
Abstract
Background and objective
Cognitive and physical functions correlate and delineate aging and disease trajectories. Whereas cognitive reserve (CR) is well-established, physical reserve (PR) is poorly understood. We, therefore, developed and evaluated a novel and more comprehensive construct, individual reserve (IR), comprised of residual-derived CR and PR in older adults with and without multiple sclerosis (MS). We hypothesized that: (a) CR and PR would be positively correlated; (b) low CR, PR, and IR would be associated with worse study outcomes; (c) associations of brain atrophy with study outcomes would be stronger in lower compared to higher IR due to compensatory mechanisms conferred by the latter.
Methods
Older adults with MS (n = 66, mean age = 64.48 ± 3.84 years) and controls (n = 66, mean age = 68.20 ± 6.09 years), underwent brain MRI, cognitive assessment, and motoric testing. We regressed the repeatable battery for the assessment of neuropsychological status and short physical performance battery on brain pathology and socio-demographic confounders to derive independent residual CR and PR measures, respectively. We combined CR and PR to define a 4-level IR variable. The oral symbol digit modalities test (SDMT) and timed-25-foot-walk-test (T25FW) served as outcome measures.
Results
CR and PR were positively correlated. Low CR, PR and IR were associated with worse SDMT and T25FW performances. Reduced left thalamic volume, a marker of brain atrophy, was associated with poor SDMT and T25FW performances only in individuals with low IR. The presence of MS moderated associations between IR and T25FW performance.
Conclusion
IR is a novel construct comprised of cognitive and physical dimensions representing collective within-person reserve capacities.
Similar content being viewed by others

Introduction
Mobility impairments are the clinical hallmark of multiple sclerosis (MS) [1, 2] but cognitive impairments are also common [3, 4]. Epidemiological evidence suggests a shift in the peak prevalence of MS into older age groups, and this will likely coincide with co-occurring aging and MS-related declines in mobility and cognition [5]. There is unequivocal evidence that mobility and cognitive functions are interrelated in aging [6,7,8] and MS [9, 10]. Hence, identifying modifiable protective factors relevant to cognitive and physical function in both populations is paramount.
Cognitive reserve (CR) is a buffer conferring differences in how individuals adapt to and execute tasks in the context of aging, disease, or injury-related effects on brain structure and function [11]. The literature devoted to this hypothetical construct is extensive [12, 13] and recent meta-analytic studies demonstrate robust protective CR effects against cognitive decline in older adults [14] and persons with multiple sclerosis (MS) [15]. Literature concerning the role of CR in physical outcomes is scarce, but recent studies reveal that higher CR is associated with more efficient brain activation, assessed during walking [16], and lower risk of incident mobility impairment among older adults [17].
By comparison, research concerning physical reserve (PR) is conspicuously scant except for limited literature on a related term, physical resilience [18]. PR may be construed as the ability to maintain and optimize motoric function in the face of physical decline attributed to age, disease, or injury. The lack of research concerning PR is notable given the robust associations between cognitive and physical function in older adults [19,20,21] and persons with MS [22, 23]. Furthermore, slower gait speed predicts multiple adverse health outcomes [24] including dementia [25], and exercise interventions have global effects on physical function, quality of life, mood and cognition across clinical populations [26]. Hence, defining PR and delineating its effects on clinical outcomes may improve predictive utility and explain variability in responses to interventions.
The residual approach to defining CR [13, 27] offers conceptual advantages as well as considerable empirical support demonstrating stronger protective effects against cognitive decline and dementia compared to traditional socio-demographic measures often used as proxies of this hypothetical construct [14]. Briefly, using regression models, the residual approach removes variance on cognitive tests performance explained by socio-demographic and brain pathology measures and utilizes the residuals of the remaining unexplained variance to quantify CR [13, 27]. Individual differences in residuals are indicative of varying CR levels wherein smaller values represent less CR. The residual approach can be applied to PR by regressing performance of a physical function test on extraneous variables and brain pathology measures.
No study, to date, has attempted to assess both CR and PR and examine the resulting independent and combined effects on clinical outcomes. Further, due to co-occurring and often correlated declines in cognitive and motor functions observed in aging and neurological disease, a broader construct may emerge and better represent within-person reserve capacities.
The current study introduced a paradigm shift proposing a reserve concept, individual reserve (IR), comprised of both CR and PR in older adults with MS and healthy controls. Using the residual approach, we derived CR and PR measures by regressing the total scores of the repeatable battery for the assessment of neuropsychological status (RBANS) [28] and short physical performance battery (SPPB) [29], respectively, on brain pathology and socio-demographic confounders. We then combined CR and PR to derive a 4-level IR variable to determine its associations with the oral symbol digit modalities test (SDMT) [30, 31] and timed-25-foot-walk test (T25FW) [32, 33], which served as study outcomes. In addition, recent research has shown that CR moderated associations between brain pathology and executive functions [34] and between in brain network connectivity and cognition [35]. Therefore, extending this line of work, the current study was designed to examine whether IR moderated associations between brain atrophy and study outcomes. We hypothesized that: (a) CR and PR would be positively correlated; (b) low CR, PR, and IR would be associated with worse study outcomes; (c) associations of brain atrophy with performances on the SDMT and T25FW would be stronger in lower compared to higher IR due to compensatory mechanisms conferred by the latter [36]. Finally, because MS impacts and likely accelerates the negative effect of aging on both physical and cognitive function, we further examined whether group status (i.e., MS vs. control) modified associations of reserve measures with study outcomes.
Materials and methods
Participants
Participants enrolled in an ongoing study titled “Brain Predictors of Mobility and Falls in Older Adults with Multiple Sclerosis” who were tested between September 2019 and July 2022 and had complete cognitive, mobility, psycho-social and brain imaging data were included. Of 138 participants with available data, 6 received a diagnosis of dementia and were thus excluded (study n = 132). MS participants are recruited from regional treatment centers and patient registry lists. Using the revised McDonald criteria [37], MS diagnoses were physician-confirmed by medical record review. MS participants had to be stable on a disease-modifying therapy (DMT) for at least 6 months prior to study enrollment. Control participants, recruited from population lists, were first mailed a letter followed by a phone call. Both cohorts were screened using a structured telephone interview to obtain verbal consent, assess medical and psychological history, and screen for dementia, mobility, and functional abilities to determine study eligibility. Participants were then invited for two in-person visits. The first consisted of a battery of neuropsychological tests, mobility protocols, and questionnaires. The second included an MRI of the brain and additional questionnaires. The average time between the two visits was 13.6 ± 16.9 days excluding two participants whose inter visit intervals were longer (218 and 219 days) due to temporary COVID-19-related suspension of in-person testing at Einstein. The two participants were retained because these longer time intervals are well within one year and inspection of their data did not suggest any notable deviation. Cognitive status was determined via established clinical case conference procedures [38]. Exclusion criteria included diagnosis of any major neurological, psychiatric, or medical disease (excluding MS), inability to ambulate independently, contraindication to MRI, impairment of vision or hearing that would negatively impact testing. The study was approved by the IRB of Albert Einstein College of Medicine (Protocol # 2019-10049). Written informed consent was obtained from all participants in the first in-person study visit. The work described in this manuscript has been executed in adherence with The Code of Ethics of the World Medical Association (Declaration of Helsinki).
Measures
Derivation of CR, PR, and IR
The residual approach defines reserve as the portion of variance on tests not explained by brain pathology and socio-demographic confounders. This approach provides a decomposed measure based on associations between test performance and confounders wherein residuals values vary across individuals and quantify reserve; smaller residuals signify less reserve. Both theoretical and data-driven considerations guided our approach for selecting the covariates and outcome measures in the regression models used to derive CR and PR. For the reserve outcome measures, we selected commonly used and validated tests of overall cognitive and physical function. With respect to the covariates, we initially identified measures of brain pathology and socio-demographic measures implicated in cognitive and physical function in aging and MS, and then retained variables that had significant associations with the outcome measures (see statistical analysis).
Cognitive reserve (CR)
Repeatable battery for the assessment of neuropsychological status (RBANS)
CR was assessed with the RBANS total score. The RBANS has been extensively researched and normed in aging [28] and MS [39, 40]. The RBANS assesses five cognitive domains (Immediate Memory, Visuospatial/constructional, Language, Attention, and Delayed Memory) with a total scale score ranging from 40 to 160. Its utility as a single measure of cognitive function has been well validated [41].
Physical reserve (PR)
Short physical performance battery (SPPB)
PR was assessed with the SPPB total score. The SPPB includes tests of balance, gait speed, and chair rise, with each portion scored on a scale of 0–4 with a possible total score ranging from 0 to 12 where higher scores are indicative of better performance. The SPPB has been extensively validated as a measure of physical function in numerous studies [29] and in older adults with MS [42].
Covariates
Brain atrophy
We selected measures sensitive to age and disease-related effects on structural integrity of white and gray matter. White matter lesions, a key clinical marker in MS [43], are common in aging [44]. The hippocampus and thalamus [45], notably left thalamic nuclei [46], are considered regions sensitive to cognitive status in aging and dementia in which atrophy could serve as a marker for a more generalized brain pathology. Thalamic atrophy is associated with multiple clinical outcomes including cognitive impairment in MS [47]. Lower right hippocampal volume is implicated in poor physical function in older adults [48]. We included total intracranial brain volume as a covariate.
Socio-demographic
Age, sex, race (Caucasian vs. Other), education, and a global health status (GHS) were considered. The GHS, a comorbidity measure, computes a total score based on the presence/absence of the following clinical conditions: diabetes, chronic heart failure, arthritis, hypertension, depression, stroke, Parkinson’s disease, chronic obstructive lung disease, angina, and myocardial infarction score (range 0–10) [38].
Individual reserve (IR)
Median splits of the PR and CR measures were used to create four quadrants demarcating low, two intermediate, and high levels of IR. The low IR group, comprised of individuals whose CR and PR were both low, was presumed to be most vulnerable to the adverse effects of aging and disease. Therefore, a priori, this group served as a reference condition for other IR levels. The low CR/high PR and high CR/low PR groups represented two intermediate levels of IR. The high IR group was comprised of individuals whose cognitive and physical reserve resources were both high.
Study outcomes
Symbol digit modalities test (SDMT)
The SDMT, oral version, is a measure of speed of processing and working memory requiring participants to pair symbols and digits based on a key within a 90-s time interval, lower scores are indicative of worse performance. The SDMT is used as a primary cognitive outcome measure in clinical trials for dementia [30] and MS [31]. The total number of correct responses served as the cognitive outcome measure.
Timed-25-foot-walk-test (T25FW)
The T25FW, a measure of gait speed, serves as a primary outcome in clinical trials and appears to be more sensitive to change than traditional measures of disability such as the Expanded Disability Status Scale [32, 33]. We used the average time for two trials administered in one study visit, and time was converted to gait speed (ft/sec) as the physical outcome measure.
Magnetic resonance imaging (MRI) of the brain
Structural image acquisition
MRI was performed in a 3 T Philips scanner equipped with a 32-channel head coil (Elition 3.0 T X, Philips Medical Systems, Best, The Netherlands) at the Gruss Magnetic Resonance Research Center of Albert Einstein College of Medicine. Analyses were extracted from a T1-weighted image (MPRAGE—TE/TR/TI = 4.6/9.8/900 ms, voxel size 1 mm isotropic, SENSE acceleration factor 2 × 1.3). 3D fluid-attenuated inversion recovery (FLAIR) images were acquired for identification of hyperintense T2 lesions using an inversion-prepared, single-shot T2 turbo spin-echo sequence (TE/TR/TI = 365/4800/1650 ms, voxel size 1 mm isotropic); both FLAIR and T1 images were used to identify and quantify white matter lesions.
White matter (WM) lesion load
Total WM lesion volume was calculated using the lesion segmentation toolbox (LST) [49], which uses both T1 and FLAIR images for identification of WM hypo/hyperintensities. While MS lesions were not expected in control participants, age-related hyperintensities of other origin (e.g., small vessel disease) were expected and thus quantified for both groups. Total lesion volume was included as a covariate in the linear regression models used to derive CR and PR.
Subcortical gray matter volume and intracranial volume
We used the FreeSurfer software package (http://surfer.nmr.mgh.harvard.edu/) to perform automatic segmentation (“aseg”) and extract subcortical volume measures from all study participants [50]. Intracranial volume was extracted from the same aseg file. Details of this process were described previously [51]. Briefly, preprocessing included brain extraction, identification of gray and white matter boundaries, and automatic volume segmentation of subcortical regions [52] based on a computed average space and surface-based smoothing of FWHM = 5 mm. FreeSurfer’s automatic segmentation identifies fourteen subcortical gray matter regions, seven in each hemisphere [53]. Based on our hypothesis and physiologically driven approach, the right hippocampus and left thalamus volumes were utilized in this study.
Statistical analysis
Descriptive statistics were used to summarize all study measures (mean ± SD for continuous measures, count and percent for categorical variables) and tabulated per group (MS vs. control) and per IR status. Two separate linear regressions were fitted to extract residuals from the RBANS and SPPB to quantify CR and PR, respectively. We employed a stepwise backward selection strategy [54] to optimize the variance accounted for in the linear regression models used to derive residual CR and PR measures. We started by considering covariates that were deemed relevant in a full model and then removed statistically insignificant variables (p > 0.05), one by one, until the final model included only variables that were statistically significant. Intracranial volume was included irrespective of statistical significance to adjust for gray matter volume measures that served as predictors in both regression models. The covariates initially considered in the full model were age, sex, education, race, WM lesion load, left thalamus volume, right hippocampus volume, intracranial volume, and GHS. For the final CR model, the right hippocampus, GHS, sex, and age were dropped during the backward selection process. For the final PR model, race, left thalamus, sex and age were dropped during the backward selection process. The final selection of covariates was based on these multi-variate models and not individual correlations with the SPPB and RBANS. Separate linear regressions for the SDMT and T25FW were fitted with CR, PR, or 4-level IR as a predictor without and with adjusting for confounders that included group (MS vs. control), age, sex, education, and GHS. In another set of linear regressions, 4-level IR served as a predictor of SDMT and T25FW performances. The moderating effects of MS group status on the associations of CR, PR and IR with the SDMT and T25FW were evaluated by adding an interaction term of group and each corresponding reserve predictor. Finally, we evaluated the hypothesis that IR moderated associations between brain atrophy and study outcomes. Specifically, we examined whether, compared to low IR, intermediate to high IR conferred protection against the effect of brain atrophy on SDMT and T25FW performances. Left thalamus, 2-level IR status (intermediate to high vs low) and their interaction were included in separate models predicting SDMT and T25FW as outcome measures. All tests of statistical significance were two-sided, and a p-value < 0.05 was considered statistically significant. Data were analyzed using SAS (version 9.4; SAS Institute Inc., Cary, NC, USA) statistical software.
Results
Participants
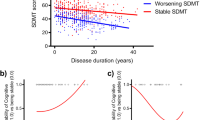
Participant characteristics were summarized per group and also stratified by IR status (Table 1). There were more female than male participants in the MS (59.09%) and control (63.64%) groups. Mean age was lower in MS (64.48 ± 3.84 years) compared to controls (68.2 ± 6.09 years). Mean RBANS total score in MS (90.85 ± 13.8) and controls (91.79 ± 11.48) was comparable and indicative of cognitive status within the normal range. Mean SPPB total score in MS (9.35 ± 2.31) and controls (10.64 ± 1.41) was indicative of relatively independent ambulatory levels. On average, both samples had college education (MS = 15.18 ± 2.19 years; control = 16.45 ± 2.4 years). Among participants with MS, 40 had relapsing remitting, 16 secondary progressive, 4 primary progressive and 6 undetermined subtypes. Mean MS disease duration was 21.74 ± 10.88 years.
Residual-derived CR and PR
The CR linear regression with WM lesion load, left thalamic volume, total intracranial volume, education, and race explained 23.7% of the variance in RBANS total score (R = 0.487, R square = 0.237, p < 0.001). The PR linear regression with WM lesion load, right hippocampal volume, total intracranial volume, education, and GHS explained 19% of the variance in SPPB total score (R = 0.435, R square = 0.19, p < 0.001). Summaries of the two linear regressions are provided in Table 2. The correlation between CR and PR was positive and significant (R = 0.313, p = 0.0002). Linear regressions utilizing the same covariates irrespective of the statistical significance of their associations with RBANS and SPPB scores yielded comparable CR and PR outcomes that were similarly correlated suggesting that excluding non-significant covariates did not bias the results (Supplemental Table 1, Supplemental Table 2 provides a summary of bi-variate correlations of covariates with RBANS and SPPB total scores).
Associations of CR with study outcomes
CR was positively associated with SDMT performance in unadjusted (estimate = 0.2621, 95% CI = 0.2027–0.3214, p < 0.0001) and adjusted (estimate = 0.2399, 95% CI = 0.1811–0.2988, p < 0.0001) models. CR was further positively associated with F25FW performance in unadjusted (estimate = 0.0125, 95% CI = 0.0049–0.0201, p = 0.0015) and adjusted (estimate = 0.0129, 95% CI = 0.0059–0.0200, p = 0.0004) models (Table 3).
Associations of PR with study outcomes
PR was positively associated with T25FW performance in unadjusted (estimate = 0.3416, 95% CI = 0.2600–0.4232, p < 0.0001) and adjusted (estimate = 0.3287, 95% CI = 0.2555– 0.4020, p < 0.0001) models. PR was further positively associated with SDMT performance in unadjusted (estimate = 1.4429, 95% CI = 0.4631–2.3591, p = 0.0023) and adjusted (estimate = 1.1603, 95% CI = 0.2721–2.0485, p = 0.0109) models (Table 4).
Associations of IR with study outcomes
T25FW
The primary contrasts of interest used low IR as a reference. Results showed that in unadjusted analysis, compared to low IR, all IR levels were positively associated with T25FT performance (high CR low PR: estimate = 0.4936, 95% CI = 0.0256–0.0616, p = 0.0389; low CR high PR: estimate = 0.7746, 95% CI = 0.3065–1.2426, p = 0.0014; high CR high PR: estimate = 1.2905, 95% CI = 0.8914–1.6896, p < 0.0001). Results from adjusted analysis were similar showing that compared to low IR, all IR levels were positively associated with T25FW performance (high CR low PR: estimate = 0.2108, 95% CI = 0.2009–0.1.0355, p = 0.0040; low CR high PR: estimate = 0.7734, 95% CI = 0.3619–1.1849, p = 0.0003; high CR high PR: estimate = 1.3658, 95% CI = 1.0091–1.7224, p < 0.0001).
SDMT
Results showed that in unadjusted analysis, compared to low IR, one intermediate and high IR levels were positively associated with SDMT performance (high CR low PR: estimate = 9.6607, 95% CI = 5.2659–14.0556, p < 0.0001; high CR high PR: estimate = 11.500, 95% CI = 7.7521–15.2479, p < 0.0001). The intermediate level of IR comprised of low CR and high PR was not significantly different than low IR (estimate = 3.5774, 95% CI = – 0.8175 to 7.9722, p = 0.1097). Results from adjusted analysis were similar showing that compared to low IR, one intermediate and high IR levels were positively associated with SDMT performance (high CR low PR: estimate = 8.8395, 95% CI = 4.5250–13.1540, p < 0.0001; high CR high PR: estimate = 10.5069, 95% CI = 6.8196–14.1914, p < 0.0001). The intermediate level of IR comprised of low CR and high PR, was not significantly different than low IR (estimate = 2.6747, 95% CI = – 1.5897 to 6.9292, p = 0.2157) (see Table 5 for complete analyses and all pairwise comparisons).
MS group status: moderation effects on associations of reserve measures with study outcomes
CR: MS group status did not moderate the association of CR with T25FW in unadjusted or adjusted models (unadjusted: estimate = 0.0045, 95% CI = – 0.0103 to 0.0193, p = 0.5470; adjusted: estimate = 0.0031, 95% CI = – 0.0109 to 0.0172, p = 0.6603). MS status did not moderate the association of CR with SDMT in unadjusted or adjusted models (unadjusted: estimate = 0.2426, 95% CI = – 0.1495 to 0.0901, p = 0.6250; adjusted: estimate = – 0.0049, 95% CI = – 0.1215 to 0.1117, p = 0.9338) (Supplemental Table 3).
PR: MS group status did not moderate the association of PR with T25FW in unadjusted or adjusted models (unadjusted: estimate = 0.0928, 95% CI = – 0.0859 to 0.2715, p = 0.3062; adjusted: estimate = – 0.0814, 95% CI = – 0.0878 to 0.2506, p = 0.3429) models. MS status marginally moderated the association of PR with SDMT in unadjusted but not in adjusted models (unadjusted: estimate = – 2.0357, 95% CI = – 4.0727 to 0.0013, p = 0.0501; adjusted: estimate = – 1.2405, 95% CI = – 3.2865 to 0.8056, p = 0.2324) (Supplemental Table 4).
IR: MS group status did not moderate the association of IR with SDMT in unadjusted or adjusted analyses (unadjusted: f = 0.3200, df = 3, MS = 24.7279, p = 0.8102; adjusted: f = 0.2100, df = 3, MS = 14.2177, p = 0.8927) (Supplemental Table 5). MS group status did moderate the association of IR with T25FW in unadjusted and adjusted analyses (unadjusted: f = 3.2700, df = 3, MS = 2.4231, p = 0.0235; adjusted: f = 3.3900, df = 3, MS = 2.0364, p = 0.0204) (Supplemental Table 5). Further group-stratified regression analyses revealed that among control participants, only high IR was associated with better T25FW performance compared to low IR in unadjusted and adjusted analyses (unadjusted: estimate = 0.7876, 95% CI = 0.2916–1.2835, p = 0.0023; adjusted: estimate = 0.8061, 95% CI = 0.3647–1.2474, p = 0.0006). In contrast, among MS participants, results showed that compared to low IR, all IR levels were positively associated with T25FW performance in unadjusted analysis (high CR low PR: estimate = 0.9225, 95% CI = 0.2852–1.5597, p = 0.0052; low CR high PR: estimate = 1.3182, 95% CI = 0.6100–2.0265, p = 0.0004; high CR high PR: estimate = 1.8587, 95% CI = 1.2937–2.4237, p < 0.0001). These associations remained significant in adjusted analysis. Compared to low IR, all IR levels were positively associated with T25FW performance (high CR low PR: estimate = 0.9550, 95% CI = 0.3504–1.5595, p = 0.0025; low CR high PR: estimate = 1.3603, 95% CI = 0.6791–2.0415, p = 0.0002; high CR high PR: estimate = 1.9041, 95% CI = 1.3620–2.4463, p < 0.0001) (Supplemental Table 6).
IR: moderation effects on associations of brain atrophy and study outcomes
We additionally evaluated whether associations between brain atrophy and study outcomes were attenuated by intermediate to high IR when compared to low IR. Two-level IR status (intermediate to high IR vs low IR) left thalamus and their interaction were included in the models predicting T25FW and SDMT performances. Results showed that the moderating effect of IR status on the association of left thalamus with T25FW performance was significant (interaction effect estimate = -0.0005, 95% CI = – 0.0010 to – 0.0001, p = 0.0300). IR status-stratified analyses further revealed that left thalamic volume was significantly associated with T25FW performance in the low (n = 42, left thalamic effect estimate = 0.0007, p = 0.0011) but not intermediate to high (n = 90, estimate = 0.0002, p = 0.2395) IR group. Similarly, the moderating effect of IR status on the association of left thalamus with SDMT performance was significant (interaction effect estimate = – 0.0056, 95% CI = – 0.0099 to – 0.0013, p = 0.0107). IR status-stratified analyses revealed that left thalamic volume was significantly associated with SDMT performance in the low IR group (n = 42, left thalamic effect estimate = 0.0072, p = 0.0002) but not intermediate to high (n = 90, estimate = 0.0016, p = 0.2214) IR group.
Discussion
The current study proposes IR as a broader construct comprised of both cognitive and physical domains. We found that CR and PR were positively associated with each other and with SDMT and T25FW performances. Results further showed that those with low IR performed worst on the SDMT and T25FW compared to individuals with intermediate and high IR and were most vulnerable to associations of brain atrophy with study outcomes. These findings are discussed below.
We used the same method to quantify residual-derived CR and PR measures. This approach presents conceptual and empirical advantages removing, at the individual level, confounding effects of brain atrophy and socio-demographic variables from both reserve dimensions. The significant correlation between CR and PR supports the notion of a broader IR construct that better represents within-person reserve capacities that could impact how one executes cognitive and motoric tasks in the context of adverse aging and disease-related effects. Recent meta-analytic studies demonstrated that compared to traditional measures residual-derived CR provided better protection against cognitive decline [14, 55]. CR effects on physical outcomes are not well documented but two recent studies extended the literature on residual-derived CR to mobility outcomes. Using functional near-infrared-spectroscopy, the first study demonstrated that higher CR was associated with more efficient prefrontal cortex activation assessed during active walking under single and dual-task conditions [16]. The second study found that higher baseline CR was associated with reduced risk of developing incident gait impairment [17] suggesting that the protective effect of CR was extended to more distal physical outcomes. The extant limited literature concerning PR or related constructs has not utilized the residual approach to define PR. This gap in research is at odds with well-replicated associations between cognitive and physical function in aging [19,20,21], and MS [22, 23], and established role of slow gait speed as a predictor of dementia [25] and multiple health outcomes [24]. The current study provides evidence that lower CR and PR were associated with worse SDMT and T25FW performances suggesting that reserve capacities in both domains were associated with proximal and distal outcomes.
We combined CR and PR to create a mutually exclusive 4-level IR variable. The quadrant approach, previously used to demonstrate the utility of combining traits/dimensions within a broader construct to identify individuals at risk of poor executive functions and walking [56] and longitudinal cognitive decline [57], is especially relevant to the current study examining the clinical utility of combined CR and PR dimensions that presumably represent a broader reserve construct. This approach facilitates the clinical extrapolation and utility of multiple reserve dimensions within a person. Specifically, individuals with low IR were presumed to be most vulnerable to adverse effects of aging and neurological disease. Therefore, a priori, we used this group as a reference condition for other IR levels predicting that individuals low on both IR dimensions would perform worse than individuals with intermediate or high IR. Results revealed that T25FW performance was indeed poor in the low IR group compared to the intermediate and high IR groups. With respect to SDMT performance, the low IR group performed worse compared to the high IR group and one intermediate IR (high CR low PR) group, but not compared to the second (low CR and high PR) intermediate IR group. These results suggest that high PR when combined with low CR did not provide an advantage with respect to cognitive performance. Additional comparisons between the intermediate and high IR groups suggested a preference for domain-specific advantage wherein both intermediate and high IR levels provided an advantage with respect to performance on a clinical outcome proximal to the high reserve dimension. These results, however, should be interpreted with caution as the study may have been underpowered to evaluate such nuanced and more exploratory comparisons.
The presence of MS did not influence separate associations of CR and PR with clinical outcomes nor the association of IR with the SDMT. These findings suggest a generalized beneficial effect of reserve capacities that extend from normal aging into neurological disease. MS status, however, did moderate associations between IR and performance on the T25FW. Specifically, among patients with MS, low IR was associated with poor walking performance compared to both intermediate and high IR groups. In contrast, among control participants, low IR was associated with poor walking performance in comparison to the high but not intermediate IR groups. These results suggest that IR-related compensation is greater among patients with MS who benefited from intermediate IR levels to support mobility function compromised by deleterious and likely synergetic disease and aging effects.
Research has shown that CR may influence the impact of brain pathology on cognitive decline [58,59,60]. The current study was designed to extend this work to a broader reserve measure, IR, to determine whether it moderated associations between brain atrophy and study outcomes. Thalamic atrophy [45] notably in the left thalamic nuclei [46] is a marker for more generalized brain pathology in aging that has been associated with multiple outcomes in MS [47]. Thalamic volume correlated with SDMT and T25FW performances in the current study. We, therefore, evaluated whether IR moderated associations between left thalamic atrophy and study outcomes. Consistent with the study hypothesis, results revealed that compared to low IR combined intermediate and high IR attenuated associations between the left thalamus and performances on the SDMT and T25FW. Specifically, associations between thalamic volume and study outcomes were evident among individuals with low, but not intermediate to high IR. The attenuation of the association between thalamic volume and performance outcomes as a function of IR is noteworthy suggesting compensatory function against brain atrophy that generalizes to both cognitive and physical outcomes. Furthermore, given that sample size was much smaller in the low IR group, the insignificant associations between thalamus and clinical outcomes in the intermediate to high IR levels could not be attributed to small sample size or restricted range in the predictor or outcome variables.
Study strengths, limitations and future directions
The RBANS and SPPB are well-established measures of cognitive and physical function, respectively. Hence, using residual-based variance to quantify reserve capacities in both domains based on these objective tests is justified. Furthermore, their common usage will facilitate replication studies across normal and disease populations. Whereas research on CR is extensive, the literature concerning PR has been limited, notably in terms of construct development and measurement [61]. The inclusion of the SPPB as a primary broad objective measure of physical function in numerous observational studies and clinical trials makes it optimal to assess residual-derived PR capacities whose clinical utility should be examined in normal and clinical populations. We note, however, that the range of scores on the SPPB is more restricted as compared to the RBANS. While inspection of the distribution of residual SPPB scores which were used to operationalize PR did not suggest skewness or restriction of range, alternative measures may be considered. For example, walking speed, a robust proxy of health outcomes [24], alone or in combination with other continuous quantitative measures of gait could be used to operationalize PR in future studies. The correlation between CR and PR supported the derivation of a broader 4-level IR construct quantifying within-person reserve in both domains in a manner that could facilitate clinical utility. We further suggest that IR has potential compensatory functions that could influence individual responses to interventions. The SDMT and T25FW have been established as primary outcomes in clinical trials. The meaningful associations reported between IR and performances on these tests bolster its potential construct validity and clinical utility. Although the SDMT and T25FW were not used to derive the reserve variables, some concerns regarding circularity between the predictor and outcome variables might exist given similarities in their domains of function, and notably given the cross-sectional study design. Furthermore, inferences regarding causality and longitudinal protective effects of IR should be examined in future cohort and intervention studies. Participants were ambulatory and met additional MRI inclusion criteria, generalizability of the findings to more variable and impaired samples should be evaluated. The unweighted summation of 10 diseases used to derive the GHS variable provided limited adjustment for comorbidity in the current study. Finally, IR introduces a broader conceptualization of reserve capacities based on established relationships of cognitive and physical function, however, inclusion of mood as a third dimension may be a limitation to be addressed in future research.
Conclusion
We proposed a novel and more comprehensive reserve construct, IR, that captures collective cognitive and physical reserve capacities within a person. Low IR levels were associated with worse performances and greater vulnerability to the impact of brain atrophy on cognitive and motor outcomes in aging and neurological disease.
Data availability
The data that support the findings of this study are available from the corresponding author, [RH], upon reasonable request.
Abbreviations
- CR :
-
Cognitive reserve
- FLAIR :
-
Fluid-attenuated inversion recovery
- GHS :
-
Global health status
- IR :
-
Individual reserve
- IRB :
-
Institutional review board
- MRI :
-
Magnetic resonance imaging
- MS :
-
Multiple sclerosis
- PR :
-
Physical reserve
- RBANS :
-
Repeatable battery for the assessment of neuropsychological status
- SPPB :
-
Short physical performance battery
- WM :
-
White matter
References
Smrtka J, Brown T, Bjorklund G (2016) Loss of mobility and the patient burden of multiple sclerosis: expert opinion on relevance to daily clinical practice. Postgrad Med 128(1):145–151
Soler B et al (2020) Clinical assessment, management, and rehabilitation of walking impairment in MS: an expert review. Expert Rev Neurother 20(8):875–886
Benedict RHB et al (2020) Cognitive impairment in multiple sclerosis: clinical management, MRI, and therapeutic avenues. Lancet Neurol 19(10):860–871
Meca-Lallana V et al (2021) Cognitive impairment in multiple sclerosis: diagnosis and monitoring. Neurol Sci 42(12):5183–5193
Marrie RA et al (2014) Intensive care unit admission in multiple sclerosis: increased incidence and increased mortality. Neurology 82(23):2112–2119
Bahureksa L et al (2017) The impact of mild cognitive impairment on gait and balance: a systematic review and meta-analysis of studies using instrumented assessment. Gerontology 63(1):67–83
Beauchet O et al (2016) Poor Gait performance and prediction of dementia: results from a meta-analysis. J Am Med Dir Assoc 17(6):482–490
Demnitz N et al (2016) A systematic review and meta-analysis of cross-sectional studies examining the relationship between mobility and cognition in healthy older adults. Gait Posture 50:164–174
Learmonth YC, Ensari I, Motl RW (2016) Cognitive motor interference in multiple sclerosis: Insights from a systematic, quantitative review. Arch Phys Med Rehabil 98:1229
Gunn HJ et al (2013) Identification of risk factors for falls in multiple sclerosis: a systematic review and meta-analysis. Phys Ther 93(4):504–513
Stern Y (2009) Cognitive reserve. Neuropsychologia 47(10):2015–2028
Stern Y (2012) Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol 11(11):1006–1012
Stern Y et al (2020) Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimers Dement 16(9):1305–1311
Nelson ME et al (2021) Cognitive reserve, Alzheimer’s neuropathology, and risk of dementia: a systematic review and meta-analysis. Neuropsychol Rev 1:1–18
Santangelo G et al (2019) Does cognitive reserve play any role in multiple sclerosis? A meta-analytic study. Mult Scler Relat Disord 30:265–276
Holtzer R et al (2021) Cognitive reserve moderates the efficiency of prefrontal cortex activation patterns of gait in older adults. J Gerontol A Biol Sci Med Sci 77:1836–1844
Holtzer R et al (2022) Cognitive reserve and risk of mobility impairment in older adults. J Am Geriatr Soc 70:3096–3104
Whitson HE et al (2016) Physical resilience in older adults: systematic review and development of an emerging construct. J Gerontol A Biol Sci Med Sci 71(4):489–495
Clouston SA et al (2013) The dynamic relationship between physical function and cognition in longitudinal aging cohorts. Epidemiol Rev 35(1):33–50
Li KZH et al (2018) Cognitive involvement in balance, gait and dual-tasking in aging: a focused review from a neuroscience of aging perspective. Front Neurol 9:913
Paraskevoudi N, Balcı F, Vatakis A (2018) “Walking” through the sensory, cognitive, and temporal degradations of healthy aging. Ann N Y Acad Sci 1426:72–92
Benedict RH et al (2011) Upper and lower extremity motor function and cognitive impairment in multiple sclerosis. J Int Neuropsychol Soc 1:1–11
Baldasso BD et al (2022) Better cognitive function predicts maintenance of dual-task walking ability over time among people with relapsing-remitting MS. Neuropsychology 36(6):520–527
Studenski S et al (2011) Gait speed and survival in older adults. JAMA 305(1):50–58
Quan M et al (2017) Walking pace and the risk of cognitive decline and dementia in elderly populations: a meta-analysis of prospective cohort studies. J Gerontol A Biol Sci Med Sci 72(2):266–270
Dauwan M et al (2021) Physical exercise improves quality of life, depressive symptoms, and cognition across chronic brain disorders: a transdiagnostic systematic review and meta-analysis of randomized controlled trials. J Neurol 268(4):1222–1246
Reed BR et al (2010) Measuring cognitive reserve based on the decomposition of episodic memory variance. Brain 133(Pt 8):2196–2209
Randolph C et al (1998) The repeatable battery for the assessment of neuropsychological status (RBANS): preliminary clinical validity. J Clin Exp Neuropsychol 20(3):310–319
Guralnik JM et al (2000) Lower extremity function and subsequent disability: consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J Gerontol A Biol Sci Med Sci 55(4):M221–M231
Hoffmann K et al (2016) Moderate-to-high intensity physical exercise in patients with Alzheimer’s Disease: a randomized controlled trial. J Alzheimers Dis 50(2):443–453
DeLuca J et al (2021) Effect of ozanimod on symbol digit modalities test performance in relapsing MS. Mult Scler Relat Disord 48:102673
Koch MW et al (2021) Comparison of the EDSS, timed 25-foot walk, and the 9-hole peg test as clinical trial outcomes in relapsing-remitting multiple sclerosis. Neurology 97(16):e1560–e1570
Koch MW et al (2022) The timed 25-foot walk is a more sensitive outcome measure than the EDSS for PPMS trials: an analysis of the PROMISE clinical trial dataset. J Neurol 269(10):5319–5327
McKenzie C et al (2022) Residual reserve index modifies the effect of amyloid pathology on fluorodeoxyglucose metabolism: Implications for efficiency and capacity in cognitive reserve. Front Aging Neurosci 14:943823
Ersoezlue E et al (2023) Lifelong experiences as a proxy of cognitive reserve moderate the association between connectivity and cognition in Alzheimer’s disease. Neurobiol Aging 122:33–44
Oosterhuis EJ et al (2022) Towards an understanding of healthy cognitive ageing: The importance of lifestyle in cognitive reserve and the scaffolding theory of aging and cognition. J Gerontol B Psychol Sci Soc Sci. https://doi.org/10.1093/geronb/gbac197
Thompson AJ et al (2018) Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol 17(2):162–173
Holtzer R et al (2008) Within-person across-neuropsychological test variability and incident dementia. JAMA 300(7):823–830
Bollaert RE et al (2017) Preliminary evidence for the effects of aging and multiple sclerosis on cognitive performance: an analysis based on effect size estimates. Exp Aging Res 43(4):346–354
Beatty WW (2004) RBANS analysis of verbal memory in multiple sclerosis. Arch Clin Neuropsychol 19(6):825–834
Torrence ND et al (2016) An empirical comparison of competing factor structures for the repeatable battery for the assessment of neuropsychological status: a project Frontier study. Arch Clin Neuropsychol 31(1):88–96
Motl RW et al (2018) Physical function in older adults with multiple sclerosis: an application of the short physical performance battery. J Geriatr Phys Ther 41(3):155–160
Simon JH (2014) MRI outcomes in the diagnosis and disease course of multiple sclerosis. Handb Clin Neurol 122:405–425
Wu X et al (2021) Pathogeneses and imaging features of cerebral white matter lesions of vascular origins. Aging Dis 12(8):2031–2051
Qing Z et al (2021) Causal structural covariance network revealing atrophy progression in Alzheimer’s disease continuum. Hum Brain Mapp 42(12):3950–3962
Low A et al (2019) Asymmetrical atrophy of thalamic subnuclei in Alzheimer’s disease and amyloid-positive mild cognitive impairment is associated with key clinical features. Alzheimers Dement (Amst) 11:690–699
Amin M, Ontaneda D (2020) Thalamic injury and cognition in multiple sclerosis. Front Neurol 11:623914
Liu LK et al (2020) Cerebellar-limbic neurocircuit is the novel biosignature of physio-cognitive decline syndrome. Aging (Albany NY) 12(24):25319–25336
Schmidt P et al (2012) An automated tool for detection of FLAIR-hyperintense white-matter lesions in Multiple Sclerosis. Neuroimage 59(4):3774–3783
Fischl B (2012) FreeSurfer. Neuroimage 62(2):774–781
Fischl B et al (2002) Whole brain segmentation: automated labeling of neuroanatomical structures in the human brain. Neuron 33(3):341–355
Fischl B et al (2004) Automatically parcellating the human cerebral cortex. Cereb Cortex 14(1):11–22
Desikan RS et al (2006) An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage 31(3):968–980
Hocking RR (1976) A Biometrics invited paper: “The analysis and selection of variables in linear regression. Biometrics 32:1–49
Bocancea DI et al (2021) Measuring resilience and resistance in aging and alzheimer disease using residual methods: a systematic review and meta-analysis. Neurology 97(10):474–488
LeMonda BC et al (2015) The association between high neuroticism-low extraversion and dual-task performance during walking while talking in non-demented older adults. J Int Neuropsychol Soc 21(7):519–530
Crowe M et al (2006) Personality and risk of cognitive impairment 25 years later. Psychol Aging 21(3):573–580
Moran C et al (2019) Type 2 diabetes mellitus, brain atrophy, and cognitive decline. Neurology 92(8):e823–e830
Vonk JMJ et al (2022) The role of cognitive and brain reserve in memory decline and atrophy rate in mid and late-life: The SMART-MR study. Cortex 148:204–214
Zahodne LB et al (2015) Is residual memory variance a valid method for quantifying cognitive reserve? A longitudinal application. Neuropsychologia 77:260–266
Bhanji RA, Watt KD (2021) Physiologic reserve assessment and application in clinical and research settings in liver transplantation. Liver Transpl 27(7):1041–1053
Funding
This research was supported by grants from the National Institutes of Health (R01NS109023).
Author information
Authors and Affiliations
Contributions
RH: drafting/revision of the manuscript for content, including medical writing for content; major role in the acquisition of data; study concept or design; analysis or interpretation of data; JC: drafting/revision of the manuscript for content, including medical writing for content; analysis or interpretation of data; RWM: drafting/revision of the manuscript for content, including medical writing for content; FWF: drafting/revision of the manuscript for content, including medical writing for content; MAP: drafting/revision of the manuscript for content, including medical writing for content; MLL: analysis or interpretation of data; MI: analysis or interpretation of data; MH: drafting/revision of the manuscript for content, including medical writing for content; MW: drafting/revision of the manuscript for content, including medical writing for content; analysis or interpretation of data.
Corresponding author
Ethics declarations
Conflicts of interest
The authors have no conflicts of interest to report in relation to the current article. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Ethics statement
The work described in this manuscript has been executed in adherence with The Code of Ethics of the World Medical Association (Declaration of Helsinki).
Informed consent
Participants signed written informed consents in the first in-person study visit.
Institutional review board
Albert Einstein College of Medicine Institutional Review Board approved this study (IRB #: 2019–10049).
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Holtzer, R., Choi, J., Motl, R.W. et al. Individual reserve in aging and neurological disease. J Neurol 270, 3179–3191 (2023). https://doi.org/10.1007/s00415-023-11656-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-023-11656-8