
Abstract
Introduction and hypothesis
We evaluated a pilot multi-component reintegration intervention to improve women’s physical and psychosocial quality of life after genital fistula surgery.
Methods
Twelve women undergoing fistula repair at Mulago Specialized Women and Neonatal Hospital (Kampala, Uganda) anticipated in a 2-week multi-component intervention including health education, psychosocial therapy, physiotherapy, and economic investment. We assessed feasibility through recruitment, retention, and adherence, acceptability through intervention satisfaction, and preliminary effectiveness through reintegration, mental health, physical health, and economic status. We collected quantitative data at enrollment, 6 weeks, 3 months, and 6 months. We conducted in-depth interviews with six participants. Quantitative data are presented descriptively, and qualitative data analyzed thematically.
Results
Participants had a median age of 34.5 years (25.5–38.0), 50% were married/partnered, 42% were separated, 50$ had completed less than primary education, and 67% were unemployed. Mean number of sessions received was 12 for health education (range 5–15), 8 for counseling (range 8–9), and 6 for physiotherapy (range 4–8). Feasibility was demonstrated by study acceptance among all those eligible (100%); comfort with study measures, data collection frequency and approach; and procedural fidelity. Acceptability was high; all participants reported being very satisfied with the intervention and each of the components. Participant narratives echoed quantitative findings and contributed nuanced perspectives to understanding approach and content.
Conclusions
Our results suggest that the intervention and associated research were both feasible and acceptable, and suggested certain modifications to the intervention protocol to reduce participant burden. Further research to determine the effectiveness of the intervention above and beyond surgery alone with regard to the health and well-being of women with fistulas is warranted.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Female genital fistula is a debilitating birth injury affecting an estimated 500,000 women, mostly in sub-Saharan Africa [1, 2]. Primarily due to prolonged obstructed labor combined with a lack of high-quality emergency obstetric care access or iatrogenic etiologies, up to 100,000 new cases occur each year globally. In Uganda, 1.4% of women of reproductive age (regional range 0.5% to 4.3%) report having experienced female genital fistula symptoms in their lifetime and approximately 1,900 new cases occur per year [3].
Fistula is associated with significant physical, psychosocial, and economic consequences. Physical symptoms include uncontrollable urine and/or fecal leakage and associated odors, pain, weakness, and mobility impairments [4,5,6,7]. Fistula-causing births have high stillbirth rates [8]. Women with fistula are often stigmatized, unable to participate in social, economic, or religious activities [6, 8] and report high psychiatric morbidity [9,10,11]. Surgery is often transformative; however, persistent post-repair symptoms may substantially lower psychosocial health [12, 13]. These factors limit women’s ability to resume their previous roles despite successful surgery, particularly in conjunction with economic hardship [14].
Owing to the significant physical and psychological disabilities that women with fistula experience, targeted rehabilitation efforts may substantially impact recovery and quality of life. Despite the need and recognition that holistic approaches to fistula care may improve recovery, most fistula services incorporate little complementary or follow-up care [15,16,17,18]. Few studies report on the development and implementation of holistic fistula care or on the effectiveness of interventions provided as an adjunct to fistula surgical care, leaving a knowledge and practice gap [13, 19]. Studies from Nigeria, Eritrea, and Tanzania support short-term facility-based psychological intervention for improving mental health [20,21,22,23], and evidence from the Democratic Republic of the Congo and Benin supports health education and physiotherapy for improved pelvic floor strength and reducing post-repair incontinence [24,25,26,27]. Economic empowerment lacks robust evidence, yet is theoretically and anecdotally considered an important adjunct to fistula programming [13, 28] and is a primary focus of social programming outside of health care settings.
Our study sought to address the gap in evidence-based practice for reintegration following female genital fistula surgery through the development and pilot test of a multi-component intervention including health education, psychosocial counseling, physiotherapy, and economic empowerment. Intervention domains and delivery structure were informed by existing evidence and our team’s experience in surgical fistula care and research on optimizing recovery from female genital fistula surgery [29]. The objectives of this pilot study were to assess the feasibility and acceptability of the multi-component reintegration intervention in conjunction with fistula surgery in a Ugandan referral hospital and to explore its preliminary effectiveness on women’s physical and psychosocial quality of life.
Materials and Methods
Study Design and Site
We employed a quasi-experimental (pre/post) mixed-methods design to assess feasibility and acceptability, and to explore the preliminary effectiveness of a multi-component reintegration intervention among women accessing care for female genital fistula at Mulago Specialised Women and Neonatal Hospital in Kampala, Uganda.
Study Participants
Eligibility criteria included being confirmed for urogenital fistula surgery, age 18 or above (or emancipated minor), and able to provide consent to study participation. Twelve study participants were enrolled in our study between October 2021 and February 2022. We invited a nested sub-sample of six study participants for in-depth interviews between December 2021 and March 2022 to understand their experience participating in the intervention and its impact. Quantitative and qualitative sample sizes were based on feasibility.
Study Procedures
Participant Recruitment and Enrollment
Potential participants were identified through surgical registry review and discussion with fistula care providers. After screening for eligibility, the research team described the study goals and procedures, ensured understanding of study procedures and risks, and ascertained women’s interest in participating. Written confirmation of informed consent was obtained from all study participants.
Intervention
Standard fistula surgical care at Mulago Hospital includes a 2-week post-surgical hospitalization during which patients receive unstructured health education and counseling on post-repair behaviors, including instruction on pelvic floor muscle strengthening exercises. Women with significant psychiatric or physiotherapy needs are referred to specialist care.
Our pilot intervention targeted four domains to support women to overcome the physical, psychological, and economic consequences of fistula: health education, psychosocial therapy, physiotherapy, and economic empowerment (Table 1; detailed schedule in Table S1, session objectives outlined in Appendix 1). These components were selected because of their importance in the fistula literature [12, 13]. Intervention activities were planned for ~75 min per day for small group delivery (e.g., 4–8 participants). Health education sessions (n = 15) delivered by nurse-midwives communicated comprehensive information about the development, treatment, and rehabilitation of fistula, contraception, and birth planning for subsequent deliveries, identification of obstetric emergencies, and nutrition. Psychosocial counseling sessions (n = 8) delivered by a social worker sought to help women to reframe their fistula experience and prepare for returning home by developing plans for positive coping and social support development. Physiotherapy sessions delivered by physiotherapists comprised evaluation (pre-surgery, pre-discharge, and at 6 weeks following surgery) and a sequential series of facilitated exercises focused on recovering mobility, balance, and strength, and building and maintaining pelvic floor musculature (daily). Economic empowerment included a short financial literacy session by the social worker and provision of 525,000 Ugandan Shillings (equivalent to US$ 150) in investment funding.
Data Collection
Mixed-methods data on intervention implementation was captured through process tracking, discussions with intervention implementers, and observation. Quantitative data were collected at enrollment (prior to fistula surgery), hospital discharge (14 days following surgery), and 6 weeks, 3 months, and 6 months following fistula repair surgery. Participants were provided with phones and monthly airtime to facilitate study communication and for remote follow-up data collection at 3 and 6 months. Qualitative data were collected between 3 and 6 months following surgery.
Study Measures
Our primary study outcomes were feasibility and acceptability. Intervention feasibility was assessed through recruitment, retention, and fidelity/adherence. Intervention acceptability was assessed quantitatively through participant satisfaction with the intervention overall and with each intervention component using a five-point Likert-type scale. Qualitative acceptability assessment included open-ended questions on participant experiences and perspectives with the intervention overall, and with each intervention component, including perspectives on appropriateness (perspectives on fit and relevance of the innovation to the patient, problem, and setting) [42, 43]. Quantitative feasibility and mixed-methods acceptability assessment were supplemented by discussions with intervention moderators regarding challenges and adaptations required to the original intervention plan.
Preliminary effectiveness assessment was based on participant self-reported reintegration as a primary outcome [12], and secondary outcomes: physical health (incontinence [44] and level of disability [45]), mental health (i.e., depression [46], and a one-item self-esteem measure), economic stability (i.e., earnings and food security), empowerment (measured through input into household decision-making across varied domains), and stigma (enacted and internalized). Most measures were collected at each time point; however, to reduce participant burden, incontinence was assessed at baseline and at 6 weeks only, and stigma at baseline and at 6 months only. Outcome assessment was implemented at 6 months owing to our study timeframe and because this is the time point at which prior research has identified reducing gains over time [13]. Qualitative assessment included participant perspectives of intervention effectiveness.
Covariates captured and used to describe the study sample included sociodemographic characteristics (age, education, marriage/partnership status, labor force participation, income, and wealth) and duration of time with fistula), all collected at baseline.
Data Analysis
Quantitative data on feasibility, acceptability, and preliminary effectiveness were descriptively analyzed using medians and standard deviations, medians and inter-quartile ranges, and proportions—per variable distribution. We explored trends over time using mixed-effects linear and logistic regression models, accounting for within-person clustering. Qualitative data were analyzed thematically across intervention and research components using an implementation science orientation focused on content, approach, acceptability, appropriateness, and feasibility [42]. A codebook was developed iteratively including deductive codes from our framework and interview guide and inductive codes emerging organically from the data. The codebook included a detailed description of each code, inclusion and exclusion criteria, and examples of the code in use. Transcripts were coded by three research team members a Ugandan researcher and qualitative interviewer (HN), an American mixed-methods researcher (AE) and an American Master of Public Health Student (SA). Coded data were analyzed thematically to understand participant experiences and perspectives across intervention components, and major findings and interpretation were reviewed by the co-author team. Change in economic status over time was analyzed through review of mixed-methods data.
Results
Study Participants
Study participants had a median age of 34.5 years (IQR 24.5–38.0; Table S2). Half had not completed primary education (6 out of 12; 50%) and half were married or in a domestic partnership (6 out of 12, 50%). Many were not employed (5 out of 12, 42%) and median monthly income was 0 (IQR 0–95,000 Ush, ~US$ 25). None had health insurance. Time with fistula varied substantially across the sample, ranging from 1 month to 23 years.
Intervention Feasibility
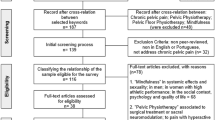
The pilot reintegration intervention was considered feasible. Recruitment and retention were successful despite fewer patients seeking fistula care during the COVID-19 pandemic. Among 13 eligible individuals, 12 agreed to participate. One declined participation owing to concerns with follow-up data collection. All 12 participants were retained throughout the 6-month study.
Intervention fidelity was good, with most but not all intended sessions received. The mean number of sessions attended by intervention component was 12 for health education (range 5–15), 8 for counseling (range 8–9), and 6 for physiotherapy (range 4–8). All participants received the economic incentive. Few family members attended the final counseling session on fistula prevention and management.
Data collection, including outcome measurement, was feasible and question comprehension was good. Participants reported that the interviews were not burdensome, with only 1 suggesting shortening the quantitative survey.
Study intervention implementation was largely feasible. Participants were generally ready to engage per plan; however, a few participants preferred to postpone physiotherapy exercises for the first few days following surgery. Some counseling topics were difficult to engage with owing to their sensitive nature; however, participants reported feeling supported to discuss challenging topics. Some participants suggested that fewer sessions would be easier.
Intervention Acceptability
Acceptability of the intervention to patients was high overall. All participants reported being very satisfied with the intervention (12 out of 12) and that each of the components were very useful (12 out of 12, for each component). Intervention moderators reported high acceptability in team discussions. Participant perspectives on the content, approach, satisfaction, appropriateness, and suggestions for each of the four components are described below, with selected quotations in Table 2.
Health Education
Study participants generally reported understanding the health education content well and recalled key content areas such as how a fistula occurs and primary discharge instructions (e.g., delaying post-repair sexual intercourse, avoiding heavy work, drinking enough water, eating healthily, and doing exercises). Participants also reported being counseled on postponing post-repair pregnancy and the importance of cesarean section for subsequent births. One participant reported some difficulty with understanding the cause of their fistula, and 2 participants particularly appreciated the family planning information given their lack of prior knowledge. Participants reported that the educational content was very useful for them, met their needs, and was understandable, and thus was considered appropriate. Participants generally appreciated the approaches used within the health education sessions. One participant specifically mentioned enjoying the handouts shared by the moderators. Most participants preferred group versus individual sessions owing to the social support provided by individuals with the same problem; however, one participant who had participated individually voiced potential confidentiality concerns with a group format.
Counseling
Participants felt that counseling covered important topics for overcoming fistula-related challenges. The counseling content was useful for them, motivated them, and met their needs (appropriateness). Some participants preferred the group counseling approach whereas others preferred individual counseling. Participants who preferred group counseling believed that the group facilitated greater learning. Participants who preferred individual counseling prioritized confidentiality. Overall, participants were satisfied with counseling. They expressed being comforted during counseling and trusted the counselor.
Physiotherapy
Participants appreciated the physiotherapy content, including exercise training. The physiotherapy was considered helpful and appropriate for fistula patients, and participants appreciated physical improvements after initiating physiotherapy, with some respondents also noting stress relief. Some participants, mainly those who underwent abdominal surgery, reported that certain exercises were painful, particularly early after surgery. Some suggested that physiotherapy exercises might be delayed by a few days or weeks to minimize the pain and allow the surgical wound to heal.
Preferred physiotherapy session mode (approach) varied, with some participants preferring individual sessions and others preferring group sessions. Some respondents feared being made fun of doing exercises, exposing their private parts, or failing to do some exercises. Others preferred group sessions for social support and encouragement.
All respondents expressed satisfaction with the exercises mainly because they believed that they helped them heal faster. However, certain exercises were more painful or difficult. Many respondents reported continuing the physiotherapy exercises beyond their hospital stay for fistula repair in order to heal. Some participants failed to continue with the exercises at home, simply because they forgot the exercises that they were meant to do, and a few missed getting discharge cards describing the different exercises.
Economic Incentive
All participants appreciated and were satisfied with the economic incentive they received as a start-up fund, and most did not expect it. Most started small businesses and reported that the amount given to them ($150) was adequate. Some participants suggested adding vocational skills training (e.g., hairdressing or baking). Most preferred money versus vocational skills training as it did not guarantee employment, whereas money met immediate family needs. Others suggested adding follow-up via phone or visits to check on business progress and well-being.
The small businesses included roadside food stalls, general trading, animal rearing or farming, and crafts. They focused on a range of commodities including charcoal, rice, and groundnuts, coffee beans, pigs, silverfish, chicken, and clothing. One participant reported investing in a popcorn machine and now makes and sells popcorn. Another participant brewed and sold alcohol. Two participants described using the funds to support other family members or household expenses such as school fees, rent, clinical care, or family funeral expenses. One participant stayed with family post-surgically and saved the money to start a restaurant after she returned home.
Research
Participants found the research approach acceptable. Some participants perceived the survey as short, whereas others noted that it was long; however, participants reported no difficulty with the questionnaire and interview length or returning to the health facility for follow-up data collection. They appreciated facilitation of their return transportation for data collection.
Preliminary Effectiveness
Reintegration score was mean 34.1 (SD 8.1) at baseline and increased to 65.4 (SD 6.9) at 6 months post-surgery. This increase represented a statistically significant trend over time, with the mean monthly increase of 4.4 points (95% CI 3.01–5.90). Secondary outcomes also suggested improving trends. For example, the mean disability score was 15.7 (6.0) at baseline and reduced to 1.8 (2.2) at 6 months post-surgery (mean 2.1-point decrease each month, 95% CI −2.79, −1.36). Mean depressive symptoms were 12.9 (SD 5.0) at baseline and reduced to 2.4 (SD 3.2) at 6 months post-surgery (mean 1.4-point per month reduction, 95% CI −2.04, −0.79). Mean self-esteem increased from 2.3 (SD 1.1) at baseline to 4.5 (SD 0.9) at 6 months, reflecting significant improvement.
At baseline, all participants were leaking urine (n = 12, 100%); at 6 weeks post-surgery, only 1 person (8.3%) reported ongoing urine leakage (not shown). Median impact of urine leakage interference on everyday life reduced from the scale maximum of 10 (IQR 9–10) at baseline to the scale minimum of 0 (IQR 0–0) at 6 weeks. Respondent input into household decision making exhibited little change over time, except for food crop and livestock farming (80% to 86% from baseline to 6-month follow-up, p = 0.006) and nonfarming economic activities (75% to 100%, marginal p = 0.091).
We observed important reductions in stigma experiences and increases in social support. From baseline to 6 months, enacted stigma reporting decreased from 6 to 2, reporting being treated differently than before fistula, 5 to 1 reporting being treated badly, and 6 to 1 reporting abandonment owing to the fistula. Internalized stigma reduced from 9 at baseline to 2 at follow-up, and similar numbers reported choosing to avoid others or join social activities owing to the fistula (6 to 1). Over the study follow-up, consistency in emotional support increased from 6 to 10 and informational support increased from 4 to 7, yet tangible support decreased from 6 to 5 (Table 3).
Changes in living status, relationship status, individual financial status, and household financial status over the study period are described in Table 4. Change in living status was reported by most participants at 6 weeks (8 out of 12) and 3 months (8 out of 12) post-surgery, most of which was positive and focused on stigma reduction; fewer participants endorsed changes in relationship status, yet comments in this domain were similarly focused on stigma reduction. Most participants reported positive changes in individual employment, income, savings, and debt at 3 (8 out of 12) and 6 months (10 out of 12), and positive household changes reported largely reflected changes in individual income.
Within 3 months of receiving the incentive, participants created small businesses (see acceptability), saved the money, used it for household essentials, or paid debt and taxes. By 6 months, many participants were involved in income-generating activities. Assets did not change over time but investments improved household income and savings. Some participants experienced an improvement in the quality of their living environment. They expressed better living conditions such as sleeping well in clean beds, working, and buying what they needed.
Discussion
Establishing feasibility and acceptability of an intervention and the surrounding research are key foundational components required before moving forward with robust assessment of intervention effectiveness. We found that a multi-component fistula reintegration intervention incorporating health education, psychosocial counseling, physiotherapy, and an economic incentive delivered within a public Ugandan referral hospital setting at the time of fistula surgery was demonstrated to be feasible and acceptable to both implementers and recipients. Furthermore, the research structure around the intervention for assessing effectiveness was also considered feasible and acceptable to implementers and participants. Research findings informed important adjustments to the original intervention protocol to reduce participant burden and improve engagement. Our research contributes to the limited evidence based on holistic fistula care, which supports the need for reintegration programming addressing the unique physical, psychosocial, and economic needs of women recovering from a fistula and fistula surgery [2].
Implementing fistula care has its own unique challenges, which are structured by the relatively low incidence but broad geographic distribution of patients, the constellation of physical and social sequelae experienced by individuals with the condition, in conjunction with traditionally siloed care models for these needs, the low socioeconomic status and health literacy of this population, and the lower-resource settings in which a fistula more commonly occurs. These challenges, relevant to both fistula surgery and reintegration programming, were considered by our research team and have similarly influenced the scope of other reintegration interventions reported in the literature. Other programs providing reintegration support have tested health education, psychosocial counseling, physical rehabilitation, social immersion, and livelihood improvement, alone or paired—and largely at the fistula repair facility [13, 47, 48].
We sought to be comprehensive in our reintegration programming approach through addressing physical and psychosocial health and economic status, employing group delivery strategies to capitalize on shared experiences and build social support, extending certain sessions to family members to strengthen community-based support, and providing an economic incentive for women to use as they desired; however, certain limitations to our design should be explored in future research and implementation. Optimal reintegration programming should extend facility-based services to community settings given the important role of the unique community environments of each individual to accommodate their individual needs, and facilitators and barriers to reintegration, which include social support networks and resources. We implemented our intervention within the fistula surgical facility to exploit the 2-week facility-based recovery period and because of service provision challenges across large distances. Building community networks and programming within this model was not possible within the scope of our small grant mechanism, but a systems approach should be prioritized for country-level reintegration program developers and implementers. Broad engagement of community health workers has been feasible within the Fistula Foundation’s Fistula Treatment Network in Kenya for surgical mobilization and follow-up [47], and other models for expanding care continuity through existing community-based services are needed. Finally, most existing reintegration programming supporting economic stability offers vocational training, with or without added financial support; owing to the referral-facility base of our intervention and geographic diversity of participant residence, we chose not to coordinate further vocational programming. This design increased implementation feasibility within our clinical setting, but further consideration should be given to connecting women with existing vocational training programs as needed to improve economic status.
Our preliminary effectiveness results identified improving trends across time within key domains of interest; however, our pilot study was not designed to test the effectiveness of the reintegration intervention components separately from the impact of fistula surgery, which we know has significant impact on improving women’s physical and psychosocial health [49, 50]. The findings of the current research confirm that the research structure around our intervention is both appropriate and feasible, but cannot be considered evidence of intervention effectiveness.
Key limitations to this study include our implementation within one site, small sample size, and lack of a comparison group; although appropriate for a pilot study such as ours, these factors did not allow us to explore feasibility and acceptability differences across diverse settings and populations and limited our ability to formally assess intervention effectiveness. Pilot study implementation and data collection occurred during the COVID-19 pandemic. Local mitigation measures included travel restrictions, reduced medical capacity, and limitations on elective surgery provision, which influenced our ability to implement this study as planned. Finally, although our study evaluated outcomes at 6 months, which is the time point at which prior longitudinal research has identified reducing physical and psychosocial gains, a longer evaluation period may be more appropriate to fully capture this impact, as well as any economic impact [13].
Conclusion
Holistic approaches to genital fistula programming are important for supporting women to overcome the significant physical and psychological disabilities associated with this condition in conjunction with surgery, yet the evidence base is limited. Our facility-based multi-component intervention, built on prior literature, theory, and field experience, was found to be both feasible and acceptable within pilot research. Further research to determine the effectiveness of this intervention above and beyond surgery on the health and well-being of women with fistulas is warranted. Future research should employ study designs capable of evaluating the value added of reintegration components on key fistula outcomes. Quality of research design and reporting has been limited for many fistula interventions [2, 13], and integrating robust research structures with ongoing and new reintegration programming is an important strategy for improving the quality of this evidence base so that others can learn from this body of literature, including attention to implementation considerations such as human resources and costs, to meet the needs of policy makers and program leadership, and ultimately improve women’s recovery from fistula.
Data Availability
De-identified data are available from the corresponding author on request.
References
United Nations General Assembly. Intensifying efforts to end obstetric fistula within a decade. Report of the secretary-general. A/75/264. New York, NY: United Nations, 2020.
UNFPA. Obstetric fistula & other forms of female genital fistula: guiding principles for clinical management and programme development. New York, NY: UNFPA, 2021.
Ministry of Health Uganda. National obstetric fistula strategy (2020/21–2024/25). Kampala: Ministry of Health Uganda, 2020.
Hilton P. Vesico-vaginal fistulas in developing countries. Int J Gynaecol Obstet. 2003;82(3):285–95.
Hilton P, Ward A. Epidemiological and surgical aspects of urogenital fistulae: a review of 25 years’ experience in southeast Nigeria. Int Urogynecol J Pelvic Floor Dysfunct. 1998;9(4):189–94.
Arrowsmith S, Hamlin EC, Wall LL. Obstructed labor injury complex: obstetric fistula formation and the multifaceted morbidity of maternal birth trauma in the developing world. Obstet Gynecol Surv. 1996;51(9):568–74.
Wall LL, Arrowsmith SD, Briggs ND, Lassey A. Urinary incontinence in the developing world: the obstetric fistula. In: Abrams P, Cardozo L, Khoury S, Wein A, eds. Incontinence. Plymouth: Health Publication Ltd, 2002.
Wall LL, Arrowsmith SD, Briggs ND, Browning A, Lassey A. The obstetric vesicovaginal fistula in the developing world. Obstet Gynecol Surv. 2005;60(7 Suppl 1):S3–51.
Zeleke BM, Ayele TA, Woldetsadik MA, Bisetegn TA, Adane AA. Depression among women with obstetric fistula, and pelvic organ prolapse in northwest Ethiopia. BMC Psychiatry. 2013;13:236.
Browning A, Fentahun W, Goh JT. The impact of surgical treatment on the mental health of women with obstetric fistula. BJOG. 2007;114(11):1439–41.
Goh JT, Sloane KM, Krause HG, Browning A, Akhter S. Mental health screening in women with genital tract fistulae. BJOG. 2005;112(9):1328–30.
El Ayadi A, Byamugisha J, Obore S, et al. Development and preliminary validation of a post-fistula repair reintegration instrument among Ugandan women. Reprod Health J. 2017;14(1):109.
El Ayadi AM, Barageine J, Korn A, et al. Trajectories of women’s physical and psychosocial recovery following fistula repair in Uganda. Trop Med Int Health. 2019;24(1):53–64.
Ahmed S, Holtz SA. Social and economic consequences of obstetric fistula: life changed forever? Int J Gynaecol Obstet. 2007;99(Suppl 1):S10–5.
Murphy M. Social consequences of vesico-vaginal fistula in northern Nigeria. J Biosoc Sci. 1981;13(2):139–50.
Ojanuga D. Social work practice with childbirth-injured women in Nigeria. Health Soc Work. 1994;19(2):120–4.
Bangser M. Obstetric fistula and stigma. Lancet. 2006;367(9509):535–6.
Shittu OS, Ojengbede OA, Wara LH. A review of postoperative care for obstetric fistulas in Nigeria. Int J Gynaecol Obstet. 2007;99(Suppl 1):S79–84.
Keyser L, McKinney J, Hosterman L, Chen CCG. Rehabilitative care practices in the management of childbirth-related pelvic fistula: a systematic review. Int Urogynecol J. 2021;32(9):2311–24.
Ojengbede OA, Baba Y, Morhason-Bello IO, et al. Group psychological therapy in obstetric fistula care: a complementary recipe for the accompanying mental ill health morbidities? Afr J Reprod Health. 2014;18(1):155–9.
Johnson KA, Turan JM, Hailemariam L, Mengsteab E, Jena D, Polan ML. The role of counseling for obstetric fistula patients: lessons learned from Eritrea. Patient Educ Couns. 2014;80(2):262–5.
Watt M, Wilson S, Sikkema K, Velloza J, Mosha M, Masenga G. Development of an intervention to improve mental health for obstetric fistula patients in Tanzania. Ann Glob Health. 2015;81(1):214–5.
Watt MH, Mosha MV, Platt AC, et al. A nurse-delivered mental health intervention for obstetric fistula patients in Tanzania: results of a pilot randomized controlled trial. Pilot Feasibility Stud. 2017;3:35.
Castille YJ, Avocetien C, Zaongo D, Colas JM, Peabody JO, Rochat CH. Impact of a program of physiotherapy and health education on the outcome of obstetric fistula surgery. Int J Gynaecol Obstet. 2014;124(1):77–80.
Castille YJ, Avocetien C, Zaongo D, Colas JM, Peabody JO, Rochat CH. One-year follow-up of women who participated in a physiotherapy and health education program before and after obstetric fistula surgery. Int J Gynaecol Obstet. 2015;128(3):264–6.
Keyser L, McKinney J, Salmon C, Furaha C, Kinsindja R, Benfield N. Analysis of a pilot program to implement physical therapy for women with gynecologic fistula in the Democratic Republic of Congo. Int J Gynaecol Obstet. 2014;127(2):127–31.
Keyser L, Hollander L, McKinney J, Benfield N. The fistula and obstetric rehabilitation initiative: using pelvic floor physical therapy to augment surgical repair of fistula. Female Pelvic Med Reconstr Surg. 2013;19:S102.
Pollaczek L, Tavrow P, Mohamed H. Obstetric Fistula in Kenya a holistic model of outreach, treatment, and reintegration. In: Dworkin S, Gandhi M, and Passano P, editors. Women's empowerment and global health: A twenty-first century agenda. University of California Press. (2016). URL: https://www.ucpress.edu/book/9780520272880/womens-empowerment-and-global-health
Uganda Ministry of Health. National Obstetric Fistula strategy. Kampala: MOH, 2011.
Care F. Counseling the obstetric fistula client: a training curriculum. New York: Engender Health; 2012.
De Bernis L. Obstetric fistula: guiding principles for clinical management and programme development, a new WHO guideline. Int J Gynaecol Obstet. 2007;99(Suppl 1):S117–21.
Patel V, Weiss HA, Chowdhary N, et al. Effectiveness of an intervention led by lay health counsellors for depressive and anxiety disorders in primary care in Goa, India (MANAS): a cluster randomised controlled trial. Lancet. 2010;376(9758):2086–95.
Patel V, Chowdhary N, Rahman A, Verdeli H. Improving access to psychological treatments: lessons from developing countries. Behav Res Ther. 2011;49(9):523–8.
Murray LK, Dorsey S, Haroz E, et al. A common elements treatment approach for adult mental health problems in low- and middle-income countries. Cogn Behav Pract. 2014;21(2):111–23.
McFarlane CA, Kaplan I. Evidence-based psychological interventions for adult survivors of torture and trauma: a 30-year review. Transcult Psychiatry. 2012;49(3–4):539–67.
Bolton P, Lee C, Haroz EE, et al. A transdiagnostic community-based mental health treatment for comorbid disorders: development and outcomes of a randomized controlled trial among Burmese refugees in Thailand. PLoS Med. 2014;11(11):e1001757.
Bolton P, Bass J, Neugebauer R, et al. Group interpersonal psychotherapy for depression in rural Uganda: a randomized controlled trial. JAMA. 2003;289(23):3117–24.
Byamugisha J, Obore S, Mwanje H, et al. Reintegration to family and community after obstetric fistula surgery: experiences of Ugandan Women. International Society of Obstetric Fistula Surgeons Conference 2014. Kampala, Uganda; 2014.
Keyser L, McKinney J. Implementing physical rehabilitation services into comprehensive fistula and maternity care: a training guide for health care workers. Washington, DC: Mama LLC and EngenderHealth/Fistula Care Plus; 2019.
Association of Microfinance Institutions of Uganda. The Uganda Microfinance Directory 2013/2014. 2014. http://www.amfiu.org.ug/images/docs/carol/Directory2013.pdf. Accessed 1 Nov 2014.
Foundation for Sustainable Development. Microfinance and Microenterprise Issues in Uganda. 2015. http://www.fsdinternational.org/country/uganda/mfissues. Accessed 1 Nov 2014.
Proctor E, Silmere H, Raghavan R, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health. 2011;38(2):65–76.
Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. 2015;10(53):4406164.
Klovning A, Avery K, Sandvik H, Hunskaar S. Comparison of two questionnaires for assessing the severity of urinary incontinence: the ICIQ-UI SF versus the incontinence severity index. Neurourol Urodyn. 2009;28(5):411–5.
Üstün TB, Kostanjsek N, Chatterji S, Rehm J. Measuring health and disability: manual for WHO disability assessment schedule WHODAS 2.0: World Health Organization; 2010.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–13.
Pollaczek L, El Ayadi AM, Mohamed HC. Building a country-wide fistula treatment network in Kenya: results from the first six years (2014–2020). BMC Health Services Res. 2022;22(1):280.
McCammon MA, Otondo NA, Kay N. Economic empowerment of the pilot reintegration program for female genital fistula survivors in Kenya during the COVID-19 pandemic. Front Glob Womens Health. 2022;3:966390.
Browning A, Menber B. Women with obstetric fistula in Ethiopia: a 6-month follow-up after surgical treatment. BJOG. 2008;115:1564–9.
Debela TF, Hordofa ZA, Aregawi AB, Sori DA. Quality of life of obstetrics fistula patients before and after surgical repair in the Jimma University Medical Center, Southwest Ethiopia. BMC Womens Health. 2021;21(1):212.
Bass JK, Annan J, McIvor Murray S, et al. Controlled trial of psychotherapy for Congolese survivors of sexual violence. N Engl J Med. 2013;368(23):2182–91.
Acknowledgements
The authors would like to thank our study participants for sharing their time and experiences with us.
Funding
This study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (Grant: R00HD086232).
Author information
Authors and Affiliations
Contributions
J.Ba.: conceptualization, writing the original draft, supervision, project administration; H.N.: conceptualization, investigation, project administration, writing, review, and editing; S.Ob.: conceptualization, writing, review, and editing; E.M.: investigation, project administration writing, review, and editing; D.M.: investigation, project administration, writing, review, and editing; A.J.: investigation, project administration, writing, review, and editing; S.Ak.: investigation, project administration, writing, review, and editing; S.Op.: investigation, project administration, writing, review, and editing; L.K.: resources, project administration, writing, review, and editing; J.M.: resources, project administration, writing, review, and editing; A.K.: conceptualization, writing, review, and editing, supervision; S.Al.: formal analysis, writing the original draft, visualization; J.By.: conceptualization, writing, review, and editing, supervision; A.M.E.: conceptualization, methodology, software, formal analysis, writing the original draft, supervision, project administration, funding acquisition.
Corresponding author
Ethics declarations
Ethics
The study protocol was approved by the University of California San Francisco Institutional Review Board, the Makerere University School of Medicine Research and Ethics Committee (Mak-SOMREC-2020–37), and the Uganda National Council on Science and Technology. All participants provided written confirmation of informed consent to participation.
Conflicts of interest
None.
Additional information
Handling Editor: Catherine Matthews
Editor in Chief: Maria A. Bortolini
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Appendix 1. Reintegration intervention session details for health education, psychosocial counseling, and physiotherapy components
Appendix 1. Reintegration intervention session details for health education, psychosocial counseling, and physiotherapy components
Health education
Session | Objective | Duration | Timinga | Delivery |
|---|---|---|---|---|
1. Admission and pre-operative management: preparing for upcoming surgery and recovery (part 1) | Introduce patients to fistula | 30 min | Pre-operatively | Group |
Introduce patients to care providers | ||||
Provide overview of procedure, risks, and outcomes | ||||
Address patient concerns and questions about procedure and recovery | Day 1 | |||
2. Admission and pre-operative management: preparing for upcoming surgery and recovery (part 2) | Familiarize patients with the patient ward and the surgical theater | 30 min | Pre-operatively | Group |
Discuss pre-operative preparations | ||||
Discuss post-operative management | ||||
Address any patient concerns and questions about procedure and recovery | Day 2 | |||
3. Overview of post-operative management | To discuss outcomes of surgery | 30 min | Day 2 (post-operatively) | Group |
To discuss post-operative care management at the facility | ||||
Address any patient concerns and questions | ||||
4. Reproductive system anatomy and function | Familiarize participants with the female reproductive system and female pelvis, anatomy, and functions | 30 min | Day 2 (post-operatively) | Group |
5. Development of fistula | Identify the causes of obstetric fistula | 30 min | Day 4 (post-operatively) | Group |
6. Common myths and misconceptions about fistula | To dispel any common rumors and myths about obstetric fistula | 30 min | Day 4 (post-operatively) | Group |
To explain how these may hamper women’s ability to prevent fistulas and to access treatment | ||||
7. Health and social consequences of fistula | To identify and discuss the health consequences of fistula | 20 min | Day 6 (post-operatively) | Group |
To identify and discuss the social consequences of fistula | ||||
8. Fistula prevention | To discuss ways of preventing obstetric fistula after repair | 40 min | Day 6 (post-operatively) | Group |
To introduce birth spacing | ||||
9. Sexual and reproductive health after fistula repair | To educate patients on sexual health | 30 min | Day 8 (post-operatively) | Group |
To familiarize participants reproductive tract issues | ||||
To identify personal timelines for family planning and fertility preferences | ||||
10. Family planning | To identify different family planning methods | 30 min | Day 8 (post-operatively) | Group |
To dispel myths and misconceptions regarding contraceptives | ||||
To facilitate discussion of which family planning method might be right for the participant | ||||
11. Future obstetric care | To understand the components and reasons for antenatal care during pregnancy | 30 min | Day 10 (post-operatively) | Group |
To recognize the danger signs during pregnancy | ||||
To discuss the importance of planning and preparation for safe delivery | ||||
Facilitate participant creation of a birth plan | ||||
12. Nutrition | To understand optimizing nutrition for recovery | 30 min | Day 10 (post-operatively) | Group |
13. Post-discharge management | To identify ways in which to take care of herself at home | 30 min | Day 12 (post-operatively) | Group |
To discuss the importance of follow-up visits | ||||
To recognize surgical warning after discharge | ||||
Facilitate participants in creating a complication | ||||
14. Recap of health education sessions | To prepare the patient for her return home, which maximizes the likelihood of a positive reintegration experience | 30 min | Day 12, 13, or 14 (post-operatively) | Group |
To review all of the materials and information discussed during the health education sessions | ||||
For participants to share their experiences, ask questions | ||||
15. Health education counseling for the participant’s family/caregiver (optional) | To communicate patient’s health condition and treatment (only if requested to be shared with family member(s)/caretaker | 60 min | TBD | Group |
To communicate any risks and possible side effects | ||||
To address any concerns and questions brought up by the patient’s social support | ||||
To identify warning signs | ||||
To develop a plan in the case of complications | ||||
To provide guidance on how to support the patient at home | ||||
To discuss sexuality after surgical repair | ||||
To discuss reproductive tract and sexually transmitted infections |
Psychosocial counseling
Session | Objective | Duration | Timinga | Delivery |
|---|---|---|---|---|
1. Introduction to psychological counseling | Introduction to counseling | 30 min | Day −1 (pre-operatively) | Individual |
Assessing the patient's needs and concerns | ||||
Set initial treatment plan/goals | ||||
Determine if the patient is ready for group counseling session | ||||
2. Recounting experience with fistula | To get familiar with each other | 60 min | Day 2 (post-operatively) | Group |
To normalize the patient’s experience | ||||
To acknowledge the negative and possible positive impacts of the fistula experience on relationships with others | ||||
To begin exploration of how the patient’s experience of an obstetric fistula impacts her feelings and thoughts about herself | ||||
3. Reframing the fistula experience | To promote cognitive reframing of the fistula experience through medical education | 60 min | Day 4 (post-operatively) | Group |
Teach medical information on fistula and surgery | ||||
Validate experiences of a normal medical condition | ||||
Help the patient to reframe her personal narrative | ||||
4. Identifying thoughts and emotions | To introduce the patient to the cognitive-behavioral model | 60 min | Day 6 (post-operatively) | Group |
To begin the teaching patient how to reframe negative or unhelpful thoughts | ||||
Review key emotions | ||||
Identify negative and problematic thoughts | ||||
Link thoughts to resulting emotions | ||||
Begin practicing reframing problematic thoughts | ||||
To manage the emotions associated with their situation | ||||
5. Develop coping strategies | To help the patient to recognize and respond to stressors by utilizing appropriate and effective coping skills | 60 min | Day 8 (post-operatively) | Group |
Discuss the patient’s negative vs positive coping strategies | ||||
Coach the patient to recognize stressors and respond by utilizing appropriate and effective coping skills | ||||
6. Explore social relationships | To examine the effect of social relationships on the patient’s life | 60 min | Day 10 (post-operatively) | Group |
To generate specific strategies to strengthen social relationships | ||||
Discuss how one’s social network influences thoughts and feelings | ||||
Formulate strategies to expand and optimize the patient’s social support network | ||||
Review tools for discussing her condition with others | ||||
To practice communication skills | ||||
Mobilize home support by identifying partner/caregiver to participate in optional combined counseling session | ||||
7. Planning for the future | To prepare the patient for her return home, which maximizes the likelihood of a positive reintegration experience | 60 min | Day 12 (post-operatively) | Group |
Make practical plans for the patient’s return to her community | ||||
Discuss the possibility of an incomplete cure and post-surgery medical recommendations | ||||
8. Patient pre-discharge assessment | Review therapy action plan and discuss progress in reaching goals | 30 min | Day 14 (post-operatively) | Individual |
Patient assessment and addressing the patient's remaining needs and concerns | ||||
Identify if the patient requires additional psychiatric counseling/emotional support/medication if she suffers from a trauma-related fistula | ||||
9. Building social support opportunities (optional) | Intended to facilitate social support for the patient returning home after repair | 60 min | Offered between days 10 and 15 (post-operatively) | Group (with patient and partner/caregiver) |
Physiotherapy
Session | Objective | Duration | Timing | Delivery |
|---|---|---|---|---|
1. Introduction to physical therapy | Introduction to physical therapy | 60 min | Day −2 (pre-operatively) | Individual |
Introduction to functional pelvic anatomy | ||||
Goal setting and expectations | ||||
Introduce breathing exercises | ||||
Complete baseline WHODAS and ICIQ with physical therapist | ||||
2. Physical therapy assessments | Functional mobility assessment | 60 min | Day −1 (pre-operatively) | Individual |
Practical abdominal assessment | ||||
External pelvic floor assessment | ||||
Internal pelvic floor assessment | ||||
3–8. Physical therapy for acute/inflammatory phase | Functional mobility exercises | 60 min | Days 2–7 (post-operatively) | Group |
Diaphragmatic breathing exercises to load the pelvic floor without straining the healing tissues | ||||
Sub-maximal pelvic floor muscle exercises while lying in bed | ||||
9–14. Physical therapy for sub-acute phase | Functional mobility exercises | 60 min | Days 8–13 (post-operatively) | Group |
Diaphragmatic breathing exercises | ||||
Sub-maximal to maximal pelvic floor muscle exercises | ||||
Exercises for the abdominal, hip, and low back muscles | ||||
Stretching areas of scar tissue and muscle and joint tightness (or contracture) | ||||
15. Physical therapy for sub-acute phase with treatment plan for discharge | Group: same objectives as sessions 9–14 | 60 min | Day 14 (post-operatively) | Group and individual |
Individual: patient assessment and development of home treatment plan | ||||
Follow-up | Physical assessment | 60 min | 6 weeks | Individual |
Reinforcement/adjustment of exercises |
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Barageine, J.K., Nalubwama, H., Obore, S. et al. Development and Pilot Test of a Multi-Component Intervention to Support Women’s Recovery from Female Genital Fistula. Int Urogynecol J (2024). https://doi.org/10.1007/s00192-024-05814-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00192-024-05814-3