
Abstract
Background
Distinguishing grade 1 chondrosarcoma from grade 2 chondrosarcoma is critical both for planning the surgical procedure and for predicting the outcome. We aimed to review the preoperative radiographic and histologic findings, and to evaluate the reliability of preoperative grading.
Methods
We retrospectively reviewed the medical records of 17 patients diagnosed with central chondrosarcoma at our institution between 1996 and 2011. In these cases, we compared the preoperative and postoperative histologic grades, and evaluated the reliability of the preoperative histologic grading. We also assessed the preoperative radiographic findings obtained using plain radiography, computed tomography (CT), and magnetic resonance imaging (MRI).
Results
Preoperative histologic grade was 1 in 12 patients, 2 in 4 patients, and 3 in 1 patient. However, 6 of the 12 cases classified as grade 1 before surgery were re-classified as grade 2 postoperatively. In the radiographic evaluation, grade 1 was suspected by the presence of a ring-and-arc pattern of calcification on plain radiography and CT and entrapped fat and ring-and-arc enhancement on MRI. Grades 2 and 3 were suspected by the absence of calcification and the presence of cortical penetration and endosteal scalloping on plain radiography and CT, as well as soft-tissue mass formation on MRI.
Conclusion
Although the combination of radiographic interpretation and histologic findings may improve the accuracy of preoperative grading in chondrosarcoma, the establishment of a standard evaluation system with the histologic and radiographic findings and/or the development of new biologic markers are necessary for preoperative discrimination of low-grade chondrosarcoma from high-grade chondrosarcoma.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Chondrosarcoma is the second most frequent primary malignant bone tumor after osteosarcoma [1] and represents a heterogeneous group of tumors, ranging from indolent, low-grade lesions (grade 1) to aggressive, high-grade neoplasms (grades 2, 3). Recently, some authors advocated the adequacy of intralesional surgery for grade 1 chondrosarcoma [2–8]. However, this tumor remains a challenge to diagnose accurately and treat effectively.
The histologic grading system is separated into three grades, based on cellularity, atypia, and pleomorphism [9], and is related to prognosis [10–12]. Accurate preoperative grading of chondrosarcoma is required because it determines the surgical approach and outcome. However, biopsy specimens do not always determine a correct diagnosis of grade [13, 14]. For this reason, it is particularly important to combine radiographic interpretation with histologic findings. Recent studies of magnetic resonance imaging (MRI) have improved the sensitivity in differential diagnosis [15–17]. The purpose of this study was to review the preoperative radiographic and histologic findings that differentiate low-grade chondrosarcoma (grade 1) from high-grade chondrosarcoma (grades 2, 3), and to evaluate the reliability of preoperative grading.
Materials and methods
This study was conducted with the approval of our institutional review board.
We retrospectively reviewed the medical records of 17 patients diagnosed with central chondrosarcoma at our institution from 1 January 1996 to 31 December 2011. There were 10 men and 7 women, with a mean age at time of diagnosis of 66 years (range 38–85 years). The tumors were located in the humerus (n = 4), ulna (n = 1), phalange (n = 2), femur (n = 7), tibia (n = 1), calcaneus (n = 1), and rib (n = 1). The final histologic grade of the resected tumor was 1 in 6 patients, 2 in 10 patients, and 3 in 1 patient.
In these cases, we compared the preoperative and postoperative histologic grading and evaluated the reliability of the preoperative histologic grading. The histologic grading system we used was based on that described by Evans and colleagues [9]. The typical histology of each grade is shown in Fig. 1. We also assessed the preoperative radiographic findings on plain radiography, computed tomography (CT), and MRI.

Histologic features of chondrosarcoma. a Grade 1: tumors are moderately cellular with chondroid matrix and absent mitosis. b Grade 2: tumors are more cellular with a greater degree of nuclear atypia and hyperchromasia and larger nuclear size. c Grade 3: tumors are densely cellular and pleomorphic. Mitoses are easily detected [hematoxylin and eosin staining; original magnification, ×100 in (a–c)]
On plain radiography and CT, we evaluated the findings of low-grade chondrosarcoma (grade 1), such as a ring-and-arc pattern of calcification, and those of high-grade chondrosarcoma (grades 2, 3), such as the absence of calcification and the presence of cortical penetration and endosteal scalloping [18]. On MRI, we evaluated the findings of low-grade chondrosarcoma, such as entrapped fat within the tumor, lobular architecture, and ring-and-arc enhancement, and those of high-grade chondrosarcoma, such as central high signal on T1-weighted images, soft-tissue mass formation, and central non-enhancement portion [19]. The ring-and-arc pattern of calcification usually represents the pathologic characteristic of enchondral ossification about the margin of the cartilaginous lobules (Fig. 2a) [18]. Higher-grade chondrosarcomas often contain relatively less extensive areas of matrix mineralization. The absence of calcification and the presence of cortical penetration, endosteal scalloping, and soft-tissue mass formation represent a more aggressive pattern, which may be seen with higher-grade (grades 2, 3) chondrosarcoma (Figs. 2b, c, and 3a). Entrapped fat on T1-weighted MR images is defined as a less-aggressive finding, with entrapped areas of pre-existing yellow marrow, which is seen as small, speckled, punctate lesions (Fig. 3b). Central high signal on T1-weighted MR images and a central non-enhancement pattern represent hemorrhagic cystic change within the tumor, which may be seen in high-grade chondrosarcoma [19].

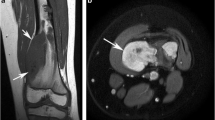
Radiographic findings of chondrosarcoma. a Presence of a ring-and-arc pattern of calcification. b Absence of calcification (arrow). c Presence of cortical penetration (arrows) and endosteal scalloping (arrowheads) is defined

Magnetic resonance imaging findings of chondrosarcoma. a Axial T2-weighted fat-suppressed image showing soft-tissue mass formation. b Coronal T1-weighted image showing entrapped fat (arrows), which indicates entrapped areas of pre-existing yellow marrow
Radiographic grading was determined by these findings and compared with the postoperative histologic grading. Finally, we reviewed the reliability and limitations of this combination of preoperative histologic and radiographic gradings.
Results
The clinical and histologic data of the 17 patients are summarized in Table 1. The method of preoperative histologic grading was needle biopsy in 4 patients, excisional biopsy in 12 patients, and curettage in 1 patient. Preoperative histologic grading was 1 in 12 patients, 2 in 4 patients, and 3 in 1 patient. However, 6 of 12 patients evaluated as grade 1 before surgery were changed to grade 2 in postoperative grading. In these 6 cases, 2 of 4 patients were diagnosed via needle biopsy. In 3 of 5 patients who had metastases, the histologic grade was changed from grade 1 to grade 2 after surgery. One of two grade 2 patients with local recurrence was evaluated as grade 1 before surgery and was selected for intralesional curettage.
In the radiographic evaluation, findings of plain radiography and CT are summarized in Table 2. Extensive areas of ring-and-arc pattern of calcification within the tumor were seen in four of six patients categorized as grade 1 (67 %) but only focally in patients of grades 2 and 3. The absence of calcification within the tumor and the presence of cortical penetration and endosteal scalloping were seen in most patients of grade 2 and 3, but only a few patients of grade 1. MRI revealed entrapped fat within the tumor on T1-weighted images and ring-and-arc enhancement on gadolinium-enhanced T1-weighted images in most patients of grade 1, while soft-tissue mass formation was seen more frequently in grades 2 and 3 (Table 3). However, in patients of grade 2, ring-and-arc enhancement was detected in only a small area of the tumor. Central high signal on T1-weighted images was seen in a few cases in all the patients. Lobular architecture and a central non-enhancing portion were detected in all grades. The results above demonstrated that grade 1 (low-grade chondrosarcoma) was suspected by the presence of an extensive area of ring-and-arc pattern of calcification on plain radiography and CT, as well as entrapped fat and ring-and-arc enhancement on MRI. However, grades 2 and 3 (high-grade chondrosarcoma) were suspected by the absence of calcification and the presence of cortical penetration and endosteal scalloping on plain radiography and CT, as well as soft-tissue mass formation on MRI (Table 4). According to these criteria, we could confirm the findings of high-grade chondrosarcoma in all six cases changed from grade 1 to grade 2 postoperatively. However, two of six cases categorized as grade 1 postoperatively had the radiographic characteristics of high-grade chondrosarcoma (Fig. 4).

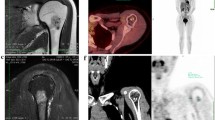
A 48-year-old man with a low-grade (grade 1) chondrosarcoma in the femur. a, b Anteroposterior radiography and computed tomography showing endosteal scalloping and the absence of calcification. c Coronal T1-weighted gadolinium-enhanced fat-suppressed magnetic resonance image showing a large area of central non-enhancement within the tumor. d Coronal T2-weighted image showing extensive bone marrow edema
Discussion
Although several studies have reviewed the differentiation criteria of grade 1 chondrosarcoma from enchondroma [13, 16, 18, 20–24], distinguishing grade 2 chondrosarcoma from grade 1 chondrosarcoma has hardly been discussed. However, distinguishing grade 1 chondrosarcoma from grade 2 chondrosarcoma is clinically among the most important aspects of diagnosis, both for planning the surgical procedure and for predicting the outcome because (1) grade 1 lesions almost never metastasize [9, 25], but grade 2 or 3 lesions tend to recur and form metastases, and (2) intralesional treatment may be adequate for grade 1 chondrosarcoma in contrast to grade 2 or 3 lesions, which may require wide resection [2–8]. We also discuss grade evaluation of several cases of chondrosarcoma at a tumor board meeting before surgery. However, the difficulties of these grade interpretations between grade 1 and grade 2 long have been suspected because there is a lack of criteria to define the limits between different subtypes. Furthermore, we often cannot determine the correct histologic grade with small biopsy specimens preoperatively since chondrosarcoma might have various histologic grades within the same tumor [11, 13]. Actually, our data indicated that preoperative histologic grading with biopsy specimens had low reliability. In our study, 6 of 12 patients evaluated as grade 1 before surgery were changed to grade 2 in postoperative grading. In these six cases, two of four patients were graded via needle biopsy. According to previous reports, a needle biopsy does not always determine a correct diagnosis of grade [12, 15]. Although needle biopsy may be performed as the first method for histologic evaluation, excisional biopsy should be performed as well when the differentiation of grade 1 from grade 2 chondrosarcoma is difficult by needle biopsy alone.
Therefore, it is particularly important to combine radiographic interpretation with histologic findings. In our study, the presence of an extensive area of ring-and-arc pattern of calcification is more common in low-grade (grade 1) chondrosarcoma, while the absence of calcification and the presence of cortical penetration and endosteal scalloping is more common in high-grade (grades 2, 3) chondrosarcoma on plain radiography and CT. Moreover, entrapped fat within the tumor and ring-and-arc enhancement are more characteristic of low-grade chondrosarcoma, but soft-tissue mass formation is more common in high-grade chondrosarcoma on MRI. Taken together, our data indicated that an extensive area of ring-and-arc pattern of calcification on CT and entrapped fat within the tumor and ring-and-arc enhancement on MRI had intermediate sensitivity (67, 67, 67 %, respectively), high specificity (100, 90, 100 %, respectively), and a positive predictive value (PPV) (100, 90, 100 %, respectively) in grade 1 chondrosarcoma. The absence of calcification and the presence of cortical penetration and endosteal scalloping on plain radiography and CT had high sensitivity (100, 100, 80 %, respectively) and a PPV (83, 83, 89 %, respectively), while soft-tissue mass formation on MRI had high specificity (83 %) and a PPV (88 %) in grade 2 chondrosarcoma (Table 4).
A previous study reported that a relatively less extensive area of matrix mineralization is often seen in higher-grade chondrosarcomas on plain radiography and CT [18]. Another study reported that soft-tissue mass formation favors the diagnosis of high-grade chondrosarcoma, and entrapped fat within the tumor is highly indicative of low-grade chondrosarcoma on MRI [19]. In addition, the radiographic classification of Lodwick is used as an index to predict the biologic behavior of bone tumors and tumor-like lesions; this classification is commonly applied for chondrosarcoma [26, 27]. Our data, which were gathered by evaluating plain radiography, CT, and MRI in the same series, were consistent with the results of previous studies. Therefore, we advocate preoperative grading in the context of a combination of findings on plain radiography, CT, and MRI to more accurately differentiate low-grade chondrosarcoma from high-grade chondrosarcoma since some cases do not have characteristic radiographic findings. If treating physicians use this method, they can avoid treating as grade 1 for grade 2 chondrosarcoma. However, two cases of grade 1 chondrosarcoma that were evaluated as grade 2 preoperatively with radiographic findings were treated with wide resection in the present study. Thus, the value of morphologic radiographic features in differentiating low-grade chondrosarcoma from high-grade chondrosarcoma was shown to be limited. In the present status, we should select wide resection if the radiographic findings have the characteristics of grade 2 in spite of a histologic evaluation pointing to grade 1. In addition, it is necessary to consider the location of the chondrosarcoma when determining the treatment strategy because chondrosarcomas arising from the pelvis or axial skeleton are generally associated with greater biologic aggressiveness and more frequent recurrence. Wide resection should be selected for these locations even if the radiographic and/or histologic findings show characteristics of grade 1 chondrosarcoma.
Recently, a new biomarker has been investigated for its ability to distinguish low-grade from high-grade chondrosarcoma and to predict clinical outcomes. Takeuchi et al. [28] demonstrated that significant differences in the endogenous secretory receptor for advanced glycation end products (esRAGE) labeling index were seen between grade 1 and grade 2 chondrosarcomas using an enzyme-linked immunosorbent assay (ELISA) in 11 cases of chondrosarcoma. However, further large-scale prospective studies are required to validate these markers as routine diagnostic and prognostic tools in the assessment of chondrosarcoma. In the future, the establishment of a standard evaluation system combining radiographic interpretation with histologic findings and/or the development of new biologic markers is necessary for accurately discriminating low-grade chondrosarcoma from high-grade chondrosarcoma prior to surgery.
References
Lee FY, Mankin HJ, Fondren G, Gebhardt MC, Springfield DS, Rosenberg AE, Jennings LC (1999) Chondrosarcoma of bone: an assessment of outcome. J Bone Joint Surg Am 81(3):326–338
Leerapun T, Hugate RR, Inwards CY, Scully SP, Sim FH (2007) Surgical management of conventional grade I chondrosarcoma of long bones. Clin Orthop Relat Res 463:166–172. doi:10.1097/BLO.0b013e318146830f
Hanna SA, Whittingham-Jones P, Sewell MD, Pollock RC, Skinner JA, Saifuddin A, Flanagan A, Cannon SR, Briggs TWR (2009) Outcome of intralesional curettage for low-grade chondrosarcoma of long bones. Eur J Surg Oncol 35(12):1343–1347. doi:10.1016/j.ejso.2009.06.001
Aarons C, Potter BK, Adams SC, Pitcher JD, Temple HT (2009) Extended intralesional treatment versus resection of low-grade chondrosarcomas. Clin Orthop Relat Res 467(8):2105–2111. doi:10.1007/s11999-008-0691-8
Donati D, Colangeli S, Colangeli M, Di Bella C, Bertoni F (2010) Surgical treatment of grade I central chondrosarcoma. Clin Orthop Relat Res 468(2):581–589. doi:10.1007/s11999-009-1056-7
Mohler DG, Chiu R, McCall DA, Avedian RS (2010) Curettage and cryosurgery for low-grade cartilage tumors is associated with low recurrence and high function. Clin Orthop Relat Res 468(10):2765–2773. doi:10.1007/s11999-010-1445-y
Souna BS, Belot N, Duval H, Langlais F, Thomazeau H (2010) No recurrences in selected patients after curettage with cryotherapy for grade I chondrosarcomas. Clin Orthop Relat Res 468(7):1956–1962. doi:10.1007/s11999-009-1211-1
Hickey M, Farrokhyar F, Deheshi B, Turcotte R, Ghert M (2011) A systematic review and meta-analysis of intralesional versus wide resection for intramedullary grade I chondrosarcoma of the extremities. Ann Surg Oncol 18(6):1705–1709. doi:10.1245/s10434-010-1532-z
Evans HL, Ayala AG, Romsdahl MM (1977) Prognostic factors in chondrosarcoma of bone: a clinicopathologic analysis with emphasis on histologic grading. Cancer 40(2):818–831
Fiorenza F, Abudu A, Grimer RJ, Carter SR, Tillman RM, Ayoub K, Mangham DC, Davies AM (2002) Risk factors for survival and local control in chondrosarcoma of bone. J Bone Joint Surg Br 84(1):93–99
Söderström M, Ekfors TO, Böhling TO, Teppo LH, Vuorio EI, Aro HT (2003) No improvement in the overall survival of 194 patients with chondrosarcoma in Finland in 1971–1990. Acta Orthop Scand 74(3):344–350
Pritchard DJ, Lunke RJ, Taylor WF, Dahlin DC, Medley BE (1980) Chondrosarcoma: a clinicopathologic and statistical analysis. Cancer 45(1):149–157
Eefting D, Schrage YM, Geirnaerdt MJ, Le Cessie S, Taminiau AH, Bovée JV, Hogendoorn PC (2009) Assessment of interobserver variability and histologic parameters to improve reliability in classification and grading of central cartilaginous tumors. Am J Surg Pathol 33(1):50–57
The skeletal lesions interobserver correlation among expert diagnosticians (SLICED) study group (2007) Reliability of histopathologic and radiologic grading of cartilaginous neoplasms in long bones. J Bone Joint Surg Am 89(10):2113–2123. doi:10.2106/JBJS.F.01530
Geirnaerdt MJ, Bloem JL, Eulderink F, Hogendoorn PC, Taminiau AH (1993) Cartilaginous tumors: correlation of gadolinium-enhanced MR imaging and histopathologic findings. Radiology 186(3):813–817
Geirnaerdt MJ, Hogendoorn PC, Bloem JL, Taminiau AH, van der Woude HJ (2000) Cartilaginous tumors: fast contrast-enhanced MR imaging. Radiology 214(2):539–546
De Beuckeleer LH, De Schepper AM, Ramon F, Somville J (1995) Magnetic resonance imaging of cartilaginous tumors: a retrospective study of 79 patients. Eur J Radiol 21(1):34–40
Murphey MD, Walker EA, Wilson AJ, Kransdorf MJ, Temple HT, Gannon FH (2003) From the archives of the AFIP: imaging of primary chondrosarcoma: radiologic-pathologic correlation. Radiographics 23(5):1245–1278
Yoo HJ, Hong SH, Choi JY, Moon KC, Kim HS, Choi JA, Kang HS (2009) Differentiating high-grade from low-grade chondrosarcoma with MR imaging. Eur Radiol 19(12):3008–3014. doi:10.1007/s00330-009-1493-4
Varma DG, Ayala AG, Carrasco CH, Guo SQ, Kumar R, Edeiken J (1992) Chondrosarcoma: MR imaging with pathologic correlation. Radiographics 12(4):687–704
Geirnaerdt MJ, Hermans J, Bloem JL, Kroon HM, Pope TL, Taminiau AH, Hogendoorn PC (1997) Usefulness of radiography in differentiating enchondroma from central grade 1 chondrosarcoma. AJR Am J Roentgenol 169(4):1097–1104
Ollivier L, Vanel D, Leclère J (2004) Imaging of chondrosarcomas. Cancer Imaging 4(1):36–38. doi:10.1102/1470-7330.2003.0022
Weiner SD (2004) Enchondroma and chondrosarcoma of bone: clinical, radiologic, and histologic differentiation. Instr Course Lect 53:645–649
Soldatos T, McCarthy EF, Attar S, Carrino JA, Fayad LM (2011) Imaging features of chondrosarcoma. J Comput Assist Tomogr 35(4):504–511
de Camargo OP, Baptista AM, Atanásio MJ, Waisberg DR (2010) Chondrosarcoma of bone: lessons from 46 operated cases in a single institution. Clin Orthop Relat Res 468(11):2969–2975. doi:10.1007/s11999-010-1368-7
Lodwick GS, Wilson AJ, Farrell C, Virtama P, Dittrich F (1980) Determining growth rates of focal lesions of bone from radiographs. Radiology 134(3):577–583
Freyschmidt J (1998) Standards and diagnostic strategies in diagnosis of bone tumors and tumor-simulating lesions [in German]. Radiologe 38(4):287–300
Takeuchi A, Yamamoto Y, Tsuneyama K, Cheng C, Yonekura H, Watanabe T, Shimizu K, Tomita K, Yamamoto H, Tsuchiya H (2007) Endogenous secretory receptor for advanced glycation end products as a novel prognostic marker in chondrosarcoma. Cancer 109(12):2532–2540. doi:10.1002/cncr.22731
Acknowledgments
We thank Jun Nakayama for evaluating the pathologic findings. We also thank Tominaga Shimizu and Tsutomu Akahane for their help in the clinical evaluation of the patients.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article
Cite this article
Yoshimura, Y., Isobe, Ki., Arai, H. et al. Preoperative radiographic and histopathologic evaluation of central chondrosarcoma. Arch Orthop Trauma Surg 133, 1225–1231 (2013). https://doi.org/10.1007/s00402-013-1800-z
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-013-1800-z