
Abstract
Purpose
To evaluate the effects of rectal enemas on rectal doses during postoperative high-dose-rate (HDR) vaginal cuff brachytherapy (VCB).
Patients and methods
This prospective trial included 59 patients. Two rectal cleansing enemas were self-administered before the second fraction, and fraction 1 was considered the basal status. Dose–volume histogram (DVH) values were generated for the rectum and correlated with rectal volume variation. Statistical analyses used paired and unpaired t-tests.
Results
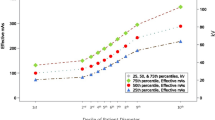
Despite a significant 15 % reduction in mean rectal volume (44.07 vs. 52.15 cc, p = 0.0018), 35.6 % of patients had larger rectums after rectal enemas. No significant rectal enema-related DVH differences were observed compared to the basal data. Although not statistically significant, rectal cleansing-associated increases in mean rectal DVH values were observed: D0.1 cc: 6.6 vs. 7.21 Gy; D1 cc: 5.35 vs. 5.52 Gy; D2 cc: 4.67 vs. 4.72 Gy, before and after rectal cleaning, respectively (where Dx cc is the dose to the most exposed x cm3). No differences were observed in DVH parameters according to rectal volume increase or decrease after the enema. Patients whose rectal volume increased also had significantly larger DVH parameters, except for D5 %, D25 %, and D50 %. In contrast, in patients whose rectal volume decreased, significance was only seen for D25 % and D50 % (Dx % dose covering x % of the volume). In the latter patients, nonsignificant reductions in D2 cc, D5 cc and V5 Gy (volume receiving at least 5 Gy) were observed.
Conclusion
The current rectal enemas protocol was ineffective in significantly modifying rectal DVH parameters for HDR-VCB.
Zusammenfassung
Ziel
Beurteilung der Auswirkungen von rektalen Dosen während postoperativer High-Dose-Rate-(HDR-)Brachytherapie an der Scheidenmanschette („vaginal cuff brachytherapy“, VCB).
Patienten und Methoden
An der prospektiven Studienahmen 59 Patientinnen teil. Vor der zweiten Fraktion wurden zwei selbstverabreichte Reinigungseinläufe durchgeführt. Fraktion 1 wurde als Grundstatus betrachtet. Für das Rektum wurden Dosis-Volumen-Histogramm-(DVH-)Werte generiert und mit der rektalen Volumenvariation korreliert. Für statistische Analysen wurden t-Tests für verbundene und unverbundene Stichproben verwendet.
Ergebnisse
Trotz einer signifikanten 15%igen durchschnittlichen Reduktion des rektalen Volumens (44,07 vs. 52,15 cc; p = 0,0018) hatten 53,6% der Patientinnen nach dem rektalen Einlauf ein vergrößertes Rektum. Im Vergleich mit den Grunddaten bestanden keine signifikanten DVH-Unterschiede bezüglich der Verabreichung des rektalen Einlaufs. Eine statistisch nichtsignifikante Zunahme der durchschnittlichen rektalen DVH-Werte wurde im Zusammenhang mit der rektalen Spülung festgestellt: D0,1 cc, 6,6 vs. 7,21 Gy; D1 cc, 5,35 vs. 5,52 Gy; D2 cc, 4,67 vs. 4,72 Gy, jeweils vor und nach Rektalspülung. Bezüglich der Zunahme oder Abnahme des rektalen Volumens nach Verabreichung des Einlaufs ergaben sich keine Unterschiede in den DVH-Parametern. Die Patientinnen, deren rektales Volumen zugenommen hatte, wiesen eine signifikante Zunahme der DVH-Parameter auf, außer bei D5%, D25%, D50%. Eine Signifikanz bei Patientinnen mit einem verkleinerten rektalen Volumen wurde hingegen nur bei D25% und D50% festgestellt. Bei Letzteren wurde eine nichtsignifikante Verringerung der Werte für D2 cc, D5 cc und V5 Gy beobachtet.
Schlussfolgerung
Die Vorgehensweise für rektale Einläufe erwies sich als unzureichend für eine signifikante Veränderung von rektalen DVH-Parametern bei der HDR-VCB.

Similar content being viewed by others


References
Creutzberg CL, van Putten WL, Koper PC et al (2000) Surgery and postoperative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: multicentre randomised trial. PORTEC Study Group. Post Operative Radiation Therapy in Endometrial Carcinoma. Lancet 355:1404–1411
Keys HM, Roberts JA, Brunetto VL et al (2004) A phase III trial of surgery with or without adjunctive external pelvic radiation therapy in intermediate risk endometrial adenocarcinoma: a Gynecologic Oncology Group study. Gynecol Oncol 92:744–751
Nout RA, Smit VT, Putter H et al (2010) Vaginal brachytherapy versus pelvic external beam radiotherapy for patients with endometrial cancer of high-intermediate risk (PORTEC-2): an open-label, non-inferiority, randomised trial. Lancet 375:816–823
Landoni F, Maneo A, Colombo A et al (1997) Randomised study of radical surgery versus radiotherapy for stage Ib–IIa cervical cancer. Lancet 350:535–540
Neumann O, Kluge A, Lyubina O et al (2014) Robotic radiosurgery as an alternative to brachytherapy for cervical cancer patients. Strahlenther Onkol 190:538–545
Davila Fajardo R, van Os R, Buist MR et al (2014) Post-operative radiotherapy in patients with early stage cervical cancer. Gynecol Oncol 134:52–59
Rotman M, Sedlis A, Piedmonte MR et al (2006) A phase III randomized trial of postoperative pelvic irradiation in Stage IB cervical carcinoma with poor prognostic features: follow-up of a gynecologic oncology group study. Int J Radiat Oncol Biol Phys 65:169–176
Mazeron R, Gilmore J, Champoudry J et al (2014) Volumetric evaluation of an alternative bladder point in brachytherapy for locally advanced cervical cancer. Strahlenther Onkol 190:41–47
Potter R, Gerbaulet A, Haie-Meder C (2002) Endometrial cancer. The GEC ESTRO Handbook of Brachytherapy. ESTRO, Leuven, pp 365–401
Small W, Beriwal S, Demanes DJ et al (2012) American Brachytherapy Society consensus guidelines for adjuvant vaginal cuff brachytherapy after hysterectomy. Brachytherapy 11:58–67
Sabater S, Arenas M, Berenguer R et al (2015) Dosimetric analysis of rectal filling on rectal doses during vaginal cuff brachytherapy. Brachytherapy 14:458–463. http://dx.doi.org/10.1016/j.brachy.2015.02.391
Sabater S, Sevillano M, Andres I et al (2013) Reduction of rectal doses by removal of gas in the rectum during vaginal cuff brachytherapy. Strahlenther Onkol 189:951–956
Deasy JO, Blanco AI, Clark VH (2003) CERR: a computational environment for radiotherapy research. Med Phys 30:979–985
About Epworth Radiation Oncology. Accessed 17 Feb 2015
Intracavitary implants (2015) Gynecologic brachytherapy. Accessed 17 Feb 2015
Lim J, Durbin-Johnson B, Valicenti R et al (2013) The impact of maximum rectal distention and tandem angle on rectal dose delivered in 3D planned gynecologic high dose-rate brachytherapy. Int J Gynecol Cancer 23:1078–1083
Iati G, Pontoriero A, Mondello S et al (2014) Three-dimensional treatment planning for vaginal cuff brachytherapy: dosimetric effects on organs at risk according to patients position. Brachytherapy 13:568–571
Guler OC, Onal C, Acibuci I (2014) Effects of bladder distension on dose distribution of vaginal vault brachytherapy in patients with endometrial cancer. J Contemp Brachytherapy 6:371–376
Hung J, Shen S, De Los Santos JF et al (2012) Image-based 3D treatment planning for vaginal cylinder brachytherapy: dosimetric effects of bladder filling on organs at risk. Int J Radiat Oncol Biol Phys 83:980–985
Kim RY, Shen S, Lin HY et al (2010) Effects of bladder distension on organs at risk in 3D image-based planning of intracavitary brachytherapy for cervical cancer. Int J Radiat Oncol Biol Phys 76:485–489
Stewart AJ, Cormack RA, Lee H et al (2008) Prospective clinical trial of bladder filling and three-dimensional dosimetry in high-dose-rate vaginal cuff brachytherapy. Int J Radiat Oncol Biol Phys 72:843–848
Hoskin PJ, Bownes P, Summers A (2002) The influence of applicator angle on dosimetry in vaginal vault brachytherapy. Br J Radiol 75:234–237
Holloway CL, Macklin EA, Cormack RA et al (2011) Should the organs at risk be contoured in vaginal cuff brachytherapy? Brachytherapy 10:313–317
Sabater S, Andres I, Sevillano M et al (2013) Dose accumulation during vaginal cuff brachytherapy based on rigid/deformable registration vs. single plan addition. Brachytherapy 13:343–351
Longo JM, Chen S, Thompson R et al (2011) Measuring the interfractional variation in dose to the rectum and the bladder using CT-based treatment planning for postoperative high dose rate vaginal brachytherapy in women with endometrial cancer. Int J Radiat Oncol Biol Phys 81:S478
Rovirosa A, Valduvieco I, Ascaso C et al (2013) Daily schedule for high-dose-rate brachytherapy in postoperative treatment of endometrial carcinoma. Clin Transl Oncol 15:111–116
Valduvieco I, Rovirosa A, Herreros A et al (2012) Three or four fractions per week in postoperative high-dose-rate brachytherapy for endometrial carcinoma. The long-term results on vaginal relapses and toxicity. Clin Transl Oncol. doi:10.1007/s12094-012-0974-0
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
S. Sabater, I. Andrés, M. Gascon, A. Rovirosa, M. Sevillano, R. Berenguer, C. Camacho-Lopez, M. Aguayo, M.V. Villas, and M. Arenasstate state that there are no conflicts of interest.
All studies on humans described in the present manuscript were carried out with the approval of the responsible ethics committee and in accordance with national law and the Helsinki Declaration of 1975 (in its current, revised form). Informed consent was obtained from all patients included in studies.
Rights and permissions
About this article

Cite this article
Sabater, S., Andrés, I., Gascon, M. et al. Effect of rectal enemas on rectal dosimetric parameters during high-dose-rate vaginal cuff brachytherapy. Strahlenther Onkol 192, 248–253 (2016). https://doi.org/10.1007/s00066-016-0940-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-016-0940-9