
Abstract
Prior to the COVID-19 pandemic, adolescents in most countries experienced a syndemic of malnutrition, obesity, deprivation, mental health problems, inequalities, and the effects of climate change. Today, other factors have added to this burden during the pandemic, and it is important to have an updated reflection. We aimed to assess the risk and protective factors for COVID-19-related adolescent mortality and morbidity in the European region. Three double models were fitted to analyze the relationship between different factors with the number of diagnosed cases and deaths. The 1a and 1b use a multiple Poisson regression. The 2a and 2b are optimized models that use the same variables as prior models but with backward selection with a p value < 0.05 as the limit. Finally, the 3a and 3b models (backward stepwise multivariable Poisson regression) include the variable “fully vaccinated.” All models used the at-risk population (15–19 years or total population) as a regression covariate (offset). Increased access to quality healthcare (IRR 0.68; CI 0.55–0.84), increased private sector involvement (IRR 0.86; CI 0.82–0.90), Gini coefficient (IRR 0.93; CI 0.88–0.99), and full vaccination (IRR 0.94; CI 0.90–0.99) represent protective factors of COVID-19 mortality in this population. Additionally, a positive association between pollution and mortality was found.
Conclusion: Being fully vaccinated and having access to quality medical care are protective factors against COVID-19 mortality in this age group. Interestingly, the more the pollution, the greater the risk of dying from COVID-19. We stress the great importance of coordination between the public and private sectors to address crises such as the current one.
What is Known: |
• Compared to other age groups, adolescents have been little studied, and most studies focused on mental health during the COVID-19 pandemic. |
What is New: |
• In this study, we show how in 19 European countries, different factors interact, such as socio-demographic, environmental, health system, and control measures with morbidity and mortality by COVID-19, in a very little studied age group as teenagers. |
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The official end of the COVID-19 pandemic is considered near; however, the coronavirus continues to be present, in part related to the unequal vaccine coverage and the appearance of new variants [1].
Adolescence is one of the least studied population groups during the pandemic; it is a period of major bodily, psychological, and social development with significant health repercussions, which leaves teens included in the Global Strategy for Women’s, Children’s, and Adolescents’ Health and the Countdown to 2030 [2,3,4]. Although young people do not belong to the population group most affected by the pandemic, the negative effects on this age group of the containment measures taken and their possible medium- and long-term connections should be monitored [5] because children and youth are usually considered vulnerable populations and sensitive to sudden changes [6, 7].
However, even in the European context, where health and social assistance is greater than what is available in other regions, there are deficiencies, vulnerabilities, and inequalities between the continent’s countries regarding loss of family income, disruption of health systems, and the implementation of containment and control measures of the pandemic [7, 8]. As a result of these measures, young people had access to health care restricted and lost spaces of protection and interaction, such as schools or parks, which led to the detriment of their physical, mental, and socioemotional well-being [9]. Existing data do not point to a rise in youth mortality related to the COVID-19 pandemic, although there are suspicions of substantial indirect effects of the pandemic on their mortality [10].
There is a lack of reliable evidence on the topic, and the need for data on this specific population group is urgent. Circumstances such as forced confinement and the closure of schools that significantly affect the lives of young people should be monitored and planned considering different factors [11].
Having updated and disseminated statistics and indicators has been one of the major problems for many countries since 2020 [12], data that are essential for planning and making decisions at all levels, mainly in the age group of children and young people.
The study of the determinants and consequences of COVID-19 [13] is essential to guide the actions and government responses for social support. This study measures the determinants and predictors of COVID-19 mortality and morbidity in the population aged 15–19 years old, and focuses on containment measures, health system indicators, vaccination coverage, and environmental pollution as possible determinants and predictors of COVID-19 morbidity and mortality in the population aged 15 to 19 in the European region.
Methods
This study uses data sources from 19 European countries to analyze the relationship between the main containment measures and characteristics of the countries with mortality and morbidity due to COVID-19 in the population aged 15 to 19 years.
The study design is a multiple-group exploratory study that uses aggregated data from countries in the European region.
Variables and data sources
The variables included in the analysis consider the COVID-19 morbidity and mortality determinants, as reported in the literature [14], and were selected based on their plausibility with the outcomes studied; whereas in the literature, there is very little available information for this age group, also because these variables have been little explored in previous studies on mortality and morbidity in adolescents, and because these variables and indicators are essential factors of the countries likely to be improved.
The data sources were chosen from databases that hold up-to-date data on adolescents as reported by the official agencies of each country.
The two outcomes studied, the cumulative incidence of diagnosed COVID-19 cases and deaths, were extracted from the Global Health 50/50-COVID-19 project [15].
As covariates, we used the scores of the linking public health and security authorities, private health sector involvement in health response planning, access to quality healthcare, and public health vulnerabilities extracted from the Global Health Security Index (GHSI) 2021 [16], and in addition, the doctors per 100 k, hospital beds per 100 k, population housing per unit land area (km2), and the Gini coefficient (Table 1).
Additionally, we used the covariate COVID-19 Containment and Health Index 2021 [17], which is based on thirteen policy response metrics (cancelation of public events, public gathering restrictions, public transport closures, general information campaigns, stay-at-home requirements, restrictions on internal movement, international controls, school recommendations, testing, contract tracing, face coverings, vaccination, and workplace closures) extracted from the Our World in Data organization [18]. We also extracted the percentage of persons (all ages) fully vaccinated (Table 1).
Finally, we also used the covariable concentration of contamination PM2.5, extracted by country (particles less than 2.5 μm in diameter; emitted by vehicles, industry, power generation, and domestic heating). Data from 2021 were obtained from the World Air Quality Report (Table 1) [19].
Statistical analysis
In total, three double models were fitted (models 1a, 1b; 2a, 2b; 3a, 3b); the first three use the number of diagnosed cases per 15- to 19-year-old population per country as the outcome, and the subsequent three use the number of deaths per 15- to 19-year-old population per country with the same analytical approach (multiple Poisson regression [20, 21].
Models 1a and 1b use the following predictor variables: linked public health/security, private sector involvement, access to quality healthcare, public health vulnerabilities, containment, and health index, doctors per 100 k 15–19-year-old population, hospital beds per 100 k 15–19-year-old population, population housing per unit land area (km2), and the Gini coefficient.
Models 2a and 2b are optimized models that use the same variables as the prior models (but now using the backward stepwise multivariable Poisson regression, having a p value < 0.05 as the cutoff); the logarithm of the risk population was used as an offset variable in the Poisson regression model with the log link function.
Finally, models 3a and 3b (also used a backward stepwise multivariable Poisson regression) included the variable “fully vaccinated.” In this model, the variable stringency index was not included (to avoid collinearity since the containment and health index contains vaccine and vaccine policy indicators).
These models produce incidence rate ratios (IRRs) for SARS-CoV-2 infections and mortality due to COVID-19. Poisson regression was used with the offset variable computed by the exposed risk population, allowing to achieve incidence rate ratios based on incidences observed in country-people. All models used the population at risk (15–19 years or total population) as a regression covariate (offset [21]).
Analyses were performed using Stata software (StataCorp. 2017. Stata Statistical Software: Release 15.1. College Station, TX, USA: StataCorp LLC).
Results
Nineteen countries of the European region that reported updated data for this age group were studied. A total of 1,388,164 adolescents were reported as confirmed cases by COVID-19 and included in this study. Table 2 shows some characteristics and indicators of the countries with variability in doctors per 100 k (Lithuania 75.4 points and Albania 14.3) and the same dynamic in public health vulnerabilities (Norway 93.6 and Albania 46.5).
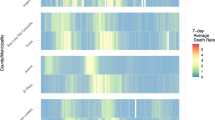
The mortality rate of 100,000 15–19-year-old population from COVID-19 is distributed variably; countries such as Malta and Montenegro show the highest mortality, but in countries such as Iceland and Slovenia, the mortality for this age group was very low (Fig. 1).

COVID-19 mortality in nineteen European countries as of March 2022, group (15 to 19 years old)
Regarding the diagnosed cases (Table 3), a greater link between public health and security (IRR 0.99; CI = 0.99–0.99), greater participation of the private sector (IRR 0.99; CI = 0.98–0.99), greater containment measures (IRR 0.93; CI = 0.93–0.94), fewer public health vulnerabilities (IRR 0.86; CI = 0.86–0.86), and full vaccination (IRR 0.82; CI = 0.82–0.82) were protective factors against becoming infected with SARS-CoV-2. The three models show that the higher the pollution, the higher the transmission of the virus and, therefore, more cases.
Regarding deaths (Table 4), the same variables of the previous model were considered. We highlight that for model 1, higher access to quality healthcare (IRR 0.68; CI 0.55–0.84), hospital beds per 100 k population (IRR 0.80; CI 0.72–0.88), greater participation of the private sector (IRR 0.97; CI 0.96–0.99), greater containment measures (IRR 0.86; CI 0.82–0.90), Gini (IRR 0.93; 0.88–0.99), and full vaccination (IRR 0.94; CI 0.90–0.99) were protective factors against mortality from COVID-19. It is important to mention that the variable “pollution” was shown to be a risk factor (IRR 1.13; CI 0.97–1.32), suggesting that the higher the pollution, the greater the risk of dying from COVID-19 after adjusting for the other covariables.
Discussion
Before the pandemic began, there was already evidence that adolescents suffered from a mixture of malnutrition, obesity, deprivation, mental health problems, inequalities, and climate change [23,24,25]; the scenario now seems worse because of the impact of the pandemic [26]; the results presented give some indication of the factors that contributed to that increased burden. There is little evidence of factors associated with adolescent mortality due to COVID-19. A study in the USA attributed deaths in children under 21 years of age to COVID-19, commonly related to obesity, asthma, and developmental problems [27].
This study addressed other causes that could be related to morbidity and mortality by COVID in a poorly studied age group (15 to 19 years). The Sustainable Development Goals (SDGs) focus on not leaving anyone behind and protecting children and young people [28, 29].
In this sense, the factors studied here are in agreement with other studies since the pandemic has shown that socioeconomic inequities, together with clinical aspects specific to individuals, play a determining role in mortality [30, 31]; this is an important dynamic to study and understand because it will allow us to mitigate the impact experienced by young people and provide key knowledge for future planning.
Our main results show that factors such as more hospital beds, Gini coefficient, number of physicians, access to quality healthcare, and linking between public health/security and public health vulnerabilities positively correlate with higher mortality and morbidity from COVID-19. These results might seem contradictory to what is expected, but it is not necessarily so; a study in the UK highlights that although at the beginning of the pandemic, young people showed good intentions to follow the rules and recommendations, in practice, this was not necessarily the truth; many young people are more likely to break the rules of social distancing [32]. In addition, the positive relationship between hospital beds/100 k and diagnosed cases of COVID-19 can be explained by the fact that more hospital beds imply greater resources, physical capacity, and possibilities to care for patients, leading to greater access and lower mortality, as our results show.
This study also showed that European countries present important differences in public health vulnerabilities. The multiple regression analysis of the diagnosed cases allowed us to identify some aggravating factors for the transmission and death by COVID-19 and some protective factors. Being fully vaccinated and having access to quality healthcare are two fundamental protective factors against mortality due to COVID-19 in this age group.
Environmental factors such as air pollution and its role in COVID-19 morbidity and mortality have been of study and concern [33]; in some studies, air quality alone is not a decisive protective factor in preventing the spread of the virus [34]. This must be immersed in a set of other factors. Therefore, we have included it in our model.
Of interest is that the higher the pollution, the higher the risk of dying by COVID-19; in this sense, reducing pollutants needs to be an important part of preventing severe cases of disease that lead to death. It is documented that pollution during the COVID-19 pandemic decreased in many parts of the world due to containment measures, limited mobility, and less use of cars, suggesting that there had not been this dichotomy, and the number of deaths could be even higher. This study found a positive association between mortality and environmental pollution, corroborated by other studies [35]. Urban growth, environmental controls, and how the built environment contributes to mortality and morbidity should be the subject of deep analysis at the local level of each country and subregion.
In this study, the stringency index variable was considered, which includes vaccines, vaccine policy, and school closures during the pandemic; the closure of schools covered primary, secondary, and university education, which means that our age group of study has been affected. Since the start of the pandemic, it was said that schools could be places of infections and that students could then transmit the virus to others at home, which generated a severe risk, especially for older adults; however, several recent studies report that this is not necessarily true, because youth-to-adult transmission is less than adult-to-youth transmission [36,37,38,39,40,41,42,43,44,45,46,47].
Some studies have reported that school restrictions do more harm than good and that they were executed in an empirical context [48,49,50,51].
It is important to say that, on the one hand, the restriction measures protect against morbidity and mortality from COVID-19. Nevertheless, on the other hand, they harm other areas of young people’s lives, as emotional abuse was likely exacerbated during this time of economic uncertainty and stress, adding to the increase in domestic violence [52]. Regarding the indicator used as a stringency index, which is a score on a set of restraint measures employed by countries, it presents differences between countries; Montenegro, Slovenia, and Luxembourg are among the countries with the highest scores, and France, Lithuania, and Hungary are among the lowest; however, it is necessary to mention that there is no linear relationship between this indicator alone and lower morbidity or mortality, which depends on a set of factors that interact dynamically.
We highlight the importance of coordination between the public and private sectors to address crisis such as the current one. This suggests that in many countries where health systems are shared, it is always important to work continuously with private organizations to increase the protection of the population.
As for another important aspect when dealing with young people in the European continent, where many countries possess a good level of development, better health systems, and better socioeconomic conditions than in other regions of the world, many of them trust themselves and enter into a so-called relaxing behavior, which meant an increase in cases, reflected in higher hospital admissions, a greater use of beds, and the need for more doctors and health workers to care for them. This finding is important for identifying interventions focused on modifying behavior and health education better targeted for future and present health crises.
It is important to report some limitations; the main one was the lack of data from selected large European countries for this specific age group, a problem in all countries worldwide. Additionally, we cannot fully ensure a causal association between diagnosed cases and death due to COVID-19 and the predictors considered. However, the criteria used in our models allow us to affirm that the study is a responsible approximation of reality. Another limitation is that confirmed infection in teens is still not as common as in older age groups, although there could not be enough variability to detect these associations. Another possible limitation not only of this study but also of COVID-19 studies, in general, that use “cases” as a variable is that the number of diagnosed cases can be underestimated as it depends on the testing policies carried out and the resources available. However, diagnosed cases reported in official sources are vital to understanding the level of virus transmission.
This study also has strengths, such as the use of the containment and health index in the multiple regression models; despite being considered a guide to evaluating measures on the spread of COVID-19 cases per country, it considers the thirteen most important actions that governments have implemented, from mobility to internal and external restrictions, among others, already detailed in the “Methods” section. Another strength is the inclusion of environmental variables, vaccinations, health system characteristics, and socioeconomic indicators to make the analysis robust.
An important lesson from this study is the importance of free and up-to-date information on the pandemic; reliable data are essential to healthcare decisions. Many models at the beginning of the pandemic failed due to an inability to update information quickly; the digital progress of information systems is an area that must be strengthened. The pandemic may cause investment in this arena to increase considerably [53].
Within the objectives of sustainable health and well-being development, we point to several protective factors for this population group in this study. Many countries were slowly moving toward development goals, and the pandemic affected that progress even more; in the case of European countries, there are still actions to be done and programs to be strengthened, and we hope this study will contribute to the laying of essential factors to be included in the current and future strategies of protection and attention.
The well-being of adolescents is called a priority. This age period represents a unique opportunity to acquire and develop human and social skills for later life [54]. The syndemic [16] has worsened social inequities, mainly in the least protected people. In many countries and contexts, the effect has been devastating, affecting all spheres of life of young people and adults, alternating between other vital aspects such as physical activity and healthy food consumption [55, 23].
Investing in interventions to favor the development and protection of European adolescents is a key part of meeting sustainable development goals and producing human capital for the future; it is estimated that for every dollar invested in adolescent health interventions, the health, social, and economic returns will be ten times greater [56].
Finally, and in line with the messages of different organizations, many mistakes were made during the pandemic despite prior preparation and knowledge. We believe that with this study, we have contributed by studying a diverse array of variables that are part of the well-being of young people. The indicators and the environments of the countries where people live are closely linked to health outcomes [57]; this study sought to study aspects related to COVID-19 cases and deaths. We believe that the risk factors identified in this study will undoubtedly serve to focus strategies and interventions addressing the pandemic’s almost irreversible current and future damage to the young population [55].
Availability of data and materials
Data are available upon reasonable request.
References
Yusha Araf, Fariya Akter, Yan-dong Tang, Rabeya Fatemi, Md. Sorwer Alam Parvez, Chunfu Zheng MGH (2021) Omicron variant of SARS-CoV-2: genomics, transmissibility, and responses to current COVID-19 vaccines. J Med Virol
Sawyer SM, Azzopardi PS, Wickremarathne D, Patton GC (2018) The age of adolescence. Lancet Child Adolesc Heal 2(3):223–228
Temmerman M, Khosla R, Bhutta ZA, Bustreo F (2015) Towards a new Global Strategy for Women’s. Children’s and Adolescents’ Health BMJ 351:h4414
Boerma T, Requejo J, Victora CG, Amouzou A, George A, Agyepong I et al (2018) Countdown to 2030: tracking progress towards universal coverage for reproductive, maternal, newborn, and child health. Lancet 391(10129):1538–1548
Bhopal SS, Bagaria J, Olabi B, Bhopal R (2021) Children and young people remain at low risk of COVID-19 mortality. Lancet Child Adolesc Heal 5(5):e12–e13
Guessoum SB, Lachal J, Radjack R, Carretier E, Minassian S, Benoit L et al (2020) Adolescent psychiatric disorders during the COVID-19 pandemic and lockdown. Psychiatry Res 291(June):113264
Adu PA, Stallwood L, Adebola SO, Abah T, Okpani AI (2022) The direct and indirect impact of COVID-19 pandemic on maternal and child health services in Africa : a scoping review. Glob Heal Res Policy
WHO (2021) Considerations in adjusting public health and social measures in the context of COVID-19. World Heal Organ Interim Guid [Internet] 1–13. Available from: https://www.who.int/publications/i/item/considerations-in-adjusting-public-health-and-social-measures-in-the-context-of-covid-19-interim-guidance
Teo SSS (2020) Child protection in the time of COVID-19. J Paediatr Child Health 22–4
Group UNI (2022) Levels & trends in child mortality: report 2022: estimates developed by the United Nations Inter-agency Group for Child Mortality Estimation
Saeed HM, Saad Elghareeb A, El-Hodhod MAA, Samy G (2023) Assessment of COVID-19 preparedness response plan on higher education students simulation of WHO intra-action review in Egypt. Sci Rep 13(1):1–9. Available from: https://doi.org/10.1038/s41598-023-27713-1
Msemburi W, Karlinsky A, Knutson V, Aleshin-Guendel S, Chatterji S, Wakefield J (2023) The WHO estimates of excess mortality associated with the COVID-19 pandemic. Nature 613(7942):130–137
Béland LP, Brodeur A, Wright T (2023) The short-term economic consequences of COVID-19: exposure to disease, remote work and government response. Plos One 18:e0270341. Available from: https://doi.org/10.1371/journal.pone.0270341
Rzymski P, Poniedziałek B, Rosińska J, Ciechanowski P, Peregrym M, Pokorska-Śpiewak M et al (2022) Air pollution might affect the clinical course of COVID-19 in pediatric patients. Ecotoxicol Environ Saf 239
Range A (2022) Sex, gender and COVID-19 project sex-disaggregated COVID-19 variable data - deaths by age and sex per 100, 000
Bell JA, Nuzzo JB (2021) Global Health Security (GHS) index: advancing collective action and accountability amid global crisis 238. Available from: https://www.ghsindex.org/wp-content/uploads/2021/12/2021_GHSindexFullReport_Final.pdf
Hale T, Angrist N, Goldszmidt R, Kira B, Petherick A, Phillips T et al (2021) A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat Hum Behav [Internet] 5(4):529–38. Available from: https://doi.org/10.1038/s41562-021-01079-8
Mathieu E, Ritchie H, Ortiz-Ospina E, Roser M, Hasell J, Appel C et al (2021) A global database of COVID-19 vaccinations. Nat Hum Behav [Internet] 5(7):947–53. Available from: https://doi.org/10.1038/s41562-021-01122-8
IQAir. World air quality report 2021 (2022) Pap Knowl Towar a Media Hist Doc [Internet] 43. Available from: https://www.iqair.com/world-air-quality-report
Barros AJD, Hirakata VN (2003) Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol 3:1–13
Knudsen DC (1992) Generalizing Poisson regression: including a priori information using the method of offsets. Prof Geogr 44(2):202–208
Action BC (2019) Building collective action and accountability [Internet]. Available from: https://www.ghsindex.org/wp-content/uploads/2019/10/2019-Global-Health-Security-Index.pdf
Mcgowan VJ, Bambra C (2022) Review COVID-19 mortality and deprivation : pandemic, syndemic, and endemic health inequalities. Lancet Public Heal 7(11):e966–e975
Swinburn BA, Kraak VI, Allender S, Atkins VJ, Baker PI, Bogard JR et al (2019) The global syndemic of obesity, undernutrition, and climate change: the Lancet Commission report. Lancet 393(10173):791–846
Vitorino LM, Sousa LM, Trzesniak C, de Sousa Valentim OM, Yoshinari Júnior GH, José HM, Lucchetti G (2022) Mental health, quality of life and optimism during the covid-19 pandemic: a comparison between Brazil and Portugal. Qual Life Res 1-3
Department of Health, Zhang F, Karamagi H, Nsenga N, Nanyunja M, Karinja M et al (2021) Predictors of COVID-19 epidemics in countries of the World Health Organization African Region. Nat Med 52
Mccormick DW, Richardson C, Young PR, Viens LJ (2021) Deaths in children and adolescents associated with COVID-19 and MIS-C in the United States 148(5)
Richardson D, Brukauf Z, Toczydlowska E, Chzhen Y (2017) Comparing child-focused Sustainable Development Goals ( SDGs ) in high-income countries: indicator development and overview 1–74
Raikes A, Yoshikawa H, Britto PR, Iruka I (2017) Children, youth and developmental science in the 2015–2030 global Sustainable Development Goals. Soc Policy Rep 30(3):1–23
Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE et al (2020) Factors associated with COVID-19-related death using OpenSAFELY. Nature [Internet]. 584(7821):430–6. Available from: https://doi.org/10.1038/s41586-020-2521-4
Martins-Filho PR, Quintans-Júnior LJ, de Souza Araújo AA, Sposato KB, Souza Tavares CS, Gurgel RQ et al (2021) Socio-economic inequalities and COVID-19 incidence and mortality in Brazilian children: a nationwide register-based study. Public Health [Internet] 190:4–6. Available from: https://doi.org/10.1016/j.puhe.2020.11.005
Levita L, Miller JG, Hartman TK, Murphy J, Shevlin M, McBride O, McKay R, Mason L, Martinez AP, Stocks TV BK (2021) Initial research findings on the impact of COVID-19 on the well-being of young people aged 13 to 24 in the UK. Vol. 2. United Kingdom
Semczuk-Kaczmarek K, Rys-Czaporowska A, Sierdzinski J, Kaczmarek LD, Szymanski FM, Platek AE (2022) Association between air pollution and COVID-19 mortality and morbidity. Intern Emerg Med [Internet] 17(2):467–73. Available from: https://doi.org/10.1007/s11739-021-02834-5
Xu R, Rahmandad H, Gupta M, DiGennaro C, Ghaffarzadegan N, Amini H et al (2021) Weather, air pollution, and SARS-CoV-2 transmission: a global analysis. Lancet Planet Heal [Internet] 5(10):e671–80. Available from: https://doi.org/10.1016/S2542-5196(21)00202-3
Yao Y, Pan J, Wang W, Liu Z, Kan H, Qiu Y et al (2020) Association of particulate matter pollution and case fatality rate of COVID-19 in 49 Chinese cities. Sci Total Environ [Internet] 741:140396. Available from: https://doi.org/10.1016/j.scitotenv.2020.140396
El JM, Edjoc R, Waddell L, Huston P, Atchessi N, Striha M et al (2021) Impact of school closures and re-openings on COVID-19 transmission. Can Commun Dis Rep 47(12):515–523
Viner RM, Russell SJ, Croker H, Packer J, Ward J, Stansfield C et al (2020) School closure and management practices during coronavirus outbreaks including COVID-19: a rapid systematic review. Lancet child Adolesc Heal 4(5):397–404
Xu W, Li X, Dozier M, He Y, Kirolos A, Mathews C (2020) What is the evidence for transmission of COVID-19 by children in schools ? A living systematic review. J Glob Health 10(2)
Walsh S, Chowdhury A, Braithwaite V, Russell S, Birch JM, Ward JL et al (2021) Reopenings affect community transmission of COVID-19 ? A systematic review of observational studies
Viner RM, Mytton OT, Bonell C, Ward J, Hudson L, Waddington C et al (2021) Susceptibility to SARS-CoV-2 infection among children and adolescents compared with adults a systematic review and meta-analysis 175(2):143–56
Walsh KA, Spillane S, Comber L, Cardwell K, Harrington P, Connell J et al (2020) The duration of infectiousness of individuals infected with SARS-CoV-2. J Infect 81(6):847–856
Thompson HA, Mousa A, Dighe A, Fu H, Arnedo-pena A, Barrett P et al (2021) Severe acute respiratory syndrome coronavirus 2 ( SARS- CoV-2 ) setting-specific transmission rates : a systematic review and meta-analysis 2(3)
Goldstein E, Lipsitch M, Cevik M (2021) On the effect of age on the transmission of SARS-CoV-2 in households, schools, and the community 223
Irfan O, Tang K, Wang Z, Bhutta ZA (2021) Risk of infection and transmission of SARS- CoV-2 among children and adolescents in households, communities and educational settings : a systematic review and meta-analysis 11
Shah K, Saxena D, Mavalankar D (2020) Secondary attack rate of COVID-19 in household contacts : a systematic review 841–50
Madewell ZJ, Yang Y, Jr IML, Halloran ME, Dean NE (2020) Household transmission of SARS-CoV-2 a systematic review and meta-analysis 3(12):1–17
Bautista L, Oróstegui-arenas M, Idrovo A (2021) Es prioritario vacunar a niños de 3–11 años contra COVID-19 en Colombia ? Salud UIS 53
Singh S, Roy D, Sinha K, Parveen S, Sharma G, Joshi G (2020) Impact of COVID-19 and lockdown on mental health of children and adolescents: a narrative review with recommendations. Psychiatry Res 293(May):113429
Gil JDC, Vargues M, Azeredo-lopes S, Soares P, Moura SD, Arcêncio RA (2022) Physical distancing and mental well-being in youth population of Portugal and Brazil during the COVID-19 pandemic. Port J Public Heal 1–10
Gil AJDC, Vargues-aguiar PM (2022) Analysis of some factors and COVID-19 mortality in the population of 0 to 24 years in 29 countries : open schools could be a protection. Microb Infect Chemother 6:1–7
Gil J, Cortés DM (2022) Government effectiveness and child development in low- middle income countries : COVID-19 pre-pandemic time. Salud UIS
Lee J (2020) Reflections features mental health effects of school closures during COVID-19. Lancet child Adolesc Heal 4(6):421
Lancet T, Health D (2022) Editorial The importance of linkage : lessons from one pandemic to another. Lancet Digit Heal 4(10):e698
The global goals for sustainable development (2020) Make adolescent well-being a priority: an urgent call to action
Neville RD, Lakes KD, Hopkins WG, Tarantino G, Draper CE, Beck R et al (2022) Global changes in child and adolescent physical activity during the COVID-19 pandemic a systematic review and meta-analysis 176(9):886–94
Sheehan P, Sweeny K, Rasmussen B, Wils A, Friedman HS, Mahon J et al (2017) Health policy building the foundations for sustainable development : a case for global investment in the capabilities of adolescents. Lancet 6736(17)
Frumkin H (2021) COVID-19, the built environment, and health. Environ Health Perspect 129(7):1–14
Funding
Open access funding provided by FCT|FCCN (b-on). The present publication was funded by Fundação para a Ciência e Tecnologia, IP national support through CHRC (UIDP/04923/2020). FCT e a Unidade de I&D CHRC—Comprehensive Health Research Centre (UI/BD/150908/2021). GHTM (UID/Multi/04413/2019) is funded by the Portuguese Science Foundation (FCT).
Author information
Authors and Affiliations
Contributions
JDCG proposed the study, prepared the analysis datasets, conducted the analysis, and wrote the article’s first draft. PMVA guided the framework, statistical approach, and the final manuscript’s elaboration. PF guided the framework, statistical approach, and the final manuscript’s development.
Corresponding author
Ethics declarations
Ethical approval
The data used in this study are public sources of information, and ethical approval was already obtained by the institutions responsible for its implementation in each country. Databases are anonymous, ensuring data confidentiality.
Competing interests
The authors declare no competing interests.
Additional information
Communicated by Peter de Winter
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cortés, J., Aguiar, P.M.V. & Ferrinho, P. COVID-19-related adolescent mortality and morbidity in nineteen European countries. Eur J Pediatr 182, 3997–4005 (2023). https://doi.org/10.1007/s00431-023-05068-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-023-05068-z