
Abstract
Background
In critically ill children with acute kidney injury (AKI), continuous kidney replacement therapy (CKRT) enables nutrition provision. The magnitude of amino acid loss during continuous venovenous hemodiafiltration (CVVHDF) is unknown and needs accurate quantification. We investigated the mass removal and clearance of amino acids in pediatric CVVHDF.
Methods
This is a prospective observational cohort study of patients receiving CVVHDF from August 2014 to January 2016 in the pediatric intensive care unit (PICU) of a tertiary children’s hospital.
Results
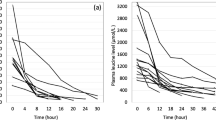
Fifteen patients (40% male, median age 2.0 (IQR 0.7, 8.0) years) were enrolled. Median PICU and hospital lengths of stay were 20 (9, 59) and 36 (22, 132) days, respectively. Overall survival to discharge was 66.7%. Median daily protein prescription was 2.00 (1.25, 2.80) g/kg/day. Median daily amino acid mass removal was 299.0 (174.9, 452.0) mg/kg body weight, and median daily amino acid mass clearance was 18.2 (13.5, 27.9) ml/min/m2, resulting in a median 14.6 (8.3, 26.7) % protein loss. The rate of amino acid loss increased with increasing dialysis dose and blood flow rate.
Conclusion
CVVHDF prescription and related amino acid loss impact nutrition provision, with 14.6% of the prescribed protein removed. Current recommendations for protein provision for children requiring CVVHDF should be adjusted to compensate for circuit-related loss.
Graphical abstract

A higher resolution version of the Graphical abstract is available as Supplementary information


Similar content being viewed by others


Abbreviations
- ACD-A:
-
Anticoagulant citrate dextrose solution A
- AKI:
-
Acute kidney injury
- ARF:
-
Acute renal failure
- BFR:
-
Blood flow rate
- BSA:
-
Body surface area
- BUN:
-
Blood urea nitrogen
- CKRT:
-
Continuous kidney replacement therapy
- CVVH:
-
Continuous venovenous hemofiltration
- CVVHD:
-
Continuous venovenous hemodialysis
- CVVHDF:
-
Continuous venovenous hemodiafiltration
- ECMO:
-
Extracorporeal membrane oxygenation
- FUN:
-
Fluid urea nitrogen
- IQR:
-
Interquartile range
- NPO:
-
Nil per os
- PELOD:
-
Pediatric logistic organ dysfunction
- PICU:
-
Pediatric intensive care unit
- pRIFLE:
-
Pediatric version of RIFLE (Risk of renal dysfunction; Injury to kidney; Failure of kidney function; Loss of kidney function, End-stage renal disease)
- PRISM-III:
-
Pediatric risk of mortality
- REE:
-
Resting energy expenditure
References
Kaddourah A, Basu RK, Bagshaw SM, Goldstein SL, AWARE Investigators (2017) Epidemiology of acute kidney injury in critically ill children and young adults. N Engl J Med 376:11–20. https://doi.org/10.1056/NEJMoa1611391
Gupta S, Sengar GS, Meti PK, Lahoti A, Beniwal M, Kumawat M (2016) Acute kidney injury in pediatric intensive care unit: incidence, risk factors, and outcome. Indian J Crit Care Med 20:526–529. https://doi.org/10.4103/0972-5229.190368
Hui WF, Chan WK, Miu TY (2013) Acute kidney injury in the paediatric intensive care unit: identification by modified RIFLE criteria. Hong Kong Med J 19:13–19
Basu RK, Wheeler DS, Goldstein S, Doughty L (2011) Acute renal replacement therapy in pediatrics. Int J Nephrol 2011:785392. https://doi.org/10.4061/2011/785392
Boschee ED, Cave DA, Garros D, Lequier L, Granoski DA, Guerra GG, Ryerson LM (2014) Indications and outcomes in children receiving renal replacement therapy in pediatric intensive care. J Crit Care 29:37–42. https://doi.org/10.1016/j.jcrc.2013.09.008
Druml W (2005) Nutritional management of acute renal failure. J Ren Nutr 15:63–70. https://doi.org/10.1053/j.jrn.2004.09.012
Druml W, Burger U, Kleinberger G, Lenz K, Laggner A (1986) Elimination of amino acids in acute renal failure. Nephron 42:62–67. https://doi.org/10.1159/000183635
Kyle UG, Akcan-Arikan A, Orellana RA, Coss-Bu JA (2013) Nutrition support among critically ill children with AKI. Clin J Am Soc Nephrol 8:568–574. https://doi.org/10.2215/CJN.05790612
Kyle UG, Jaimon N, Coss-Bu JA (2012) Nutrition support in critically ill children: underdelivery of energy and protein compared with current recommendations. J Acad Nutr Diet 112:1987–1992. https://doi.org/10.1016/j.jand.2012.07.038
Fortenberry JD, Paden ML, Goldstein SL (2013) Acute kidney injury in children: an update on diagnosis and treatment. Pediatr Clin N Am 60:669–688. https://doi.org/10.1016/j.pcl.2013.02.006
Daniels RC, Bunchman TE (2013) Renal complications and therapy in the PICU: hypertension, CKD, AKI, and RRT. Crit Care Clin 29:279–299. https://doi.org/10.1016/j.ccc.2013.01.002
Macias WL, Alaka KJ, Murphy MH, Miller ME, Clark WR, Mueller BA (1996) Impact of the nutritional regimen on protein catabolism and nitrogen balance in patients with acute renal failure. JPEN J Parenter Enteral Nutr 20:56–62. https://doi.org/10.1177/014860719602000156
Bellomo R, Tan HK, Bhonagiri S, Gopal I, Seacombe J, Daskalakis M, Boyce N (2002) High protein intake during continuous hemodiafiltration: impact on amino acids and nitrogen balance. Int J Artif Organs 25:261–268. https://doi.org/10.1177/039139880202500403
Castillo A, Santiago MJ, Lopez-Herce J, Montoro S, Lopez J, Bustinza A, Moral R, Bellon JM (2012) Nutritional status and clinical outcome of children on continuous renal replacement therapy: a prospective observational study. BMC Nephrol 13:125. https://doi.org/10.1186/1471-2369-13-125
Scheinkestel CD, Adams F, Mahony L, Bailey M, Davies AR, Nyulasi I, Tuxen DV (2003) Impact of increasing parenteral protein loads on amino acid levels and balance in critically ill anuric patients on continuous renal replacement therapy. Nutrition 19:733–740. https://doi.org/10.1016/s0899-9007(03)00107-2
Symons JM, Chua AN, Somers MJ, Baum MA, Bunchman TE, Benfield MR, Brophy PD, Blowey D, Fortenberry JD, Chand D, Flores FX, Hackbarth R, Alexander SR, Mahan J, McBryde KD, Goldstein SL (2007) Demographic characteristics of pediatric continuous renal replacement therapy: a report of the prospective pediatric continuous renal replacement therapy registry. Clin J Am Soc Nephrol 2:732–738. https://doi.org/10.2215/CJN.03200906
Oh WC, Gardner DS, Devonald MA (2015) Micronutrient and amino acid losses in acute renal replacement therapy. Curr Opin Clin Nutr Metab Care 18:593–598. https://doi.org/10.1097/MCO.0000000000000220
Btaiche IF, Mohammad RA, Alaniz C, Mueller BA (2008) Amino Acid requirements in critically ill patients with acute kidney injury treated with continuous renal replacement therapy. Pharmacotherapy 28:600–613. https://doi.org/10.1592/phco.28.5.600
Zappitelli M, Goldstein SL, Symons JM, Somers MJ, Baum MA, Brophy PD, Blowey D, Fortenberry JD, Chua AN, Flores FX, Benfield MR, Alexander SR, Askenazi D, Hackbarth R, Bunchman TE, Prospective Pediatric Continuous Renal Replacement Therapy Registry Group (2008) Protein and calorie prescription for children and young adults receiving continuous renal replacement therapy: a report from the Prospective Pediatric Continuous Renal Replacement Therapy Registry Group. Crit Care Med 36:3239–3245. https://doi.org/10.1097/CCM.0b013e31818f3f40
(1985) Energy and protein requirements. Report of a joint FAO/WHO/UNU Expert Consultation. World Health Organ Tech Rep Ser 724:1–206
Mehta NM, Compher C, A.S.P.E.N. Board of Directors (2009) A.S.P.E.N. Clinical Guidelines: nutrition support of the critically ill child. JPEN J Parenter Enteral Nutr 33:260–276. https://doi.org/10.1177/0148607109333114
Akcan-Arikan A, Zappitelli M, Loftis LL, Washburn KK, Jefferson LS, Goldstein SL (2007) Modified RIFLE criteria in critically ill children with acute kidney injury. Kidney Int 71:1028–1035. https://doi.org/10.1038/sj.ki.5002231
Goldstein SL, Currier H, Graf C, Cosio CC, Brewer ED, Sachdeva R (2001) Outcome in children receiving continuous venovenous hemofiltration. Pediatrics 107:1309–1312. https://doi.org/10.1542/peds.107.6.1309
Pollack MM, Patel KM, Ruttimann UE (1996) PRISM III: an updated pediatric risk of mortality score. Crit Care Med 24:743–752. https://doi.org/10.1097/00003246-199605000-00004
Costa GA, Delgado AF, Ferraro A, Okay TS (2010) Application of the pediatric risk of mortality (PRISM) score and determination of mortality risk factors in a tertiary pediatric intensive care unit. Clinics (Sao Paulo) 65:1087–1092. https://doi.org/10.1590/s1807-59322010001100005
Pereira M, Rodrigues N, Godinho I, Gameiro J, Neves M, Gouveia J, Costa ESZ, Lopes JA (2017) Acute kidney injury in patients with severe sepsis or septic shock: a comparison between the ' Risk, Injury, Failure, Loss of kidney function, End-stage kidney disease ' (RIFLE), Acute Kidney Injury Network (AKIN) and Kidney Disease: Improving Global Outcomes (KDIGO) classifications. Clin Kidney J 10:332–340. https://doi.org/10.1093/ckj/sfw107
Leteurtre S, Duhamel A, Salleron J, Grandbastien B, Lacroix J, Leclerc F, Groupe Francophone de Réanimation et d’Urgences Pédiatriques (GFRUP) (2013) PELOD-2: an update of the PEdiatric logistic organ dysfunction score. Crit Care Med 41:1761–1773. https://doi.org/10.1097/CCM.0b013e31828a2bbd
Waterlow JC (1972) Classification and definition of protein-calorie malnutrition. Br Med J 3:566–569. https://doi.org/10.1136/bmj.3.5826.566
Zappitelli M, Juarez M, Castillo L, Coss-Bu J, Goldstein SL (2009) Continuous renal replacement therapy amino acid, trace metal and folate clearance in critically ill children. Intensive Care Med 35:698–706. https://doi.org/10.1007/s00134-009-1420-9
Maxvold NJ, Smoyer WE, Custer JR, Bunchman TE (2000) Amino acid loss and nitrogen balance in critically ill children with acute renal failure: a prospective comparison between classic hemofiltration and hemofiltration with dialysis. Crit Care Med 28:1161–1165. https://doi.org/10.1097/00003246-200004000-00041
Prowle JR, Schneider A, Bellomo R (2011) Clinical review: optimal dose of continuous renal replacement therapy in acute kidney injury. Crit Care 15:207. https://doi.org/10.1186/cc9415
Claure-Del Granado R, Macedo E, Chertow GM, Soroko S, Himmelfarb J, Ikizler TA, Paganini EP, Mehta RL (2011) Effluent volume in continuous renal replacement therapy overestimates the delivered dose of dialysis. Clin J Am Soc Nephrol 6:467–475. https://doi.org/10.2215/CJN.02500310
Wong Vega M, Juarez Calderon M, Tufan Pekkucuksen N, Srivaths P, Akcan Arikan A (2019) Feeding modality is a barrier to adequate protein provision in children receiving continuous renal replacement therapy (CRRT). Pediatr Nephrol 34:1147–1150. https://doi.org/10.1007/s00467-019-04211-z
Vega MW, Juarez M, Lee JY, Srivaths P, Williams E, Akcan Arikan A (2018) Quality improvement bedside rounding audits enhance protein provision for pediatric patients receiving continuous renal replacement therapy. Pediatr Crit Care Med 19:1054–1058. https://doi.org/10.1097/PCC.0000000000001698
Stevenson JM, Heung M, Vilay AM, Eyler RF, Patel C, Mueller BA (2013) In vitro glucose kinetics during continuous renal replacement therapy: implications for caloric balance in critically ill patients. Int J Artif Organs 36:861–868. https://doi.org/10.5301/ijao.5000232
Acknowledgements
We would like to acknowledge the collaborative efforts of the Texas Children’s Hospital Pediatric Intensive Care Unit, the Nephrology Department Physician and Nursing Staff, and the Critical Care Research Team, in particular Nancy Jaimon and Daphne Peoples, without whom this study would not have been possible. We also would like to thank Mr. Uluc Arikan for his assistance with figures.
Availability of data and material
Deidentified data will be available from the authors by way of Baylor College of Medicine Institutional Review Board.
Code availability
Not applicable.
Funding
This study is supported by the Texas Children’s Hospital Pediatric Pilot Award.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
The study was approved by Baylor College of Medicine Institutional Review Board.
Consent to participate
Parental permission was obtained from all subjects’ parents/guardians.
Consent for publication
Not applicable.
Conflict of interest
The authors have no financial relationships relevant to this article to disclose.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(PPTX 1433 kb)
Rights and permissions
About this article

Cite this article
Lion, R.P., Vega, M.R., Smith, E. et al. The effect of continuous venovenous hemodiafiltration on amino acid delivery, clearance, and removal in children. Pediatr Nephrol 37, 433–441 (2022). https://doi.org/10.1007/s00467-021-05162-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-021-05162-0