
Abstract
Introduction
A new system has been developed to assess global end-diastolic volume (GEDV), a volumetric marker of cardiac preload, and extravascular lung water (EVLW) from a transpulmonary thermodilution curve. Our goal was to compare this new system with the system currently in clinical use.
Methods
Eleven anesthetized and mechanically ventilated pigs were instrumented with a central venous catheter and a right (PulsioCath; Pulsion, Munich, Germany) and a left (VolumeView™; Edwards Lifesciences, Irvine, CA, USA) thermistor-tipped femoral arterial catheter. The right femoral catheter was used to measure GEDV and EVLW using the PiCCO2™ (Pulsion) method (GEDV1 and EVLW1, respectively). The left femoral catheter was used to measure the same parameters using the new VolumeView™ (Edwards Lifesciences) method (GEDV2 and EVLW2, respectively). Measurements were made during inotropic stimulation (dobutamine), during hypovolemia (bleeding), during hypervolemia (fluid overload), and after inducing acute lung injury (intravenous oleic acid).
Results
One hundred and thirty-seven paired measurements were analyzed. GEDV1 and GEDV2 ranged from 701 to 1,629 ml and from 774 to 1,645 ml, respectively. GEDV1 and GEDV2 were closely correlated (r2 = 0.79), with mean bias of -11 ± 80 ml and percentage error of 14%. EVLW1 and EVLW2 ranged from 507 to 2,379 ml and from 495 to 2,222 ml, respectively. EVLW1 and EVLW2 were closely correlated (r2 = 0.97), with mean bias of -5 ± 72 ml and percentage error of 15%.
Conclusions
In animals, and over a very wide range of values, a good agreement was found between the new VolumeView™ system and the PiCCO™ system to assess GEDV and EVLW.
Similar content being viewed by others


Introduction
Transpulmonary thermodilution (TPTD) is increasingly used for hemodynamic evaluations in critically ill patients [1–4]. After injection of a cold indicator in the superior vena cava, TPTD allows the computation of cardiac output (CO) from a TPTD curve recorded by a thermistor-tipped femoral arterial catheter [4]. Additional physiological parameters can be derived from the dilution curve, such as global end diastolic volume (GEDV), a volumetric marker of cardiac preload [5–7], and extravascular lung water (EVLW) [7–10].
The TPTD method currently in clinical use and implemented in the PiCCO™ system (Pulsion Medical Systems, Munich, Germany) is based on mathematical models described in the 1950 s [11, 12]. A new and original method has recently been developed to derive GEDV and EVLW from a TPTD curve (VolumeView™; Edwards Lifesciences, Irvine, CA, USA). The aim of the present animal study was to compare the new VolumeView™ system with the PiCCO™ system, over a wide range up to extreme pathophysiological conditions.
Materials and methods
The study was approved for the use of swine by the Institutional Animal Care and Use Committee at the Edwards Lifesciences Biological Resource Center, and all experimentation was done in accordance with the Guide for the Care and Use of Laboratory Animals (1996; ILAR, NAP, Washington, DC, USA).
Eleven anesthetized and mechanically ventilated pigs (90 to 110 kg) were studied. Animals were premedicated with intramuscular midazolam (0.5 mg/kg) and atropine (0.5 mg) and were anesthetized with an injection of propofol (1 mg/kg) followed by continuous infusion of propofol (150 μg/kg/min) and sufentanil (2.5 μg/kg/h). After tracheal intubation, pigs were mechanically ventilated in a volume-controlled mode with a FiO2 of 50%, a respiratory rate between 12 and 16 breaths/minute (to maintain an end-expiratory partial pressure of carbon dioxide within the normal range), a positive end-expiratory pressure of 0 cmH2O and a tidal volume of 10 ml/kg.
All animals were instrumented with a right (PulsioCath™; Pulsion Medical Systems) and a left (VolumeView™; Edwards Lifesciences) 5F thermistor-tipped femoral arterial catheter. The correct position of femoral catheters was confirmed by radioscopy (Figure 1).

Transpulmonary thermodilution curve. The assessment of global end-diastolic volume (GEDV) by the PiCCO™ system is based on the mean transit time (MTt) and exponential downslope time (DSt), while the assessment of GEDV by the new VolumeView™ method is based on MTt, maximum ascending slope (S1) and maximum descending slope (S2).
All animals were also instrumented with a pulmonary artery catheter (CCComboV™, 7.5F; Edwards Lifesciences) inserted through the right jugular vein and with a central venous catheter in the left jugular vein (Figure 1). The pulmonary artery catheter was used for continuous monitoring of CO (Vigilance II; Edwards Lifesciences) and pulmonary arterial pressures during the experimental protocol. The central venous catheter was used for cold indicator injections and for central venous pressure monitoring. Pulmonary artery pressures, continuous CO and central venous pressure data were used to guide therapy at various stages (as described below) but were not recorded nor analyzed.
The current transpulmonary thermodilution system
The right femoral catheter was connected to a PiCCO2™ monitor (Pulsion Medical Systems) and used to measure CO (CO1), GEDV (GEDV1) and EVLW (EVLW1) using the following equations [1, 7, 9, 10]:
where Vi is the injectate volume, Tb is blood temperature, Ti is injectate temperature, k is a constant proportional to the specific weights and specific heat of blood and injectate, and AUC is the area under the TPTD curve.
where MTt is the mean transit time of the cold indicator and DSt is the exponential downslope time (Figure 1).
The new transpulmonary thermodilution system
The left femoral catheter was connected to the EV1000™ monitor (Edwards Lifesciences) and used to measure CO (CO2), GEDV (GEDV2) and EVLW (EVLW2). CO was derived from the dilution curve using the same Stewart Hamilton equation:
GEDV, however, was derived from a different equation as follows:
where S1 and S2 are respectively the maximum ascending and descending slopes of the thermodilution curve (Figure 1) and f is a proprietary function.
Finally, EVLW was assessed using the equation:
The same cold saline bolus injected through the central venous catheter was used to compute simultaneously the two transpulmonary curves: one with the right femoral catheter PiCCO2™ (Pulsion Medical Systems), the other with the left femoral catheter (EV1000™; Edwards Lifesciences). The average of three bolus measurements was considered for analysis and is reported in Results.
Experimental protocol
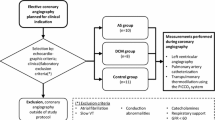
The experimental protocol is summarized in Figure 2. Measurements were performed: at baseline; during dobutamine infusion (DOBU, starting at 7.5 μg/kg/minute and titrated to induce a 30 to 50% increase in continuous CO); 5 minutes after stopping dobutamine infusion; after inducing hypovolemia (HYPO, controlled hemorrhage to decrease mean arterial pressure (MAP) around 50 mmHg); after blood restitution and fluid loading (2/3 blood + 1/3 serum saline); and after fluid overloading (HYPER, 75% serum saline + 25% gelatin in order to increase MAP up to 130 mmHg and/or central venous pressure up to 20 mmHg). At each stage, a 10-minute stabilization period was observed before doing the measurements. Finally, additional measurements were performed after inducing acute lung injury (ALI) by injecting intravenously oleic acid (O1383, 100 mg/kg/hour).

Flow chart of the experimental protocol. *Multiple measurements. IV, intravenous.
At this stage, several measurements were performed successively in order to capture high EVLW values. Oleic acid-induced pulmonary edema was confirmed by the occurrence of arterial hypoxemia (drop in PaO2/FiO2 and SaO2), a drop in the compliance of the respiratory system (increase in airway pressures while the tidal volume was maintained constant or even decreased) and lung infiltrates on chest X-ray scan (Figure 1). At this point, FiO2 and the positive end-expiratory pressure were respectively increased up to 100% and 15 cmH2O when necessary to maintain SaO2 > 90%. Oleic acid may induce a dramatic increase in pulmonary artery pressures and a decrease in CO (right ventricular failure). Phenylephrine and dobutamine were therefore also administered when necessary to maintain MAP >50 mmHg and continuous CO >5 l/minute as long as possible. When it was no longer possible to maintain SaO2 > 90% and MAP >50 mmHg, data collection was stopped and animals were sacrificed (with pentobarbital and phenytoin).
Statistical analysis
Results are expressed as the mean ± standard deviation (SD), unless specified otherwise. Percentage errors for CO, GEDV and EVLW comparisons were calculated as twice the SD of the bias over the average CO, GEDV or EVLW value, respectively [13]. All bias, SDs, limits of agreement (2SD) and percentage errors reported in the manuscript have been corrected for multiple measurements according to the method proposed by Bland and Altman [14].
Reproducibility of TPTD measurements was assessed by calculating the standard deviation/mean ratio of triplicate measurements and is expressed as a percentage. The effect of each intervention (DOBU, HYPO, HYPER, ALI) versus the previous stage was assessed using a parametric test (paired t test) or nonparametric test (paired Wilcoxon test) when appropriate. Values obtained using both methods were also compared at each stage using unpaired tests (parametric or nonparametric as appropriate).
Several measurements were performed at the latest stage (ALI) in order to capture high EVLW values. At this stage, only measurements corresponding to the maximum EVLW1 (the reference method in the present study) have been selected for comparisons with EVLW2. For the linear regression analysis, however, all measurements were taken into account. P < 0.05 was considered statistically significant.
Results
A total of 137 paired measurements were available for comparisons. Sixty-six paired measurements were collected from stages 1 to 6 (6 stages × 11 pigs) and 71 additional paired measurements (6.5 ± 2.1 per pig) were collected at the final lung injury stage. No data were discarded. The reproducibility of hemodynamic parameters is reported in Table 1.
Overall, CO1 and CO2 ranged from 3.1 to 15.4 l/minute and from 3.4 to 15.1 l/minute, respectively. CO1 and CO2 were closely correlated (r2 = 0.99), with mean bias (± SD) of 0.20 ± 0.30 l/minute and percentage error of 7% (Figure 3). GEDV1 and GEDV2 ranged from 701 to 1,629 ml and from 774 to 1,645 ml. GEDV1 and GEDV2 were closely correlated (r2 = 0.79), with mean bias of -11 ± 80 ml and percentage error of 14% (Figure 4). EVLW1 and EVLW2 ranged from 507 to 2,379 ml and from 495 to 2,222 ml. EVLW1 and EVLW2 were closely correlated (r2 = 0.97), with mean bias of -5 ± 72 ml and percentage error of 15% (Figure 5).

Cardiac output comparison. Left: correlation between cardiac output (CO) measured by the PiCCO™ system (CO1) and the VolumeView™ system (CO2). Right: Bland-Altman representation depicting the agreement between both methods. SD, standard deviation.

Global end-diastolic volume comparison. Left: correlation between global end-diastolic volume (GEDV) measured by the PiCCO™ system (GEDV1) and the VolumeView™ system (GEDV2). Right: Bland-Altman representation depicting the agreement between both methods. SD, standard deviation.

Extravascular lung water comparison. Left: correlation between extravascular lung water (EVLW) measured by the PiCCO™ system (EVLW1) and the VolumeView™ system (EVLW2). Right: Bland-Altman representation depicting the agreement between both methods. SD, standard deviation.
Changes in CO2, GEDV2, and EVLW2 were closely correlated with changes in CO1, GEDV1, and EVLW1, respectively (Figure 6).

Correlations between changes in hemodynamic parameters between the two measurement methods. Correlations between changes in cardiac output (CO), changes in global end-diastolic volume (GEDV) and changes in extravascular lung water (EVLW) measured by the PiCCO™ system (CO1, GEDV1 and EVLW1) and by the VolumeView™ system (CO2, GEDV2 and EVLW2).
The effects of each intervention are summarized in Table 2. Inotropic stimulation (DOBU) was achieved by administering an average 23 μg/kg/minute dose of dobutamine, hypovolemia (HYPO) by an average 1.2 l controlled hemorrhage, and hypervolemia (HYPER) by the average infusion of 4.5 l serum saline and 1.5 l gelatin. Both GEDV1 and GEDV2 decreased significantly during bleeding and increased significantly after blood restitution and fluid loading (Table 2). EVLW1 and EVLW2 increased slightly but significantly during fluid overload and dramatically (+110%) during ALI (Table 2). At each stage, values measured with the new VolumeView™ and with the current PiCCO™ method were comparable (Table 2).
Discussion
In animals, and over a wide range of values, the present study demonstrates that GEDV and EVLW derived from the new VolumeView™ method and from the current PiCCO™ method are interchangeable.
Both methods derive CO from the TPTD curve using the Stewart-Hamilton principles and the same equation [4] so, not surprisingly, the agreement was extremely good with a percentage error of 7%, far below the clinically acceptable threshold value of 30% proposed by Critchley and Critchley [13].
In contrast, GEDV was derived from two different equations. The PiCCO™ equation is based on time characteristics of the TPTD curve (mean transit time of the cold indicator and exponential downslope time) while the new VolumeView™ equation additionally relies on the ascending and descending slopes of the dilution curve (Figure 1). The present results show that both methods are interchangeable to assess GEDV even when significant changes in cardiac preload are induced by bleeding and fluid loading. They also confirm that GEDV is not affected by dobutamine-induced changes in CO, and hence that there is no mathematical coupling between both parameters [3, 5]. The GEDV has been shown to be a reliable indicator of cardiac preload [5], varying in the same direction as echocardiographic preload indices [6]. A goal-directed strategy based on the optimization of GEDV has been shown to be useful to improve the postoperative outcome of cardiac surgical patients [15].
Both methods were also interchangeable for the assessment of EVLW; not only during slight modifications induced by fluid overload, but also during dramatic increases related to capillary leak as those observed during the ALI phase (Table 2). Assessing EVLW may be useful for clinicians treating patients with ALI or left ventricular failure [16]. EVLW has been shown to be more sensitive and specific than chest X-ray and ALI criteria to diagnose pulmonary edema [17, 18]. EVLW is also a prognostic parameter since it has repeatedly been shown to be correlated with mortality in patients with ALI as well as in the general intensive care unit population [19–22]. Moreover, it has been suggested in critically ill patients that goal-directed strategies based on the measurement of EVLW may be associated with a decrease in the duration of mechanical ventilation and length of hospital stay [15, 23, 24].
Surprisingly, EVLW1 increased slightly but significantly during dobutamine infusion and decreased slightly but significantly during bleeding, while EVLW2 did not change (Table 2). From a pathophysiological point of view, no change in lung water is expected during inotropic stimulation or hypovolemia, particularly over such a short period of time [25]. Since our study was not designed to compare the PiCCO™ method and the VolumeView™ method with a third reference method (such as gravimetry), however, we cannot draw any definitive conclusions regarding the superiority of one method over the other.
Our study also confirms the very good reproducibility of TPTD measurements. These findings are in line with previous studies [5, 26] reporting reproducibility of CO, GEDV and EVLW of 4 to 7%, 5 to 8% and 11%, respectively.
Study limitations
The gravimetric method in animals and the double indicator (cold green dye) dilution method in humans are considered gold standard methods to quantify EVLW [9, 10]. The goal of the present study was to compare the new VolumeView™ system with the TPTD system currently in clinical use - this is why the PiCCO™ system has been selected as the reference method in our study. A clinical validation is necessary to investigate whether the new VolumeView™ system is also comparable with the PiCCO™ system in critically ill patients. The new VolumeView™ algorithm was originally developed to decrease the sensitivity of TPTD to recirculation and thermal baseline drifts. The present study was not designed to investigate this potential advantage over the existing TPTD technology, but instead to ensure that the new VolumeView™ system and the PiCCO™ system are interchangeable in clinical-like conditions where CO, blood volume and lung water vary significantly. Further studies are therefore required to compare both systems in situations where technical (thermal baseline drift) or other clinical challenges (for example, valvular regurgitation-induced recirculation) are encountered.
Conclusions
In animals, and over a very wide range of values, the new TPTD VolumeView™ system is comparable with the current PiCCO™ system to assess CO, GEDV and EVLW during inotropic stimulation, acute hemorrhage, fluid overload and severe acute lung injury.
Key messages
-
TPTD is increasingly used for hemodynamic evaluations in critically ill patients.
-
The TPTD method currently in clinical use and implemented in the PiCCO™ system (Pulsion Medical Systems) is based on mathematical models described in the 1950 s.
-
A new and original method has recently been developed to derive GEDV and EVLW from a TPTD curve (VolumeView™; Edwards Lifesciences).
-
In animals, and over a very wide range of values, the new transpulmonary thermodilution VolumeView™ system is comparable with the current PiCCO™ system to assess CO, GEDV and EVLW during inotropic stimulation, acute hemorrhage, fluid overload and severe acute lung injury.
Abbreviations
- ALI:
-
acute lung injury induced by oleic acid
- CO:
-
cardiac output
- CO1:
-
cardiac output measured by PiCCO2™
- CO2:
-
cardiac output measured by EV1000
- DOBU:
-
dobutamine infusion
- GEDV:
-
global end-diastolic volume
- GEDV1:
-
global end-diastolic volume measured by PiCCO2™
- GEDV2:
-
global end-diastolic volume measured by EV1000
- EVLW:
-
extravascular lung water
- EVLW1:
-
extravascular lung water measured by PiCCO2™
- EVLW2:
-
extravascular lung water measured by EV1000
- HYPO:
-
hypovolemia induced by bleeding
- HYPER:
-
hypervolemia induced by volume loading
- MAP:
-
mean arterial pressure
- SD:
-
standard deviation
- TPTD:
-
transpulmonary thermodilution.
References
Michard F, Perel A: Management of circulatory and respiratory failure using less invasive hemodynamic monitoring. In Yearbook of Intensive Care and Emergency Medicine. Edited by: Vincent JL. Berlin: Springer; 2003:508-520.
Isakow W, Schuster DP: Extravascular lung water measurements and hemodynamic monitoring in the critically ill: bedside alternatives to the pulmonary artery catheter. Am J Physiol Lung Cell Mol Physiol 2006, 291: L1118-L1131. 10.1152/ajplung.00277.2006
Benington S, Ferris P, Nirmalan M: Emerging trends in minimally invasive haemodynamic monitoring and optimization of fluid therapy. Eur J Anaesthesiol 2009, 26: 893-905. 10.1097/EJA.0b013e3283308e50
Reuter DA, Huang C, Edrich T, Shernan SK, Eltzschig HK: Cardiac output monitoring using indicator-dilution techniques: basics, limits, and perspectives. Anesth Analg 2010, 110: 799-811. 10.1213/ANE.0b013e3181cc885a
Michard F, Alaya S, Zarka V, Bahloul M, Richard C, Teboul JL: Global end-diastolic volume as an indicator of cardiac preload in patients with septic shock. Chest 2003, 124: 1900-1908. 10.1378/chest.124.5.1900
Hofer CK, Furrer L, Matter-Ensner S, Maloigne M, Klaghofer R, Genoni M, Zollinger A: Volumetric preload measurement by thermodilution: a comparison with transoesophageal echocardiography. Br J Anaesth 2005, 94: 748-755. 10.1093/bja/aei123
Sakka SG, Rühl CC, Pfeiffer UJ, Beale R, McLuckie A, Reinhart K, Meier-Hellmann A: Assessment of cardiac preload and extravascular lung water by single transpulmonary thermodilution. Intensive Care Med 2000, 26: 180-187. 10.1007/s001340050043
Michard F, Schachtrupp A, Toens C: Factors influencing the estimation of extravascular lung water by transpulmonary thermodilution in critically ill patients. Crit Care Med 2005, 33: 1243-1247. 10.1097/01.CCM.0000164566.23147.35
Michard F: Bedside assessment of extravascular lung water by dilution methods: temptations and pitfalls. Crit Care Med 2007, 35: 1186-1192. 10.1097/01.CCM.0000259539.49339.66
Brown LM, Liu KD, Matthay MA: Measurement of extravascular lung water using the single indicator method in patients: research and potential clinical value. Am J Physiol Lung Cell Mol Physiol 2009, 297: L547-L558.
Newman EV, Merrell M, Genecin A, Monge C, Milnor WR, McKeever WP: The dye dilution method for describing the central circulation. An analysis of factors shaping the time-concentration curves. Circulation 1951, 4: 735-746.
Meier P, Zierler KL: On the theory of the indicator-dilution method for measurement of blood flow and volume. J Appl Physiol 1954, 6: 731-744.
Critchley LA, Critchley JA: A meta-analysis of studies using bias and precision statistics to compare cardiac output measurement techniques. J Clin Monit Comput 1999, 15: 85-91. 10.1023/A:1009982611386
Bland JM, Altman DG: Agreement between methods of measurement with multiple observations per individual. J Biopharm Stat 2007, 17: 571-582. 10.1080/10543400701329422
Goepfert MSG, Reuter DA, Akyol D, Lamm P, Kilger E, Goetz A: Goal-directed fluid management reduces vasopressor and catecholamine use in cardiac surgery patients. Intensive Care Med 2007, 33: 96-103. 10.1007/s00134-006-0404-2
Michard F, Phillips C: Measuring extravascular lung water (and derived parameters) in patients with acute respiratory distress syndrome: what's right, what's wrong, and what's ahead? Crit Care Med 2009, 37: 2118-2119. 10.1097/CCM.0b013e3181a5c20f
Michard F, Zarka V, Alaya S: Better characterization of acute lung injury/ARDS using lung water. Chest 2004, 125: 1166-1167. 10.1378/chest.125.3.1166
Martin GS, Eaton S, Mealer M, Moss M: Extravascular lung water in patients with severe sepsis: a prospective cohort study. Crit Care 2005, 9: R74-R82. 10.1186/cc3025
Berkowitz DM, Danai PA, Eaton S, Moss M, Martin GS: Accurate characterization of extravascular lung water in acute respiratory distress syndrome. Crit Care Med 2008, 36: 1803-1809. 10.1097/CCM.0b013e3181743eeb
Sakka SG, Klein M, Reinhart K, Meier-Hellmann A: Prognostic value of extravascular lung water in critically ill patients. Chest 2002, 122: 2080-2086. 10.1378/chest.122.6.2080
Kuzkov VV, Kirov MY, Sovershaev MA, Kuklin VN, Suborov EV, Waerhaug K, Bjertnaes LJ: Extravascular lung water determined with single transpulmonary thermodilution correlates with the severity of sepsis-induced acute lung injury. Crit Care Med 2006, 34: 1647-1653. 10.1097/01.CCM.0000218817.24208.2E
Phillips CR, Chesnutt MS, Smith SM: Extravascular lung water in sepsis-associated acute respiratory distress syndrome: indexing with predicted body weight improves correlation with severity of illness and survival. Crit Care Med 2008, 36: 69-73. 10.1097/01.CCM.0000295314.01232.BE
Mitchell JP, Schuller D, Calandrino FS, Schuster DP: Improved outcome based on fluid management in critically ill patients requiring pulmonary artery catheterization. Am Rev Respir Dis 1992, 145: 990-998.
Eisenberg PR, Hansbrough JR, Anderson D, Schuster DP: A prospective study of lung water measurements during patient management in an intensive care unit. Am Rev Respir Dis 1987, 136: 662-668.
Nirmalan M, Willard TM, Edwards DJ, Little RA, Dark PM: Estimation of errors in determining intrathoracic blood volume using the single transpulmonary thermal dilution technique in hypovolemic shock. Anesthesiology 2005, 103: 805-812. 10.1097/00000542-200510000-00019
Gödje O, Peyerl M, Seebauer T, Dewald O, Reichart B: Reproducibility of double-indicator dilution measurements of intrathoracic blood compartments, extravascular lung water, and liver function. Chest 1998, 113: 1070-1077.
Acknowledgements
The present study was funded by Edwards Lifesciences. The study was designed and conducted, and the results analyzed, under the supervision of KB, with the support of Kate Willibyro (Edwards, Irvine, CA, USA) for data collection, Pascal Candolfi (Edwards, Nyon, Switzerland) for statistics, and Dr Michard (Edwards, Nyon, Switzerland) for design and writing. KB, RG and NS had full control of the database, which was locked before analysis, were responsible for interpretation of the results, and made the final decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
KB received consultant fees from Edwards LifeSciences. FM is a director at Edwards Lifesciences and is coinventor on transpulmonary thermodilution patents (US2005267378, US2007282213, WO2009049872). RG and NS have no potential conflicts of interest to declare.
Authors' contributions
KB and FM designed the study and wrote the article. KB was responsible for data collection and data analysis, with the help of RG and NS. All authors reviewed and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Bendjelid, K., Giraud, R., Siegenthaler, N. et al. Validation of a new transpulmonary thermodilution system to assess global end-diastolic volume and extravascular lung water. Crit Care 14, R209 (2010). https://doi.org/10.1186/cc9332
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/cc9332