
Abstract
Background
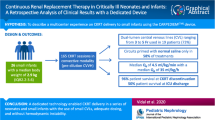
The Cardio-Renal Pediatric Dialysis Emergency Machine (CA.R.P.E.D.I.E.M.®) device is a continuous kidney replacement therapy (CKRT) equipment dedicated to neonates and small infants. This study aimed to assess the effectiveness, feasibility, outcomes, and technical considerations relating to CARPEDIEM® use.
Methods
This retrospective multicenter study included 19 newborns and six infants receiving CARPEDIEM® in five French pediatric and neonatal intensive care units. Laboratory parameters were collected at the initiation and end of the first CARPEDIEM® session. Results are presented as median [IQR] (range).
Results
At initiation, age was 4 days [2–13] (1–1134) with a body weight of 3.3 kg [2.5–4] (1.3–11.1). Overall, 131 sessions and 2125 h of treatment were performed. Treatment duration per patient was 42 h [24–91] (8–557). Continuous veno-venous hemofiltration (CVVH) was performed in 20 children. Blood flow rate was 8 mL/kg/min [6–9] (3–16). The effluent flow rate for CVVH was 74 mL/kg/h [43–99] (28–125) and net ultrafiltration (UF) 6 mL/kg/h [2–8] (1–12). In the five children treated by hemodialysis, the blood and dialysate flow rates were 6 mL/kg/min [5–7] (4–7) and 600 mL/h [300–600] (120–600), respectively, while session duration was 8 h [6–12] (2–24). Most infants required a catheter between 4.5 and 6.5 French. Hemodynamic instability with a need for volume replacement occurred in 31 sessions (23%). Thrombocytopenia was observed in 29 sessions (22%). No hemorrhage occurred; all the patients survived the sessions, but only eight patients (32%) were alive at hospital discharge.
Conclusions
These data confirm that the use of CARPEDIEM® is safe and effective in critically ill neonates and infants.
Graphical abstract

A higher resolution version of the Graphical abstract is available as Supplementary information

Similar content being viewed by others


Data availability
The data is available if requested from the corresponding author.
References
Sutherland SM, Ji J, Sheikhi FH, Ling XB et al (2013) AKI in hospitalized children: epidemiology and clinical associations in a national cohort. Clin J Am Soc Nephrol 8:1661–1669. https://doi.org/10.2215/CJN.00270113
Jetton JG, Boohaker LJ, Sethi SK, Askenazi DJ et al (2017) Incidence and outcomes of neonatal acute kidney injury (AWAKEN): a multicentre, multinational, observational cohort study. Lancet Child Adolesc Health 1:184–194. https://doi.org/10.1016/S2352-4642(17)30069-X
de Galasso L, Picca S, Guzzo I (2020) Dialysis modalities for the management of pediatric acute kidney injury. Pediatr Nephrol 35:753–765. https://doi.org/10.1007/s00467-019-04213-x
Ronco C, Brendolan A, Bragantini L, La Greca G et al (1986) Treatment of acute renal failure in newborns by continuous arterio-venous hemofiltration. Kidney Int 29:908–915. https://doi.org/10.1038/ki.1986.85
Ronco C, Garzotto F, Brendolan A, Goldstein SL et al (2014) Continuous renal replacement therapy in neonates and small infants: development and first-in-human use of a miniaturised machine (CARPEDIEM). Lancet 383:1807–1813. https://doi.org/10.1016/S0140-6736(14)60799-6
Ronco C, Garzotto F, Ricci Z (2012) CA.R.PE.DI.E.M. (cardio-renal pediatric dialysis emergency machine): evolution of continuous renal replacement therapies in infants A personal journey. Pediatr Nephrol 27:1203–1211. https://doi.org/10.1007/s00467-012-2179-8
Lorenzin A, Garzotto F, Alghisi A, Ronco C et al (2016) CVVHD treatment with CARPEDIEM: small solute clearance at different blood and dialysate flows with three different surface area filter configurations. Pediatr Nephrol 31:1659–1665. https://doi.org/10.1007/s00467-016-3397-2
Vidal E, Cocchi E, Paglialonga F, Ronco C et al (2019) Continuous veno-venous hemodialysis using the Cardio-Renal Pediatric Dialysis Emergency MachineTM: first clinical experiences. BPU 47:149–155. https://doi.org/10.1159/000494437
Garzotto F, Vidal E, Ricci Z, Ronco C et al (2020) Continuous kidney replacement therapy in critically ill neonates and infants: a retrospective analysis of clinical results with a dedicated device. Pediatr Nephrol 35:1699–1705. https://doi.org/10.1007/s00467-020-04562-y
Schwartz GJ, Work DF (2009) Measurement and estimation of GFR in children and adolescents. Clin J Am Soc Nephrol 4:1832–1843. https://doi.org/10.2215/CJN.01640309
Goldstein SL, Vidal E, Ricci Z, Ronco C et al (2022) Survival of infants treated with CKRT: comparing adapted adult platforms with the CarpediemTM. Pediatr Nephrol 37:667–675. https://doi.org/10.1007/s00467-021-05180-y
Sethi SK, Raina R, Rana A, Wazir S et al (2022) Validation of the STARZ neonatal acute kidney injury risk stratification score. Pediatr Nephrol 37:1923–1932. https://doi.org/10.1007/s00467-021-05369-1
Gorga SM, Sahay RD, Askenazi DJ, Selewski DT et al (2020) Fluid overload and fluid removal in pediatric patients on extracorporeal membrane oxygenation requiring continuous renal replacement therapy: a multicenter retrospective cohort study. Pediatr Nephrol 35:871–882. https://doi.org/10.1007/s00467-019-04468-4
Selewski DT, Cornell TT, Lombel RM, Heung M et al (2011) Weight-based determination of fluid overload status and mortality in pediatric intensive care unit patients requiring continuous renal replacement therapy. Intensive Care Med 37:1166–1173. https://doi.org/10.1007/s00134-011-2231-3
Alobaidi R, Morgan C, Basu RK, Bagshaw SM et al (2018) Association between fluid balance and outcomes in critically ill children: a systematic review and meta-analysis. JAMA Pediatr 172:257–268. https://doi.org/10.1001/jamapediatrics.2017.4540
Fayad AI, Buamscha DG, Ciapponi A (2016) Intensity of continuous renal replacement therapy for acute kidney injury. Cochrane Database Syst Rev 10:CD010613. https://doi.org/10.1002/14651858.CD010613.pub2
Naorungroj T, Neto AS, Zwakman-Hessels L, Bellomo R et al (2021) Early net ultrafiltration rate and mortality in critically ill patients receiving continuous renal replacement therapy. Nephrol Dial Transplant 36:1112–1119. https://doi.org/10.1093/ndt/gfaa032
Murugan R, Kerti SJ, Chang C-CH, Bellomo R et al (2019) Association of net ultrafiltration rate with mortality among critically ill adults with acute kidney injury receiving continuous venovenous hemodiafiltration: a Secondary Analysis of the Randomized Evaluation of Normal vs Augmented Level (RENAL) of Renal Replacement Therapy Trial. JAMA Netw Open 2:e195418. https://doi.org/10.1001/jamanetworkopen.2019.5418
Khwaja A (2012) KDIGO clinical practice guidelines for acute kidney injury. NEC 120:c179–c184. https://doi.org/10.1159/000339789
Vinsonneau C, Allain-Launay E, Blavau C, Vong LV (2015) Épuration extrarénale en réanimation adulte et pédiatrique - La SFAR. Société Française d’Anesthésie et de Réanimation. https://sfar.org/epuration-extrarenale-en-reanimation-adulte-et-pediatrique/. Accessed 4 May 2022
Werner HA, Herbertson MJ, Seear MD (1994) Functional characteristics of pediatric veno-venous hemofiltration. Crit Care Med 22:320–325. https://doi.org/10.1097/00003246-199402000-00025
Kaempfen S, Dutta-Kukreja P, Mok Q (2017) Continuous venovenous hemofiltration in children less than or equal to 10 kg: a single-center experience. Pediatr Crit Care Med 18:e70–e76. https://doi.org/10.1097/PCC.0000000000001030
Hackbarth R, Bunchman TE, Chua AN, Goldstein SL et al (2007) The effect of vascular access location and size on circuit survival in pediatric continuous renal replacement therapy: a report from the PPCRRT registry. Int J Artif Organs 30:1116–1121. https://doi.org/10.1177/039139880703001212
Garzotto F, Zaccaria M, Vidal E, Ronco C et al (2019) Choice of catheter size for infants in continuous renal replacement therapy: bigger is not always better. Pediatr Crit Care Med 20:e170–e179. https://doi.org/10.1097/PCC.0000000000001825
Coulthard MG, Crosier J, Griffiths C, Lambert HJ et al (2014) Haemodialysing babies weighing <8 kg with the Newcastle infant dialysis and ultrafiltration system (Nidus): comparison with peritoneal and conventional haemodialysis. Pediatr Nephrol 29:1873–1881. https://doi.org/10.1007/s00467-014-2923-3
Askenazi D, Ingram D, White S, Fathallah-Shaykh S et al (2016) Smaller circuits for smaller patients: improving renal support therapy with AquadexTM. Pediatr Nephrol 31:853–860. https://doi.org/10.1007/s00467-015-3259-3
Raina R, Bedoyan JK, Lichter-Konecki U, Warady BA et al (2020) Consensus guidelines for management of hyperammonaemia in paediatric patients receiving continuous kidney replacement therapy. Nat Rev Nephrol 16:471–482. https://doi.org/10.1038/s41581-020-0267-8
Arbeiter AK, Kranz B, Wingen A-M, Büscher R et al (2010) Continuous venovenous haemodialysis (CVVHD) and continuous peritoneal dialysis (CPD) in the acute management of 21 children with inborn errors of metabolism. Nephrol Dial Transplant 25:1257–1265. https://doi.org/10.1093/ndt/gfp595
Celik M, Akdeniz O, Ozgun N, Ozbek MN et al (2019) Short-term results of continuous venovenous haemodiafiltration versus peritoneal dialysis in 40 neonates with inborn errors of metabolism. Eur J Pediatr 178:829–836. https://doi.org/10.1007/s00431-019-03361-4
Snauwaert E, Van Biesen W, Raes A, Vande Walle J et al (2017) Accumulation of uraemic toxins is reflected only partially by estimated GFR in paediatric patients with chronic kidney disease. Pediatr Nephrol 33:315–323. https://doi.org/10.1007/s00467-017-3802-5
Nishimi S, Sugawara H, Onodera C, Oyama K et al (2019) Complications during continuous renal replacement therapy in critically ill neonates. Blood Purif 47(Suppl 2):74–80. https://doi.org/10.1159/000496654
Jiritano F, Serraino GF, ten Cate H, Lorusso R et al (2020) Platelets and extra-corporeal membrane oxygenation in adult patients: a systematic review and meta-analysis. Intensive Care Med 46:1154–1169. https://doi.org/10.1007/s00134-020-06031-4
Thachil J, Warkentin TE (2017) How do we approach thrombocytopenia in critically ill patients? Br J Haematol 177:27–38. https://doi.org/10.1111/bjh.14482
Mulder J, Tan HK, Bellomo R, Silvester W (2003) Platelet loss across the hemofilter during continuous hemofiltration. Int J Artif Organs 26:906–912. https://doi.org/10.1177/039139880302601006
Griffin BR, Jovanovich A, You Z, Lorusso R et al (2019) Effects of baseline thrombocytopenia and platelet decrease following renal replacement therapy initiation in patients with severe acute kidney injury. Crit Care Med 47:e325–e331. https://doi.org/10.1097/CCM.0000000000003598
Griffin BR, Ten Eyck P, Faubel S, Bellomo R et al (2022) Platelet decreases following continuous renal replacement therapy initiation as a novel risk factor for renal nonrecovery. Blood Purif 51:559–566. https://doi.org/10.1159/000517232
Griffin BR, Wu C, O’Horo JC, Kashani K et al (2021) The association of platelet decrease following continuous renal replacement therapy initiation and increased rates of secondary infections. Crit Care Med 49:e130–e139. https://doi.org/10.1097/CCM.0000000000004763
Ranchin B, Plaisant F, Demède D, Bacchetta J et al (2021) Review: Neonatal dialysis is technically feasible but ethical and global issues need to be addressed. Acta Paediatr 110:781–788. https://doi.org/10.1111/apa.15539
Acknowledgements
The authors would like to thank the physicians involved in this clinical study aiming at improving our management practices with the use of CARPEDIEM®. The authors would also like to thank Véréna Landel (Direction de la Recherche en Santé, HCL) for help in manuscript preparation.
Funding
D. De Luca has received research assistance and speaker fees from MEDTRONIC Inc., outside of the present work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics
The study was approved by an ethics committee (Comité d’Ethique des Recherches non Interventionelles Université Côte d’Azur, session 23 September 2020, approval N°2020–68) and respected all local and European relevant regulations. This study was performed with the appropriate participants’ informed consent in compliance with the Helsinki Declaration.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Battista, J., De Luca, D., Eleni Dit Trolli, S. et al. CARPEDIEM® for continuous kidney replacement therapy in neonates and small infants: a French multicenter retrospective study. Pediatr Nephrol 38, 2827–2837 (2023). https://doi.org/10.1007/s00467-022-05871-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-022-05871-0