
Abstract
Background
For complex patients in the intensive care unit or in the operating room, many questions regarding their haemodynamic management cannot be answered with simple clinical examination. In particular, arterial pressure allows only a rough estimation of cardiac output. Transpulmonary thermodilution is a technique that provides a full haemodynamic assessment through cardiac output and other indices.
Main body
Through the analysis of the thermodilution curve recorded at the tip of an arterial catheter after the injection of a cold bolus in the venous circulation, transpulmonary thermodilution intermittently measures cardiac output. This measure allows the calibration of pulse contour analysis. This provides continuous and real time monitoring of cardiac output, which is not possible with the pulmonary artery catheter. Transpulmonary thermodilution provides several variables beyond cardiac output. It estimates the end-diastolic volume of the four cardiac cavities, which is a marker of cardiac preload. It provides an estimation of the systolic function of the combined ventricles. It is more direct than the pulmonary artery catheter, but does not allow the distinct estimation of right and left cardiac function. It is easier and faster to perform than echocardiography, but does not provide a full evaluation of the cardiac structure and function. Transpulmonary thermodilution has the unique advantage of being able to estimate at the bedside extravascular lung water, which quantifies the volume of pulmonary oedema, and pulmonary vascular permeability, which quantifies the degree of a pulmonary capillary leak. Both indices are helpful for guiding fluid strategy, especially in case of acute respiratory distress syndrome.
Conclusions
Transpulmonary thermodilution provides a full cardiovascular evaluation that allows one to answer many questions regarding haemodynamic management. It belongs to the category of “advanced” devices that are indicated for the most critically ill and/or complex patients.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
A task force of the European Society of Intensive Care Medicine recently recommended using advanced haemodynamic monitoring in severe shock and complex situations and stated that the pulmonary artery catheter and transpulmonary thermodilution (TPTD) devices are suitable for this purpose [1]. The TPTD technique emerged in the early 2000s. The PiCCO (Pulsion Medical Systems, Munich, Germany) and the Volume View (Edwards LifeSciences, Irvine, United States of America) devices measure cardiac output but also provide several other valuable pieces of haemodynamic information (Fig. 1). In our opinion, the approach of TPTD is quite different from pulmonary artery catheterisation in many repects. The attractiveness of this approach and the fact that the technique is easy to set up likely explain why TPTD use has increased. Which methods are used by TPTD to measure cardiac output and the other variables and what can be said regarding the validation of these variables? What are the indications of TPTD and what is its place in the haemodynamic management of ICU and surgical patients? These are the questions we address in this review.

Haemodynamic variables provided by transpulmonary thermodilution and calibrated pulse contour analysis, with their meaning, utility and normal values (N). ARDS acute respiratory distress syndrome
Measurement of cardiac output
How does TPTD measure cardiac output?
TPTD requires the injection of a bolus of cold saline in the superior vena cava territory. At the tip of a femoral arterial catheter (the tip stands in the iliac artery), a thermistor senses the decrease in blood temperature. As with standard pulmonary thermodilution, TPTD measures cardiac output by using the Stewart–Hamilton principle. Compared to the pulmonary artery catheter, the difference is that, with TPTD, cold saline is injected not in the right atrium but in a central vein and the blood temperature is measured not in the pulmonary artery but in a systemic artery.
Is TPTD accurate for measuring cardiac output?
From all the studies that have investigated the validity of TPTD [2], it can be reasonably concluded that this measurement of cardiac output is accurate compared to the pulmonary artery catheter and the Fick method. Besides its accuracy, the ability of TPTD devices to reliably track changes in cardiac output is also important. It is recommended to average the result of three bolus injections [3]. In such a case, the smallest change in cardiac output that can be accurately detected by TPTD is 12% (this is the “least significant change” of the technique) [4]. It is comparable with the pulmonary artery catheter [5].
The reliability of the measurement requires a significant difference in blood temperature induced by TPTD. According to the manufacturer’s recommendations, 15 mL of saline <8 °C must be injected. Therapeutic hypothermia does not affect the precision of the measurement of cardiac output by TPTD [6]. It seems that boluses at room temperature create a sufficient difference [7], although this may result in a slight but significant overestimation of cardiac output [8]. Very importantly, great caution should be applied when performing thermodilution (volume of injection, absence of leaks in the circuit, regularity of the speed of injection, bolus temperature), since any error in the thermodilution curve may affect the estimation of cardiac output but also of all variables that are inferred from the curve analysis.
When the venous catheter is inserted not in the superior vena cava but in a femoral vein, contralateral to the arterial catheter, the measurement of cardiac output is unaffected, while it is not the case for thoracic volumes measured by the technique (see below) [9, 10]. Of course, the arterial catheter must not be inserted in the femoral site on the same side as the venous catheter used for injection. Injecting the bolus in a port-a-catheter provides reliable measurements of cardiac output and its variations [11]. The technique cannot be used in case of extracorporeal membrane oxygenation. By contrast, continuous veno-venous haemofiltration does not affect the reliability of cardiac output measurement by TPTD [12,13,14], even for high blood pump flows [13]. The thermistor-tipped catheter is most often inserted in the femoral artery, but the axillary, brachial and radial (long catheter) arteries may also be used, although this requires that the elbow remains in the extended position.
What are the limitations of TPTD for measuring cardiac output?
One drawback of TPTD is that recirculation of the cold indicator is larger than with pulmonary thermodilution [2]. Also, if cardiac output is very low, typically below 2 L/min, TPTD devices do not provide any measure because of uncertainty about the technique’s reliability. The loss of injectate temperature is greater than with conventional thermodilution. In this regard, high volumes of lung water may theoretically amplify the loss of injectate temperature through the pulmonary circulation, even though this phenomenon is likely negligible [15]. Finally, the main drawback of TPTD for measuring cardiac output is that it performs only intermittent measurements (Table 1). It cannot detect short term changes, as induced by mechanical ventilation, passive leg raising [16] or end-expiratory occlusion [17] tests, for instance.
Calibration of pulse contour analysis
Besides TPTD, the PiCCO and VolumeView devices estimate cardiac output by analysis of the arterial curve (“pulse contour”) sampled through the arterial catheter. This allows real-time monitoring of cardiac output.
Pulse contour analysis is based on the relationship between stroke volume and the amplitude and shape of the aortic pressure curve [18]. Devices analyse the geometry of the pressure waveform recorded in a peripheral artery, estimate the arterial curve at the aortic level, and estimate stroke volume from the geometrical properties of the pressure waveform through proprietary algorithms.
The measure of cardiac output by pulse contour analysis is very precise, more so than with TPTD [5], but it may drift over time, especially when the arterial resistance changes [19,20,21]. Then, the PiCCO and Volume View devices calibrate pulse contour analysis by the value obtained by TPTD each time TPTD is performed. Compared to uncalibrated pulse contour analysis devices, calibrated ones have better accuracy, especially when arterial tone changes to a significant extent, for instance under vasopressors [20, 22]. Calibration of pulse contour analysis should be encouraged after a 1-h calibration-free period [23]. This does not mean that calibration must be performed every hour in patients with a TPTD device, but rather that, when cardiac output is mandatory for interpreting the haemodynamic condition, calibration of pulse contour analysis must be performed if 1 h or more has elapsed since the last calibration (Table 1).
Assessment of cardiac preload: global end-diastolic volume
What is the global end-diastolic volume?
Besides cardiac output, TPTD estimates some intrathoracic volumes of great pathophysiological interest (Fig. 1). This estimation is based on the analysis of both the thermodilution curve and its logarithmic transformation (Fig. 2). According to the Stewart–Hamilton principle, the total distribution volume of the cold indicator between the injection and detection sites, the intrathoracic thermal volume, is obtained by multiplying cardiac output by the mean transit time of the cold indicator. According to the Newman principle, the largest distribution volume of the cold indicator between the injection and detection sites, the total pulmonary volume, is obtained by multiplying cardiac output by the downslope time of the thermodilution curve. Then, subtracting the pulmonary thermal volume from the intrathoracic thermal volume estimates the global end-diastolic volume (GEDV). This corresponds to the volume of all four cardiac chambers at the end of diastole (Fig. 2). Whereas the PiCCO device assesses GEDV according to the Newman principle, the VolumeView device assesses it from a different geometrical analysis of the thermodilution curve, which is based on the slopes of the up and down parts of the curve and a proprietary function [24]. Nevertheless, both techniques have been demonstrated to be interchangeable [25].

Assessment of intrathoracic volume by the PiCCO device. With the VolumeView device, the geometrical analysis of the thermodilution curve directly estimates the global end-diastolic volume. Dt downslope time, MTt mean transit time. For explanation, see the text
Is GEDV valid as a measure?
GEDV behaves as it is typically expected from a marker of cardiac preload [26]. In patients with septic shock, GEDV increased with fluid administration but remained constant during dobutamine administration, despite similar increases of cardiac output [26]. It has been suspected that there is a mathematical coupling between GEDV and cardiac output since both variables are derived from the same thermodilution curve, but this has not been confirmed by clinical investigations [26,27,28].
GEDV includes the cardiac volume and also a part of the superior vena cava volume and the volume of the aorta that are between the bolus injection site and the thermistor. This may explain why GEDV is larger than the actual volume of the four cardiac chambers. Nevertheless, these vascular volumes are roughly unchanged during changes in cardiac preload. It has been demonstrated that GEDV reliably tracks the changes in volumetric preload induced by volume expansion when compared to echocardiographic measurements, better than the volumetric assessment allowed by some modified versions of the pulmonary artery catheter [29, 30].
The least significant change of GEDV when three cold boluses are injected is 12% [4]. If boluses are injected through the femoral vein, the normal values of GEDV are higher than if they are injected through the superior vena cava, since it includes the volume of the inferior vena cava [9, 10]. They can be estimated from formulas using a patient’s biometric data [10]. The changes in “femoral” GEDV are correlated with those of “superior vena cava” GEDV [10].
Measures of cardiac preload volumes or pressures?
It has been argued that volume markers of cardiac preload (end-diastolic volume measured by TPTD or echography) are better than pressure markers (central venous pressure, pulmonary artery occlusion pressure (PAOP)) since studies reported that left ventricular end-diastolic dimensions were better correlated with stroke volume than PAOP [31,32,33].
Nevertheless, two points must be kept in mind. First, if the ventricular compliance is low, small changes in volume induce larger changes in pressure, and changes in volume may underestimate changes in cardiac preload. Second, the risk of hydrostatic pulmonary oedema, the formation of which directly depends on the hydrostatic pressure gradient between the pulmonary capillary and interstitium [34], is better indicated by PAOP than by any volume indices.
A specific limitation of GEDV is that it does not distinguish between left and right cardiac preload. In practice, in case of right ventricular dilation, GEDV is increased while the left ventricular preload is normal [35, 36].
How do we use GEDV in practice?
Like all static markers of cardiac preload, GEDV is a poor indicator of fluid responsiveness [37]. Nevertheless, this does not mean that it is useless. Knowing the level of cardiac preload is essential for determining the shock origin when it is unclear. Also, during volume expansion, cardiac preload must be measured in order to check that it actually increases and that fluid has not just been diluted in the vasodilated venous reservoir [26].
Cardiac systolic function
Two indices provided by TPTD
TPTD estimates the left ventricular systolic function through the cardiac function index and the global ejection fraction. Cardiac function index is the ratio of cardiac output (measured by TPTD) and GEDV (Fig. 1). The global ejection fraction is equal to stroke volume divided by GEDV and multiplied by 4, assuming that the left ventricular end-diastolic volume is a quarter of GEDV. Of course, this is a rough assumption since all cardiac cavities are not of similar volume.
Some studies showed a good correlation between absolute values of cardiac function index and of the left ventricular ejection fraction (LVEF) measured by echocardiography in animals [38] and in patients [35, 36, 39]. Some specific cut-off values of cardiac function index and global ejection fraction accurately detected low values of LVEF [35, 36, 38, 40]. Moreover, changes in cardiac function index and global ejection fraction track changes in echocardiographic LVEF [35, 36, 40], especially when induced by inotropes [36, 40]. The least significant change of cardiac function index is 12% when three cold boluses are injected [4].
What are the limitations?
As for GEDV, the main limitation of cardiac function index and global ejection fraction comes from the dilation of the right cardiac chambers. In this situation, the GEDV is increased and the cardiac function index and global ejection fraction are decreased while the left ventricular contractility is unchanged [35, 36, 38, 40]. Also, although this has not been formally investigated, cardiac function index and global ejection fraction likely share with LVEF the limitation that they depend on left ventricular preload and afterload [41]. Moreover, even though it is possible to identify threshold values in order to detect low LVEF, the correlation between LVEF and cardiac function index obviously cannot be perfect since the cardiac function index is a marker of the “global” cardiac systolic function [35, 36, 38, 40] (Table 1). Echocardiography remains the most accurate bedside technique for measuring LV systolic function. Finally, echocardiography has the advantage of performing a complete assessment of cardiac structure and function, while it is not allowed by TPTD (Table 1).
What is the place of TPTD indices of systolic function in practice?
Echocardiography requires many more skills than TPTD. Moreover, it is rather tedious and time consuming, so it may not be performed as often as it should be during acute circulatory failure. Though the correlation between cardiac function index and LVEF is not perfect [35, 36, 39], every time thermodilution measurements are performed, global ejection fraction and cardiac function index give a rapid estimation of cardiac systolic function. They can easily warn clinicians that the left ventricular contractility is deteriorating and encourage them to perform echocardiography, which would not have been performed otherwise. In a patient that is receiving inotropes, TPTD systolic function indices also allow clinicians to follow the treatment effect [36].
Extravascular lung water
Extravascular lung water (EVLW) is fluid that accumulates in the interstitial and alveolar spaces (Fig. 1). EVLW increases because of increased lung permeability or because of increased hydrostatic pressure in the pulmonary capillaries, or both [42]. Since it is the main pathophysiological pattern of hydrostatic pulmonary oedema and of acute respiratory distress syndrome (ARDS), it might be of very special help for establishing diagnosis, assessing the severity of the disease and guiding the therapeutic strategy.
How does TPTD measure lung water?
With the PiCCO device, the estimation of EVLW is performed by subtracting the intrathoracic blood volume from the intrathoracic thermal volume (Fig. 2). The intrathoracic blood volume is estimated by multiplying GEDV by 1.25 [43]. The VolumeView device is based on the same principle but, as explained above, it estimates GEDV differently from the PiCCO device [24, 25] (Fig. 2). However, a good agreement between the values provided by both devices has been reported [24, 25].
The EVLW value is indexed to the predicted body weight, not the actual body weight, in order to avoid underestimation of EVLW [44]. When three cold boluses are used, the least significant change in EVLW is 12% [4]. Using room temperature boluses results in a slight but significant overestimation of EVLW [8].
Is the estimation of EVLW valid?
Several arguments support the reliability of the estimation of EVLW by TPTD. First, it has been validated against transpulmonary thermo-dye dilution in humans [43], and against gravimetry, the reference technique, in animals [45, 46] and humans [47]. Second, experimental [48, 49] and clinical [4, 50] studies demonstrated that the TPTD estimation of EVLW is precise. In an autopsy study in 30 patients, the correlation coefficient between EVLW measured by TPTD and by gravimetry was 0.90 [47]. TPTD was able to detect the small and short-term changes in EVLW induced by bronchoalveolar lavage [50]. With TPTD, it is also possible to detect the rapid increase in EVLW that occurs during a weaning-induced pulmonary oedema, sometimes over a few minutes only [51]. Third, the reliability of the TPTD estimation of EVLW is indirectly supported by studies showing that EVLW predicts mortality in critically ill patients [52,53,54,55,56] independent of other severity indices [52,53,54], which would be impossible to establish if the TPTD measurement of EVLW was unreliable.
What are the potential limitations of EVLW measurement?
In case of vascular occlusion due to pulmonary embolism, the volume of distribution of the cold indicator is reduced, resulting in underestimation of EVLW [57] (Table 1). Nevertheless, the occlusion of some small-diameter vessels during ARDS, which results from vascular remodelling, microthrombi, hypoxic vasoconstriction or positive end-expiratory pressure (PEEP), has no impact on the TPTD estimation of EVLW [58, 59].
The theoretical effects of PEEP on the measurement of EVLW by TPTD are contradictory. PEEP squeezes some pulmonary vessels and reduces the distribution volume of the cold indicator. By contrast, PEEP could recruit some atelectatic regions and alleviate the hypoxic constriction that prevents the thermal indicator from reaching such regions. By decreasing cardiac output, PEEP may also reduce the pulmonary microvascular hydrostatic pressure and hence EVLW. On the contrary, PEEP increases the central venous pressure, which may impede the lymphatic drainage of EVLW. Studies investigating the net effect of these mechanisms in clinical practice are scarce. One study reports that, in ARDS patients, there was a strong correlation between the EVLW measured by transpulmonary thermo-dye dilution and lung weight measured by computed tomography over a broad range of PEEP levels [60].
Lung resection logically decreases the volume of EVLW [61, 62] but TPTD may overestimate the remaining volume of EVLW [61]. Similarly, the estimation of EVLW by TPTD is significantly affected by one-lung ventilation [63].
The type of ARDS may affect the reliability of TPTD for estimating EVLW. In heterogeneous forms of ARDS, the pulmonary blood flow may be redistributed away from oedematous areas, which could lead to underestimation of EVLW [64], even though this redistribution phenomenon has been demonstrated to be severely blunted [65].
Pleural effusions of large volume could induce an overestimation of EVLW because the cold indicator also diffuses in the pleural liquid [66]. Nevertheless, a study found that, by contrast, removing pleural effusion increased EVLW, perhaps by alleviating atelectasis in contact with the pleural effusion [67]. As for cardiac output or GEDV, renal replacement therapy [12, 13] and therapeutic hypothermia [6] do not alter the measurement of EVLW.
Pulmonary vascular permeability index
TPTD estimates the permeability of the alveolo-capillary barrier through the pulmonary vascular permeability index, which is the ratio of EVLW over pulmonary blood volume, i.e. the ratio of the fluid volume that is out of the vessels over the fluid volume that remains in the vessels [68,69,70].
This index has been validated in animal [45] and clinical [68,69,70] studies showing that it is lower in hydrostatic pulmonary oedema than in ARDS. A pulmonary vascular permeability index value of 3 was found to be the best threshold for distinguishing between both forms of pulmonary oedema [68, 69] and should be considered as the maximal normal value. The number of human studies on the index is small for the moment, so that the normal value might be slightly different from 3. The pulmonary vascular permeability index shares the same limitations as EVLW.
How do we use EVLW and the pulmonary vascular permeability index in clinical practice?
Definition of ARDS
Although an increase in lung water and permeability is the pathophysiological hallmark of ARDS, its current definition does not take them into account [71]. In order to exclude hydrostatic pulmonary oedema, the Berlin definition only stipulates that the filling pressure of the left ventricle should not be elevated. Not only is this obviously a very indirect estimation of lung permeability, but also an elevated filling pressure of the left ventricle does not preclude that lung permeability is increased, especially after a few days of fluid resuscitation. Moreover, some clinical studies suggest that taking EVLW and/or pulmonary vascular permeability index values into account has helped to predict the progression to lung injury in patients with risk factors 2.6 ± 0.3 days before the patients met American-European Consensus Conference criteria of ARDS [72]. Changes in the pulmonary vascular permeability index should thus be taken into consideration for following worsening or improvement of ARDS in clinical practice. In another study, the value of EVLW was in close relationship with the severity of ARDS as defined by the categories of the Berlin definition [73]. It has also been shown that the use of EVLW improves by up to eightfold the post-test odds ratio for the diagnosis of acute lung injury, ARDS and severe lung injury [70]. At the least, all these reasons argue for using TPTD in order to better characterise the ARDS pattern [74, 75]. Of course, the cost of such devices prevents their use as a standard for every ARDS patient across the world.
Fluid management
In order to avoid fluid overload in critically ill patients, fluids should be administered only if preload responsiveness has been assessed by appropriate indices [76]. In addition, the risk of fluid therapy should also be considered. EVLW indicates the volume of water that has already leaked toward the lung interstitium and alveoli, while the pulmonary vascular permeability index indicates a priori the risk of leakage. In patients with ARDS, if EVLW and the pulmonary vascular permeability index are much higher than their normal values, fluid administration should be as restricted as possible.
In the context of ARDS, it has been reported that management based on protocols including EVLW measurements is safe [77], leads to a lower cumulative fluid balance [78], decreases ICU mortality [77], and reduces the duration of mechanical ventilation [78] and of ICU stay [78]. Some studies have provided different results. In a mixed population of ICU patients, TPTD was associated with an increased fluid balance [79]. In another study, TPTD-based fluid management did not improve outcome when compared to central venous pressure-based fluid [80]. Nevertheless, the protocols associated with the two latter studies have been strongly criticised [81, 82]. In studies investigating monitoring devices, the effect on prognosis is tightly related to the quality of the protocol attached to the device. Whatever the device, results from questionable management protocols are inherently questionable [81].
Weaning from mechanical ventilation
Our group demonstrated that an increase in EVLW during a spontaneous breathing trial was able to diagnose weaning-induced pulmonary oedema with good accuracy, in particular with 100% specificity [51]. This does not mean that a TPTD device should be set up only for the purpose of detecting weaning-induced pulmonary oedema, but rather that, if the device is already in place, one should pay attention to EVLW during weaning trials.
Side effects of TPTD
TPTD is an invasive technique although the invasiveness is not very different from the pulmonary artery catheter, even though it is easier to set up. Nevertheless, in a multicentre prospective series of 514 patients, the most common complications were small local haematomas after insertion (4.5%) and removal (1.2%) of the catheter. Other complications such as ischaemia (0.4%), pulse loss (0.4%) or femoral artery thrombosis (0.2%) were uncommon and transient, and all resolved with catheter removal or embolectomy [83]. This study is the only one that investigated such complications, and these results should be taken with caution. Nevertheless, in our opinion, they suggest that the technique has acceptable rates of complications when compared to the other risks incurred by critically ill patients.
The technique is contraindicated in case of femoral vascular prostheses. In our practice, in patients with arteriopathy, if two attempts to insert the catheter and the guide fail, we abandon the option of using the technique in this patient without further attempts. The weight of these complications must be compared to the severity of the patient condition, unacceptable for monitoring surgical interventions of patients at low risk but justified for high-risk surgical patients or critically ill patients [84].
The place of TPTD among haemodynamic monitoring devices
Haemodynamic monitoring: for which patients?
In the peri-operative setting
In the peri-operative setting, haemodynamic monitoring should be used to detect hypovolemia or low oxygen delivery for early prevention. In spite of its invasiveness, advanced haemodynamic monitoring should be preferred over less invasive devices in two circumstances. The first is when the patient is particularly complex and when more variables than just cardiac output are mandatory, such as during cardiac surgery and prolonged major surgery for instance [84]. The second is when less invasive techniques are more likely to be unreliable, as for instance uncalibrated pulse contour analysis during liver surgery because major changes in vasomotor tone are expected [19]. Several studies conducted in cardiac surgery and major abdominal surgery have shown that cardiac output monitoring led to a reduction in the rate of complications and the length of stay [85].
In the intensive care unit
In contrast to the peri-operative setting, no study has compared management with versus without haemodynamic monitoring in terms of mortality. In this context, demonstrating such a benefit would be very difficult. The prognosis of critically ill patients is influenced by so many factors that it is hard to believe a monitoring device alone could influence mortality. Many other monitoring techniques are used in ICU patients, such as electrocardiogram or blood gas analysis, while they have never been shown to improve prognosis. The decision to use haemodynamic monitoring in severe ICU patients should not be guided by outcome studies but by studies showing that it provides more complete information than basic monitoring with heart rhythm and blood pressure. In this regard, changes in arterial pressure only roughly detect changes in cardiac output [86, 87], especially when vasopressors change the arterial tone [86], monitoring EVLW can lead to decreases in fluid balance and advanced monitoring may change clinical decisions [88].
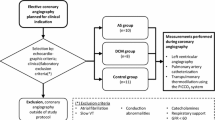
Based on such arguments, recent recommendations state that haemodynamic monitoring is mandatory in patients with hypotension that resists initial fluid therapy [1] (Fig. 3). Advanced monitoring is particularly warranted in patients with ARDS and in patients where the dose of vasopressor is high and/or increasing (Fig. 3). Nevertheless, it seems that this is less common in practice [89] than recommended by a recent consensus [1].

Indication for haemodynamic monitoring in the intensive care unit. A-line arterial line, CV-line central venous line. The choice also depends on team experience
Which TPTD device?
Today, two TPTD devices are commercially available: the PiCCO system, which is integrated in the ProAQT platform (Pulsion Medical Systems, Munich, Germany), and the VolumeView system, which is incorporated in the EV1000 platform (Edwards Life Sciences, Irvine, USA). Of course, the manufacturers’ software packages are proprietary and not open, but both systems work on the same principles and technological differences between them are likely very small. In two studies, the measurements of cardiac output and volumetric variables were similar between both devices [24, 25]. In one study, pulse contour analysis by the VolumeView method was found to have a slightly better precision than by the PiCCO system [90]. The VolumeView device overestimates GEDV and the derived variables when the inferior vena cava route is used for injecting the cold bolus, and corrections that have been described for the PiCCO reduce this overestimation [91].
TPTD versus pulmonary artery catheter?
TPTD/calibrated pulse contour analysis and traditional pulmonary thermodilution are both sophisticated techniques that provide several haemodynamic variables besides cardiac output. In this regard, both are suitable for complex and critically ill patients [1, 3, 84, 92]. An advantage of traditional pulmonary thermodilution is that it does not require recalibration. With the pulmonary artery catheter, however, semi-continuous estimation of cardiac output is not measured in real time and the response to a change in cardiac output is delayed by several minutes [93]. With calibrated pulse contour analysis, the displayed value of cardiac output is an average calculated over a few seconds only. Besides cardiac output, both techniques do not provide the same variables. PAOP has been repeatedly demonstrated to be unreliable for predicting fluid responsiveness, while calibrated pulse contour analysis allows one to perform passive leg raising or end-expiratory occlusion tests [76].
In order to decide to stop fluid administration, a given value of PAOP may correspond to different risk levels of increasing EVLW depending on the level of lung permeability [42]. For instance, fluid infusion at a PAOP of 12 mmHg would induce absolutely no lung oedema in a patient with normal lungs, while it would be extremely prone to increase EVLW in a patient with severe ARDS. Regarding the systolic function, in our opinion, the cardiac function index and global ejection fraction provide a more direct estimation than TPTD.
Unlike TPTD devices, the pulmonary artery catheter provides a direct estimation of pulmonary artery resistance. Right heart failure and severe pulmonary hypertension represent specific indications for the pulmonary artery catheter (Fig. 3) [1, 92]. Nevertheless, errors in the measurement of cardiac output resulting from tricuspid regurgitations must be kept in mind, even though it seems to exist mostly for severe regurgitations [94]. Also, the pulmonary artery catheter measures both central venous pressure and pulmonary artery pressure, allowing the estimation of right and left cardiac functions, while TPTD only estimates the global cardiac function. Another strong advantage of the pulmonary artery catheter is that it directly measures oxygen saturation of mixed venous blood, not central venous blood.
In conclusion, both types of devices can be used to monitor the haemodynamic status of critically ill patients with shock, although they provide clinicians with different answers to their questions. Clinicians should choose the device they know the best. The pulmonary artery catheter has a specific indication in case of acute right heart failure and acute pulmonary hypertension [1] (Fig. 3).
TPTD or echocardiography? No choice: TPTD and echocardiography!
In our opinion, clinicians do not need to choose between TPTD devices and echocardiography. Echocardiography is unique for a complete assessment of cardiac structure and function. It must be performed early in every patient with acute circulatory failure [1, 3] (Fig. 3). Nevertheless, it is difficult to consider echocardiography as a device for haemodynamic monitoring because of the time that is required for the ultrasound examination [95]. An advantage of TPTD over echocardiography is that nurse-driven approaches can be used and that several patients can be evaluated simultaneously. In addition, TPTD provides clinicians with information that is not offered by echocardiography, like EVLW. Our practice for monitoring the most critically ill patients is a combination of TPTD for continuous and repeated haemodynamic monitoring and echocardiography for punctual assessments of cardiac function (Fig. 3). In addition, TPTD measurements may trigger recourse to echocardiography if global ejection fraction or cardiac function index suddenly decrease.
Conclusions
Beyond cardiac output, TPTD provides several indices that help answer questions that clinicians ask themselves during haemodynamic management. In particular, it is a unique tool for guiding fluid therapy because it estimates lung water and permeability. Its place is in the management of the most critically ill and/or complex patients, which requires a reliable, precise and global vision of the cardiopulmonary condition. It will be very interesting to see how progress in technology in the era of digital health will transform and improve TPTD [96].
Abbreviations
- ARDS:
-
Acute respiratory distress syndrome
- EVLW:
-
Extravascular lung water
- GEDV:
-
Global end-diastolic volume
- LVEF:
-
Left ventricular ejection fraction
- PAOP:
-
Pulmonary artery occlusion pressure
- PEEP:
-
Positive end-expiratory pressure
- TPTD:
-
Transpulmonary thermodilution.
References
Cecconi M, De Backer D, Antonelli M, Beale R, Bakker J, Hofer C, Jaeschke R, Mebazaa A, Pinsky MR, Teboul JL, et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014;40(12):1795–815.
Sakka SG, Reuter DA, Perel A. The transpulmonary thermodilution technique. J Clin Monit Comput. 2012;26(5):347–53.
Teboul JL, Saugel B, Cecconi M, De Backer D, Hofer CK, Monnet X, Perel A, Pinsky MR, Reuter DA, Rhodes A, et al. Less invasive hemodynamic monitoring in critically ill patients. Intensive Care Med. 2016;42(9):1350–9.
Monnet X, Persichini R, Ktari M, Jozwiak M, Richard C, Teboul JL. Precision of the transpulmonary thermodilution measurements. Crit Care. 2011;15(4):R204.
Stetz CW, Miller RG, Kelly GE, Raffin TA. Reliability of the thermodilution method in the determination of cardiac output in clinical practice. Am Rev Respir Dis. 1982;126(6):1001–4.
Tagami T, Kushimoto S, Tosa R, Omura M, Hagiwara J, Hirama H, Yokota H. The precision of PiCCO(R) measurements in hypothermic post-cardiac arrest patients. Anaesthesia. 2012;67(3):236–43.
Faybik P, Hetz H, Baker A, Yankovskaya E, Krenn CG, Steltzer H. Iced versus room temperature injectate for assessment of cardiac output, intrathoracic blood volume, and extravascular lung water by single transpulmonary thermodilution. J Crit Care. 2004;19(2):103–7.
Huber W, Kraski T, Haller B, Mair S, Saugel B, Beitz A, Schmid RM, Malbrain ML. Room-temperature vs iced saline indicator injection for transpulmonary thermodilution. J Crit Care. 2014;29(6):1133.e7–1133.e14.
Schmidt S, Westhoff TH, Hofmann C, Schaefer JH, Zidek W, Compton F, van der Giet M. Effect of the venous catheter site on transpulmonary thermodilution measurement variables. Crit Care Med. 2007;35(3):783–6.
Saugel B, Umgelter A, Schuster T, Phillip V, Schmid RM, Huber W. Transpulmonary thermodilution using femoral indicator injection: a prospective trial in patients with a femoral and a jugular central venous catheter. Crit Care. 2010;14(3):R95.
Suria S, Wyniecki A, Eghiaian A, Monnet X, Weil G. Measurement of cardiac index by transpulmonary thermodilution using an implanted central venous access port: a prospective study in patients scheduled for oncologic high-risk surgery. PLoS One. 2014;9(8):e104369.
Sakka SG, Hanusch T, Thuemer O, Wegscheider K. The influence of venovenous renal replacement therapy on measurements by the transpulmonary thermodilution technique. Anesth Analg. 2007;105(4):1079–82.
Dufour N, Delville M, Teboul JL, Camous L, Favier du Noyer A, Richard C, Monnet X. Transpulmonary thermodilution measurements are not affected by continuous veno-venous hemofiltration at high blood pump flow. Intensive Care Med. 2012;38(7):1162–8.
Heise D, Faulstich M, Morer O, Brauer A, Quintel M. Influence of continuous renal replacement therapy on cardiac output measurement using thermodilution techniques. Minerva Anestesiol. 2012;78(3):315–21.
Pohl T, Kozieras J, Sakka SG. Influence of extravascular lung water on transpulmonary thermodilution-derived cardiac output measurement. Intensive Care Med. 2008;34(3):533–7.
Monnet X, Teboul JL. Passive leg raising: five rules, not a drop of fluid! Crit Care. 2015;19:18.
Monnet X, Osman D, Ridel C, Lamia B, Richard C, Teboul JL. Predicting volume responsiveness by using the end-expiratory occlusion in mechanically ventilated intensive care unit patients. Crit Care Med. 2009;37(3):951–6.
Monnet X, Teboul JL. Minimally invasive monitoring. Crit Care Clin. 2015;31(1):25–42.
Biais M, Nouette-Gaulain K, Cottenceau V, Vallet A, Cochard JF, Revel P, Sztark F. Cardiac output measurement in patients undergoing liver transplantation: pulmonary artery catheter versus uncalibrated arterial pressure waveform analysis. Anesth Analg. 2008;106(5):1480–6.
Monnet X, Anguel N, Naudin B, Jabot J, Richard C, Teboul JL. Arterial pressure-based cardiac output in septic patients: different accuracy of pulse contour and uncalibrated pressure waveform devices. Crit Care. 2010;14(3):R109.
Monnet X, Lahner D. Can the “FloTrac” really track flow in septic patients? Intensive Care Med. 2011;37(2):183–5.
Monnet X, Anguel N, Naudin B, Jabot J, Richard C, Teboul JL. Pulse contour-derived cardiac output in septic patients: different performance of calibrated and uncalibrated devices. Crit Care. 2010;14(3):R109.
Hamzaoui O, Monnet X, Richard C, Osman D, Chemla D, Teboul JL. Effects of changes in vascular tone on the agreement between pulse contour and transpulmonary thermodilution cardiac output measurements within an up to 6-hour calibration-free period. Crit Care Med. 2008;36(2):434–40.
Kiefer N, Hofer CK, Marx G, Geisen M, Giraud R, Siegenthaler N, Hoeft A, Bendjelid K, Rex S. Clinical validation of a new thermodilution system for the assessment of cardiac output and volumetric parameters. Crit Care. 2012;16(3):R98.
Bendjelid K, Giraud R, Siegenthaler N, Michard F. Validation of a new transpulmonary thermodilution system to assess global end-diastolic volume and extravascular lung water. Crit Care. 2010;14(6):R209.
Michard F, Alaya S, Zarka V, Bahloul M, Richard C, Teboul JL. Global end-diastolic volume as an indicator of cardiac preload in patients with septic shock. Chest. 2003;124(5):1900–8.
McLuckie A, Bihari D. Investigating the relationship between intrathoracic blood volume index and cardiac index. Intensive Care Med. 2000;26(9):1376–8.
Reuter DA, Kirchner A, Felbinger TW, Weis FC, Kilger E, Lamm P, Goetz AE. Usefulness of left ventricular stroke volume variation to assess fluid responsiveness in patients with reduced cardiac function. Crit Care Med. 2003;31(5):1399–404.
Hofer CK, Ganter MT, Matter-Ensner S, Furrer L, Klaghofer R, Genoni M, Zollinger A. Volumetric assessment of left heart preload by thermodilution: comparing the PiCCO-VoLEF system with transoesophageal echocardiography. Anaesthesia. 2006;61(4):316–21.
Hofer CK, Furrer L, Matter-Ensner S, Maloigne M, Klaghofer R, Genoni M, Zollinger A. Volumetric preload measurement by thermodilution: a comparison with transoesophageal echocardiography. Br J Anaesth. 2005;94(6):748–55.
Goedje O, Seebauer T, Peyerl M, Pfeiffer UJ, Reichart B. Hemodynamic monitoring by double-indicator dilution technique in patients after orthotopic heart transplantation. Chest. 2000;118(3):775–81.
Kumar A, Anel R, Bunnell E, Habet K, Zanotti S, Marshall S, Neumann A, Ali A, Cheang M, Kavinsky C, et al. Pulmonary artery occlusion pressure and central venous pressure fail to predict ventricular filling volume, cardiac performance, or the response to volume infusion in normal subjects. Crit Care Med. 2004;32(3):691–9.
Huber W, Umgelter A, Reindl W, Franzen M, Schmidt C, von Delius S, Geisler F, Eckel F, Fritsch R, Siveke J, et al. Volume assessment in patients with necrotizing pancreatitis: a comparison of intrathoracic blood volume index, central venous pressure, and hematocrit, and their correlation to cardiac index and extravascular lung water index. Crit Care Med. 2008;36(8):2348–54.
Staub NC. Pulmonary edema: physiologic approaches to management. Chest. 1978;74(5):559–64.
Combes A, Berneau JB, Luyt CE, Trouillet JL. Estimation of left ventricular systolic function by single transpulmonary thermodilution. Intensive Care Med. 2004;30(7):1377–83.
Jabot J, Monnet X, Lamia B, Chemla D, Richard C, Teboul JL. Cardiac function index provided by transpulmonary thermodilution behaves as an indicator of left ventricular systolic function. Crit Care Med. 2009;37:2913–8.
Reuter DA, Felbinger TW, Schmidt C, Kilger E, Goedje O, Lamm P, Goetz AE. Stroke volume variations for assessment of cardiac responsiveness to volume loading in mechanically ventilated patients after cardiac surgery. Intensive Care Med. 2002;28(4):392–8.
Meybohm P, Gruenewald M, Renner J, Maracke M, Rossee S, Hocker J, Hagelstein S, Zacharowski K, Bein B. Assessment of left ventricular systolic function during acute myocardial ischemia: a comparison of transpulmonary thermodilution and transesophageal echocardiography. Minerva Anestesiol. 2011;77(2):132–41.
Trepte CJ, Eichhorn V, Haas SA, Richter HP, Goepfert MS, Kubitz JC, Goetz AE, Reuter DA. Thermodilution-derived indices for assessment of left and right ventricular cardiac function in normal and impaired cardiac function. Crit Care Med. 2011;39(9):2106–12.
Perny J, Kimmoun A, Perez P, Levy B. Evaluation of cardiac function index as measured by transpulmonary thermodilution as an indicator of left ventricular ejection fraction in cardiogenic shock. Biomed Res Int. 2014;2014:598029.
Robotham JL, Takata M, Berman M, Harasawa Y. Ejection fraction revisited. Anesthesiology. 1991;74(1):172–83.
Jozwiak M, Teboul JL, Monnet X. Extravascular lung water in critical care: recent advances and clinical applications. Ann Intensive Care. 2015;5(1):38.
Sakka SG, Ruhl CC, Pfeiffer UJ, Beale R, McLuckie A, Reinhart K, Meier-Hellmann A. Assessment of cardiac preload and extravascular lung water by single transpulmonary thermodilution. Intensive Care Med. 2000;26(2):180–7.
Berkowitz DM, Danai PA, Eaton S, Moss M, Martin GS. Accurate characterization of extravascular lung water in acute respiratory distress syndrome. Crit Care Med. 2008;36(6):1803–9.
Katzenelson R, Perel A, Berkenstadt H, Preisman S, Kogan S, Sternik L, Segal E. Accuracy of transpulmonary thermodilution versus gravimetric measurement of extravascular lung water. Crit Care Med. 2004;32(7):1550–4.
Kirov MY, Kuzkov VV, Kuklin VN, Waerhaug K, Bjertnaes LJ. Extravascular lung water assessed by transpulmonary single thermodilution and postmortem gravimetry in sheep. Crit Care. 2004;8(6):R451–8.
Tagami T, Kushimoto S, Yamamoto Y, Atsumi T, Tosa R, Matsuda K, Oyama R, Kawaguchi T, Masuno T, Hirama H, et al. Validation of extravascular lung water measurement by single transpulmonary thermodilution: human autopsy study. Crit Care. 2010;14(5):R162.
Fernandez-Mondejar E, Rivera-Fernandez R, Garcia-Delgado M, Touma A, Machado J, Chavero J. Small increases in extravascular lung water are accurately detected by transpulmonary thermodilution. J Trauma. 2005;59(6):1420–3. discussion 1424.
Garcia-Delgado M, Touma-Fernandez A, Chamorro-Marin V, Ruiz-Aguilar A, Aguilar-Alonso E, Fernandez-Mondejar E. Alveolar fluid clearance in healthy pigs and influence of positive end-expiratory pressure. Crit Care. 2010;14(2):R36.
Dres M, Teboul JL, Guerin L, Anguel N, Amilien V, Clair MP, Gruner A, Richard C, Monnet X. Transpulmonary thermodilution enables to detect small short-term changes in extravascular lung water induced by a bronchoalveolar lavage. Crit Care Med. 2014;42(8):1869–73.
Dres M, Teboul JL, Anguel N, Guerin L, Richard C, Monnet X. Extravascular lung water, B-type natriuretic peptide, and blood volume contraction enable diagnosis of weaning-induced pulmonary edema. Crit Care Med. 2014;42(8):1882–9.
Cordemans C, De Laet I, Van Regenmortel N, Schoonheydt K, Dits H, Huber W, Malbrain ML. Fluid management in critically ill patients: the role of extravascular lung water, abdominal hypertension, capillary leak, and fluid balance. Ann Intensive Care. 2012;2 Suppl 1:S1.
Jozwiak M, Silva S, Persichini R, Anguel N, Osman D, Richard C, Teboul JL, Monnet X. Extravascular lung water is an independent prognostic factor in patients with acute respiratory distress syndrome. Crit Care Med. 2013;41(2):472–80.
Tagami T, Nakamura T, Kushimoto S, Tosa R, Watanabe A, Kaneko T, Fukushima H, Rinka H, Kudo D, Uzu H, et al. Early-phase changes of extravascular lung water index as a prognostic indicator in acute respiratory distress syndrome patients. Ann Intensive Care. 2014;4:27.
Martin GS, Eaton S, Mealer M, Moss M. Extravascular lung water in patients with severe sepsis: a prospective cohort study. Crit Care. 2005;9(2):R74–82.
Sakka SG, Klein M, Reinhart K, Meier-Hellmann A. Prognostic value of extravascular lung water in critically ill patients. Chest. 2002;122(6):2080–6.
Schreiber T, Huter L, Schwarzkopf K, Schubert H, Preussler N, Bloos F, Gaser E, Karzai W. Lung perfusion affects preload assessment and lung water calculation with the transpulmonary double indicator method. Intensive Care Med. 2001;27(11):1814–8.
Phillips CR, Chesnutt MS, Smith SM. Extravascular lung water in sepsis-associated acute respiratory distress syndrome: indexing with predicted body weight improves correlation with severity of illness and survival. Crit Care Med. 2008;36(1):69–73.
Ryan D, Frohlich S, McLoughlin P. Pulmonary vascular dysfunction in ARDS. Ann Intensive Care. 2014;4:28.
Patroniti N, Bellani G, Maggioni E, Manfio A, Marcora B, Pesenti A. Measurement of pulmonary edema in patients with acute respiratory distress syndrome. Crit Care Med. 2005;33(11):2547–54.
Roch A, Michelet P, D’Journo B, Brousse D, Blayac D, Lambert D, Auffray JP. Accuracy and limits of transpulmonary dilution methods in estimating extravascular lung water after pneumonectomy. Chest. 2005;128(2):927–33.
Kuzkov VV, Suborov EV, Kirov MY, Kuklin VN, Sobhkhez M, Johnsen S, Waerhaug K, Bjertnaes LJ. Extravascular lung water after pneumonectomy and one-lung ventilation in sheep. Crit Care Med. 2007;35(6):1550–9.
Haas SA, Trepte CJ, Nitzschke R, Jurgens TP, Goepfert MS, Goetz AE, Reuter DA. An assessment of global end-diastolic volume and extravascular lung water index during one-lung ventilation: is transpulmonary thermodilution usable? Anesth Analg. 2013;117(1):83–90.
Roch A, Michelet P, Lambert D, Delliaux S, Saby C, Perrin G, Ghez O, Bregeon F, Thomas P, Carpentier JP, et al. Accuracy of the double indicator method for measurement of extravascular lung water depends on the type of acute lung injury. Crit Care Med. 2004;32(3):811–7.
Schuster DP, Anderson C, Kozlowski J, Lange N. Regional pulmonary perfusion in patients with acute pulmonary edema. J Nucl Med. 2002;43(7):863–70.
Bigatello LM, Kistler EB, Noto A. Limitations of volumetric indices obtained by trans-thoracic thermodilution. Minerva Anestesiol. 2010;76(11):945–9.
Saugel B, Phillip V, Ernesti C, Messer M, Meidert AS, Schmid RM, Huber W. Impact of large-volume thoracentesis on transpulmonary thermodilution-derived extravascular lung water in medical intensive care unit patients. J Crit Care. 2013;28(2):196–201.
Kushimoto S, Taira Y, Kitazawa Y, Okuchi K, Sakamoto T, Ishikura H, Endo T, Yamanouchi S, Tagami T, Yamaguchi J, et al. The clinical usefulness of extravascular lung water and pulmonary vascular permeability index to diagnose and characterize pulmonary edema: a prospective multicenter study on the quantitative differential diagnostic definition for acute lung injury/acute respiratory distress syndrome. Crit Care. 2012;16(6):R232.
Monnet X, Anguel N, Osman D, Hamzaoui O, Richard C, Teboul JL. Assessing pulmonary permeability by transpulmonary thermodilution allows differentiation of hydrostatic pulmonary edema from ALI/ARDS. Intensive Care Med. 2007;33(3):448–53.
Chew MS, Ihrman L, During J, Bergenzaun L, Ersson A, Unden J, Ryden J, Akerman E, Larsson M. Extravascular lung water index improves the diagnostic accuracy of lung injury in patients with shock. Crit Care. 2012;16(1):R1.
ArdsDefinitionTaskForce, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526–33.
LeTourneau JL, Pinney J, Phillips CR. Extravascular lung water predicts progression to acute lung injury in patients with increased risk. Crit Care Med. 2012;40(3):847–54.
Kushimoto S, Endo T, Yamanouchi S, Sakamoto T, Ishikura H, Kitazawa Y, Taira Y, Okuchi K, Tagami T, Watanabe A, et al. Relationship between extravascular lung water and severity categories of acute respiratory distress syndrome by the Berlin definition. Crit Care. 2013;17(4):R132.
Schuster DP. Identifying patients with ARDS: time for a different approach. Intensive Care Med. 1997;23(12):1197–203.
Perel A. Extravascular lung water and the pulmonary vascular permeability index may improve the definition of ARDS. Crit Care. 2013;17(1):108.
Monnet X, Marik PE, Teboul JL. Prediction of fluid responsiveness: an update. Ann Intensive Care. 2016;6(1):111.
Eisenberg PR, Hansbrough JR, Anderson D, Schuster DP. A prospective study of lung water measurements during patient management in an intensive care unit. Am Rev Respir Dis. 1987;136(3):662–8.
Mitchell JP, Schuller D, Calandrino FS, Schuster DP. Improved outcome based on fluid management in critically ill patients requiring pulmonary artery catheterization. Am Rev Respir Dis. 1992;145(5):990–8.
Trof RJ, Beishuizen A, Cornet AD, de Wit RJ, Girbes AR, Groeneveld AB. Volume-limited versus pressure-limited hemodynamic management in septic and nonseptic shock. Crit Care Med. 2012;40(4):1177–85.
Zhang Z, Ni H, Qian Z. Effectiveness of treatment based on PiCCO parameters in critically ill patients with septic shock and/or acute respiratory distress syndrome: a randomized controlled trial. Intensive Care Med. 2015;41(3):444–51.
Teboul JL, Monnet X, Perel A. Results of questionable management protocols are inherently questionable. Crit Care Med. 2012;40(8):2536. Author reply 2536–2537.
Huber W, Henschel B, Schmid RM, Haller B. Comments on Zhang et al.: Effectiveness of treatment based on PiCCO parameters in critically ill patients with septic shock and/or acute respiratory distress syndrome: a randomized controlled trial. Intensive Care Med. 2015;41(7):1389–90.
Belda FJ, Aguilar G, Teboul JL, Pestana D, Redondo FJ, Malbrain M, Luis JC, Ramasco F, Umgelter A, Wendon J, et al. Complications related to less-invasive haemodynamic monitoring. Br J Anaesth. 2011;106(4):482–6.
Vincent JL, Rhodes A, Perel A, Martin GS, Rocca GD, Vallet B, Pinsky MR, Hofer CK, Teboul JL, de Boode WP, et al. Clinical review: Update on hemodynamic monitoring - a consensus of 16. Crit Care. 2011;15(4):229.
Benes J, Giglio M, Brienza N, Michard F. The effects of goal-directed fluid therapy based on dynamic parameters on post-surgical outcome: a meta-analysis of randomized controlled trials. Crit Care. 2014;18(5):584.
Monnet X, Letierce A, Hamzaoui O, Chemla D, Anguel N, Osman D, Richard C, Teboul JL. Arterial pressure allows monitoring the changes in cardiac output induced by volume expansion but not by norepinephrine. Crit Care Med. 2011;39:1394–9.
Pierrakos C, Velissaris D, Scolletta S, Heenen S, De Backer D, Vincent JL. Can changes in arterial pressure be used to detect changes in cardiac index during fluid challenge in patients with septic shock? Intensive Care Med. 2012;38(3):422–8.
Perel A, Saugel B, Teboul JL, Malbrain ML, Belda FJ, Fernandez-Mondejar E, Kirov M, Wendon J, Lussmann R, Maggiorini M. The effects of advanced monitoring on hemodynamic management in critically ill patients: a pre and post questionnaire study. J Clin Monit Comput. 2016;30(5):511–8.
Cecconi M, Hofer C, Teboul JL, Pettila V, Wilkman E, Molnar Z, Della Rocca G, Aldecoa C, Artigas A, Jog S, et al. Fluid challenges in intensive care: the FENICE study: A global inception cohort study. Intensive Care Med. 2015;41(9):1529–37.
Bendjelid K, Marx G, Kiefer N, Simon TP, Geisen M, Hoeft A, Siegenthaler N, Hofer CK. Performance of a new pulse contour method for continuous cardiac output monitoring: validation in critically ill patients. Br J Anaesth. 2013;111(4):573–9.
Huber W, Phillip V, Hollthaler J, Schultheiss C, Saugel B, Schmid RM. Femoral indicator injection for transpulmonary thermodilution using the EV1000/VolumeView((R)): do the same criteria apply as for the PiCCO((R))? J Zhejiang Univ Sci B. 2016;17(7):561–7.
Levy B, Bastien O, Karim B, Cariou A, Chouihed T, Combes A, Mebazaa A, Megarbane B, Plaisance P, Ouattara A, et al. Experts’ recommendations for the management of adult patients with cardiogenic shock. Ann Intensive Care. 2015;5(1):52.
Haller M, Zollner C, Briegel J, Forst H. Evaluation of a new continuous thermodilution cardiac output monitor in critically ill patients: a prospective criterion standard study. Crit Care Med. 1995;23(5):860–6.
Balik M, Pachl J, Hendl J. Effect of the degree of tricuspid regurgitation on cardiac output measurements by thermodilution. Intensive Care Med. 2002;28(8):1117–21.
Jozwiak M, Monnet X, Cinotti R, Bontemps F, Reignier J, Belliard G. Prospective assessment of a score for assessing basic critical-care transthoracic echocardiography skills in ventilated critically ill patients. Ann Intensive Care. 2014;4:12.
Michard F. Hemodynamic monitoring in the era of digital health. Ann Intensive Care. 2016;6(1):15.
Acknowledgements
Not applicable.
Funding
Institutional.
Availability of data and materials
Not applicable.
Authors’ contributions
XM and J-LT both wrote the manuscript. Both authors read and approved the final manuscript.
Competing interests
J-LT and XM are members of the Medical Advisory Board of Pulsion Medical Systems. As consultants for this company, they have received honoraria. The company did not provide funding for the preparation of this manuscript.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Monnet, X., Teboul, JL. Transpulmonary thermodilution: advantages and limits. Crit Care 21, 147 (2017). https://doi.org/10.1186/s13054-017-1739-5
Published:
DOI: https://doi.org/10.1186/s13054-017-1739-5