficiency among older adults: results of a population-based study. Scand J Gastroenterol. 2005;40:697–704.
Tolstrup JS, Kristiansen L, Becker U, et al. Smoking and risk of acute and chronic pancreatitis among women and men: a population-based cohort study. Arch Intern Med. 2009;169:603–9.
Yadav D, Hawes RH, Brand RE, et al. Alcohol consumption, cigarette smoking, and the risk of recurrent acute and chronic pancreatitis. Arch Intern Med. 2009;169:1035–45.
Law R, Parsi M, Lopez R, et al. Cigarette smoking is independently associated with chronic pancreatitis. Pancreatology. 2010;10:54–9.
Nikkola J, Rinta-Kiikka I, Räty S, et al. Pancreatic morphological change in long-term follow-up after initial episode of acute alcoholic pancreatitis. J Gastrointest Surg. 2014;18:164–70 (discussion 170).
Ahmed Ali U, Issa Y, Hagenaars JC, et al. Risk of recurrent pancreatitis and progression to chronic pancreatitis after a first episode of acute pancreatitis. Clin Gastroenterol Hepatol. 2016;14:738–46.
Cavallini G, Talamini G, Vaona B, et al. Effect of alcohol and smoking on pancreatic lithogenesis in the course of chronic pancreatitis. Pancreas. 1994;9:42–6.
Imoto M, DiMagno EP. Cigarette smoking increases the risk of pancreatic calcification in late-onset but not early-onset idiopathic chronic pancreatitis. Pancreas. 2000;21:115–9.
Maisonneuve P, Lowenfels AB, Müllhaupt B, et al. Cigarette smoking accelerates progression of alcoholic chronic pancreatitis. Gut. 2005;54:510–4.
Maisonneuve P, Frulloni L, Müllhaupt B, et al. Impact of smoking on patients with idiopathic chronic pancreatitis. Pancreas. 2006;33:163–8.
Talamini G, Bassi C, Falconi M, et al. Smoking cessation at the clinical onset of chronic pancreatitis and risk of pancreatic calcifications. Pancreas. 2007;35:320–6.
Hirota M, Shimosegawa T, Masamune A, et al. The seventh nationwide epidemiological survey for chronic pancreatitis in Japan: clinical significance of smoking habit in Japanese patients. Pancreatology. 2014;14:490–6.
Luaces-Regueira M, Iglesias-García J, Lindkvist B, et al. Smoking as a risk for complications in chronic pancreatitis. Pancreas. 2014;43:275–80.
Kadiyala V, Lee LS, Banks PA, et al. Cigarette smoking impairs pancreatic duct cell bicarbonate secretion. JOP. 2013;14:31–8.
Delhaye M, Arvanitakis M, Verset G, et al. Long-term clinical outcome after endoscopic pancreatic ductal drainage for patients with painful chronic pancreatitis. Clin Gastroenterol Hepatol. 2004;2:1096–106.
Tantau A, Mandrutiu A, Leucuta DC, et al. Prognostic factors of response to endoscopic treatment in painful chronic pancreatitis. World J Gastroenterol. 2017;23:6884–93.
Seven G, Schreiner MA, Ross AS, et al. Lon-term outcomes associated with pancreatic extracorporeal shock wave lithotripsy for chronic calcific pancreatitis. Gastrointest Endosc. 2012;75:997-1004.e1.
Wilder-Smith CH, Hill L, Osler W, et al. Effect of tramadol and morphine on pain and gastrointestinal motor function in patients with chronic pancreatitis. Dig Dis Sci. 1999;44:1107–16.
Siepsiak M, Szałek E, Karbownik A, et al. Pharmacokinetics of paracetamol in patients with chronic pancreatitis. Pharmacol Rep. 2016;68:733–6.
Paisley P, Kinsella J. Pharmacological management of pain in chronic pancreatitis. Scott Med J. 2014;59:71–9.
American Gastroenterological Association. American Gastroenterological Association Medical Position Statement: treatment of pain in chronic pancreatitis. Gastroenterology. 1998;115:763–4.
Mössner J, Keim V, Niederau C, et al. Guidelines for therapy of chronic pancreatitis. Consensus Conference of the German Society of Digestive and Metabolic Diseases. Halle 21-23 November 1996. Z Gastroenterol (in German). 1998;36:359–67.
Talukdar R, Lakhtakia S, Nageshwar Reddy D, et al. Ameliorating effect of antioxidants and pregabalin combination in pain recurrence after ductal clearance in chronic pancreatitis: results of a randomized, double blind, placebo-controlled trial. J Gastroenterol Hepatol. 2016;31:1654–62.
Brown A, Hughes M, Tenner S, et al. Does pancreatic enzyme supplementation reduce pain in patients with chronic pancreatitis: a meta-analysis. Am J Gastroenterol. 1997;92:2032–5.
Yaghoobi M, McNabb-Baltar J, Bijarchi R, et al. Pancreatic enzyme supplements are not effective for relieving abdominal pain in patients with chronic pancreatitis: meta-analysis and systematic review of randomized controlled trials. Can J Gastroenterol Hepatol. 2016;2016(1–6):8541839.
Shafiq N, Rana S, Bhasin D, et al. Pancreatic enzymes for chronic pancreatitis. Cochrane Database Syst Rev. 2009;4:CD006302.
de la Iglesia-García D, Huang W, Szatmary P, et al. Efficacy of pancreatic enzyme replacement therapy in chronic pancreatitis: systematic review and meta-analysis. Gut. 2017;66:1354–5.
Gubergrits N, Malecka-Panas E, Lehman GA, et al. A 6-month, open-label clinical trial of pancrelipase delayed-release capsules (Creon) in patients with exocrine pancreatic insufficiency due to chronic pancreatitis or pancreatic surgery. Aliment Pharmacol Ther. 2011;33:1152–61.
Whitcomb DC, Lehman GA, Vasileva G, et al. Pancrelipase delayed-release capsules (Creon) for exocrine pancreatic insufficiency due to chronic pancreatitis or pancreatic surgery: a double-blind randomized trial. Am J Gastroenterol. 2010;105:2276–86.
Sai JK, Suyama M, Kubokawa Y, et al. Efficacy of camostat mesilate against dyspepsia associated with non-alcoholic mild pancreatic disease. J Gastroenterol. 2010;45:335–41.
Yamawaki H, Futagami S, Kaneko K, et al. Camostat mesilate, pancrelipase, and rabeprazol combination therapy improves epigastric pain in early chronic pancreatitis and functional dyspepsia with pancreatic enzyme abnormalities. Digestion. 2019;99:283–92.
Díte P, Ruzicka M, Zboril V, et al. A prospective, randomized trial comparing endoscopic and surgical therapy for chronic pancreatitis. Endoscopy. 2003;35:553–8.
Cahen DL, Gouma DJ, Nio Y, et al. Endoscopic versus surgical drainage of the pancreatic duct in chronic pancreatitis. N Engl J Med. 2007;356:676–84.
Cahen DL, Gouma DJ, Laramée P, et al. Long-term outcomes of endoscopic vs surgical drainage of the pancreatic duct in patients with chronic pancreatitis. Gastroenterology. 2011;141:1690–5.
Issa Y, Kempeneers MA, Bruno MJ, et al. Effect of early surgery vs endoscopy-first approach on pain in patients with chronic pancreatitis: the Escape randomized clinical trial. JAMA. 2020;323:237–47.
Yang CJ, Bliss LA, Schapira EF, et al. Systematic review of early surgery for chronic pancreatitis: impact on pain, pancreatic function, and re-intervention. J Gastrointest Surg. 2014;18:1863–9.
Jiang L, Ning D, Cheng Q, et al. Endoscopic versus surgical drainage treatment of calcific chronic pancreatitis. Int J Surg. 2018;54:242–7.
Farnbacher MJ, Mühldorfer S, Wehler M, et al. Interventional endoscopic therapy in chronic pancreatitis including temporary stenting: a definitive treatment? Scand J Gastroenterol. 2006;41:111–7.
Binmoeller KF, Jue P, Seifert H, et al. Endoscopic pancreatic stent drainage in chronic pancreatitis and a dominant stricture: long-term results. Endoscopy. 1995;27:638–44.
Boerma D, van Gulik TM, Rauws EA, et al. Outcome of pancreaticojejunostomy after previous endoscopic stenting in patients with chronic pancreatitis. Eur J Surg. 2005;168:223–8.
Ahmed Ali U, Pahlplatz JM, Nealon WH, et al. Endoscopic or surgical intervention for painful obstructive chronic pancreatitis. Cochrane Database Syst Rev. 2012;18:CD007884.
D’Haese JG, Ceyhan GO, Demir IE, et al. Treatment options in painful chronic pancreatitis: a systematic review. HPB (Oxford). 2014;16:512–21.
Jawad ZAR, Kyriakides C, Pai M, et al. Surgery remains the best option for the management of pain in patients with chronic pancreatitis: a systematic review and meta-analysis. Asian J Surg. 2017;40:179–85.
Jalal M, Campbell JA, Hopper AD. Practical guide to the management of chronic pancreatitis. Frontline Gastroenterol. 2019;10:253–60.
Dominguez-Munoz JE, Drewes AM, Lindkvist B, et al. Recommendations from the United European gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis. Pancreatology. 2018;18:847–54.
Thorat V, Reddy N, Bhatia S, et al. Randomised clinical trial: the efficacy and safety of pancreatin enteric-coated minimicrospheres (Creon 40000 MMS) in patients with pancreatic exocrine insufficiency due to chronic pancreatitis–a double-blind, placebo-controlled study. Aliment Pharmacol Ther. 2012;36:426–36.
Czakó L, Takács T, Hegyi P, et al. Quality of life assessment after pancreatic enzyme replacement therapy in chronic pancreatitis. Can J Gastroenterol. 2003;17:597–603.
Marotta F, O’Keefe SJ, Marks IN, et al. Pancreatic enzyme replacement therapy: importance of gastric acid secretion, H2-antagonists, and enteric coating. Dig Dis Sci. 1989;34:456–61.
Domínguez-Muñoz JE. Pancreatic enzyme replacement therapy for pancreatic exocrine insufficiency: when is it indicated, what is the goal and how to do it? Adv Med Sci. 2011;56:1–5.
Domínguez-Muñoz JE, Iglesias-García J, Iglesias-Rey M, et al. Optimising the therapy of exocrine pancreatic insufficiency by the association of a proton pump inhibitor to enteric coated pancreatic extracts. Gut. 2006;55:1056–7.
Delhaye M, Meuris S, Gohimont AC, et al. Comparative evaluation of a high lipase pancreatic enzyme preparation and a standard pancreatic supplement for treating exocrine pancreatic insufficiency in chronic pancreatitis. Eur J Gastroenterol Hepatol. 1996;8:699–703.
Sander-Struckmeier S, Beckmann K, Janssen-van Solingen G, et al. Retrospective analysis to investigate the effect of concomitant use of gastric acid-suppressing drugs on the efficacy and safety of pancrelipase/pancreatin (CREON®) in patients with pancreatic exocrine insufficiency. Pancreas. 2013;42:983–9.
O’Brien SJ, Omer E. Chronic pancreatitis and nutrition therapy. Nutr Clin Pract. 2019;34(Suppl 1):S13–26.
Duggan SN, Ewald N, Kelleher L, et al. The nutritional management of type 3c (pancreatogenic) diabetes in chronic pancreatitis. Eur J Clin Nutr. 2017;71:3–8.
Kawabe K, Ito T, Igarashi H, et al. The current managements of pancreatic diabetes in Japan. Clin J Gastroenterol. 2009;2:1–8.
Ito T, Otsuki M, Igarashi H, et al. Epidemiological study of pancreatic diabetes in japan in 2005: a nationwide study. Pancreas. 2010;39:829–35.
Niebisz-Cieślak AB, Karnafel W. Insulin sensitivity in chronic pancreatitis and features of insulin resistance syndrome. Pol Arch Med Wewn. 2010;120:255–63.
Hart PA, Bellin MD, Andersen DK, et al. Type 3c (pancreatogenic) diabetes mellitus secondary to chronic pancreatitis and pancreatic cancer. Lancet Gastroenterol Hepatol. 2016;1:226–37.
Stevens RJ, Ali R, Bankhead CR, et al. Cancer outcomes and all-cause mortality in adults allocated to metformin: systematic review and collaborative meta-analysis of randomised clinical trials. Diabetologia. 2012;55:2593–603.
Araki E, Goto A, Kondo T, et al. Japanese clinical practice guideline for diabetes 2019. Diabetol Int. 2020;11:165–223.
Terzin V, Takács R, Lengyel C, et al. Improved glycemic control in pancreatic diabetes through intensive conservative insulin therapy. Pancreatology. 2012;12:100–3.
Dumonceau JM, Delhaye M, Tringali A, et al. Endoscopic treatment of chronic pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) guideline-updated August 2018. Endoscopy. 2019;51:179–93.
Andrén-Sandberg A, Dervenis C. Pancreatic pseudocysts in the 21st century Part II: natural history. JOP. 2004;5:64–70.
Khan MA, Hammad T, Khan Z, et al. Endoscopic versus percutaneous management for symptomatic pancreatic fluid collections: a systematic review and meta-analysis. Endosc Int Open. 2018;6:E474–83.
Zhao X, Feng T, Ji W. Endoscopic versus surgical treatment for pancreatic pseudocyst. Dig Endosc. 2016;28:83–91.
Bang JY, Hawes R, Bartolucci A, et al. Efficacy of metal and plastic stents for transmural drainage of pancreatic fluid collections: a systematic review. Dig Endosc. 2015;27:486–98.
Chen YI, Khashab MA, Adam V, et al. Plastic stents are more cost-effective than lumen-apposing metal stents in management of pancreatic pseudocysts. Endosc Int Open. 2018;6:E780–8.
Garg PK, Meena D, Babu D, et al. Endoscopic versus laparoscopic drainage of pseudocyst and walled-off necrosis following acute pancreatitis: a randomized trial. Surg Endosc. 2020;34:1157–66.
O’Toole D, Vullierme MP, Ponsot P, et al. Diagnosis and management of pancreatic fistulae resulting in pancreatic ascites or pleural effusions in the era of helical CT and magnetic resonance imaging. Gastroenterol Clin Biol. 2007;31:686–93.
Kurumboor P, Varma D, Rajan M, et al. Outcome of pancreatic ascites in patients with tropical calcific pancreatitis managed using a uniform treatment protocol. Indian J Gastroenterol. 2009;28:102–6.
Chebli JM, Gaburri PD, de Souza AF, et al. Internal pancreatic fistulas: proposal of a management algorithm based on a case series analysis. J Clin Gastroenterol. 2004;38:795–800.
Olakowski M, Mieczkowska-Palacz H, Olakowska E, et al. Surgical management of pancreaticopleural fistulas. Acta Chir Belg. 2009;109:735–40.
Tajima Y, Tsutsumi R, Kuroki T, et al. Evaluation and management of thoracopancreatic fistula. Surgery. 2006;140:773–8.
Dumonceau JM, Tringali A, Blero D, et al. Biliary stenting: indications, choice of stents and results: European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline. Endoscopy. 2012;44:277–98.
Siiki A, Helminen M, Sand J, et al. Covered self-expanding metal stents may be preferable to plastic stents in the treatment of chronic pancreatitis-related biliary strictures: a systematic review comparing 2 methods of stent therapy in benign biliary strictures. J Clin Gastroenterol. 2014;48:635–43.
Haapamäki C, Kylänpää L, Udd M, et al. Randomized multicenter study of multiple plastic stents vs. Covered self-expandable metallic stent in the treatment of biliary stricture in chronic pancreatitis. Endoscopy. 2015;47:605–10.
Hu B, Sun B, Cai Q, et al. Asia-Pacific consensus guidelines for endoscopic management of benign biliary strictures. Gastrointest Endosc. 2017;86:44–58.
Dumonceau JM, Tringali A, Papanikolaou IS, et al. Endoscopic biliary stenting: indications, choice of stents, and results: European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline-updated. Endoscopy. 2017;50:910–30.
Ueda J, Tanaka M, Ohtsuka T, et al. Surgery for chronic pancreatitis decreases the risk for pancreatic cancer: a multicenter retrospective analysis. Surgery. 2013;153:357–64.
Kempeneers MA, Issa Y, Ali UA, et al. International consensus guidelines for surgery and the timing of intervention in chronic pancreatitis. Pancreatology. 2020;20:149–57.
Löhr JM, Dominguez-Munoz E, Rosendahl J, et al. United European gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis (HaPanEU). United European Gastroenterol J. 2017;5:153–99.
Nealon WH, Thompson JC. Progressive loss of pancreatic function in chronic pancreatitis is delayed by main pancreatic duct decompression. A longitudinal prospective analysis of the modified puestow procedure. Ann Surg. 1993;217:458–66 (discussion 466).
Ahmed Ali U, Nieuwenhuijs VB, van Eijck CH, et al. Clinical outcome in relation to timing of surgery in chronic pancreatitis: a nomogram to predict pain relief. Arch Surg. 2012;147:925–32.
Riediger H, Adam U, Fischer E, et al. Long-term outcome after resection for chronic pancreatitis in 224 patients. J Gastrointest Surg. 2007;11:949–59 (discussion 959–60).
Zhou Y, Shi B, Wu L, et al. Frey procedure for chronic pancreatitis: evidence-based assessment of short- and long-term results in comparison to pancreatoduodenectomy and Beger procedure: a meta-analysis. Pancreatology. 2015;15:372–9.
Acknowledgements
This article was supported by a Grant-in-Aid from the JSGE. The authors thank Keijiro Ueda (Neuroendocrine Tumor Centre, Fukuoka Sanno Hospital), Takamasa Oono (Department of Medicine and Bioregulatory Science, Graduate School of Medical Sciences, Kyushu University), Keiko Kamei (Department of Surgery, Kindai University Faculty of Medicine), Kazuhiro Kikuta (Division of Gastroenterology, Tohoku University Graduate School of Medicine), Yuki Koyama (Department of Gastroenterology and Hepatology, Kyoto Prefectural University of Medicine), Yuki Sawai (Department of Gastroenterology and Hepatology, Kyoto Prefectural University of Medicine),Yoshio Sogame (Department of Gastroenterology and Hepatology, Kyoto Prefectural University of Medicine), Katsuyuki Dainaka (Department of Gastroenterology and Hepatology, Kyoto Prefectural University of Medicine), Tomoki Takata (Department of Gastroenterology and Hepatology, Kyoto Prefectural University of Medicine), Yu Takamatsu (Department of Medicine and Bioregulatory Science, Graduate School of Medical Sciences, Kyushu University), Tetsuya Takikawa (Division of Gastroenterology, Tohoku University Graduate School of Medicine), Ayumu Takeno (Department of Medicine and Bioregulatory Science, Graduate School of Medical Sciences, Kyushu University), Keisuke Takemura (Department of Gastroenterology and Hepatology, Kyoto Prefectural University of Medicine), Katsuhito Teramatsu (Department of Medicine and Bioregulatory Science, Graduate School of Medical Sciences, Kyushu University), Kenji Notohara (Department of Pathology, Kurashiki Central Hospital), Shin Hamada (Division of Gastroenterology, Tohoku University Graduate School of Medicine), Kazuki Hayashi (Department of Gastroenterology and Metabolism, Nagoya City University Graduate School of Medical Sciences), Kazuhide Matsumoto (Department of Medicine and Bioregulatory Science, Graduate School of Medical Sciences, Kyushu University), Hayato Miyake (Department of Gastroenterology and Hepatology, Kyoto Prefectural University of Medicine), Hiroaki Yasuda (Department of Gastroenterology and Hepatology, Kyoto Prefectural University of Medicine), and Akira Yamamiya (Department of Gastroenterology, Dokkyo Medical University School of Medicine)
Author information
Authors and Affiliations
Contributions
Writing—original draft: TI, KS, AI, TO, HO, AK, MK, JS, NS, YT, JT, MH, NF, and AM. Writing—review and editing: KS and TI. Supervision: TS, MS, HI, KO, TK, HM, and KK. Approval of final manuscript: all authors.
Corresponding author
Ethics declarations
Conflict of interest
Any financial relationship with enterprises, businesses, or academic institutions in the subject matter or materials discussed in the manuscript is listed as follows: (1) those from which the authors, the spouse, partner or immediate relatives of the authors have received individually any income, honoraria or any other type of renumeration; Teijin Phrma, Novartis Pharma, Mylan EPD, Olympus, Asahi Kasei Pharna, EA Pharma, Otsuka Pharmaceutical, Daiichi-Sankyo, Takeda Pharmaceutical; (2) those from which the academic institutions of the authors received manuscript fee; Olympus, Mylan EPD; (3) those from which the authors have received scholarship/research grant; Tsumura, Bristol Myers Squibb, Toray, Astellas, Abbvie, EA Pharma, Eisai, MSD, Ono Pharmaceutical, Covidien Japan, Taiho Pharma, Takeda Pharmaceutical, Chugai Pharmaceutical, Novartis Pharma, Bayer Yakuhin, Asahi Kasei Pharna, Nippon Kayaku, Mochida Pharmaceutical, Jonson & Johnson, Otsuka Pharmaceutical, Daiichi Sankyo, Mitsubishi Tanabe Pharma, Cyubu Health Insurance Society; and (4) those from which the authors have received individually endowed chair; SNBL Japan, Chugai Pharmaceutical, City of Iga, Aichi Prefectural Government, Aichi Prefectural Welfare Agricultural Cooperative Union, Aichi Municipal Promotion Association, City of Nagoya.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The members of the Guidelines Committee are listed in the Appendix.
Appendices
Appendix
The members of the Guidelines committee who created and evaluated the Japanese Society of Gastroenterology ‘‘Evidence-based clinical practice guidelines for chronic pancreatitis’’ are listed below.
Creation committee
Chair: Tetsuhide Ito (Neuroendocrine Tumor Centre, Fukuoka Sanno Hospital, International University of Health and Welfare). Vice Chair: Kyoko Shimizu (Department of Gastroenterology, Tokyo Women’s Medical University).
Members: Atsushi Irisawa (Department of Gastroenterology, Dokkyo Medical University School of Medicine), Takao Ohtsuka (Department of Digestive Surgery, Breast and Thyroid Surgery, Kagoshima University Graduate School of Medical and Dental Science), Hirotaka Ohara (Department of Community-Based Medical Education, Nagoya City University Graduate School of Medical Sciences), Atsushi Kanno (Department of Medicine, Division of Gastroenterology, Jichi Medical University), Mitsuhiro Kida (Department of Gastroenterology, Kitasato University School of Medicine), Junichi Sakagami (Fukuchiyama City Hospital), Naohiro Sata (Department of Surgery, Jichi Medical University), Yoshifumi Takeyama (Department of Surgery, Kindai University Faculty of Medicine), Junko Tahara (Department of Gastroenterology, Tokyo Women’s Medical University), Morihisa Hirota (Division of Gastroenterology, Tohoku Medical and Pharmaceutical University), Nao Fujimori (Department of Medicine and Bioregulatory Science, Graduate School of Medical Sciences, Kyushu University), and Atsushi Masamune (Division of Gastroenterology, Tohoku University Graduate School of Medicine).
Evaluation committee
Chair: Tooru Shimosegawa (South Miyagi Medical Center). Vice Chair: Masanori Sugiyama (Tokyo Rosai Hospital). Members: Hiroshi Ishiguro (Nagoya University Graduate School of Medicine), Kazuichi Okazaki (Kansai Medical University Kori Hospital), Terumi Kamisawa (Tokyo Metropolitan Komagome Hospital), Hiroyuki Miyagawa (Sapporo Kohsei Hospital), and Keisho Kataoka (Otsu City Hospital).
The Japanese society of gastroenterology
President: Kazuhiko Koike (Kanto Central Hospital). Past President: Tooru Shimosegawa (South Miyagi Medical Center). Directors Responsible: Satoshi Mochida (Department of Gastroenterology and Hepatology, Saitama Medical University) and Nobuyuki Enomoto (First Department of Internal Medicine, Faculty of Medicine, University of Yamanashi).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shimizu, K., Ito, T., Irisawa, A. et al. Evidence-based clinical practice guidelines for chronic pancreatitis 2021. J Gastroenterol 57, 709–724 (2022). https://doi.org/10.1007/s00535-022-01911-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-022-01911-6