
Abstract
Background
Compression anastomotic ring-locking procedure (CARP) is a novel procedure for creating colonic anastomoses. The surgical procedure allows perioperative quantification of the compression pressure between the intestinal ends within the anastomosis and postoperative monitoring of the anastomotic integrity. We have recently shown that CARP is a safe and effective method for colonic anastomoses in pigs, and the purpose of the present study was to evaluate CARP for colonic anastomoses in humans.
Materials and methods
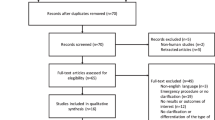
This is a prospective study on 25 patients undergoing elective left-sided colonic resection. Time for evacuation of the anastomotic rings, perioperative compression pressure, and adverse effects were recorded. Postoperative blood samples were collected daily, and flexible sigmoidoscopy was performed 8–12 weeks after surgery to examine the anastomoses.
Results
Fourteen out of 25 patients underwent CARP. CARP was not used in 11 patients due to advanced tumor disease (two cases) and size restrictions (nine cases). No case of anastomotic leakage, bowel obstruction, or stenosis formation was observed. No device-related perioperative adverse events were noted. The surgical device evacuated spontaneously in all patients by the natural route after a median of 10 days. Perioperative compression pressure ranged between 85 and 280 mBar (median 130 mBar). Flexible sigmoidoscopy revealed smooth anastomoses without signs of pathological inflammation or stenosis in all cases.
Conclusion
Our results indicate that the novel suture-less CARP is a safe and effective method for creating colonic anastomoses. Further studies are warranted in larger patient populations to compare CARP head-on-head with stapled and/or hand-sewn colonic anastomoses.





Similar content being viewed by others

References
Mirnezami A, Mirnezami R, Chandrakumaran K, Sasapu K, Sagar P, Finan P (2011) Increased local recurrence and reduced survival from colorectal cancer following anastomotic leak: systematic review and meta-analysis. Ann Surg 253(5):890–899
Law WL, Choi HK, Lee YM, Ho JW, Seto CL (2007) Anastomotic leakage is associated with poor long-term outcome in patients after curative colorectal resection for malignancy. J Gastrointest Surg 11(1):8–15
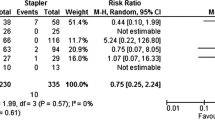
Neutzling CB, Lustosa SA, Proenca IM et al (2012) Stapled versus hand-sewn methods for colorectal anastomosis surgery. Cochrane Database Syst Rev 2:CD003144
Davis B, Rivadeneira DE (2013) Complications of colorectal anastomoses: leaks, strictures and bleeding. Surg Clin N Am 93(1):61–87
Ågren MS, Andersen T, Mirastschijski U, Syk I, Bruun S, Surve V, Lindebjerg J, Delaissé JM (2006) Action of matrix metalloproteinases at restricted sites in colon anastomosis repair: an immunohistochemical and biochemical study. Surgery 140:72–82
Zbar AP, Nir Y, Weizman A, Rabau M, Senagore A (2012) Compression anastomoses in colorectal surgery: a review. Tech Coloproctol 16(3):187–199
Ho YH, Ashour MA (2010) Techniques for colorectal anastomosis. World J Gastroenterol 16(13):1610–1621
Buchberg BS, Masoomi H, Bergman H, Mills SD, Stamos MJ (2011) The use of a compression device as an alternative to hand-sewn and stapled colorectal anastomoses: is three a crowd? J Gastrointest Surg 15(2):304–310
Kaidar-Person O, Rosenthal RJ, Wexner SD, Szomstein S, Person B (2008) Compression anastomosis: history and clinical consideration. Am J Surg 195(6):818–826
Aggarwal R, Darzi A (2005) Compression anastomoses revisited. J Am Coll Surg 201(6):965–971
Påhlman L, Ejerblad S, Graf W, Kader F, Kressner U, Lindmark G, Raab Y (1997) Randomized trial of a biofragmentable bowel anastomosis ring in high-risk colonic resection. Br J Surg 84(9):1291–1294
Chen S, Yang B, He JH, Zhang YC, Lai DM (2009) Randomized trial on the application of biofragmentable anastomosis ring in intestinal anastomosis. Chin Med J (Engl) 122(15):1755–1758
Forde KA, Godell KH, DellaBadia M (2006) A 10-year single-institutional study of the biofragmentable anastomosis ring. Am J Surg 191(4):483–487
Choi HJ, Kim HH, Jung GJ, Kim SS (1998) Intestinal anastomosis by use of the biofragmentable anastomotic ring: is it safe and efficacious in emergency operations as well? Dis Colon Rectum 41(10):1281–1286
Corman ML, Prager ED, Hardy TG Jr, Bubrick MP (1989) Comparison of the Valtrac biofragmentable anastomosis ring with conventional suture and stapled anastomosis in colon surgery. Result of a prospective, randomized clinical trial. Dis Colon Rectum 32(3):183–187
Kim SH, Choi HJ, Park KJ, Kim JM, Kim KH, Kim MC, Kim YH, Cho SH, Jung GJ (2005) Sutureless intestinal anastomosis with the biofragmentable anastomosis ring: experience of 632 anastomoses in a single institute. Dis Colon Rectum 48(11):2127–2132
Cahill CJ, Betzler M, Gruwez JA, Jeekel J, Patel JC, Zederfeldt B (1989) Sutureless large bowel anastomosis: European experience with the biofragmentable anastomosis ring. Br J Surg 76(4):344–347
Ghitulescu GA, Morin N, Jetty P, Belliveau P (2003) Revisiting the biofragmentable anastomotic ring: is it safe in colonic surgery? Can J Surg 46(2):92–98
Galizia G, Lieto E, Castellano P, Pelosio L, Imperatore V, Canfora F, Pignatelli C (1999) Comparison between the biofragmentable anastomosis ring and stapled anastomoses in the extraperitoneal rectum: a prospective, randomized study. Int J Color Dis 14(6):286–290
Nudelman IL, Fuko VV, Morgenstern S, Giler S, Lelcuk S (2000) Gastrointestinal anastomosis with the nickel-titanium double ring. World J Surg 24(7):874–877
Nudelman IL, Fuko V, Greif F, Lelcuk S (2002) Colonic anastomosis with the nickel-titanium temperature-dependent memory-shape device. Am J Surg 183(6):697–701
Nudelman I, Fuko V, Rubin M, Lelcuk S (2004) A nickel-titanium memory-shape device for colonic anastomosis in laparoscopic surgery. Surg Endosc 18(7):1085–1089
Nudelman I, Fuko V, Waserberg N, Niv Y, Rubin M, Szold A, Lelcuk S (2005) Colonic anastomosis performed with a memory-shaped device. Am J Surg 190(3):434–438
Avgoustou C, Penlidis P, Tsakpini A, Sioros C, Giannousis D (2012) Compression anastomoses in colon and rectal surgery with the NiTi ColonRingTM. Tech Coloproctol 16(1):29–35
Vilhjalmsson D, Olofsson P, Syk I, Thorlacius H, Grönberg A (2015) Compression anastomotic ring-locking procedure (CARP) is a novel technique for creating a suture-less colonic anastomosis. Eur Surg Res 54:139–147
Ricciardi R, Roberts PL, Marcello PW, Hall JF, Read TE, Schoetz DJ (2009) Anastomotic leak testing after colorectal resection. What are the data? Arch Surg 144(5):407–411
Welsch T, Müller SA, Ulrich A, Kischlat A, Hinz U, Kienle P, Büchler MW, Schmidt J, Schmied BM (2007) C-reactive protein as early predictor for infectious postoperative complications in rectal surgery. Int J Color Dis 22(12):1499–1507
Kørner H, Nielsen HJ, Søreide JA, Nedrebø BS, Søreide K, Knapp JC (2009) Diagnostic accuracy of C-reactive protein for intraabdominal infections after colorectal resections. J Gastrointest Surg 13(9):1599–1606
Acknowledgments
This work was supported by grants from the Swedish Medical Research Council (2012-3685), Crafoordska stiftelsen, Einar och Inga Nilssons stiftelse, Harald och Greta Jaenssons stiftelse, Greta och Johan Kocks stiftelser, Fröken Agnes Nilssons stiftelse, Franke och Margareta Bergqvists stiftelse för främjande av cancerforskning, Magnus Bergvalls stiftelse, Mossfelts stiftelse, Nanna Svartz stiftelse, Ruth och Richard Julins stiftelse, Svenska Läkaresällskapet, Allmänna sjukhusets i Malmö stiftelse för bekämpande av cancer, MAS fonder, Malmö University Hospital, and Lund University.
Conflict of interest
AG and HT are co-inventors of CARP, and both hold shares in CarpoNovum AB.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Vilhjalmsson, D., Appelros, S., Toth, E. et al. Compression anastomotic ring-locking procedure (CARP) is a safe and effective method for intestinal anastomoses following left-sided colonic resection. Int J Colorectal Dis 30, 969–975 (2015). https://doi.org/10.1007/s00384-015-2257-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-015-2257-z