
Abstract
Background
Hip fractures are an increasingly common consequence of falls in older people that are associated with a high risk of death and reduced function. The vast majority of intertrochanteric fractures require surgical treatment to withstand early mobilization and weight bearing, which prevents complications due to prolonged bed rest and aids in fracture healing.
Methods
This study is compromised by two parts, the experimental study and the clinical part. In the first part, a standard 130° nail will be used with the appropriate lag screw(s) and dynamic distal locking in synthetic osteoporotic femurs and the transmission of forces in the proximal femur, measured by a cortical surface-strain distribution, will be evaluated using digital image correlation. Finite element parametric models of the bone, the nails and their interface will be also developed. Finite element computations of surface strains in implanted femurs, after being validated against biomechanical testing measurements, will be used to assist the comparison of the nails by deriving important data on the developed stress and strain fields, which cannot be measured through biomechanical testing. In the other part, will set up a prospective, randomized, comparative clinical study among the Gamma3 and IT cephalomedullary nailing, in order to investigate if there are any statistical important differences in the main radiological measurements and functional status in closed unstable intertrochanteric fractures (A21-3) in patients aged over 70 years old at the 24-week follow-up evaluation using patient reported disease-specific outcomes.
Discussion
This study will be the first to compare clinical, radiological and biomechanical measurements of the two different cephalomedullary nails. Our main hypothesis is that the IT nail would provide better radiological outcome and probably better clinical results than the Gama3 nail.
Clinical trial registration International Standard Randomized Controlled Trial Number (ISRCTN): https://doi.org/10.1186/ISRCTN15588442, registered on 19/4/2022.
Similar content being viewed by others


Introduction
Hip fractures are an increasingly common consequence of falls in older people that are associated with a high risk of death and reduced function [1, 2]. In fact, hip fractures constitute one of the most common impairments worldwide in terms of loss in disability-adjusted years for people older than 60 years old [1, 3]. The absolute number of hip fracture hospitalizations in the US are estimated to approach 289,000 in 2030 with an expected increase to 4.5 million by the year 2050 [4, 5]. In the UK, there is an ongoing age-standardized fall of hip fractures of 0.5% per year, but it is estimated that the annual incidence will double in the next 25 years [6]. The consequences for hip fractures in elderly individuals are significant in terms of lives lost and the associated negative impacts on hip fracture patients’ functioning and quality of life [7, 8]. In a recent critical review of 38 studies by Dyer et al. [1], hip fracture survivors experienced significantly worse mobility, independence in function, health, quality of life and higher rates of institutionalization than age matched controls. Even with integrated, multidisciplinary models for the treatment of hip fragility fractures the in-hospital mortality rate was 2.4%, and the overall mortality at 1 year from the intervention 18.7%; full mobility status or a low impairment of mobility was reached 32.1% of patients [9]. The reported mortality rate at 1 year in a very recent study from the Swedish Hip Fracture Registry [10] was approximately 20% for women and 30% for men in a total population study of 289,603 first hip fractures during a 20-year-old period (1998–2017).
The vast majority of intertrochanteric fractures require surgical treatment to withstand early mobilization and weight bearing, which prevents complications due to prolonged bed rest and aids in fracture healing. The type of surgery is generally based on fracture pattern and patient characteristics and is usually carried out with Dynamic Hip Screw (DHS) devices or cephalomedullary nails (Proximal femoral nails [PFN], PFN-antirotation nails [PFNA], Gamma nails [GN], Trigen Intertan [IT] nails or other implants) [11,12,13,14,15,16]. The optimal device for surgical fixation of trochanteric fractures remains under debate [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33]. Considering the substantial burdens attributed to the management of intertrochanteric fractures, we believe that more evidence is required to evaluate the effectiveness of a single lag cephalomedullary screw vs dual integrated screw nailing for unstable intertrochanteric fractures. The aims of the present study are:
-
(a)
to perform a biomechanical testing between IT and Gamma3 in relation to axial stiffness, torsional stiffness, and failure load in unstable intertrochanteric fractures created in 4th-generation osteoporotic sawbones;
-
(b)
to create finite element parametric models of the bone, the nails and their interface; finite element predictions of surface strains in implanted femurs, after being validated against biomechanical testing measurements, will be used to assist the comparison of the nails by deriving important data on the developed stress and strain fields, which cannot be measured through biomechanical testing. Such parameters including non-central lag screw(s) position in either the anteroposterior or lateral plane and varus or valgus reduction.
-
(c)
To compare the clinical and radiological results of the two implants in a prospective, randomized clinical study in patients over 70 years old with unstable AO/OTA A2 fractures with a minimum follow-up of 6 months.
Materials and methods
Biomechanical study
Implants
The experimental work will be undertaken in the Laboratory of Technology and Strength of Materials at the Department of Mechanical Engineering and Aeronautics of Patras University. Two implant systems will be compared against biomechanical testing, the classic Gamma3 and the InterTan nail (IT).
The Gamma3®nail (Stryker, Mahwah, NJ, USA) that would be used in the current study has a length of 180 mm, 11 mm nail diameter and 130° neck-shaft angle and utilizes a single lag screw with a standard diameter of 10.5 mm. The Trigen Intertan (Smith + Nephew, Watford, UK) nail is a current generation IM device, featuring a dual lag screw configuration comprised of a 11.0 mm superior lag screw and a 7.0 mm smaller integrated screw that allows for linear compression of the fragments at the fracture site while providing high rotational stability [32, 33]. The proximal part of the nail has a trapezoid design that provides a pressfit fixation in the metaphyseal region thus positioning more material on the lateral side of the nail where tensile/stretching forces tend to be greatest. Finally, the “clothes pin” distal tip provides less rigidity to decrease the stress riser and reduce the incidence of anterior thigh pain. An 11 mm nail with a 130° neck-shaft angle will be used for the present study.
We would hypothesize that the above variations, may create differences in strain distribution and thus dissimilar biomechanical behaviors of these two nails. The main hypothesis of our biomechanical study is that the InterTan nail would provide higher stiffness and load to failure and less varus collapse in unstable intertrochanteric fractures (AO/OTA A2). The transmission of forces as measured by cortical surface-strain distribution in the proximal femur will be evaluated using digital image correlation (DIC) and classic strain gauges.
Preparation of specimens
Eight synthetic composite osteoporotic femurs of medium size (model: 3503; SawBones Worldwide, WA, USA) with 10 PCF low-density cancellous, thin-walled low-density cortical shell and 16 mm hollow canal, would be randomly assigned to two groups (n = 4 in each group) to receive either a classic Gamma3 or an IT nail. Two additional specimens will be kept intact and will be served as reference for system calibration and material properties validation. The use of sawbone models with validated mechanical properties [34,35,36] was preferred instead of cadaveric bones to eliminate size, geometry and mechanical variability between specimens thus increasing stanchness of our numerical analysis due to the availability of the finite element 3D digital file with coded material properties of our specimen (Femur, Finite Element Model of #3503, SawBones Worldwide, WA, USA).
The instrumentation of Gamma3 and IT will be applied in a standard manner, according to the manufacturer’s manual, first on the intact sawbones (prior to fracture creation) under image intensifier using antero-posterior and lateral imaging to ensure proper implant position and a tip-to-apex distance (TAD) < 20 mm (Fig. 1a–c).

a The instrumentation of Gamma3 has been applied in a standard manner, according to the manufacturer’s manual in an osteoporotic Sawbone model, first on the intact sawbones; b–d Fluoroscopic images of Gamma3 in the intact and fractured Sawbone; c–e Fluoroscopic images of InterTan in the intact and fractured Sawbone
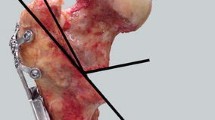
The instrumentation will be removed and the fractures would be created using an electric saw and a custom-made cutting guide. For the creation of an unstable intertrochanteric fracture (AO/OTA 31A2.2) the fracture line will be at an angle of 47° to the horizontal level running from the lesser trochanter followed by removal of an additional wedge of bone, containing the lesser trochanter. The sawbones will be re-instrumented and prepared for biomechanical testing (Fig. 1d, e).
The natural inclination of the femur at the single-leg stance, which is 11° of abduction in the frontal plane and neutral on the sagittal plane will be ensured using the surface of the posterior condyle as reference point [37] (Fig. 2a). The femurs will then be fixed distally at the supracondylar level to a custom resin mold (Smooth-Cast 300 Series) properly reinforced with an orthogonal steel plate (Fig. 2b). Standard strain gauges (model C2A-06-125LW-350, 350Ω ± 0.6%, − 50° up to + 80 °C) will be applied at the medial and lateral side of the specimen 2 cm below the fracture line as well as 2 cm below the distal interlocking screw (Fig. 2c). Finally, a thin layer of white paint with black speckles (Fig. 2d) will be applied at the proximal end of the femur to measure the transmission of forces, in the cortical surface-strain distribution using digital image correlation (DIC) (Fig. 2e).

a position of the composite femur at 11° of abduction in the frontal plane and neutral on the sagittal plane; b Fixation of the specimen distally at the supracondylar level to a custom resin mold (Smooth-Cast 300 Series); c Standard strain gauges will be applied at the medial and lateral side of the specimen 2 cm below the fracture line as well as 2 cm below the distal interlocking screw; d A thin layer of white paint with black speckles will be applied at the proximal end of the femur to measure the transmission of forces, in the cortical surface-strain distribution using DIC; e and f the biomechanical testing machine and the mode of cycling loading
Loading scheme
Once the implants were settled well and distal ends were embedded, the two groups of model bones were fixed on the biomechanical test machine (MTS 647, hydraulic wedge grip) (Fig. 2f). Initially, all specimens will be subjected to an axial pressure of 100–200 N for 10 cycles with a loading rate of 1 Hz to eliminate creeping effect.
Axial cycling load compression will be applied to simulate the stress experienced by a patient with 70 kg body weight at 4–6 weeks postoperatively [38, 39]. Firstly, the axial compression test is carried out under cyclic loading, with an initial load of 400 N, incremental load of 100 N, and maximum load set to 1400 N, divided into 10 subgroups; each subgroup will be conducted in a cycle of 10,000 times, respectively, with a loading rate of 1 Hz. After the cyclic test, the average fracture gap movements will be recorded. A torsional test will follow with the following parameters: Starting from 0°, the maximum torsion angle will be set to 3° with a loading rate of 0.1°/s. Torque at the angle of 1°, 2°, 3° will be recorded, respectively. Finally, an axial compression failure test will be performed with a loading rate of 4.6 mm/s continuously, until fatigue failure; the latter is defined as fracture gap > 20 mm, nail cutting‐out or breakage and fracture line found near the distal locking screw.
Statistical analysis
The SPSS 19.0 statistical software package will produce the statistical analysis of the study. With the aid of Shapiro–Wilk test, the normal deviation of cycles to failure, failure load and axial construct stiffness in each group will be monitored. To screen the fluctuation in the parameters of interest, the Levene test will be utilized. Any major difference between the two implants will be registered with paired-samples t test, while we set a p = 0.05 as level of significance.
Finite element analysis (FEA)
Finite element analysis of the implanted sawbones will be performed using the ANSYS v.19.2 commercial FE code (ANSYS inc. Cannonsburg, Pennsylvania, USA). The femoral geometry model will be obtained by the manufacturer (3D CAD digital file with coded material properties, Sawbones, Vashon Island, Washington, USA). The geometrical features of each implant (Gamma3 and IT) will be characterized following 3D CT scanning. Only the basic geometrical features will be modeled using FEA, since it has been recognized that several additional details (i.e., threads of the lag screw(s) or distal interlocking screw) significantly complicate the analysis, without affecting considerably the computed stress and strain fields [40].
Sawbones geometry will be imported in the ANSYS FE code and the fracture plane will be modelled by creating a proper surface that divide the cortical and cancellous volumes of the bone for the unstable fracture cases. The native neck shaft angle and the anatomic reduction angle will be 135°. A central position of the hip screw with a TAD of 16–18 mm and a minimum of 2 mm width of cancellous bone between the hip screw and the femoral cortex will be applied. Several FEA models will be created with the aim to study different scenarios of reduction (in varus or valgus) as well as inappropriate lag screw positions as illustrated in Fig. 3. Our hypothesis is that even with inappropriate reduction or lag screw(s) mispositioning the biomechanical properties of IT will be better than Gamma3.

Several FEA models will be created with the aim to study different scenarios of reduction (in varus or valgus) as well as inappropriate lag screw positions
As has been proposed in a similar study [40], the developed geometries will be meshed using tetrahedral elements with an optimal element size of 3 mm as this leads to acceptable results regarding accuracy, without significantly increasing the computational cost. Appropriate linear elastic, isotropic and homogeneous material properties will be assigned to the several parts of the FE model, based on the data provided by the manufacturers. The longitudinal Young’s modulus for the cortical bone (82 pcf fiber filled epoxy) is Ecortical = 5.2 GPa, and for the cancellous bone (10 pcf solid foam) Ecancellous = 58 MPa, while for the Gamma3 and IT the titanium alloy the Young’s modulus is Ematerial = 116 GPa. For the modeling of the distal femoral fixation during the experiments, fully fixed boundary conditions will be applied on the FE models surface nodes situated at the lower 130 mm of the femur model. A constant vertical force of 1000 N will be applied on the top of the femoral head; as a linear-elastic FE analysis will be considered, the calculated results will be derived for other load values using linear interpolation or extrapolation. Linear regression modeling will be utilized in order to associate a set of independent variables or predictors (implant type, lag screw(s) positioning and reduction angle) with any measurement outcome, also referred to as the dependent variable or target, separately. For each model, the beta estimates and the p values will be returned, among others. Statistical significance was taken when p < 0.05.
Clinical study
Design
This study will be a prospective, randomized clinical trial to compare the clinical and radiological outcome between single screw cephalomedullary nailing (Gamma3) and integrated dual interlocking nailing (InterTan-IT) for the treatment of unstable (31A21–3) intertrochanteric fractures. The paper complies with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) 2013 Statement for reporting of clinical trial protocols. The study is sponsored by the University of Patras Research Committee (ELKE) (University of Patras Campus, Rio, Greece). Ethical approval has been already acquired by the Ethics Committee of the University Hospital of Patras (approval number: 3373/7-2-2022) and the patients’ written consent will be obtained before participating in the study. The study is listed with the International Standard Randomized Controlled Trial Number (ISRCTN): https://doi.org/10.1186/ISRCTN15588442 (registered on 19/4/2022).
Primary objective
The primary aim of this study is to investigate if there are any significant differences in the main radiological measurements (cut-out, varus displacement, loss of reduction, malunion, nonunion) between Gamma3 and IT in closed unstable intertrochanteric fractures (31A21–3) in patients aged over 70 years old at the 24-week follow-up evaluation.
The second primary aim would be the functional status at the 24-week follow-up using patient reported disease-specific scores (Harris Hip score HHS-and Oxford hip score-OHS).
Secondary objectives (Table 1)
Several secondary objectives will also be studied to evaluate the effectiveness and safety of the devices by quantifying and drawing presumptions from observed differences between treatment groups in the following:
-
(a)
Comparison of perioperative and intraoperative surgical data (age-adjusted Carlson Comorbidity Index [41], operation time, fluoroscopy time and dosage, blood loss, length of hospital stay, prescription of pain-killers, osteoporosis assessment using postoperative DEXA of the unaffected hip, union time and intraoperative surgeon related complications, including lag screw malposition, propagation of the fracture, non-anatomical reduction, varus/valgus deformity, rotational deformity and tip-apex distance-TAD).
-
(b)
Pain level at the perioperative period and at 6-, 12-, and 24-weeks postoperatively using the visual analogue scale (VAS) Pain Score.
-
(c)
Patient reported general health status prior to surgery and at 6-, 12- and 24-weeks post-surgery using the SF-36 form, the EQ-5D-3L Questionnaire, the SARC-F Index and the Elderly Mobility Scale (EMS).
Patient selection
The patients that will take part in the study, are those over 70 years old, admitted in the Orthopaedic Clinic of the University Hospital of Patras, Greece, suffering from a closed unstable (31A21–3) intertrochanteric fracture. Those patients will be randomized in two groups (Gamma3 and IT). The pre-operative data will be comprised of demographic information, radiological examination of the hips and other questionnaires to conclude the overall physical health and mobility prior the fracture. The participants will be free to withdraw from the study or the investigator can withdraw a patient. If a participant withdraws, they will be listed to a “Change of Status” form and will be invited to present for an endpoint follow-up (Fig. 4).

Flowchart of the clinical study
Eligibility criteria
-
1.
Closed intertrochanteric fracture (AO/OTA:31A2).
-
2.
Age over 70 years.
-
3.
Presentation to hospital within 7 days of injury.
-
4.
No concomitant injuries or prior operations to the unaffected hip.
Exclusion criteria
-
1.
Concomitant injuries affecting treatment or rehabilitation of the affected limb.
-
2.
Associated neurovascular injuries requiring immediate surgery.
-
3.
Patients with limited Greek proficiency including family members.
-
4.
Patients where consent is refused.
-
5.
Patients with severe dementia, non-ambulated and with severe associated diseases prohibiting operative intervention.
Sample size
This study will use two primary clinical outcome measures namely the Oxford Hip Score and the Harris Hip Score. The minimum clinically important differences (MCIDs) for the HHS have been estimated between 7 and 10, whereas for the OHS between 5 and 7. The aim will be to recruit 78 patients in each group as this will provide sufficient participants to obtain a power of 90% for both primary clinical outcome measures. With an allowance for 15% drop-out, the total number of patients required will be 194 (97 in each group). If recruitment proves to be problematic during the course of the trial, then the target will be lowered and the more usual 80% power level will be considered sufficient. For this scenario, the total number of patients required will be 140 (including 15% for drop-out).
Randomization
Randomization sequence will be created using Stata 9.0 (StataCorp, College Station, TX) statistical software and will be stratified with a 1:1 allocation ratio using random block sizes of 2, 4, and 6. An investigator not involved in the main study will perform the randomization process. These data will be stored on computer and will be available at the day of the intervention.
Concealment mechanism
For each surgical session patient details and the randomized treatment will be sealed in an opaque envelope that will be given to the coordinated nurse just before the start of the intervention. The patients, relatives, investigators, nurses, and all relevant personnel would be blinded to the indented treatment. The envelope will be opened by the coordinated nurse after the patient is sedated and placed to the radiological table, the hip is properly prepared and the surgeons are ready to apply the intervention. Both instrumentations for Gamma3 or IT would be available at the operative room. After opening the envelope, the procedure will be unblinded for all participants.
Surgical intervention
The patients for the study will be randomly divided in two groups. Group A: Gamma3 nail (Stryker) and Group B: InterTan (IT) nail (Smith & Nephew). The surgery will take place in one specific operating room with the standardized surgical technique, using the same c-arm for the intra-operative radiological evaluation. Anatomical reduction of the fracture will be intended in all cases prior to nail insertion. If this is not possible, several techniques of closed or open reduction will be applied in order to achieve an acceptable fixation of the fracture. The patients’ position will be on the traction table, using a minimal approach. The lag screw(s) in both groups will be put in the center of the femoral head in the lateral and anteroposterior X-ray view, while the Tip to Apex Distance (TAD) will be approximately 20 mm. All participants in both groups will receive the same physical therapy and adequate anti-osteoporotic treatment.
Radiographic evaluation
A standard technique will be kept, in order to have the same parameters in all radiographs. For the antero-posterior ones of the pelvis, both legs of the patients will be rotated inwards 15°. The radiographic measurements will be monitored by two distinguished examiners through RadiAnt DICOM Viewer. Intra-class correlation coefficients (ICC) will check the inter- and intra-rater reliability. The parameters that will be radiographically evaluated are the TAD, the position of the chephalomedulary nail in the femur head and the alignment [42]. Moreover, throughout the follow-up the varus malalignment of the implant will be assessed, as well as the cut-out of the nail and the percentage of nonunion or malunion. Varus collapse is a rotation of the proximal part of the femur anteriorly for at least 3°.
Outcome assessment
-
Patient reported general health status prior to surgery and at 6-, 12- and 24-weeks post-surgery using the SF-36 form, the EQ-5D-3L Questionnaire, the SARC-F Index and the Elderly Mobility Scale (EMS).
-
Pain level at the perioperative period and at 6, 12 and 24 weeks postoperatively using the visual analogue scale (VAS) Pain Score.
-
Comparison of perioperative and intraoperative surgical data (delay for surgery, age-adjusted Carlson Comorbidity Index, operation time, fluoroscopy time and dosage, blood loss, length of hospital stay, prescription of pain-killers, osteoporosis assessment using postoperative DEXA of the unaffected hip, union time and intraoperative surgeon related complications, including lag screw malposition, propagation of the fracture, non-anatomical reduction, varus/valgus deformity, rotational deformity and tip-apex distance (TAD) using postoperative CT of the pelvis).
-
Patients’ functional status at 24-week follow-up using the patient reported disease-specific scores (Harris Hip score HHS and Oxford hip score-OHS).
Follow-up assessments
All the patients should undergo a clinical and radiological follow-up at 6-, 12- and 24 weeks postoperatively. The follow-up will be concluded by antero-posterior radiographs of the pelvis, lateral radiography of the treated hip and questionnaire like HHS, OHS, SF-36, EQ-5D-3L, EMS, Sarc-f, NPRS scale and Vas score.
Statistical analysis
The primary outcome measure of device radiological failure is considered a binary outcome (device failed/did not fail). A binary logistic regression model will be performed to assess the association between the outcome of device failure and the predictor of device type (Gamma3, Intertan). The complication rate of G3 versus InterTan at 24 weeks post-operatively would be compared using a chi-squared (at the 5% level). The differences between HHS and OHS between groups will be assessed using an independent samples t test at 24 weeks postoperatively at the 5% level. Test levels, will be adjusted using the methods of Holm-Bonferroni to allow for the multiple comparisons. A linear regression analysis will also be used to quantify the effects of the treatment groups on each of the primary outcome measures, after adjusting for the effects of a range of other important, potentially confounding, factors (e.g. age, gender) recorded for each patient.
Discussion
Since the 1960s, the DHS has become the standard implant for surgical treatment of stable intertrochanteric fractures as it allows controlled fracture compression but despite additional modifications, such as trochanteric support plates and antirotational screws, unstable trochanteric fractures are less successfully treated by this method [17,18,19,20]. Cephalomedullary nails can provide better lateral wall support in more complex fracture patterns but nevertheless, cut-out of the hip screw has been described as the most frequent mechanical failure for all implants [21,22,23]. Several studies have shown that the incidence of cut-out for different compression hip screws and cephalomedullary nails ranges from 0 to 16.5% [24,25,26]. In a recent study by Bojan et al. [27] the primary cut-out rate of Gamma-nail in 3066 consecutive patients was 1.85% and was strongly associated either with unstable fractures involving the trochanteric and cervical regions or the combination of both, non-anatomical reduction and non-optimal screw position which are the only two factors that can be controlled by the surgeon. Recent developments including locking plates, antirotational screws and cement-augmented fixation techniques indicate that the problem of fixation failure is still unresolved [28,29,30,31].
The Trigen Intertan (IT) nail (Smith and Nephew) is a current generation IM device, featuring a configuration comprised of a larger superior lag screw and a smaller integrated screw that allows for linear compression of the fragments at the fracture site while providing high rotational stability [32, 33]. Clinical studies evaluating the IT nail against other single screw intramedullary or extramedullary devices have shown controversial results, either similar regarding Harris Hip Score, operation time, blood loss, time to union, mean hospital stay, union problems and perioperative complications [43, 44], inferior, comparing surgical time, blood loss, fluoroscopy usage and intraoperative complications [45,46,47], or superior in terms of implant failure, mal-union, lag screw cut-out, short term reduction of pain, functional outcomes and uncontrolled varus fracture collapse [33, 48,49,50].
The aim of this study is to perform a comparative biomechanical testing between a commonly used single screw cephalomedullary nail (Gamma3) and an integrated dual lag screw nail (InterTan) in unstable (AO A21–3) intertrochanteric fractures created on osteoporotic composite femurs. We would hypothesize that the InterTan nail would provide higher stiffness and load to failure and less varus collapse in unstable intertrochanteric fractures after cycling loading. Finite element parametric models of different screw positioning in both implants would be probably reveal the reasons for early or late mechanical complications and implant failures. A prospective, randomized, 2-arm, parallel clinical study will follow including approximately 200 patients. The primary aim would be the differences in radiological measurements (cut-out, varus displacement, loss of reduction, malunion, nonunion) between Gamma3 and IT in closed unstable intertrochanteric fractures (AO A21–3) in patients aged over 70 years old at the 24-week follow-up evaluation. The second primary aim would be the functional status at the 24-week follow-up using patient reported disease-specific scores (HHS and OHS) along with several other perioperative and postoperative data, level of pain and general health status (SF-36, EQ-5D-3L, SARC-F Index and Elderly Mobility Scale).
Recent systematic reviews and metanalyses have reported controversial results regarding the superiority of InterTan to other single or double lag crew cephalomedullary nailing systems. Ma et al. [13] demonstrated that IT was not found to be superior to 1-screw nailing system (Gamma3, PFNA) in terms of Harris Hip Score (HHS), blood loss, total complications, union time, length of hospital stay, revision rate, and fluoroscopy time; in contrast IT showed less implant cut-out rate and femoral fractures when compared with the control groups. The authors concluded that since IT shows similar functional recovery, revision rate and longer surgery time, it is not worthy of being recommended as an alternative intramedullary nail in intertrochanteric fractures.
Nerhera et al. [51] found that InterTan was clinically more effective when compared to a single screw cephalomedullary nail (PFNA) resulting in fewer complications, fewer revisions and fewer patients complaining of pain. No difference has been established regarding non-unions and Harris Hip Score. Intraoperative outcomes favour PFNA with less blood loss and fluoroscopy usage. The authors concluded that further studies are warranted to explore the cost-effectiveness of these and other implants in managing patients with intertrochanteric fractures.
Date et al. [52] showed that PFNA and Gamma3 had better intraoperative outcomes compared with IT; however, IT had superior implant-related outcomes of cut-out and screw migration. No difference was found between IT and PFNA or Gamma3 in Harris Hip Scores, time to union, malunion and nonunion. The authors suggested that further long-term studies are needed to evaluate clinical outcomes and cost–effectiveness of these cephalomedullary devices.
Onggo et al. [53], reported that InterTan was associated with lower complication rates in terms of all-cause revisions, cut-outs, medial or lateral screw as well as persistent hip and thigh pain. In terms of perioperative parameters, InterTan was associated with longer operative and fluoroscopy times. There was no statistically significant difference in terms of clinical Harris Hip Score and radiological outcomes, non-union, haematoma, femoral fractures, varus collapse, length of stay and mean intraoperative blood loss between the 2 groups. The authors concluded that integrated dual lag screw cephalomedullary nails are associated with fewer revisions and complications but there is insufficient data to suggest that either nail construct is associated with better functional outcomes.
Finally, Quartley et al. [54] in their recent metanalysis of 23 studies (17 with unstable fractures) found that IntetTan reduced the risk of revision/reoperation by 64%, implant failures by 62% and hip and thigh pain by 50% in unstable fractures. No differences were noted between IM nail designs for infection rates, healing time, non-union rates, femoral shortening, or Harris Hip Score. The authors concluded that IT nail may reduce incidence of implant-related complications, hip and thigh pain, and the need for revision/reoperation without compromising clinical and functional outcomes.
Limitations
Our study has several limitations. Firstly, the surgery will be performed by several orthopedic surgeons of our department that have different surgical experience, but they all were trained at the same hospital and the reduction will be closed monitored to be as anatomical as possible. Second, the assessment of fracture healing, cut-out, varus displacement and other complications will be measured with digitalized radiographs that can be misinterpreted by wrong patient positioning and intraobserver variability. Third, there are many factors contributing to fracture healing and regain of functional status that are mostly patient depended, especially in these fragile population of > 70 years old. The main weaknesses of the biomechanical study are its static nature and uniplanar loading configuration. Mechanical failure is a dynamic event in clinical practice, and rotational displacement is equally important to frontal plane displacement postoperatively. However, the current study will test the initial loading characteristics of various lag screw(s) configurations at subcritical stress levels and can serve both as a guide at events at early postoperative ambulation status and as a reference for future dynamic studies with more complex loading characteristics.
Conclusions
Despite recent advances in the treatment of intertrochanteric fractures, the surgeon related parameters (type of reduction, implant selection and optimal surgical technique) remain the most important factors for a successful clinical and radiological outcome. Taking into consideration the increased health risks related to the treatment of mechanical complications alongside the increased hospitalization and health care costs in the setting of an aging European population, the need to improve treatment outcomes of these fractures is evident. This entails both enhancing our understanding of the prognostic factors of mechanical failure and improving all aspects of intertrochanteric fracture treatment through the optimization of the biomechanical behavior of the fracture-osteosynthesis model by the application of the ideal reduction angle and implant; this is expected to have a positive effect on the rate of mechanical failure and, subsequently, the healing rates, morbidity, and mortality in this fragile patient group.
Availability of data and materials
The primary investigators are responsible for data storage and availability upon request.
References
Dyer SM, Crotty M, Fairhall N, et al. A critical review of the long-term disability outcomes following hip fracture. BMC Geriatr. 2016;16(1):158. https://doi.org/10.1186/s12877-016-0332-0.
Maffulli N, Aicale R. Proximal femoral fractures in the elderly: a few things to know, and some to forget. Medicina (Kaunas). 2022;58(10):1314. https://doi.org/10.3390/medicina58101314.
Karagiannis A, Papakitsou E, Dretakis K, et al. Mortality rates of patients with a hip fracture in a southwestern district of Greece: ten-year follow-up with reference to the type of fracture. Calcif Tissue Int. 2006;78(2):72–7. https://doi.org/10.1007/s00223-005-0169-6.
Stevens JA, Rudd RA. The impact of decreasing U.S. hip fracture rates on future hip fracture estimates. Osteoporos Int. 2013;24(10):2725–8. https://doi.org/10.1007/s00198-013-2375-9.
Veronese N, Maggi S. Epidemiology and social costs of hip fracture. Injury. 2018;49(8):1458–60. https://doi.org/10.1016/j.injury.2018.04.015.
White SM, Griffiths R. Projected incidence of proximal femoral fracture in England: a report from the NHS hip fracture anaesthesia network (HIPFAN). Injury. 2017;42:1230–3. https://doi.org/10.1016/j.injury.2010.11.010.
Chen YP, Kuo YJ, Hung SW, et al. Loss of skeletal muscle mass can be predicted by sarcopenia and reflects poor functional recovery at one year after surgery for geriatric hip fractures. Injury. 2021;52(11):3446–52. https://doi.org/10.1016/j.injury.2021.08.007.
Quaranta M, Miranda L, Oliva F, Migliorini F, Pezzuti G, Maffulli N. Haemoglobin and transfusions in elderly patients with hip fractures: the effect of a dedicated orthogeriatrician. J Orthop Surg Res. 2021;16(1):387. https://doi.org/10.1186/s13018-021-02524-0.
Civinini R, Paoli T, Cianferotti L, et al. Functional outcomes and mortality in geriatric and fragility hip fractures-results of an integrated, multidisciplinary model experienced by the “Florence hip fracture unit.” Int Orthop. 2019;43(1):187–92. https://doi.org/10.1007/s00264-018-4132-3.
Meyer AC, Ek S, Drefahl S, Ahlbom A, Hedström M, Modig K. Trends in hip fracture incidence, recurrence, and survival by education and comorbidity: a Swedish register-based study. Epidemiology. 2021;32(3):425–33. https://doi.org/10.1097/EDE.0000000000001321.
Papasimos S, Koutsojannis CM, Panagopoulos A, Megas P, Lambiris E. A randomised comparison of AMBI, TGN and PFN for treatment of unstable trochanteric fractures. Arch Orthop Trauma Surg. 2005;125(7):462–8. https://doi.org/10.1007/s00402-005-0021-5.
Socci AR, Casemyr NE, Leslie MP, Baumgaertner MR. Implant options for the treatment of intertrochanteric fractures of the hip: rationale, evidence, and recommendations. Bone Joint J. 2017;99-B(1):128–33. https://doi.org/10.1302/0301-620X.99B1.BJJ-2016-0134.R1.
Ma KL, Wang X, Luan FJ. Proximal femoral nails antirotation, gamma nails, and dynamic hip screws for fixation of intertrochanteric fractures of femur: a meta-analysis. Orthop Traumatol Surg Res. 2014;100(8):859–66. https://doi.org/10.1016/j.otsr.2014.07.023.
Arirachakaran A, Amphansap T, Thanindratarn P, Piyapittayanun P, Srisawat P, Kongtharvonskul J. Comparative outcome of PFNA, gamma nails, PCCP, Medoff plate, LISS and dynamic hip screws for fixation in elderly trochanteric fractures: a systematic review and network meta-analysis of randomized controlled trials. Eur J Orthop Surg Traumatol. 2017;27(7):937–52. https://doi.org/10.1007/s00590-017-1964-2.
Gargano G, Poeta N, Oliva F, Migliorini F, Maffulli N. Zimmer natural nail and ELOS nails in pertrochanteric fractures. J Orthop Surg Res. 2021;16(1):509. https://doi.org/10.1186/s13018-021-02634-9.
Marsillo E, Pintore A, Asparago G, Oliva F, Maffulli N. Cephalomedullary nailing for reverse oblique intertrochanteric fractures 31A3 (AO/OTA). Orthop Rev (Pavia). 2022;14(6):38560. https://doi.org/10.52965/001c.38560.
Parker MJ, Handoll HH. Gamma and other cephalocondylic intramedullary nails versus extramedullary implants for extracapsular hip fractures in adults. Cochrane Database Syst Rev. 2010;9:CD000093. https://doi.org/10.1002/14651858.CD000093.pub3.
Barton TM, Gleeson R, Topliss C, Greenwood R, Harries WJ, Chesser TJ. A comparison of the long gamma nail with the sliding hip screw for the treatment of AO/OTA 31–A2 fractures of the proximal part of the femur: a prospective randomized trial. J Bone Jt Surg Am. 2010;92(4):792–8. https://doi.org/10.2106/JBJS.I.00508.
Li AB, Zhang WJ, Wang J, Guo WJ, Wang XH, Zhao YM. Intramedullary and extramedullary fixations for the treatment of unstable femoral intertrochanteric fractures: a meta-analysis of prospective randomized controlled trials. Int Orthop. 2017;41(2):403–13. https://doi.org/10.1007/s00264-016-3308-y.
Selim A, Ponugoti N, Naqvi AZ, Magill H. Cephalo-medullary nailing versus dynamic hip screw with trochanteric stabilisation plate for the treatment of unstable per-trochanteric hip fractures: a meta-analysis. J Orthop Surg Res. 2021;16(1):47. https://doi.org/10.1186/s13018-020-02193-.
Caruso G, Bonomo M, Valpiani G, et al. A six-year retrospective analysis of cut-out risk predictors in cephalomedullary nailing for pertrochanteric fractures: Can the tip-apex distance (TAD) still be considered the best parameter? Bone Jt Res. 2017;6(8):481–8. https://doi.org/10.1302/2046-3758.68.BJR-2016-0299.R1.
Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am. 1995;77(7):1058–64. https://doi.org/10.2106/00004623-199507000-00012.
Lang NW, Arthold C, Joestl J. Does an additional antirotation U-Blade (RC) lag screw improve treatment of AO/OTA 31 A1–3 fractures with gamma 3 nail? Injury. 2016;47(12):2733–8. https://doi.org/10.1016/j.injury.2016.10.032.
Tsai SW, Lin CJ, Tzeng YH, et al. Risk factors for cut-out failure of Gamma3 nails in treating unstable intertrochanteric fractures: an analysis of 176 patients. J Chin Med Assoc. 2017;80(9):587–94. https://doi.org/10.1016/j.jcma.2017.04.007.
Caruso G, Andreotti M, Pari C, Soldati F, Gildone A, Lorusso V. Can TAD and CalTAD predict cut-out after extra-medullary fixation with new generation devices of proximal femoral fractures? A retrospective study. J Clin Orthop Trauma. 2017;8(1):68–72. https://doi.org/10.1016/j.jcot.2016.09.009.
Murena L, Moretti A, Meo F, Saggioro E, Barbati G, Ratti C, et al. Predictors of cut-out after cephalomedullary nail fixation of pertrochanteric fractures: a retrospective study of 813 patients. Arch Orthop Trauma Surg. 2018;138(3):351–9. https://doi.org/10.1007/s00402-017-2863-z.
Bojan AJ, Beimel C, Taglang G, Collin D, Ekholm C, Jönsson A. Critical factors in cut-out complication after Gamma Nail treatment of proximal femoral fractures. BMC Musculoskelet Disord. 2013;14:1. https://doi.org/10.1186/1471-2474-14-1.
Georgiannos D, Lampridis V, Bisbinas I. Complications following treatment of trochanteric fractures with the Gamma3 Nail: Is the latest version of gamma nail superior to its predecessor? Surg Res Pract. 2014. https://doi.org/10.1155/2014/143598.
Neuerburg C, Mehaffey S, Gosch M, Böcker W, Blauth M, Kammerlander C. Trochanteric fragility fractures: treatment using the cement-augmented proximal femoral nail antirotation. Oper Orthop Traumatol. 2016;28(3):164–76. https://doi.org/10.1007/s00064-016-0449-5.
Kouzelis A, Kravvas A, Mylonas S, Giannikas D, Panagopoulos A. Double axis cephalocondylic fixation of stable and unstable intertrochanteric fractures: early results in 60 cases with the Veronail system. Open Orthop J. 2014;8:60–8. https://doi.org/10.2174/1874325001408010060.
He S, Yan B, Zhu J, Huang X, Zhao J. High failure rate of proximal femoral locking plates in fixation of trochanteric fractures. J Orthop Surg Res. 2018;13(1):248. https://doi.org/10.1186/s13018-018-0951-6.
Knobe M, Gradl G, Buecking B, et al. Locked minimally invasive plating versus fourth generation nailing in the treatment of AO/OTA 31A2.2 fractures: a biomechanical comparison of PCCP(®) and Intertan nail(®). Injury. 2015;46:1475–82. https://doi.org/10.1016/j.injury.2015.05.011.
Serrano R, Blair JA, Watson DT, et al. Cephalomedullary nail fixation of Intertrochanteric femur fractures: Are two proximal screws better than one? J Orthop Trauma. 2017;31:577–82. https://doi.org/10.1097/BOT.0000000000000967.
Cristofolini L, Viceconti M, Cappello A, Toni A. Mechanical validation of whole bone composite femur models. J Biomech. 1996;29(4):525–35. https://doi.org/10.1016/0021-9290(95)00084-4.
Gardner MP, Chong AC, Pollock AG, Wooley PH. Mechanical evaluation of large size fourth-generation composite femur and tibia models. Ann Biomed Eng. 2010;38(3):613–20. https://doi.org/10.1007/s10439-009-9887-7.
Lamb JN, Coltart O, Adekanmbi I, Pandit HG, Stewart T. Comparison of axial rotational postoperative periprosthetic fracture of the femur in composite osteoporotic femur versus human cadaveric specimens: a validation study. Proc Inst Mech Eng H. 2022;236(7):973–8. https://doi.org/10.1177/09544119221092842.
Ruff CB, Hayes WC. Cross-sectional geometry of Pecos Pueblo femora and tibiae—a biomechanical investigation: I. Method and general patterns of variation. Am J Phys Anthropol. 1983;60(3):359–81. https://doi.org/10.1002/ajpa.1330600308.
Rupprecht M, Grossterlinden L, Ruecker AH, et al. A comparative biomechanical analysis of fixation devices for unstable femoral neck fractures: the Intertan versus cannulated screws or a dynamic hip screw. J Trauma. 2011;71(3):625–34. https://doi.org/10.1097/TA.0b013e31820e86e6.
Luo W, Fu X, Ma JX, Huang JM, Wu J, Ma XL. Biomechanical comparison of INTERTAN nail and Gamma3 nail for intertrochanteric fractures. Orthop Surg. 2020;12(6):1990–7. https://doi.org/10.1111/os.12853.
Kyriakopoulos G, Panagopoulos A, Pasiou E, et al. Optimizing fixation methods for stable and unstable intertrochanteric hip fractures treated with sliding hip screw or cephalomedullary nailing: a comparative biomechanical and finite element analysis study. Injury. 2022;53(12):4072–85. https://doi.org/10.1016/j.injury.2022.10.006.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–83. https://doi.org/10.1016/0021-9681(87)90171-8.
Kaynak G, Ünlü MC, Güven MF, et al. Intramedullary nail with integrated cephalocervical screws in the intertrochanteric fractures treatment: position of screws in fracture stability. Ulus Travma Acil Cerrahi Derg. 2018;24(3):268–73. https://doi.org/10.5505/tjtes.2017.96933.
Matre K, Vinje T, Havelin LI, et al. TRIGEN INTERTAN intramedullary nail versus sliding hip screw: a prospective, randomized multicenter study on pain, function, and complications in 684 patients with an intertrochanteric or subtrochanteric fracture and one year of follow-up. J Bone Jt Surg Am. 2013;95(3):200–8. https://doi.org/10.2106/JBJS.K.01497.
Liu W, Liu J, Ji G. Comparison of clinical outcomes with proximal femoral nail anti-rotation versus InterTAN nail for intertrochanteric femoral fractures: a meta-analysis. J Orthop Surg Res. 2020;15(1):500. https://doi.org/10.1186/s13018-020-02031-8.
Zhao F, Guo L, Wang X, Zhang Y. Benefit of lag screw placement by a single- or two-screw nailing system in elderly patients with AO/OTA 31–A2 trochanteric fractures. J Int Med Res. 2021;49(3):3000605211003766. https://doi.org/10.1177/03000605211003766.
Wu D, Ren G, Peng C, Zheng X, Mao F, Zhang Y. InterTan nail versus Gamma3 nail for intramedullary nailing of unstable trochanteric fractures. Diagn Pathol. 2014;9:191. https://doi.org/10.1186/s13000-014-0191-y.
Zehir S, Şahin E, Zehir R. Comparison of clinical outcomes with three different intramedullary nailing devices in the treatment of unstable trochanteric fractures. Ulus Travma Acil Cerrahi Derg. 2015;21(6):469–76. https://doi.org/10.5505/tjtes.2015.28227.
Gavaskar AS, Tummala NC, Srinivasan P, Gopalan H, Karthik BSS. Helical blade or the integrated lag screws: a matched pair analysis of 100 patients with unstable trochanteric fractures. J Orthop Trauma. 2018;32(6):274–7. https://doi.org/10.1097/BOT.0000000000001145.
Berger-Groch J, Rupprecht M, Schoepper S, Schroeder M, Rueger JM, Hoffmann M. Five-year outcome analysis of intertrochanteric femur fractures: a prospective randomized trial comparing a 2-screw and a single-screw cephalomedullary nail. J Orthop Trauma. 2016;30(9):483–8. https://doi.org/10.1097/BOT.0000000000000616.
Seyhan M, Turkmen I, Unay K, Ozkut AT. Do PFNA devices and Intertan nails both have the same effects in the treatment of trochanteric fractures? A prospective clinical study. J Orthop Sci. 2015;20(6):1053–61. https://doi.org/10.1007/s00776-015-0750-4.
Nherera L, Trueman P, Horner A, Watson T, Johnstone AJ. Comparison of a twin interlocking derotation and compression screw cephalomedullary nail (InterTAN) with a single screw derotation cephalomedullary nail (proximal femoral nail antirotation): a systematic review and meta-analysis for intertrochanteric fractures. J Orthop Surg Res. 2018;13(1):46. https://doi.org/10.1186/s13018-018-0749-6.
Date A, Panthula M, Bolina A. Comparison of clinical and radiological outcomes in intertrochanteric fractures treated with InterTAN nail against conventional cephalomedullary nails: a systematic review. Future Sci OA. 2020;7(1):FSO668. https://doi.org/10.2144/fsoa-2020-0182.
Onggo JR, Nambiar M, Onggo JD, Ambikaipalan A, Singh PJ, Babazadeh S. Integrated dual lag screws versus single lag screw cephalomedullary nail constructs: a meta-analysis and systematic review. Hip Int. 2022;32(4):550–7. https://doi.org/10.1177/1120700020985067.
Quartley M, Chloros G, Papakostidis K, Saunders C, Giannoudis PV. Stabilisation of AO OTA 31-A unstable proximal femoral fractures: Does the choice of intramedullary nail affect the incidence of post-operative complications? A systematic literature review and meta-analysis. Injury. 2022;53(3):827–40. https://doi.org/10.1016/j.injury.2022.02.002.
Acknowledgements
The authors express their gratitude to ELKE (Eidikos Logariasmos Kondilion kai Ereunas) of Patras University for covering the entire amount of the APC of the article.
Funding
Funding will be provided by University Hospital of Patras.
Author information
Authors and Affiliations
Contributions
Authorship will be considered according to the ICMJE recommendations (a) Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; (b) Drafting the work or revising it critically for important intellectual content; (b) Final approval of the version to be published; (d) Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. AP is the Chief Investigator; he conceived the study, led the proposal and protocol development. EA is the main investigator and participant in the study as the latter has been approved as a doctoral thesis from Patras University Hospital. ZK is a primary investigator also who contributed to the conception and design of the study, NP is a resident in Orthopaedics who will examine the patients at the scheduled follow-ups, KT is a Mechanical Engineering who will organize and assist to the biomechanical and FEA study.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval has been already acquired by the Ethics Committee of the University Hospital of Patras (approval number: 3373/7-2-2022) and the patients’ written consent will be obtained before participating in the study. The study is listed with the International Standard Randomized Controlled Trial Number (ISRCTN): https://doi.org/10.1186/ISRCTN15588442 (registered on 19/4/2022).
Consent for publication
A detailed consent form will be obtained from the patients regarding the use of their data for future publication (s) (images, x-rays). The BMJ model will be used (Greek translation) that includes multiple information that patient has to consent (such as approval of his personal “material”, copy of the material, copy of the article, possibility for incomplete anonymity, no financial benefit, possibility of article distribution to press or the social media etc.)
Competing interests
The authors declare that they have no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Panagopoulos, A., Argyropoulou, E., Kokkalis, Z.T. et al. Study protocol: biomechanical testing, finite element analysis and prospective, randomized, clinical study of single screw cephalomedullary nailing versus integrated dual interlocking screw fixation for unstable (31A21–3) intertrochanteric fractures in patients > 70 years old. J Orthop Surg Res 18, 542 (2023). https://doi.org/10.1186/s13018-023-04009-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-023-04009-8