
Abstract
Previous studies suggest that saturated fat (SFA) intake may negatively impact on bone. However, few human studies on the topic exist. Women and men aged 31–46 years from the Cardiovascular Risk in Young Finns study attended the peripheral quantitative computed tomography and ultrasound bone measurements in 2008 (n = 1884–1953, ~ 56% women). In addition, fracture diagnoses in 1980–2018 were searched for the national health care registers and 431 participants had at least one fracture. Food consumption was gathered with the 48-h dietary recall interviews and food frequency questionnaire in 1980–2007. In the present study, radial, tibial, and calcaneal bone traits, and fractures were examined relative to the long-term intake of SFA. No consistent associations were seen between bone outcomes and SFA intake that would have replicated in both women and men. The only evidence for differential distributions was seen in cortical density and cortical-to-total area ratio at the radial shaft, and speed of sound at the calcaneus, which were 0.1–0.4% higher in women in the lowest tertile of SFA intake compared with the highest tertile. In addition, among men, the odds ratio (OR) of fractures was greater in the second (OR 1.86, 95% confidence interval (CI) 1.03–3.33) and third tertile of SFA intake (OR 2.45, 95% CI 1.38–4.36) compared with the lowest tertile, independently of many risk factors of osteoporosis. In this observational study, we found no robust evidence of the associations of dietary long-term SFA intake with bone outcomes. Therefore, additional studies are needed to confirm the association of dietary SFA with bone health in humans.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A decrease in bone mineral density (BMD) and content (BMC), or a change in bone architecture, may subsequently lead to decreased bone strength and eventually also to osteoporosis [1]. A general diagnostic criterion of osteoporosis is defined as a BMD 2.5 standard deviation or more below the mean of young adult women. Osteoporotic bones break more likely than a healthy bone and may cause severe disability to their carrier including, for instance, pain and loss of independence. It is estimated that in the European Union, the annual number of incident fractures was approximately 3.5 million in 2010 and was estimated to rise to 4.5 million until the year 2025 [2].
There is an experimental evidence that dietary fats may affect bone tissue as, for instance, shown in a study conducted in mice where a diet including plenty of saturated fat was associated with lower total bone mineral mass and density [3]. These mice have probably been influenced by dyslipidemia which has shown to inhibit bone formation and increase bone resorption [4, 5]. The delivery of cholesterol to osteoclasts by low-density lipoprotein (LDL) increases osteoclast activity and formation; meanwhile, the efflux of cholesterol from osteoclasts to high-density lipoprotein (HDL) induces osteoclast apoptosis by suppressing intracellular signals and osteoclast fusion. Other factors in the cholesterol pathway mentioned regulating osteoclastogenesis were, for instance, estrogen-related receptor α, oxysterol, liver X receptors, and retinoid X receptors α and β [5]. Also, the growth and function of osteoblasts require LDL and other lipid particles as an energy source which acquisition and oxidation are regulated by several factors such as those related to the Wnt and parathyroid hormone signaling pathways [4].
Fatty acids, both endogenous and exogenous, may also connect with bone cells directly and thereby influence bone remodeling and structure [5, 6]. The effects of different fatty acids in targeted bone cells are mediated through several receptors in which fatty acids can attach and thereby influence internal signaling cascades such as osteoclast stimulating receptor activator of nuclear factor kappa-B ligand (RANKL) pathway [6]. In addition to bone cells, Bao et al. noted that fatty acids can also influence other properties of bone, such as calcium metabolism and bone collagen synthesis. In human cell studies, unsaturated fatty acids have been found to suppress the formation and activity of osteoclasts [7, 8]. In addition, the intakes of polyunsaturated fatty acids and fish have been found to be positively associated with BMD at the hip and lumbar spine and the lower risk of fractures mainly in older adults [9, 10]. Contrary to unsaturated fatty acids, saturated fatty acids (SFA), such as palmitic acid, have been noticed to enhance the formation and survival of murine osteoclasts and influence negatively on femoral cortical density [3, 11, 12]. In addition to enhanced bone resorption activity, SFA may also inhibit bone formation as shown earlier in vitro [13]. In the previous observational and case–control studies, SFA intake was found to be associated with lower BMD and increased risk of fractures at the hip [14,15,16,17]. However, the intake of saturated fat may also have some protective effect on femoral neck bone density as shown in a population-based study using the Healthy Eating Index based on Dietary Guidelines for Americans [18].
Associations of fatty acids and bone may also be related to the insulin-induced uptake of glucose and fatty acids in the bone marrow. Ojala et al. noticed that men with insulin resistance had the decreased uptake of fatty acids and glucose in bone marrows and lower bone turnover markers in plasma compared with controls [19]. Weivoda et al. revealed that dipeptidyl peptidase-4 secreted by osteoclasts might be a link between bone and energy metabolism as it blocks the effect of glucagon-like peptide-1 on the pancreas and thereby reduces the synthesis of insulin and its secretion to circulation [20]. In addition to unbalanced glucose homeostasis, impaired bone marrow metabolism has been found in conditions related to remarkable overweight and underweight [21]. In general, impaired bone marrow metabolism may lead to increased adiposity inside the bone which, on the other hand, seems to be inversely associated with BMD and in some studies related to the prevalence of vertebral fractures [21]. Previously, factors that have been found regulating the association of bone marrow adiposity and bone are, for instance, insulin-like growth factor-1 [22, 23], estrogen [24, 25], sclerostin [26, 27], and proinflammatory cytokines and adipokines [28, 29].
In general, the intake of SFA is above the recommendations in many western populations, such as those in Europe and North America, and therefore, it is important to study the associations of SFA with human health. In the present study population of adult women and men, we investigated the associations of dietary SFA with different bone phenotypes at calcaneus, tibia, and radius. We also studied whether SFA was associated with bone fractures in the present population. To our knowledge, no other previous study has as long follow-up data on saturated fat intake as here which allows us to study if the mean long-term intake of saturated fat accumulated between 1980 and 2007 will have an impact on bone outcomes studied.
Methods
Study Population and Bone Data
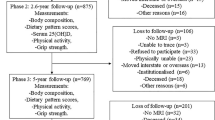
The Cardiovascular Risk in Young Finns Study (the Young Finns cohort) explores the contribution of childhood factors to the risk of diseases in adulthood [30]. In 1980, the first baseline study was carried out by the universities and university hospitals of Turku, Helsinki, Tampere, Kuopio, and Oulu (3–18-years, n = 3596). After this, there have been several follow-ups of which the latest was conducted in 2018–2020. The participation rate has varied from 83.2% at the first survey to around 60–80% at the later follow-ups. In 2008, persons in the register of the Young Finns cohort received an invitation to the peripheral quantitative computed tomography (pQCT) and quantitative ultrasound (QUS) bone measurements [31]. Altogether, 1884 participants aged 31–46-years (of which 56.2% women) from Turku, Helsinki, Tampere, Kuopio, and Oulu attended the pQCT measurements. The corresponding number of the QUS measurements was 1953 (56% women).
The non-weight-bearing radius and weight-bearing tibia were measured with the same pQCT measurement device in each study center (XCT 2000R, Stratec Medizintechnik GmbH, Pforzheim, Germany). In ~ 99.7% of the cases, radius was measured on the nonwriting hand and tibia on the left leg if no contraindication emerged. The lengths of ulna and tibia were measured with a tape measure and the measurement sections of the distal radius and tibia were defined as 4% and 5% from the distal cortical endplate, respectively. The diaphyseal sites were 30% for both studied bones. Finally, 1842–1856 radius and 1853–1857 tibia measurements were successfully scanned and analyzed in the distal and shaft parts of the bones, respectively (~ 98% of those who participated). Numbers for the successful ultrasound scans of the left heel were 1494–1515 (~ 77% of the participants).
Bone Geometrical Traits and Mineral Density
The analysis of bone density and geometrical traits from the pQCT scan images was done using specific threshold values and mode options according to the previously described standard procedures [32]. Analyses of the pQCT measurements yielded the following bone parameters: BMC (mg), trabecular and cortical bone mineral densities (mg/cm3), and total and cortical bone areas (mm2). Additionally, the following bone strength indices were calculated: stress–strain index (SSI, mm3) and cortical-to-total area ratio. SSI reflects the torsional strength of the bone diaphysis and is based on the density-weighted polar section modulus.
At the calcaneus, the speed of sound (SOS, m/s) and broadband ultrasound attenuation (BUA, dB/MHz) were measured with the QUS technique (Sahara Clinical Bone Sonometer, Hologic Inc., Waltham, MA, USA). The in vivo precision of the pQCT and QUS measurements evaluated in a subgroup (n = 39) varied between 0.3 and 4.8%.
Fractures
Primary and secondary fracture diagnosis codes of the skull, cervical vertebrae, ribs, sternum, thoracic vertebrae, lumbar vertebrae, pelvis, shoulder girdle, upper arm, forearm, carpal and metacarpal bones, phalanges of hand and foot, femur, patella, lower leg, and foot in 1980–2018 were searched for the national health care registers maintained by the Finnish Institute for Health and Welfare according to the International Classification of Diseases 9th and 10th revisions (ICD-9 and ICD-10) with the SPSS-software. In total, there were 431 participants with at least one registered fracture diagnosis.
Dietary Habits
At the baseline in 1980, dietary data were gathered with 48-h dietary recall interviews done by trained dietitians for around half of the study subjects (3–18 years, n = 1768). The interviews were repeated in 1986 and 2001 with participation rates of 59–68% [33]. This method gives detailed information on participants’ dietary habits during the two days prior to the interview. In 2007, information on food consumption and nutrient intake was collected with a modified 131- item food frequency questionnaire developed by the Finnish Institute for Health and Welfare [34]. In 1980 and 1986, the nutrient calculations were based on the Finnish food composition tables maintained by the University of Helsinki and analytical data were obtained from the local food industry. Later, 2001 and 2007, the nutrient contents of reported foods were calculated using the Finnish Food Composition database, Fineli® [35]. Dietary intakes of energy (kJ/day), carbohydrate (E%), fiber (g/day), protein (E%), total fat (E%), polyunsaturated fat (E%, g/day), monounsaturated fat (E%, g/day), calcium (mg/day), vitamin D (μg/day), and dairy products (g/day) were given as a mean intake/day or as an energy percentage of total energy intake. In addition, the intakes of dietary SFA (g/day) in 1980, 1986, 2001, and 2007 were combined as the mean long-term intake of SFA which was energy-adjusted using the residual method and divided into thirds by tertile classification for the further analyses.
Physical Activity
Three sum indices of physical activity collected with the questionnaires in 2007 and 2008 were used to describe the habitual physical activity of the participants and skeletal loadings [31, 36]. In 2007, the items of the physical activity index were the intensity of physical activity, frequency and duration of vigorous physical activity, the average duration of a physical activity session, and participation in organized exercise training. In 2008, the bone loading indices of radius and tibia were collected through the questions concerning the type of mechanical loading exerted on bone and calculated with the following equation for each type of mechanical loading: participant’s body weight (kg) × EL × I x ln (1 + F × D), where EL = exercise loading, I = intensity of exercise (ranging from 1 to 4, where 1 = no breathlessness at all and 4 = strong breathlessness and sweating), F = frequency of exercise (asked in two questions; how many months of the year and how often per month or week), and D = duration of exercise (ranging from 1 to 5, where 1 = under 20 min and 5 = more than 2 h). The total bone loading indices of radius and tibia combined each type of exercise loading which were high impacts (e.g., ball games, track and field events), strength training, repetitions (e.g., jogging, skiing), non-weight-bearing exercise (e.g., cycling, swimming), and work or recreational activities (e.g., working in the garden, construction work). In addition to leisure-time physical activity, physical load of work was estimated with questions regarding if a participant was in sedentary or manual work.
Clinical Measures
Body weight and height were measured, and body mass index (BMI, kg/m2) was calculated. Alcohol consumption was estimated from a self-administered questionnaire as the standard number of drinks per day. Smoking habits were defined as pack-years (the number of years a person has smoked one pack of cigarettes per day) and as a proportion of daily smokers (%). In addition, the use of oral corticosteroid medication for at least one month (yes/no) was gathered with the questionnaire.
Participants’ venous blood samples were drawn after an overnight fast and serum was separated for the biochemical analyses [30]. The levels of serum total cholesterol (mmol/l), high-density lipoprotein (HDL)-cholesterol (mmol/l), and glucose (mmol/l) were measured using enzymatic assays with an AU400-analyser (Olympus, Japan). Low-density lipoprotein (LDL)-cholesterol was estimated using the Friedewald formula in those with triglycerides < 4.0 mmol/l. In addition, due to changes in methods or kits between the years 2001 and 2007, the levels of glucose and insulin were corrected with the specific equations as described elsewhere [37]. Serum calcidiol concentrations (nmol/l) were determined using radioimmunoassay (DiaSorin, Stillwater, Minnesota).
Statistical Analyses
The analysis of variance, Brown–Forsythe, and Chi-square tests were chosen to compare the participant characteristics in the tertiles of dietary SFA intake after the tests of homogeneity of group variances. Analysis of covariance with the established risk factors of osteoporosis as covariates (age, height, weight, energy intake, serum calcidiol concentration, calcium intake, physical activity in leisure-time and work, and smoking) was then performed to study if the between-group differences in bone phenotypes measured with pQCT and QUS showed a dose-dependent association. The fracture frequencies across the tertiles of dietary SFA intake were tested with the Chi-square test. In addition, the adjusted odds ratios (ORs) of fractures and their 95% confidence intervals (95% CIs) in the tertiles of dietary SFA intake were calculated with binary logistic regression analysis (the lowest intake of SFA as the reference). All comparisons were performed with IBM SPSS Statistics 27 separately for women and men. To avoid possible multiple comparison bias, those associations that replicated in both males and females with P value less than 0.05 were interpreted as being supportive for the main hypothesis.
Results
Background Characteristics
Background characteristics of participating women and men within the tertiles of dietary SFA intake are shown in Tables 1 and 2, respectively. Women with the lowest intake of SFA (≤ 27.4 g/day) had 694 kJ higher energy intake per day compared with women in the highest tertile of SFA intake (P < 0.001, Table 1). In addition, their diet included more carbohydrates, fiber, calcium, vitamin D, milk, and sour-milk products compared with women in the two upper tertiles of SFA intake (P ≤ 0.04, Table 1). The intakes of fats in total, monounsaturated fats, and cheese were, on the contrary, higher among women in the upper tertiles of SFA intake compared with the lowest tertile (P < 0.001). Like the intake of dietary vitamin D, also serum calcidiol concentration was the highest among women in the lowest tertile of SFA intake (P < 0.001). In addition, there were also fewer daily smokers in the lowest tertile of SFA intake and their physical activity indices were higher compared with the upper tertiles of SFA intake (P ≤ 0.02, Table 1).
Men in the lowest tertile of SFA intake had lower body weight and body mass index compared with men in the upper tertiles of SFA intake (P ≤ 0.04, Table 2). In addition, the intakes of carbohydrate, fiber, and vitamin D as well as the calcidiol concentration were the highest among men in the lowest tertile of SFA intake (P ≤ 0.02). The intakes of energy, fats, calcium, and cheese were, on the contrary, the highest among men in the third tertile of SFA intake (P ≤ 0.01, Table 2). In addition, there were more men who smoked daily and had used corticosteroid medication for at least one month in the highest tertile of SFA intake (P ≤ 0.04). Men with higher SFA intake were also more frequently manual workers compared with men in the lowest tertile (P < 0.001). Physical activity indices were the highest in men with the lowest intake of SFA (P < 0.001, Table 2).
Dietary Saturated Fat and Bone Outcomes
In the radius, cortical density (mg/cm3) and cortical-to-total area ratio at the radial shaft differed significantly across the tertiles of SFA intake in women (P for trend ≤ 0.02, Table 3). Both cortical bone traits were 0.1–0.2% lower in women with the highest SFA intake compared with women with the lowest SFA intake (Table 3). No statistically significant differences were found in other radial traits or any trait in the tibia across the tertiles of SFA intake in either gender (Tables 3 and 4).
At the calcaneus, difference in SOS value (m/s) across the tertiles of SFA intake was statistically significant only in women (P = 0.04, Table 5). Women with the highest intake of SFA had 0.4% lower SOS value compared with women with the lowest SFA intake (Table 5).
In addition, there were 60, 75, and 87 men who had at least one fracture in the first, second, and third tertile of SFA intake, respectively (Table 6, χ2-test, P = 0.05). The most common fracture sites in the present population were shoulder area and upper arm, forearm, and lower leg (Table 6). Also, the adjusted odds ratio for having at least one fracture was increased in men in the second (OR 1.86, 95% CI 1.03–3.33, P = 0.04) and third tertile of SFA intake (OR 2.45, 95% CI 1.38–4.36, P = 0.002) compared with men with the lowest SFA intake. However, no significant association of fractures and SFA intake was found in women (ORs 1.10–1.25, 95% CI 0.59–2.28, P = 0.46–0.76).
Discussion
In the present population-based study, we found no consistent associations between SFA intake and bone health indicators. In the previous studies, saturated fat has been found to enhance bone resorption rather than bone formation and has an unfavorable impact on cortical density at the femur and the risk of hip fractures [3, 11,12,13,14,15,16,17,18]. Since few human studies are done on this topic previously, only tentative conclusions can be made of the associations of SFA and bone in humans. It may be, for instance, that the association of SFA and bone differs according to each bone phenotype or other factors may influence this association. In the present study, the dietary intake of vitamin D and physical activity indices were greater in both genders, and the frequency of daily smoking lower in the lowest tertile of SFA intake compared with those with higher SFA intake. In men, those in the highest tertile of SFA intake had also higher body weight and greater intake of calcium compared with the lowest tertile. In addition, in men, difference was seen in socioeconomic occupational status as those with higher SFA intake worked more frequently in manual work. In the previous studies of the Young Finns cohort, overweight [31, 38], the dietary intake of calcium and leisure-time physical activity [39,40,41], and exposure to passive smoke in childhood [42] have been found to be associated with different bone outcomes in the present population. Therefore, all these generally well-known risk factors of osteoporosis were included in the statistical model to exclude their possible confounding effect on the results. Also, other nutritional and clinical factors were considered as potential confounding factors between SFA intake and bone phenotypes but were not included in the model because of correlations with factors already existing in the model, or there was no adequate previous evidence of bone effect. For instance, the intake of protein correlated with total energy intake which was added to the final model. In addition, the differences in protein intake are clinically small although statistically significant in women. All the participants had also enough protein in their diets if compared with the national nutritional recommendation which is 10–20% of total energy intake. Greater differences were seen in the intakes of carbohydrate and fat, but as these energy nutrients are less studied relative to bone health, we decided not to add them to the final model.
The strength of the present study was that both a variety of bone phenotypes and fractures were drawn from a multi-center study including both women and men. In addition, lifestyle information on the Young Finns cohort has been gathered since 1980 which have yielded a longitudinal data, among other things, of dietary SFA intake. Although, two different dietary methods were used to study the intake of SFA over the study years, we assume that this has not considerably confounded the results as the mean intake of SFA was calculated and energy-adjusted and further divided into three equal-sized groups for the statistical comparisons. This should have given comparable information on the long-term SFA intake of the present cohort. There are, however, some shortcomings with the used dietary methods as the information gathered is self-reported. Thus, it is probable that reporting bias occurs as it may be difficult to recall all the foods and beverages that one has actually consumed. Some of the participants may therefore have exaggerated their eating habits, whereas others may have reported smaller portions of foods and beverages than usual. However, in general, underreporting and overreporting are common features, not only in nutrition research, but also in other areas of research that examine lifestyle habits in humans.
In addition, there may be some other reasons for small differences in bone phenotypes between the SFA tertiles of present population. Surprisingly, no differences were seen in blood cholesterol and glucose levels between the SFA groups which earlier have related to the function of bone cells and bone marrow metabolism [4, 5, 19]. In addition, it might be that the differences in the intake of dietary saturated fat were too small between the SFA tertiles that any remarkable differences in bone phenotypes could be detected. This explanation is supported by the fact that according to the latest national survey, most adult Finns consume more saturated fat than is recommended [43]. Thus, it may be difficult to find study participants who consume the recommendable amount of saturated fat. In men, the dietary intake of saturated fat was, however, associated with the incidence of all fractures occurred between 1980 and 2018. Men also had the greater intake of saturated fat compared with women which may partly explain why the association of SFA and fractures was found only in men. Fractures were gathered from the national health care registers and hence confirmed by the healthcare professionals in Finnish hospitals. In general, bone fractures have clinical and economic significance when considering the harm they cause to the individual and more broadly [44]. However, no association of dietary saturated fat and fractures was found in women, why further studies would be needed to confirm if these fractures really are associated with SFA intake or, for instance, with accidents at work and leisure-time activities. Specific reasons how the fractures occurred remain still uncertain as no information was available on this matter in registered data.
Conclusion
We did not find consistent associations between bone phenotypes and SFA intake that would have replicated in both men and women. Therefore, large clinical and prospective studies are needed to confirm if dietary SFA intake affects bone health in humans.
References
World Health Organization. (1994). Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: report of a WHO study group [meeting held in Rome from 22 to 25 June 1992]. World Health Organization. https://apps.who.int/iris/handle/10665/39142
Hernlund E, Svedbom A, Ivergård M, Compston J, Cooper C, Stenmark J, McCloskey EV, Jönsson B, Kanis JA (2013) Osteoporosis in the European Union: medical management, epidemiology and economic burden: a report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch Osteoporos 8:136. https://doi.org/10.1007/s11657-013-0136-1
Wang Y, Dellatore P, Douard V, Qin L, Watford M, Ferraris RP, Lin T, Shapses SA (2016) High fat diet enriched with saturated, but not monounsaturated fatty acids adversely affects femur, and both diets increase calcium absorption in older female mice. Nutr Res 36:742–750
Alekos NS, Moorer MC, Riddle RC (2020) Dual effects of lipid metabolism on osteoblast function. Front Endocrinol (Lausanne) 11:578194. https://doi.org/10.3389/fendo.2020.578194
Kim H, Oh B, Park-Min KH (2021) Regulation of osteoclast differentiation and activity by lipid metabolism. Cells 10:89. https://doi.org/10.3390/cells10010089
Bao M, Zhang K, Wei Y, Hua W, Gao Y, Li X, Ye L (2020) Therapeutic potentials and modulatory mechanisms of fatty acids in bone. Cell Prolif 53:e12735. https://doi.org/10.1111/cpr.12735
Kasonga AE, Deepak V, Kruger MC, Coetzee M (2015) Arachidonic acid and docosahexaenoic acid suppress osteoclast formation and activity in human CD14+ monocytes, in vitro. PLoS ONE 10:e0125145. https://doi.org/10.1371/journal.pone.0125145
Kasonga A, Kruger MC, Coetzee M (2019) Activation of PPARs modulates signalling pathways and expression of regulatory genes in osteoclasts derived from human CD14+ monocytes. Int J Mol Sci 20:1798. https://doi.org/10.3390/ijms20071798
Longo AB, Ward WE (2016) PUFAs, bone mineral density, and fragility fracture: findings from human studies. Adv Nutr 7:299–312
Lavado-García J, Roncero-Martin R, Moran JM, Pedrera-Canal M, Aliaga I, Leal-Hernandez O, Rico-Martin S, Canal-Macias ML (2018) Long-chain omega-3 polyunsaturated fatty acid dietary intake is positively associated with bone mineral density in normal and osteopenic Spanish women. PLoS ONE 13:e0190539. https://doi.org/10.1371/journal.pone.0190539
Oh SR, Sul OJ, Kim YY, Kim HJ, Yu R, Suh JH, Choi HS (2010) Saturated fatty acids enhance osteoclast survival. J Lipid Res 51:892–899
Drosatos-Tampakaki Z, Drosatos K, Siegelin Y, Gong S, Khan S, Van Dyke T, Goldberg IJ, Schulze PC, Schulze-Späte U (2014) Palmitic acid and DGAT1 deficiency enhance osteoclastogenesis, while oleic acid-induced triglyceride formation prevents it. J Bone Miner Res 29:1183–1195
Gunaratnam K, Vidal C, Boadle R, Thekkedam C, Duque G (2013) Mechanisms of palmitate-induced cell death in human osteoblasts. Biol Open 2:1382–1389
Corwin RL, Hartman TJ, Maczuga SA, Graubard BI (2006) Dietary saturated fat intake is inversely associated with bone density in humans: analysis of NHANES III. J Nutr 136:159–165
Orchard TS, Cauley JA, Frank GC, Neuhouser ML, Robinson JG, Snetselaar L, Tylavsky F, Wactawski-Wende J, Young AM, Lu B, Jackson RD (2010) Fatty acid consumption and risk of fracture in the Women’s Health Initiative. Am J Clin Nutr 92:1452–1460
Zeng FF, Xie HL, Fan F, Xue WQ, Wu BH, Zhu HL, Chen YM (2015) Association of dietary fat intake with the risk of hip fractures in an elderly Chinese population: a matched case-control study. Geriatr Gerontol Int 15:1171–1178
Mozaffari H, Djafarian K, Mofrad MD, Shab-Bidar S (2018) Dietary fat, saturated fatty acid, and monounsaturated fatty acid intakes and risk of bone fracture: a systematic review and meta-analysis of observational studies. Osteoporos Int 29:1949–1961
Fan Y, Ni S, Zhang H (2022) Association between Healthy Eating Index-2015 total and component food scores with osteoporosis in middle-aged and older Americans: a cross-sectional study with U.S. National Health and Nutrition Examination Survey. Osteoporos Int 33:921–929
Ojala R, Motiani KK, Ivaska KK, Arponen M, Eskelinen JJ, Virtanen KA, Löyttyniemi E, Heiskanen MA, U-Din M, Nuutila P, Kalliokoski KK, Hannukainen JC (2020) Bone marrow metabolism is impaired in insulin resistance and improves after exercise training. J Clin Endocrinol Metab 105:e4290–e4303
Weivoda MM, Chew CK, Monroe DG, Farr JN, Atkinson EJ, Geske JR, Eckhardt B, Thicke B, Ruan M, Tweed AJ, McCready LK, Rizza RA, Matveyenko A, Kassem M, Andersen TL, Vella A, Drake MT, Clarke BL, Oursler MJ, Khosla S (2020) Identification of osteoclast-osteoblast coupling factors in humans reveals links between bone and energy metabolism. Nat Commun 11:87. https://doi.org/10.1038/s41467-019-14003-6
Paccou J, Penel G, Chauveau C, Cortet B, Hardouin P (2019) Marrow adiposity and bone: review of clinical implications. Bone 118:8–15
Bredella MA, Torriani M, Ghomi RH, Thomas BJ, Brick DJ, Gerweck AV, Rosen CJ, Klibanski A, Miller KK (2011) Vertebral bone marrow fat is positively associated with visceral fat and inversely associated with IGF-1 in obese women. Obesity 19:49–53
Kim TY, Schwartz AV, Li X, Xu K, Black DM, Petrenko DM, Stewart L, Rogers SJ, Posselt AM, Carter JT, Shoback DM, Schafer AL (2017) Bone marrow fat changes after gastric bypass surgery are associated with loss of bone mass. J Bone Miner Res 32:2239–2247
Syed FA, Oursler MJ, Hefferanm TE, Peterson JM, Riggs BL, Khosla S (2008) Effects of estrogen therapy on bone marrow adipocytes in postmenopausal osteoporotic women. Osteoporos Int 19:1323–1330
Singhal V, Karzar NH, Bose A, Buckless C, Ackerman KE, Bredella MA, Klibanski A, Misra M (2021) Changes in marrow adipose tissue in relation to changes in bone parameters following estradiol replacement in adolescent and young adult females with functional hypothalamic amenorrhea. Bone 145:115841. https://doi.org/10.1016/j.bone.2021
Ma YH, Schwartz AV, Sigurdsson S, Hue TF, Lang TF, Harris TB, Rosen CJ, Vittinghoff E, Eiriksdottir G, Hauksdottir AM, Siggeirsdottir K, Sigurdsson G, Oskarsdottir D, Napoli N, Palermo L, Gudnason V, Li X (2014) Circulating sclerostin associated with vertebral bone marrow fat in older men but not women. J Clin Endocrinol Metab 99:E2584-2590. https://doi.org/10.1210/jc.2013-4493
Baroi S, Czernik PJ, Chougule A, Griffin PR, Lecka-Czernik B (2021) PPARG in osteocytes controls sclerostin expression, bone mass, marrow adiposity and mediates TZD-induced bone loss. Bone 147:115913. https://doi.org/10.1016/j.bone.2021.115913
Pino AM, Ríos S, Astudillo P, Fernández M, Figueroa P, Seitz G, Rodríguez JP (2010) Concentration of adipogenic and proinflammatory cytokines in the bone marrow supernatant fluid of osteoporotic women. J Bone Miner Res 25:492–498
Scheller EL, Burr AA, MacDougald OA, Cawthorn WP (2016) Inside out: Bone marrow adipose tissue as a source of circulating adiponectin. Adipocyte 5:251–269
Raitakari OT, Juonala M, Rönnemaa T, Keltikangas-Järvinen L, Räsänen L, Pietikäinen M, Hutri-Kähönen N, Taittonen L, Jokinen E, Marniemi J, Jula A, Telama R, Kähönen M, Lehtimäki T, Åkerblom HK, Viikari JS (2008) Cohort profile: the Cardiovascular Risk in Young Finns Study. Int J Epidemiol 37:1220–1226
Laaksonen MML, Sievänen H, Tolonen S, Mikkilä V, Räsänen L, Viikari J, Lehtimäki T, Kähönen M, Raitakari OT (2010) The Cardiovascular Risk in Young Finns Study Group: determinants of bone strength and fracture incidence in adult Finns: Cardiovascular Risk in Young Finns Study (the GENDI pQCT study). Arch Osteoporos 5:119–130
Sievänen H, Koskue V, Rauhio A, Kannus P, Heinonen A, Vuori I (1998) Peripheral quantitative computed tomography in human long bones: evaluation of in vitro and in vivo precision. J Bone Miner Res 13:871–882
Mikkilä V, Räsänen L, Raitakari OT, Pietinen P, Viikari J (2005) Consistent dietary patterns identified from childhood to adulthood: the Cardiovascular Risk in Young Finns Study. Br J Nutr 93:923–931
Paalanen L, Männistö S, Virtanen MJ, Knekt P, Räsänen L, Montonen J, Pietinen P (2006) Validity of a food frequency questionnaire varied by age and body mass index. J Clin Epidemiol 59:994–1001
Finnish Institute for Health and Welfare, Public Health Promotion Unit. Fineli. Finnish food composition database. Release 10. Helsinki 2009. www.fineli.fi.
Telama R, Yang X, Leskinen E, Kankaanpää A, Hirvensalo M, Tammelin T, Viikari JS, Raitakari OT (2014) Tracking of physical activity from early childhood through youth into adulthood. Med Sci Sports Exerc 46:955–962
Raiko JR, Viikari JS, Ilmanen A, Hutri-Kähönen N, Taittonen L, Jokinen E, Pietikäinen M, Jula A, Loo BM, Marniemi J, Lehtimäki T, Kähönen M, Rönnemaa T, Raitakari OT, Juonala M (2010) Follow-ups of the Cardiovascular Risk in Young Finns Study in 2001 and 2007: levels and 6-year changes in risk factors. J Intern Med 267:370–384
Uusi-Rasi K, Laaksonen M, Mikkilä V, Tolonen S, Raitakari OT, Viikari J, Lehtimäki T, Kähönen M, Sievänen H (2012) Overweight in childhood and bone density and size in adulthood. Osteoporos Int 23:1453–1461
Tolonen S, Laaksonen M, Mikkilä V, Sievänen H, Mononen N, Räsänen L, Viikari J, Raitakari OT, Kähönen M, Lehtimäki TJ (2011) Cardiovascular Risk in Young Finns Study Group: lactase gene c/t(-13910) polymorphism, calcium intake, and pQCT bone traits in Finnish adults. Calcif Tissue Int 88:153–161
Tolonen S, Sievänen H, Mikkilä V, Telama R, Oikonen M, Laaksonen M, Viikari J, Kähönen M, Raitakari OT (2015) Adolescence physical activity is associated with higher tibial pQCT bone values in adulthood after 28-years of follow-up-the Cardiovascular Risk in Young Finns Study. Bone 75:77–83
Tolonen S, Sievänen H, Hirvensalo M, Laaksonen M, Mikkilä V, Pälve K, Lehtimäki T, Raitakari O, Kähönen M (2018) Higher step count is associated with greater bone mass and strength in women but not in men. Arch Osteoporos 13:20. https://doi.org/10.1007/s11657-018-0425-9
Juonala M, Pitkänen N, Tolonen S, Laaksonen M, Sievänen H, Jokinen E, Laitinen T, Sabin MA, Hutri-Kähönen N, Lehtimäki T, Taittonen L, Jula A, Loo BM, Impivaara O, Kähönen M, Magnussen CG, Viikari JSA, Raitakari OT (2019) Childhood exposure to passive smoking and bone health in adulthood: the Cardiovascular Risk in Young Finns Study. J Clin Endocrinol Metab 104:2403–2411
Valsta L, Kaartinen N, Tapanainen H, Männistö S ja Sääksjärvi K, (eds.) (2018) Ravitsemus Suomessa—FinRavinto 2017—tutkimus [Nutrition in Finland—The National FinDiet 2017 Survey]. Institute for Health and Welfare (THL). Report 12/2018, 239 pages. Helsinki, Finland. ISBN 978–952–343–238–3 (online publication).
Kanis JA, Norton N, Harvey NC, Jacobson T, Johansson H, Lorentzon M, McCloskey EV, Willers C, Borgström F (2021) SCOPE 2021: a new scorecard for osteoporosis in Europe. Arch Osteoporos 16:82
Acknowledgements
Finally, we would like to thank the participants of the Young Finns cohort that made the study possible. We also appreciate all those that have worked in the Cardiovascular Risk in Young Finns Study over the study years. This work was financially supported by a grant from the Juho Vainio Foundation.
Funding
Open Access funding provided by University of Turku (UTU) including Turku University Central Hospital.
Author information
Authors and Affiliations
Contributions
Material preparation and data collection were performed by Sanna Tolonen, Markus Juonala, Marika Laaksonen, Harri Sievänen, Mika Kähönen, Jorma Viikari, and Olli Raitakari. Sanna Tolonen was responsible for the statistical data analysis and prepared the first draft of the manuscript. All authors revised the paper critically for intellectual content and approved the final version.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare they have no relevant financial or non-financial interests to disclose.
Human and Animal Rights
This study was performed in line with the principles of the Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects and was approved by the local ethics committees of the participating universities.
Informed Consent
Written informed consent was obtained from all participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tolonen, S., Juonala, M., Fogelholm, M. et al. Dietary Saturated Fat and Bone Health in Young Adults: The Young Finns Cohort. Calcif Tissue Int 111, 419–429 (2022). https://doi.org/10.1007/s00223-022-01008-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00223-022-01008-5