
Abstract
Cell death is a basic physiological process that occurs in all living organisms. A few key players in these mechanisms, as well as various forms of cell death programming, have been identified. Apoptotic cell phagocytosis, also known as apoptotic cell clearance, is a well-established process regulated by a number of molecular components, including ‘find-me’, ‘eat-me’ and engulfment signals. Efferocytosis, or the rapid phagocytic clearance of cell death, is a critical mechanism for tissue homeostasis. Despite having similar mechanism to phagocytic clearance of infections, efferocytosis differs from phagocytosis in that it induces a tissue-healing response and is immunologically inert. However, as field of cell death has rapid expanded, much attention has recently been drawn to the efferocytosis of additional necrotic-like cell types, such as necroptosis and pyroptosis. Unlike apoptosis, this method of cell suicide allows the release of immunogenic cellular material and causes inflammation. Regardless of the cause of cell death, the clearance of dead cells is a necessary function to avoid uncontrolled synthesis of pro-inflammatory molecules and inflammatory disorder. We compare and contrast apoptosis, necroptosis and pyroptosis, as well as the various molecular mechanisms of efferocytosis in each type of cell death, and investigate how these may have functional effects on different intracellular organelles and signalling networks. Understanding how efferocytic cells react to necroptotic and pyroptotic cell uptake can help us understand how to modulate these cell death processes for therapeutic purposes.
Similar content being viewed by others


Background
Every day, approximately 37.2 trillion cells die in the adult body, the majority which are cause by the caspase-dependent apoptosis mechanism [1]. This apoptotic mechanism has been determined to be essential for the protection of cellular functions in physiological, embryogenesis, tissue repair and also the restoration of homeostasis after disease and inflammation have subsided in a variety of tissues [1, 2]. As an example, neutrophils, the primary innate immune cells that serve as the body’s primary defence mechanism against pathogen attack, have a relatively short lifespan (24 h) and a daily turnover rate of more than 100 billion. Millions of immature T lymphocytes or B lymphocytes are synthesised in the thymus or bone marrow, but only a small percentage mature; the rest are destroyed by apoptosis. Apoptosis aids in the reorganisation of tissues during organs and embryo development. Furthermore, as part of our daily physical cleaning, many ‘used’ cells, such as ageing red blood cells, are discarded [3]. Apoptosis occurs after neutrophils, monocytes and lymphocytes that infiltrate inflammatory disorders have completed their function. As the primary pathogen, serious COVID-19 affects the process of apoptosis in virus-infected cells. The influx of monocytes, macrophages and T lymphocytes into the lungs defined severe COVID-19 [1, 3]. Pathogen infection can cause pathogen cells to die, triggering phagocytic removal in either an immunologically silent or pro-inflammatory mode [4].
Cell death is classified into two types: regulated (apoptosis) and non-regulated (necrosis). Necrosis is the medical term for the unintentional death of cells caused by significant physiological or chemical trauma, such as membrane shearing and breakage caused by high temperatures, osmotic pressure, acidity, or contact with substances such as surfactants and endotoxins. Necrotic cell death, can be either accidental or programmed (for example, pyroptosis and necroptosis) [5]. Programmed necrosis is a type of genetically regulated cell death characterised by morphological characteristics such as cellular enlargement (oncosis), membrane rupture and release of cellular content release. According to new research, certain signalling pathways are required to mediate the programmed necrosis carried out by various death signals, such as necroptosis triggered by the tumor necrosis factor (TNF) superfamily cytokines, interferon and T-cell receptors, toll-like receptors (TLRs), cellular metabolic and genotoxic stresses. Terms like ‘programmed necrosis’ have been employed to highlight the fact that necrotic cell injury is a ‘programmed’ form of cellular death rather than merely an ‘accidental death’. Specific substances (such as death cytokines and their related death receptors) and a sophisticated biochemical signalling cascade are among the triggers that cause necrotic cell injury [6]. Necrosis is distinct from apoptosis because necrotic cells do not transform into apoptotic bodies, which requires enzyme activity. Importantly, these differences suggest that the methods for removing cell debris produced by necrosis versus apoptosis may differ significantly [5].
Apoptosis was the first recognised form of programmed cell death, and it is frequently immune-silent due to apoptotic effectors such as caspase 3 and 7 [7]. When cell death receptors are activated, extrinsic apoptosis occurs, whereas intrinsic apoptosis occurs when cellular stress activates the mitochondrial pathway. Pro-caspase 8 is drawn to the intracellular signalling complex during apoptosis by the adaptor protein FADD (FAS associated via death domain). Caspase 9 is activated and cytochrome c is released via the intrinsic route. Caspases 3 and 7 activation results in the development of both apoptotic pathways. Find-me signals are released when caspases are activated during apoptosis to guide apoptotic cells toward phagocytes [8]. This procedure is depicted in Fig. 1. The lytic forms of cell death necroptosis and pyroptosis, on the other hand, allow the secretion of immunostimulatory substances. According to genetic evidence, these cell death mechanisms have the potential to cause severe inflammatory reactions in living organisms, contributing to the pathology of a variety of inflammatory diseases. Necroptosis and pyroptosis are pro-inflammatory pathways because they promote excessive escape of cell contents, including damage-associated molecular patterns (DAMPs) [9]. Necroptosis is distinguished from other types of necrosis by the presence of receptor-interacting protein kinase 1 (RIPK1) and RIPK3, which attract and phosphorylate the mixed lineage kinase domain-like protein (MLKL). MLKL then oligomerises and moves to the inner leaflet of the plasma membrane, where it stimulates membrane permeabilization and cell death [5]. Excessive inflammasome activation, on the other hand, causes pyroptosis. Inflammasome-expressing cell types, such as macrophages, are exposed to it following infection (with the intracellular pathogen Salmonella typhimurium) or LPS treatment [10]. Inflammasomes containing activated caspases 1 or 11 form gasdermin D pores by processing the precursor of gasdermin D pores at the plasma membrane. These pores allow IL-1 to be released, but they also permeate the plasma membrane excessively, causing cell lysis and pyroptosis [5]. Nonetheless, necroptotic and pyroptotic cells must be eliminated quickly and without causing inflammation.

Cell death molecular mechanisms schematic. Both intrinsic and extrinsic apoptotic signals activate death receptors on the cell surface, which activates caspase 3/7. The progression of secondary necrosis may be accelerated by caspase-3-cleaved GSDME and NINJ1. Primary necrosis typically has a randomness, resulting in an uncontrolled rupture of membranes. Through its interaction with the INF-R, TNF-may induce necroptosis by activating RIPK1/3 and creating MLKL membrane holes. Pyroptosis is triggered by the detection of PAMPs/DAMPs like ATP. Pyroptosis is induced by caspase 1, and caspases 4/5/11 converge with the activation of Gasdermin D
Despite the fact that the vast majority of apoptotic cells are produced on a regular basis, they are rarely seen in tissues in vivo. This is because of the fascinating relationship between cell death and efferocytosis, the phagocytic process that effectively removes apoptotic cells [2]. Professional and non-professional phagocytic cells use efferocytosis to remove apoptotic cells quickly and effectively [11]. Due to efferocytosis, early multicellular creatures were able to control their growth by eliminating dead cells as they developed. Efferocytosis is required for development and growth, as well as to reduce inflammation and maintain cellular homeostasis [12, 13]. The mechanisms of efferocytosis are distinct from those of standard phagocytosis, both visually and mechanistically. Phagocytosis necessitates the expression of signals and receptors on the phagocyte, cytoskeleton reorganisation to ingest apoptotic cells and induction of phagosome-lysosome fusion to destroy the content of apoptotic cells [8]. When the number of apoptotic cells exceeds the number of accessible classical phagocytes, as occurs during acute inflammatory responses, phagocytes must be able to consume them quickly, a process known as constant efferocytosis. In this case, macrophages regulate inflammation to aid tissue recovery. When efferocytosis is inadequate, this process is ineffective and causes tissue injury [14].
The majority of the contents of an infected apoptotic cell (such as proteins, nucleic acids and lipids) are similar to those of a non-infected dead cell; however, efferocytes such as macrophages can detect the difference, allowing the efferocyte to produce an effective immune response against pathogens within efferocytes cells [13]. This demonstrates how efferocytosis differs from phagocytosis and how efferocytes can tell the difference between harmful and apoptotic cargo. Defective efferocytosis can lend to the accumulation of apoptotic cells in inflammatory foci, resulting in necrosis, cytolysis and the production of intracellular contents tissue damage. Lesional efferocytosis and larger necrotic cores were associated with low-density lipoprotein receptor deficiencies in chronic diseases when compared to healthy animals. Inadequate efferocytosis is a common diabetic side effect that can prevent tissue repair and lead to chronic inflammation as a result of a build-up of apoptotic cells at the wound site [15]. The molecular pathway of efferocytosis in necroptosis and pyroptosis is less well understood than the apoptosis mechanism. We discuss what is known about the efferocytosis process in necroptosis conditions such as inflammatory diseases and pathogen infection-induced pyroptosis, as well as the differences between these and apoptosis and their effects on organism physiology. This mechanism ‘find-me’ and ‘eat-me’, signals, as well as engulfing dead cells.
Hallmark of infection and inflammation
Understanding the distinctions between infection and inflammation mechanism is the first step towards understanding necroptosis and pyroptosis mechanisms. Inflammation occurs as a complex biological response when vascular tissues come into contact with pathogens, dying cells, or irritants. Some of the most common symptoms acute inflammation include swelling (tumour), heat (calor), pain (dolour), redness (rubor) and loss of function (functio laesa). Inflammation is the body’s reaction to potentially harmful stimuli in an attempt to rid itself of them and begin the healing process. Even when caused by an infection, inflammation is not always synonymous with infection. Even though a bacterium causes an infection, inflammation is one of the pathogen’s responses. Inflammation, on the other hand, is a stereotypical reaction, so it is classifies as innate immunity rather than adaptive immunity, which is tailored to each specific pathogen [16]. In the same way, an infection is defined as the invasion of tissues by pathogenic organisms, their proliferation and the host tissues’ response to their toxins. Infections are caused by bacteria, viruses, prions and viroid’s, as well as larger organisms such as parasites and fungi. The immune system in hosts enables pathogen defence. Mammalian hosts respond to infections by first undergoing an innate response, which frequently includes inflammation, and then an adaptive response. As a result, while inflammation is not always associated with infection, infection is usually associated with inflammation [17].
The host detects the presence of microorganisms through a variety of mechanisms, the most important of which include various receptor families. These numerous sensors are constantly scanning for microorganisms in various subcellular compartments. Several Toll-like receptors (TLR) and C-type lectins are found in the plasma membrane and can detect the presence of bacteria in extracellular fluids [18, 19]. Each of the 11 distinct TLRs recognises microbial components that are chemically distinct from those produced by the host (also known as PAMPs—pathogen-associated molecular patterns). TLR4, recognises lipopolysaccharides, which are membrane components found in the majority of gram-negative bacteria. TLR2 recognises lipopeptides, which are found in many gram-positive organisms. By focusing on these conserved pathogen-associated molecular patterns, the host is able to accomplish two remarkable and significant feats. Despite the enormous diversity of these organisms, it can distinguish between self and nonself components by employing a relatively small number of receptors capable of identify the majority of bacteria, fungi and viruses [18].
The inflammatory response clearly contributes to an infection. Vasodilatation greatly accelerates the delivery of blood-borne defences to the affected site. Increased vascular permeability allows soluble immune proteins such as complement and antibody to enter the environment and fight invasive microorganisms. Neoexpressed vascular adhesion molecules and chemokines attracts leukocytes into the tissue space. When pathogens arrive at the infection site, leukocytes digest them and try to get rid of them. As a result, both soluble and cellular immune responses are rapidly provided by these systems [20].
The immune system has evolved several mechanisms to detect cell death and warn of potential dangers. An infection, such as a toxin or a cytopathic bacterium, can cause necrotic cell death. Even if it is not directly caused by a pathogen, cell death frequently occurs in a location where microbes have been introduced as a result of an injury, such as a penetrating wound. Because of their 20-min doubling time, microbes pose a massive threat that requires an immediate response to contain. When the host detects dead cells, it immediately initiates an inflammatory response to neutralise the threat [20]. However, in a variety of other circumstances, cells die and cause inflammation in the absence of a microbial infection. When a tumour is forming, for example, dying cells may still be harmful to the body and may be eliminated by the host immune system [21]. Other times, the inflammatory response may work against some disease processes in different ways. Apoptosis can occasionally be quiet or inflammatory in chronic situations, such as diabetes. It is thought that how quickly phagocytes remove apoptotic cells is an important factor. If apoptotic cells are not given enough time to clear, they undergo secondary necrosis, allowing macromolecules to pass through their membranes. If this process occurs before the phagocytes digest the dead cells, the pro-inflammatory intracellular contents of the dead cells will be released, triggering a host response [20]. Because harmful activities, such as infections, can cause cells to die, this inflammatory response to apoptotic cells may be beneficial teleologically.
Death cell in necroptosis and pyroptosis
Necroptosis
Necroptosis can be aided extrinsic apoptotic receptors. When apoptosis is inhibited, a process known as necroptosis takes place, which results in cellular self-destruction. Necroptosis differs from other types of programmed necrotic cell death in that it occurs without caspase activation. Necroptosis is a non-apoptotic, the core necroptotic pathway is triggered by the proteins RIPK3 and MLKL (Fig. 1). Necroptosis is thought to be a type of controlled necrosis and is considered inflammatory because to lacks the find-me and eat-me signals of apoptosis. The RIPK1 recruits and phosphorylates RIPK3, forming the RIPK1/RIPK3 complex, and it activates MLKL and releases DAMPs for phagocytes to recognise [22, 23]. Multiple sclerosis and amyotrophic lateral sclerosis, both of which cause cell death and inflammation, have recently been linked to necroptosis in humans [24,25,26,27].
Both apoptosis and necroptosis are regulated by the same molecular machinery [28]. Apoptosis is a natural biological process that allows the majority of cells in the body to keep their internal environment stable by preserving a specific developmental pathway. As a result, apoptosis is a tightly regulated process of irreversible caspase-dependent cell death, whereas necroptosis is caspase-independent signalling pathway that is primarily dependent on the RIPK1/RIPK3/MLKL complex [29]. Apoptosis is characterised by cell shrinkage, membrane blebbing, chromatin condensation, the formation of apoptotic bodies and rapid phagocytosis by nearby phagocytes. Because there is no materials overflow during apoptosis, there is no inflammatory immunological reaction. Necroptosis, on the other hand, is a type of cytolytic death. As a result of the plasma membrane’s rapid loss of integrity, pro-inflammatory molecules escape from the cells, triggering a variety of inflammatory reactions [28,29,30]. Furthermore, all necroptosis pathways share one feature: they all prevented by caspase 8 activation (Fig. 1).
Necroptosis occurs frequently when components of the death receptor (DR) apoptotic signalling pathway fail. For example, in order to trigger DR Necroptosis, the majority of studies to date have suppressed cIAP1/2 and caspase 8, two cellular proteins that generally ubiquitylate or cleave RIPK1/3 to prevent necroptosis [31]. When caspase-8 and/or cIAPs are not expressed, activation of RIPK1/3 by DRs (such as TNFR1, TRAIL-R, CD95), Toll-like receptors (such as TLR3 or TLR4), or the cytosolic Z-DNA/Z-RNA detecting receptor, Z-DNA binding protein 1 (ZBP1/DAI/DLM-1), can instantly cause necroptosis. Activation of these receptors leads to the establishment of a RIPK1-RIPK3 cell death platform known as the necrosome by interacting with heteroamyloid-structured RIPK1/RIPK3 RHIM-RHIM domains [32]. The necroptotic executioner MLKL is phosphorylated by RIPK3, allowing MLKL to oligomerise and associate with membranes, potentially damaging the plasma membrane and releasing DAMPs [33,34,35]. In many cases, RIPK1 and its kinase activity are critical for necroptosis; however, recent research has shown that the RHIM, a RIPK1 scaffolding role, functions as a critical blocker of fatal necroptotic death by inhibiting ZBP1 binding and RIPK3 oligomerisation [36, 37]. Non-necroptotic transcriptional (such as activating inflammatory cytokines) and post-translational (such as activating apoptotic cell death) activities of RIPK1 and RIPK3 should also be considered [38]. As a result, the requirement for MLKL is the best way to describe mammalian necroptosis.
Pyroptosis
Pyroptosis is made up of the words ‘pyro’ and ‘ptosis’. Pyro means ‘fire’, which refers to the inflammatory properties of pyroptosis, and ‘ptosis’ means ‘falling’, which is related to other types of programmed cell death. Apoptosis and pyroptosis share two characteristics: DNA damage and chromatin condensation [39]. Interestingly, pyroptotic cells had multiple bubble-like protuberances on the exterior of the cell membrane’s exterior that were inflated until they ruptured [40]. Apoptosis, like membrane blabbing, results in this process and caspase 3 is required for it [41,42,43,44]. Specific morphological characteristics distinguish pyroptosis from apoptosis. Although the pyroptotic cells undergo chromatin condensation and DNA fragmentation, their nucleuses remain intact. The integrity of the nucleus and a bit of DNA laddering are present during pyroptosis. The inflammation-induced pore formation results in swelling and osmotic lysis in pyroptotic cells. In comparison to pyroptotic cells, cells undergoing apoptosis maintain intact membranes. Although pyroptosis can cause inflammation when triggered by external or intracellular triggers such as bacteria, viruses, toxins and chemotherapeutic drugs, apoptosis is widely accepted to be a benign type of cell death [45]. In fact, pyroptosis, as opposed to necrosis, allows the cytoplasm to flatten as a result of plasma membrane leakage [40]. In contrast to necroptosis, pyroptosis is induced response to infection, such as caspases like caspases 1, 4 and 5 detect lipopolysaccharide on intracellular gram-negative bacteria (Fig. 1). When activated, this caspase cleaves gasdermin D (GSDMD), resulting in cell lysis. Pyroptosis and necrosis cause the released as a result of pro-inflammatory cytokines [30].
Caspase activation or granzyme release results in the N-terminal oligomerisation of gasdermin and the formation of a pore (1–2 m diameter) in the plasma membrane, allowing mature IL-1/IL-18 with a diameter of 4.5 nm and caspase-1 with a diameter of 7.5 nm, respectively [46]. Water leaking through the perforations causes cell swelling and osmotic lysis, rupturing the plasma membrane and releasing IL-1 and IL-18. The pyroptotic cells are permeable to several dyes due to their low molecular weight, including 7-aminoactinomycin (7-AAD), ethidium bromide and propidium iodide [47]. Apoptotic cells, unlike pyroptotic cells, maintain the integrity of their membranes, preventing these dyes from staining them [48,49,50]. Annexin V stains both apoptotic and pyroptotic cells, and the colour binds to phosphatidyl serine (PS). As a result, Annexin V cannot tell the difference between apoptotic and pyroptotic cells. Furthermore, pyroptosis causes the formation of pyroptotic bodies, whereas apoptosis causes the formation of apoptotic bodies. It is worth noting that pyroptotic entities have a 1–5 m diameter, which is comparable to the size of apoptotic bodies [51].
Numerous caspases, including caspase 11 and its human orthologs caspase 4 and 5, as well as the apoptotic effector caspase 3 [52, 53], have been shown in studies to be capable of inducing pyroptosis, also known as caspase-1-mediated cell death. The ability of these caspases to cleave and stimulate specific components of the pore-forming gasdermin gene family, which includes six genes in humans and ten genes in rats, mediates pyroptotic cell death. Caspases-1/4/5/11 have been found to target GSDMD, whereas caspase-3 can handle GSDME/DFNA5 (Fig. 1) [54, 55]. The cleavage of the linker domain of gasdermin between the N- and C-termini separates an active N-terminal area from inhibitory C-terminal fragment. Thus, expression of the gasdermin-N domain from GSDMA, GSDMA3, GSDMB, GSDMAC, GSDMD and GSDME alone could indicate cell death; however, more research into the physiological functions of these gasdermins, as well as possible proteolytic enzymes that target GSDMA to GSDMC, is needed [46, 54]. However, when the gasdermin-N domain is released by proteolysis, it interacts with acidic phospholipids, such as phosphoinositides found on the inner leaflet of the mammalian plasma membrane, and forms oligomeric death-inducing holes [46, 56,57,58]. While in vivo studies show that bacteria can survive pyroptosis and are removed by neutrophils, in vitro studies show that gasdermins can target bacterial membranes to induce lysis. [59, 60] Regardless, we can now say that gasdermin is required for mammalian cell pyroptosis.
Inflammasomes, which are intracellular multiprotein signalling complexes, are activated when inflammatory ligands are detected, according to the classical theory of caspase-1 mediated pyroptosis (Fig. 1). AIM2 (absent in Melanoma 2), Pyrin and the NOD-like receptor family members NLRP1, NLRP3 and NLRC4 are among the most extensively studied inflammasome sensors [61]. For example, cytosolic double-stranded DNA binds to and activates the AIM2 inflammasome. The NLRP3 inflammasome reacts with a wide range of molecules, including ATP, crystalline substances (such as cholesterol crystals) and viral elements, which when combined cause potassium efflux and the subsequent association of NEK7 (NIMA-related kinase 7) with NLRP3 to cause NLRP3 activity [62, 63]. Caspase-1 is frequently attracted to inflammasome sensor like NLRP3 via the adaptor protein ASC, which contains a CARD-domain. As a result of this recruitment, the inactive caspase-1 species, p46 and p33/p10 subunits, are automatically processed into their catalytically active forms [64].
Active caspase-1 not only cleaves and activates GSDMD, but it also activates the inflammatory cytokines IL-1 and IL-18 (Fig. 2). Caspase-4/5/11, which have been discovered to specifically engage cytosolic LPS, are what differentiate non-canonical inflammasomes from caspase-1 and result in GSDMD targeting and activation [52]. Caspase-4/5/11 does not directly process IL-1 and IL-18 [65], but their activity is sufficient to initiate the classical NLRP3 inflammasome and activate IL-1 by inducing GSDMD-mediated potassium efflux [66, 67]. Other membrane-damaging mechanisms, such as those driven by the mixed lineage kinase domain-like pseudo kinase (MLKL) or monosodium urate crystals, have been shown to trigger IL-1 production even in the absence of the GSDMD pore [68, 69].

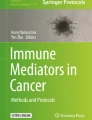
Mechanism of find-me and eat-me signal release in necroptosis and pyroptosis. A Immunomodulatory signal is induced by MLKL phosphorylation. PS is exposed to the outer membrane, and extracellular vesicles are released together with necroptotic bodies as a result of the creation of MLKL pores, which also causes the release of cytoplasmic DAMPs. Necroptotic cells lose the integrity of their membrane, which leads to the release of their DAMPs, which include HMGBl and IL-1. B The GSDMD-N is released and translocated to the inner plasma membrane together with PS, which is exposed to the outer membrane as a ‘eat-me’ signal when the inflammasome is active. The oligomerisation induces transmembrane pores to open, the production of pro-inflammatory cytokines like IL-1 and IL-18, and cell swelling that triggers the release of DAMPs like ATP
Pyroptosis and necroptosis are both types of inflammatory lytic cell death. However, pyroptotic and necroptotic death may serve different functions, as evidenced by their distinct genetic drivers. Caspase 8 inhibition of fatal necroptotic signalling, for example emphasises that necroptosis is primarily recognised as a backup cell death defence system activated when apoptosis is inhibited [70, 71]. Pyroptosis, on the other hand, is a basic cellular response triggered by the identification of potentially harmful insults such as pathogen ligands, DAMPs, elevated prevalence of host metabolites and environmental irritants [72, 73].
GSDMD is activated by pyroptosis cleavage during proteolytic, whereas MLKL is activated by phosphorylation during necroptosis. MLKL’s equilibrium will shift from inactive cytoplasmic monomeric MLKL to membrane-associated MLKL oligomers as a result of RIPK3 phosphorylation (Fig. 1) [74,75,76]. Furthermore, the GSDMD-N domain has shown the monomer-to-oligomer transition, which a critical stage in MLKL’s ability to disrupt membranes [46, 58, 76]. Current studies on the physiological implications are focusing on whether GSDMD and MLKL-induced membrane destruction is sufficient to allow the production of DAMPs and other small soluble cytosolic components prior to complete cell lysis. However, evidence suggests that prelytic GSDMD holes may allow for ion flux or cytokine secretion even before to plasma membrane rupture [77]. Numerous studies have also suggested this possibility, including those that found MLKL/GSDMD-mediated or GSDMD-independent IL-1 secretion prior to cellular lysis or in the absence of cell death [68, 78,79,80].
MLKL and GSDMD killing can result in a variety of morphologies. Changes in MLKL and GSDMD targeting and pore-creation processes, as well as experimental variations in the kinetics of necroptotic and pyroptotic cell death, may aid in understanding. The non-selective diffusion of ions produced by GSDMD-N whole creation is thought to cause decreased cell enlargement and demolished cytoplasm during pyroptosis, and cells going through pyroptosis maintain adhesion until the plasma membrane is damaged [76, 77]. While disruption to the ion-selective MLKL protein affects intracellular osmolarity, causing cell swelling and osmolysis, necroptotic signalling causes cellular detachment [76]. Because all three types of cell death involve the breakdown of the plasma membrane, Phosphatidylserine Annexin V staining cannot distinguish between apoptosis, pyroptosis and necroptosis [77].
Efferocytosis of necroptosis and pyroptosis
Efferocytosis typically terminates apoptosis by preventing the accumulation of dead cells, inflammatory reactions and secondary necrosis [81, 82]. Efferocytosis is the phagocytosis of dying and dead cells as well as their debris by phagocytes [83, 84]. Efferocytosis, which results in uptake into ‘spacious phagosomes’, combines characteristics of traditional phagocytosis and the liquid absorption process macro pinocytosis [85, 86]. Although efferocytosis distinguishes the identification and digestion of dead and dying cells from other types of phagocytosis [84, 87], its molecular properties are unknown. Efferocytosis necessitates the use of a large number of soluble and cell surface receptor-ligand interactions that have been identified for phagocytosis. Efferocytosis is controlled by several communications between the phagocyte and its dying target cell. Originally, efferocytosis was defined as the removal of apoptotic cells, but this definition has since been expanded to include other types of cell death [86].
Efferocytosis is carried out by professional and non-professional phagocytes, such as DCs, macrophages, fibroblasts and epithelial cells, by identifying find-me and eat-me signals from apoptotic cells [82]. Phagocytes interact with apoptotic cells via a set of signals known as ‘apoptotic cell-associated molecular patterns’, or ACAMPs [87]. Externalised phosphatidylserine, calreticulin and modified carbohydrates known as ACAMPs will be discussed briefly below. These compounds are recognised by a specific set of receptors and bridging molecules. Efferocytosis is compensated by four steps: (1) phagocyte recruitment controlled by find-me signals, (2) dead cell recognition controlled by eat-me signals, (3) dead cell absorption and (4) dying cell degradation [23, 88]. Healthy cells send tolerate I signals, also known as ‘keep-me’ or ‘do not eat-me’ signals, to prevent efferocytosis [15]. Some receptors, such as complement and antibody Fc receptors, communicate with the cytoskeleton and initiate direct phagocytic activity in response to eat-me signals, whereas others, such as the TIM-4 receptor, only anchor the target cell [89, 90]. To determine whether or not to ingest the target cell, a phagocyte will combine information from multiple receptors [89,90,91]. Cellular material is completely swallowed via cytoskeletal remodelling of the plasma membrane [92,93,94,95]. The ingested cell is often, but not always, cleared within a phagolysosome-type compartment after processing [96,97,98]. During the target cell identification phase, phagocytes may also examine the target’s chemical components to assess the danger it poses, as well as its physical characteristics, such as size, shape and topography [99,100,101]. This analysis determines three things: (i) the fate of the target cell within the phagocyte; (ii) whether the clearance process is immunologically silent, such as apoptotic cells efferocytosis; and (iii) whether engulfment occurs or is replaced by, for example, neutrophil NETosis, an anti-microbial cell killing process in which neutrophils expel chromatin extracellular snares [90, 102, 103].
Find-me signals
Apoptotic cells emit find-me signals in order to distinguish themselves from healthy cells and to attract phagocytes to areas of death [15]. These signals primarily function as DAMPs, promoting the production of a variety of cytokines and chemokines that activate phagocytes [3, 4]. Sphingosine-1-phosphate (S1P), lysophosphatidylcholine (LPC), nucleotides and C-X-C motif chemokine ligand 1 (CX3CL1) are components of find-me signals [104,105,106,107]. Sphingosine kinases generate S1P from sphingosine, which regulates phagocyte cell migration by interacting with G-protein-coupled receptors ([104, 108], whereas caspase-3 and phospholipase A2 generate LPC [109]. Nucleotides such as uridine diphosphate (UDP) and adenosine triphosphate (ATP) promote phagocyte engagement with purinergic receptors, resulting in the phagocytic clearance of apoptotic cells [106]. Apoptotic cells secrete the chemokine CX3CL1 under the control of caspase and Bcl-2. By interacting with CX3CL1 and the macrophage fractalkine receptor (a find-me signal), macrophages are directed to apoptotic sites [105]. However, the molecular mechanisms underlying this process are still poorly understood. While all of these factors may cause macrophages to apoptotic cells, the significance of specific find-me signals in efferocytosis is dependent on a variety of factors, including phagocyte and apoptotic cell type, as well as the apoptotic impulses and phase of apoptotic cell death being studied (reviewed in [110]). Several of these find-me signals are also important regulators of macrophages inflammatory responses, as will be discussed further below.
Apoptotic cells can release adenine and uridine nucleotides from their surface via hexametric pannexin-1 channels activated by caspase-3/7 [107]. Necrosis, inflammatory cells and all caspase-dependent processes, including necroptosis and pyroptosis, also release these nucleotides (Fig. 2) to speed up cell removal, the extracellular nucleotides ATP and UTP act as ‘find-me’ signals [111]. They achieve this by increasing the number of P2Y purinergic-expressing motile phagocytes and upregulating phagocytic receptors [106, 112, 113].
Extracellular nucleotides can influence macrophage immune responses by converting ATP to adenosine, a well-known and powerful regulator of macrophage inflammation [111, 114]. Recent research has shown that during efferocytosis, Gs-linked A2a and A2b adenosine receptors on macrophages reduce pro-inflammatory cytokines (such as the C-X-C motif chemokine ligand 1 (CXCL1) and CXCL2) and increase pro-resolution factors (such as Nr4a, Thbs1) [115, 116]. The specific pathways involved in the production of extracellular adenosine during efferocytosis are unknown. Although adenosine can be transferred directly from macrophages (117), extracellular adenosine accumulates in a variety of tissue conditions as a result of ecto-enzymes like CD39 (ATP/ADPAMP) and CD73 (AMP adenosine) hydrolysing extracellular adenine nucleotides (ATP, ADP and AMP) [111, 114]. It is unknown how these ecto-enzymes influence adenosine synthesis and macrophage immunology during efferocytosis. According to Wang et al. research, pyroptotic cells use ATP as a find-me signal to attract macrophages. They also discovered that necroptotic cells caused THP-1 cells to migrate in a Trans well migration study. Additional research discovered that the activity of ATP released by necroptotic cells as a find-me signal caused THP-1 cell migration [117].
In contrast to the clearance of apoptotic and necrotic cells, the clearance of dead cells via alternate cell death pathways, such as necroptosis, is only now being reported. When caspase inhibition is present, as it is during viral infections, the RIPK1/3 and MLKL factors drive necroptosis and necroptosis can be induced via the TNF pathway. As a result, necroptosis does not typically involve the activation of several of the caspase 3/7-induced essential regulators (such as PANX1 and Xrk8) required for clearance systems (such as ATP production and PS presence) (Fig. 2) [118]. Recent research has shown that the critical necroptotic regulators RIPK3 and MLKL are required for necroptotic cells to reveal PS prior to membrane permeabilization [119, 120]. Thus, increased phagocytic receptor TIM4 levels can improve necroptotic cell removal, and the PS binding protein Milk fat globule (MFG) epidermal growth factor 8 (MFG-E8) can be used to identify necroptotic cells [120]. In addition to PS, the lipid mediator Resolvin D1 may aid in the clearance of necroptotic cells by promoting phagocytic CRT production, which identifies and makes it easier to identify necroptotic bone marrow-derived macrophages (BMDM) [121]. Necroptotic bodies are small PS-positive extracellular vehicles released by necroptotic cells that look like apoptotic bodies [119, 120], the question of whether these necroptotic bodies have any bearing on the efficacy of necroptotic cell removal remains unanswered.
The signalling pathways underlying the elimination of pyroptotic cells are currently being described, similar to the mechanism for necroptotic cell clearance. Similar to how PANX1 is cleaved by caspase 3/7 during apoptosis, PANX1 is triggered by caspase 1/11 during pyroptosis and helps generate ATP ‘find-me’ signals to promote phagocytic migration. In order to attract phagocytes, pyroptotic cells release IL-1 and IL-18 through GSDMD pores in a manner independent of cell lysis (Fig. 2) [60, 122]. In comparison to apoptotic ‘find-me’ signals, necroptosis and pyroptosis cells may lack the ability and power required to interpret their own signals. The majority of the molecules found to be produced by dying cells are DAMPs, which are actual biological elements that are normally hidden within the cell but become visible to the outer membrane when the cell injured or death. DAMPs include the nuclear protein high mobility group box-1 protein (HMGB1), N-formylated peptides derived from mitochondria, RNA, DNA, ATP, uric acid, actin, histones, calcium-binding S100 proteins and heat-shock proteins (Fig. 2) [123]. Additionally, necrotic cells mare lease accumulating inflammatory mediators such as IL-1, IL-33 and chemokines. These mediators may either directly or indirectly attract phagocytes to the area. Furthermore, when necrosis occurs, the complement and coagulation proteolytic cascades are immediately activated, exposing ‘unique’ molecules. The powerful chemoattractant C5a is one of the ‘find-me’ signals produced by complement activation on necrotic debris [124]. Even though necroptosis and pyroptosis are both parts of the necrotic process, the mediators that are released during each of them may be different from those that are released during necrosis as a whole. However, research into these systems is ongoing. A brief description of additional necrosis mediators is provided below.
In the scientific literature, formyl-peptides have a well-established role as a necrotic ‘find-me’ signal. In seminal studies using targeted thermal injury to the liver, formyl-peptide receptor 1 (FPR1) activation of neutrophils was the critical process required for mobility into the necrotic area [125]. Formyl-peptides bind to the FPR1, FPR2 and FPR3 receptors, but the classic chemotactic effects are primarily caused by FPR1 activity. An intravascular gradient of CXC chemokines aided in the initial migration of neutrophils toward the liver. Clinically relevant drug-induced liver damage and hepatic ischaemia–reperfusion disease models have revealed neutrophils’ reliance on formyl-peptide gradients for migration to necrotic areas [126], while the majority of research has focused on formyl-peptide-induced neutrophil chemotaxis and activation, macrophages also express FPR1 and respond to formyl-peptide stimulation. When mitochondrial extracts containing formyl-peptide are present, human peripheral blood mononuclear cells significantly release the CXCL8 [127], it is worth noting that when formyl-peptides are combined with other immunostimulatory DAMPs, such as HMGB1, the response is improves. This demonstrates that formyl-peptides can stimulate existing macrophages to produce more chemo attractants, which could then attract phagocytes to necrotic areas in an indirect manner (CXCL8).
Chemotactic cytokines, or chemokines, control where and how leukocyte populations are recruited within an organism. When there is necrosis, chemokines can be produced by both damaged and healthy observer cells, acting as both primary and secondary ‘find-me’ signals. Almost all cell types, including resident leukocytes, can produce CC and CXC chemokine’s [128], the chemokine CXCL1 can be released by endothelial cells, hepatocytes, macrophages, pericytes and fibroblasts. Kupffer cells, for example, express CCL2 after necrotic injury, whereas neutrophils release CXCL2 during transendothelial migration [129]. The fact that there are various chemokine sources that can trigger phagocyte migration to necrotic sites demonstrates the importance of chemokines as necrotic ‘find-me’ signals.
Leukotriene B4 (LTB4) is another find-me signal that increased cell movement in necrosis. LTB4 is a phospholipid facilitator that is synthesised from lipid membranes. LTB4 is a powerful neutrophil chemoattractant. When it comes into contract with GI, it stimulates the BLT1/LTB4R1 receptor, causing Rho GTPases and Src-family kinases to pair with it and accelerate neutrophil motility [130]. Neutrophils recruited to the region that produces LTB4 to boost other neutrophil recruitment to necrotic foci and form the recognisable densely populated clusters associated with neutrophil swarming. Neutrophil LTB4 can act as a signal relay molecule required for cell–cell interaction to increase neutrophil aggregation at the damaged site. LTB4 has also been found to collaborate with other necrotic ‘find-me’ signals, such as formyl-peptides and chemokines, implying that there is not just one necrotic ‘find-me’ signal, but rather a collaborative pool of signals with varying chemotactic potencies and ranges that work together to facilitate an effective response [131, 132].
Organelles such as mitochondria and phagosomes frequently produce reactive oxygen species (H2O2). Leukocytes must be equipped with a method for detecting the transitory H2O2 gradient produced by damaged cells. According to preliminary research, the redox sensor is the Src-family kinase Lyn, which is activated by wound-derived H2O2 and facilitates neutrophil migration to damaged areas in zebra fish [133]. H2O2 oxidises cysteine C466, activating Lyn and allowing neutrophils to migrate to the wound. Except for T cells (which express related Src-family kinases), all mammalian leukocytes express Lyn and human and murine neutrophils are also chemotactic to H2O2 [133, 134]. As a result, H2O2 acts as a necrotic ‘find-me’ signal for several types of leukocytes. In addition to its direct effects on phagocyte migration to injury sites, H2O2 can modify other ‘find-me’ signals such as fMLP, LTB4 and CXCL8 (141). Indeed, the NADPH oxidase at the leading edge of neutrophils is required for the generation of reactive oxygen species, which oxidise and inhibit the phosphoinositide phosphatase PTEN. This keeps PI (3, 4 and 5) P3 levels high at the leading edge and promotes neutrophil directed movement [135].
One of the first substances produced by injured and dead cells is nucleotides [136]. Nucleotide detection is mediated by the P2Y and P2X receptor families, which are G protein-coupled receptors and nucleotide-gated ion channels, respectively. Although there are several of these receptors, each with different sensitivity to different nucleotides (such as ATP, ADP and UTP), the majority of research has focused on the function of ATP and its breakdown products. Apoptotic cells initially used ATP as a ‘find-me’ signal [106]. the researchers discovered that P2Y2-dependent ATP and UTP produced during apoptosis are required for monocyte migration toward apoptotic cell supernatants. Furthermore, the absence of P2Y2 prevented monocytes from migrating toward apoptotic cells in vivo. Even more intriguing is the role of purinergic signalling in necrotic injuries. Using a focused necrotic lesion to the liver, it was demonstrated that ATP is required for peritoneal macrophage incursion into the necrotic site [137].
Eat-me signals
Apoptotic cells attach to cell surface receptors such as stabilin-1 and stabilin-2, adhesion G protein-coupled receptor B1, T cell immunoglobulin mucin receptor (TIM) 1, TIM3 and TIM4 in the second stage of efferocytosis [138,139,140,141,142]. This would have pleiotropic effects via a number of bridging molecules, such as protein S and MFG epiderma, this would have pleiotropic effects [143,144,145]. Similarly, transglutaminase 2 (TG2) binds to MFG-E8 and acts as an activator of Rac 1 by acting as an integrin 3 receptor. As a result, apoptotic cells are digested. Integrin 3, on the other hand, is unable to recognise apoptotic cells in the absence of TG2 [146]. Phosphatidylserine (PS), which is found in the inner membrane of cells and is produced externally by caspase signals upon death, appears to have a significant impact on eat-me signals [147, 148].
Eat-me signals are either directly recognised by PS binding receptors or indirectly recognised by phagocytes bonding facilitators. PS is abundant on the exofacial side of the membrane, where it is normally restricted to the inner leaflet of live cells, as a result of caspase-mediated changes in the activity of numerous important phospholipid transport enzymes. There are currently at least 12 PS efferocytosis receptors identified, which are a group of surface proteins with a variety of structural properties that can either directly or indirectly bind to PS by recognising soluble PS binding opsonins [149]. The receptor for advanced glycation end products (RAGE) can recognise PS and is involved in the efferocytosis in macrophage [84]. MFG-E8 recognises PS and is recognised by the αVβ3 and αVβ5 phagocyte receptors (such as those on DCs and macrophages). When these receptors engage, the cytoskeleton may change, promoting the absorption of apoptotic cells [150,151,152]. Furthermore, soluble CD93 interacting with PS and integrin × 2 on apoptotic cells induces efferocytosis via an opsonin, and endothelial and phagocytic cells detect the interaction of the complement factor C1q with PS [153]. These findings suggest that being exposed to PS may increase the engulfment of dying cells. PS is recognised by membrane number receptors such as Stabilin-1, Stabilin-2, TIM4, RAGE, BAI-1 and CD300. PS receptors have been shown to be required for identifying dead cells [139, 140, 142, 154]. Macrophages that express stabilins 1 and 2, for example, can detect PS on apoptotic cells and absorb more apoptotic debris [147, 155]. This method is necessary for identifying and removing PS-stimulated aged or injured erythrocytes. During apoptosis CD300 can detect PS and phosphatidylethanolamine [156]. As a result, a lack of CD300f and CD300d can impair normal macrophage efferocytosis [157]. PS is detected by scavenger receptors (SR) SR-A1, SR-B1 and CD36, which stimulates macrophage efferocytosis [156]. It is well known that the traditional DAMP, HMGB1, inhibits RAGE/PS-mediated efferocytosis in macrophages by binding to integrin v3 [158]. While HMGB1-deficient macrophages effectively phagocytize apoptotic neutrophils and thymocytes [159], HMGB1 is translocated into the cytoplasm before being released into the extracellular environment [160]. Rac, CDC42, Rab5, Rho A and Rho-associated coiled-coil kinases (ROCK) members of the Ras homolog family (Rho) of small GTPases are also important in regulating the absorption of dying cells [161,162,163].
Overall, the literature shows that apoptotic cell clearance dominates the topic cell elimination [164,165,166]. Phagocytic receptors may be unable to recognise necrotic cells because they contain varying amounts of PS [164]. As a result, necrotic cells may take longer to be digested by phagocytes than apoptotic cells [165]. Furthermore, necrotic cells frequently produce a single massive bleb and continue to exist as a single biological entity, as opposed to apoptotic cells, which rapidly bleb and divide into apoptotic bodies [166]. Given the importance of dying cell breakup in facilitating cell elimination, this could also explain why necrotic cell removal is less efficient than apoptotic cell absorption and the many mechanisms involved [165, 167]. It has been demonstrated in both in vitro and in vivo experiments clearing apoptotic cells is more effective than engulfing necroptotic or pyroptotic cells, as well as clearing necroptotic cells [164, 167, 168]. However, contradictory results have been observed [166].
Exposed PS can also be found in necroptotic cells after phosphorylated mixed lineage kinase-like (pMLKL) translocation to the membrane (Fig. 2). Necroptotic cells exposed to PS produce extracellular vesicles transporting pMLKL and proteins. Furthermore, after exposure to PS, pMLKL suppression can prevent necroptosis and restore cells. Finally, PS externalisation by necroptotic cells promotes phagocytosis and recognition, which may help to reduce the inflammatory response to this nonapoptotic form of cell death. Because of the specific find-me and eat-me signals produced when PS is exposed to the outer membrane and extracellular vesicles, necroptotic cell death may provide an immunologically silent window [167].
Similarly to necroptotic cells, pyroptotic cells emitted a find-me signal that was inhibited by apyrase, which converts nucleoside triphosphate to nucleoside monophosphate. According to Wang et al., findings pyroptotic cells caused by microbial infection can be effectively engulfed by either mice peritoneal macrophages or human monocytic THP-1-cell-derived macrophages. This engulfment was inhibited by the D89E mutant of MFG-E8, a phosphatidylserine-binding protein that has previously been shown to disrupt phosphatidylserine-dependent engulfment of apoptotic cells by macrophages. They found that after being treated with muramyl dipeptide, both pyroptotic and apoptotic cells adhered to a T cell immunoglobulin and mucin domain-containing 4 (Tim4; an additional phosphatidylserine-binding protein), whereas necrotic cells that had been destroyed by heat did not. This demonstrated that phosphatidylserine was activated in pyroptosis and apoptosis but not in necrosis [164]. When phagocytes are drawn to the area of cell death, they will interact with PS that is has appeared on the pyroptotic cell outer membrane either directly through scavenger receptors (TIM4) or indirectly through bridge molecules (MFG-E8). Because the mechanism is caspase 1 independent, it is unclear whether PS exposure occurs actively or passively during pyroptosis [58]. Given that the phospholipid scramblase TMEM16F can be activated by Ca2+ signalling, it would be interesting to see if such scramblases result in PS exposure during cell death mechanisms that do not involve caspase 3/7 activation, such as pyroptosis [118]. Apoptotic cells were the easiest for macrophages to consume, followed by pyroptotic cells and finally necrotic cells killed by heat. These findings suggest that pyroptotic cells, like apoptotic cells, actively stimulate macrophage phagocytosis by emitting eat-me and find-me signals [164].
Engulfment of dead cells is required for tissue homeostasis and the suppression of inflammatory responses. The process of engulfing apoptotic cells has been extensively studied, and it involves receptors on the engulfing cells that detect eat-me signals on the apoptotic cells’ outer membrane [82]. To maintain tissue homeostasis, necrotic cells must be eliminated because they may leak intracellular components that contribute to inflammation [167], as previously stated, in both in vitro and in vivo conditions, apoptotic cell clearance has been shown to be more efficient than necroptotic and pyroptotic cell engulfment [164, 167, 168]. Non-professional phagocytes digested necroptotic and pyroptotic cells much more efficiently than apoptotic cells in a study using NIH3T3 cells by Lu et al. Furthermore, they compared the ability of peritoneal macrophages, BMDM and bone marrow-derived dendritic cells to phagocytise apoptotic cells to necrotic and pyroptotic cells [164].
The processes of pyroptosis and efferocytosis in necroptosis are detailed in the previous chapter in order to reduce the pro-inflammatory effects of intracellular components that contribute to inflammation. Extensive research has been conducted on the cellular mechanism used to describe engulfed apoptotic cells. However, recent research has not revealed the cellular mechanism of necroptotic and pyroptotic cells after engulfment. As illustrated below, we believe that several cellular mechanisms in necroptosis and pyroptosis are similar to post-engulfment in apoptosis. More research is needed in necroptosis and pyroptosis to determine this.
After being recognised, classical apoptotic cells are absorbed by the efferocyte into an efferosome, a fluid-filled membrane vesicle. Efferosomes, like phagosomes that transport ingested infections, merge with early endosomes, late endosomes and then lysosomes in a highly controlled process [11]. Some of the proteins that control these merger processes are Rab GTPases and SNAREs and the merger activities deliver the hydrolytic enzymes that destroy the apoptotic cell inside the efferosome [169]. This is referred to as efferosome maturation, and it is similar to the maturation mechanisms observed following phagocytosis and endocytosis [97].
The activation of the Rab GTPases Rab5 and Rab7 is one of several similarities between the phagosome and efferosome maturation processes [139, 170]. Rab5 is attracted to efferosomes as the apoptotic cell is absorbed and remains firmly attached to them for a few moments after the cell membrane is exposed [171]. In this case, Rab5 promotes the fusion of the efferosome and the early endosomes, thereby initiating the catabolic process that eventually destroys the apoptotic cell [104]. Rab5 is converted to Rab7 shortly after the efferosome forms, and Rab7 mediates the merging of late endosomes and lysosomes to the efferosome to create a highly enzymatic hydrolysis environment capable of completely destroying the apoptotic cell [171, 172]. In contrast to phagocytosis, this efferosome maturation pathway also includes Rab17, which transports the efferosome’s broken contents to the renewing endosome, where they are exocytose. This inhibits their transfer to antigen loading compartments [172].
Furthermore, efferosomes have been shown to participate in LC3-associated phagocytosis (LAP), a process in which autophagy mediators, such as the class III phosphatidylinositol-3-kinase (PI3KCIII) complex ATG5 and ATG7, conjugate LC3 to the surface of developing efferosomes [173]. These variables then control the efferosome’s rapid expansion and the clearance of its apoptotic contents, preventing antigen presentation and polarising macrophages toward an anti-inflammatory phenotype [174]. The Medzhitov group demonstrated that antigen presentation requires contents to be directed into the conventional phagocytic pathway (for example, non-LAP). This pathway is dependent on phagosome-derived TLR signalling [138, 175]. This demonstrates that, in addition to inducing the activation of genes involved in inflammation and antigen presentation, TLR identification of pathogen products results in rapid changes in the trafficking of cargo containing TLR ligands versus cargo lacking these ligands [176]. Rab39a, GTPase that reduces autophagy in response to TLR stimulation and is required for the transfer of MHC I to phagosomes for antigen cross-presentation, may inhibit LAP after phagocytosis [177]. However, no studies on Rab39a’s function in efferocytosis have been published, so its role in efferocytosis-associated LAP is unknown.
Restricting the antigen presentation of efferosome-derived antigens is a critical reaction of phagocytes following efferocytosis, as evidenced by the existence of three concurrent mechanisms. These mechanisms include LAP, faster maturation and cargo redirected out of the maturing efferosome via Rab17 action. Efferocytes not only use non-trafficking processes, but they also prevent autoimmune reactions to efferocytosis materials. Efferocytosis is typically associated with increased levels of cytokines such as IL-10, which reduce the activity of mature T cells and promote the development of Treg cells from naive T cells [55]. As a result, T cell responses are suppressed by efferocytosis. It is critical to investigate this complex mechanism that engulfs necroptotic and pyroptotic cells. Small changes could have a different effect that benefits the drug.
Conclusion
Cell death and the clearance of dead cells are linked to a number of inflammatory disorders. To develop new disease therapeutics, it is critical to understand the molecular mechanisms underlying phagocytic clearance and the functional implications of phagocyte engulfment. The inclusion of necroptotic and pyroptotic cells as a significant, continuous contributor to overall cell death provides a novel perspective on how debris are identified, eliminated and how it contributes to inflammation. The three steps of recruitment, recognition and engulfment contribute to the efficient efferocytosis in the necroptosis and pyroptosis pathways. These three phases are mediated by the exposure and release of the find-me, eat-me and engulfment signals. As previously stated, significant progress has recently been made in our understanding of the molecular mechanisms underlying pyroptosis and necroptosis. Several markers have been discovered, and some of them point to label linkages between various cell death pathways. According to current research, necroptotic and pyroptotic dying cells release several DAMPs as a find-me signal. PS is one of the most powerful eat-me signals recognised by phagocytes in necroptotic and pyroptotic cells. Despite significant advances in our understanding of efferocytosis in necroptotic and pyroptotic cells over the last few decades, there are still many unanswered questions. Concerns about the role of efferocytosis in pathogens elimination and efferocytes metabolic remodelling are two examples. Further investigation is required to comprehend efferocytosis in necroptosis and pyroptosis in order to understand the molecular mechanisms that contribute to the discovery of new markers and how they can be therapeutically targeted.
Availability of data and materials
Not applicable.
Abbreviations
- TNF:
-
Tumor necrosis factor
- FADD:
-
FAS associated via death domain
- DAMP:
-
Damage-associated molecular pattern
- RIPK:
-
Receptor-interacting protein kinase
- MLKL:
-
Mixed lineage kinase domain-like protein
- TLR:
-
Toll-like receptor
- PAMP:
-
Pathogen-associated molecular patterns
- DR:
-
Death receptor
- GSDMD:
-
Gasdermin D
- S1P:
-
Sphingosine-1-phosphate
- LPC:
-
Lysophosphatidylcholine
- CXCL:
-
Chemokine (C-X-C motif) ligand
- ATP:
-
Adenosine triphosphate
- HMGB1:
-
High mobility group box-1
- MFG:
-
Milk fat globule
- MFG-E8:
-
Milk fat globule epidermal growth factor 8
- BMDM:
-
Bone marrow-derived macrophages
- FPR:
-
Formyl-peptide receptor
- LTB4:
-
Leukotriene B4
- TIM:
-
T cell immunoglobulin mucin
- TG2:
-
Transglutaminase 2
- PS:
-
Phosphatidylserine
- RAGE:
-
Receptor for advanced glycation end products
- PMLKL:
-
Phosphorylated mixed lineage kinase domain-like protein
- LAP:
-
LC3-associated phagocytosis
References
Doran AC, Yurdagul A, Tabas I. Efferocytosis in health and disease. Nat Rev Immunol. 2020;20:254–67.
Mehrotra P, Ravichandran KS. Drugging the efferocytosis process: concepts and opportunities. Nat Rev Drug Discov. 2022;21:601–20.
Morioka S, Maueröder C, Ravichandran KS. Living on the edge: efferocytosis at the interface of homeostasis and pathology. Immunity. 2019;50:1149–62.
Karaji N, Sattentau QJ. Efferocytosis of pathogen-infected cells. Front Immunol. 2017;8:1863.
Westman J, Grinstein S, Marques PE. Phagocytosis of necrotic debris at sites of injury and inflammation. Front Immunol. 2020;10:3030.
Kim EH, Wong SW, Martinez J. Programmed necrosis and disease: we interrupt your regular programming to bring you necroinflammation. Cell Death Differ. 2019;25:25–40.
Frank D, Vince JE. Pyroptosis versus necroptosis: similarities, differences, and crosstalk. Cell Death Differ. 2019;26:99–114.
Fredman G, Tabas I. Boosting inflammation resolution in atherosclerosis: the next frontier for therapy. Am J Pathol. 2017;187:1211–21.
Galluzzi L, Bravo-San Pedro JM, Vitale I, Aaronson SA, Abrams JM, Adam D, et al. Essential versus accessory aspects of cell death: recommendations of the NCCD 2015. Cell Death Differ. 2015;22:58–73.
Lieberman J, Wu H, Kagan JC. Gasdermin D activity in inflammation and host defense. Sci Immunol. 2019;4: eaav1447.
Yin C, Heit B. Cellular responses to the efferocytosis of apoptotic cells. Front Immunol. 2021;12: 631714.
Phagocytosis GS. An immunobiologic process. Immunity. 2016;44:463–75.
Martin CJ, Peters KN, Behar SM. Macrophages clean up: efferocytosis and microbial control. Curr Opin Microbiol. 2014;17:17–23.
Purnama CA, Meiliana A, Barliana MI, Dandan KL, Wijaya A. Apoptosis and efferocytosis in inflammatory diseases. Indones Biomed J. 2021;13:221–336.
Ge Y, Huang M, Yao YM. Efferocytosis and its role in inflammatory disorders. Front Cell Dev Biol. 2022;10: 839248.
Abbas A, Lichtman A. Basic immunology: functions and disorders of the immune system/Abul K. Abbas, Andrew H. Lichtman; illustrated by David L. Baker and Alexandra Baker. Philadelphia: Saunders/Elsevier; 2022. p. 239–43.
Signore A, Glaudemans AWJM. The molecular imaging approach to image infections and inflammation by nuclear medicine techniques. Ann Nucl Med. 2011;25:681–700.
Takeda K, Akira S. Toll-like receptors in innate immunity. Int Immunol. 2005;17:1–14.
Osorio F, Reis e Sousa C. Myeloid c-type lectin receptors in pathogen recognition and host defense. Immunity. 2011;34:651–64.
Rock KL, Kono H. The inflammatory response to cell death. Annu Rev Pathol. 2008;3:99–126.
Dunn GP, Koebel CM, Schreiber RD. Interferons, immunity and cancer immunoediting. Nat Rev Immunol. 2006;6:836–48.
Weinlich R, Oberst A, Beere HM, Green DR. Necroptosis in development, inflammation and disease. Nat Rev Mol Cell Biol. 2017;18:127–36.
Boada-Romero E, Martinez J, Heckmann BL, Green DR. The clearance of dead cells by efferocytosis. Nat Rev Mol Cell Biol. 2020;21:398–414.
Ito Y, Ofengeim D, Najafov A, Das S, Saberi S, Li Y, et al. RIPK1 mediates axonal degeneration by promoting inflammation and necroptosis in ALS. Science. 2016;353:603–8.
Ofengeim D, Ito Y, Najafov A, Zhang Y, Shan B, DeWitt JP, et al. Activation of necroptosis in multiple sclerosis. Cell Rep. 2015;10:1836–49.
Zhou W, Yuan J. Necroptosis in health and diseases. Semin Cell Dev Biol. 2014;35:14–23.
Yuan J, Najafov A, Py BF. Roles of caspases in necrotic cell death. Cell. 2016;167:1693–704.
Newton K. RIPK1 and RIPK3: critical regulators of inflammation and cell death. Trends Cell Biol. 2015;25:347–53.
Schwarzer R, Laurien L, Pasparakis M. New insights into the regulation of apoptosis, necroptosis, and pyroptosis by receptor interacting protein kinase 1 and caspase-8. Curr Opin Cell Biol. 2020;63:186–93.
Liu X, Xie X, Ren Y, Shao Z, Zhang N, Li L, et al. The role of necroptosis in disease and treatment. MedComm. 2021;2:730–55.
Grootjans S, vanden Berghe T, Vandenabeele P. Initiation and execution mechanisms of necroptosis: an overview. Cell Death Differ. 2017;24:1184–95.
Mompeán M, Li W, Li J, Laage S, Siemer AB, Bozkurt G, et al. The structure of the necrosome RIPK1-RIPK3 core, a human hetero-amyloid signaling complex. Cell. 2018;173:1244–53.
Sun L, Wang H, Wang Z, He S, Chen S, Liao D, et al. Mixed lineage kinase domain-like protein mediates necrosis signaling downstream of RIP3 kinase. Cell. 2012;148:213–27.
Zhao J, Jitkaew S, Cai Z, Choksi S, Li Q, Luo J, et al. Mixed lineage kinase domain-like is a key receptor interacting protein 3 downstream component of TNF-induced necrosis. Proc Natl Acad Sci USA. 2012;109:5322–7.
Kaczmarek A, Vandenabeele P, Krysko DV. Necroptosis: the release of damage-associated molecular patterns and its physiological relevance. Immunity. 2013;38:209–23.
Newton K, Wickliffe KE, Maltzman A, Dugger DL, Strasser A, Pham VC, et al. RIPK1 inhibits ZBP1-driven necroptosis during development. Nature. 2016;540:129–33.
Lin J, Kumari S, Kim C, Van TM, Wachsmuth L, Polykratis A, et al. RIPK1 counteracts ZBP1-mediated necroptosis to inhibit inflammation. Nature. 2016;540:124–8.
Khan N, Lawlor KE, Murphy JM, Vince JE. More to life than death: molecular determinants of necroptotic and non-necroptotic RIP3 kinase signaling. Curr Opin Immunol. 2014;26:76–89.
Kurokawa M, Kornbluth S. Caspases and kinases in a death grip. Cell. 2009;138:838–54.
Chen X, He WT, Hu L, Li J, Fang Y, Wang X, et al. Pyroptosis is driven by non-selective gasdermin-D pore and its morphology is different from MLKL channel-mediated necroptosis. Cell Res. 2016;26:1007–20.
Poon IKH, Lucas CD, Rossi AG, Ravichandran KS. Apoptotic cell clearance: basic biology and therapeutic potential. Nat Rev Immunol. 2014;14:166–80.
Coleman ML, Sahai EA, Yeo M, Bosch M, Dewar A, Olson MF. Membrane blebbing during apoptosis results from caspase-mediated activation of ROCK I. Nat Cell Biol. 2001;3:339–45.
Sebbagh M, Renvoizé C, Hamelin J, Riché N, Bertoglio J, Bréard J. Caspase-3-mediated cleavage of ROCK I induces MLC phosphorylation and apoptotic membrane blebbing. Nat Cell Biol. 2001;3:346–52.
Fackler OT, Grosse R. Cell motility through plasma membrane blebbing. J Cell Biol. 2008;81:879–84.
Tang R, Xu J, Zhang B, Liu J, Liang C, Hua J, et al. Ferroptosis, necroptosis, and pyroptosis in anticancer immunity. J Hematol Oncol. 2020;13:110.
Ding J, Wang K, Liu W, She Y, Sun Q, Shi J, et al. Pore-forming activity and structural autoinhibition of the gasdermin family. Nature. 2016;535:111–6.
Fink SL, Cookson BT. Caspase-1-dependent pore formation during pyroptosis leads to osmotic lysis of infected host macrophages. Cell Microbiol. 2006;8:1812–25.
Zhang Y, Chen X, Gueydan C, Han J. Plasma membrane changes during programmed cell deaths. Cell Res. 2018;28:9–21.
Chen Y, Chen H, Xie H, Yuan S, Gao C, Yu L, et al. Non-covalent proteasome inhibitor PI-1840 induces apoptosis and autophagy in osteosarcoma cells. Oncol Rep. 2019;41:2803–17.
Ray M, Hostetter DR, Loeb CRK, Simko J, Craik CS. Inhibition of granzyme B by PI-9 protects prostate cancer cells from apoptosis. Prostate. 2012;72:846–55.
Siegel RM. Caspases at the crossroads of immune-cell life and death. Nat Rev Immunol. 2006;6:308–17.
Wang Y, Gao W, Shi X, Ding J, Liu W, He H, et al. Chemotherapy drugs induce pyroptosis through caspase-3 cleavage of a gasdermin. Nature. 2017;547:99–103.
Rogers C, Fernandes-Alnemri T, Mayes L, Alnemri D, Cingolani G, Alnemri ES. Cleavage of DFNA5 by caspase-3 during apoptosis mediates progression to secondary necrotic/pyroptotic cell death. Nat Commun. 2017;8:14128.
Shi J, Zhao Y, Wang K, Shi X, Wang Y, Huang H, et al. Cleavage of GSDMD by inflammatory caspases determines pyroptotic cell death. Nature. 2015;526:660–5.
Kayagaki N, Stowe IB, Lee BL, O’Rourke K, Anderson K, Warming S, et al. Caspase-11 cleaves gasdermin D for non-canonical inflammasome signalling. Nature. 2015;526:666–71.
Aglietti RA, Estevez A, Gupta A, Ramirez MG, Liu PS, Kayagaki N, et al. GsdmD p30 elicited by caspase-11 during pyroptosis forms pores in membranes. Proc Natl Acad Sci USA. 2016;113:7858–63.
Sborgi L, Rühl S, Mulvihill E, Pipercevic J, Heilig R, Stahlberg H, et al. GSDMD membrane pore formation constitutes the mechanism of pyroptotic cell death. EMBO J. 2016;35:1766–78.
Liu X, Zhang Z, Ruan J, Pan Y, Magupalli VG, Wu H, et al. Inflammasome-activated gasdermin D causes pyroptosis by forming membrane pores. Nature. 2016;535:153–8.
Miao EA, Leaf IA, Treuting PM, Mao DP, Dors M, Sarkar A, et al. Caspase-1-induced pyroptosis is an innate immune effector mechanism against intracellular bacteria. Nat Immunol. 2010;11:1136–42.
Jorgensen I, Zhang Y, Krantz BA, Miao EA. Pyroptosis triggers pore-induced intracellular traps (PITs) that capture bacteria and lead to their clearance by efferocytosis. J Exp Med. 2016;213:2113–28.
Broz P, Dixit VM. Inflammasomes: mechanism of assembly, regulation and signalling. Nat Rev Immunol. 2016;16:407–20.
Muñoz-Planillo R, Kuffa P, Martínez-Colón G, Smith BL, Rajendiran TM, Núñez G. K+ efflux is the common trigger of NLRP3 inflammasome activation by bacterial toxins and particulate matter. Immunity. 2013;38:1142–53.
He Y, Zeng MY, Yang D, Motro B, Núñez G. NEK7 is an essential mediator of NLRP3 activation downstream of potassium efflux. Nature. 2016;530:354–7.
Boucher D, Monteleone M, Coll RC, Chen KW, Ross CM, Teo JL, et al. Caspase-1 self-cleavage is an intrinsic mechanism to terminate inflammasome activity. J Exp Med. 2018;215:827–40.
Ramirez MLG, Poreba M, Snipas SJ, Groborz K, Drag M, Salvesen GS. Extensive peptide and natural protein substrate screens reveal that mouse caspase-11 has much narrower substrate specificity than caspase-1. J Biol Chem. 2018;293:7058–67.
Baker PJ, Boucher D, Bierschenk D, Tebartz C, Whitney PG, D’Silva DB, et al. NLRP3 inflammasome activation downstream of cytoplasmic LPS recognition by both caspase-4 and caspase-5. Eur J Immunol. 2015;45:2918–26.
Rühl S, Broz P. Caspase-11 activates a canonical NLRP3 inflammasome by promoting K+ efflux. Eur J Immunol. 2015;45:2927–36.
Conos SA, Chen KW, de Nardo D, Hara H, Whitehead L, Núñez G, et al. Active MLKL triggers the NLRP3 inflammasome in a cell-intrinsic manner. Proc Natl Acad Sci USA. 2017;114:E961–9.
Gutierrez KD, Davis MA, Daniels BP, Olsen TM, Ralli-Jain P, Tait SWG, et al. MLKL activation triggers NLRP3-mediated processing and release of IL-1β independently of gasdermin-D. J Immunol. 2017;198:2156–64.
Brault M, Oberst A. Controlled detonation: evolution of necroptosis in pathogen defense. Immunol Cell Biol. 2017;95:131–6.
Naderer T, Fulcher MC. Targeting apoptosis pathways in infections. J Leukoc Biol. 2018;103:275–85.
Kaiser WJ, Upton JW, Long AB, Livingston-Rosanoff D, Daley-Bauer LP, Hakem R, et al. RIP3 mediates the embryonic lethality of caspase-8-deficient mice. Nature. 2011;471:368–73.
Oberst A, Dillon CP, Weinlich R, McCormick LL, Fitzgerald P, Pop C, et al. Catalytic activity of the caspase-8-FLIP(L) complex inhibits RIPK3-dependent necrosis. Nature. 2011;471:363–8.
Cai Z, Jitkaew S, Zhao J, Chiang HC, Choksi S, Liu J, et al. Plasma membrane translocation of trimerized MLKL protein is required for TNF-induced necroptosis. Nat Cell Biol. 2014;16:55–65.
Hildebrand JM, Tanzer MC, Lucet IS, Young SN, Spall SK, Sharma P, et al. Activation of the pseudokinase MLKL unleashes the four-helix bundle domain to induce membrane localization and necroptotic cell death. Proc Natl Acad Sci USA. 2014;111:15072–7.
Chen X, Li W, Ren J, Huang D, He WT, Song Y, et al. Translocation of mixed lineage kinase domain-like protein to plasma membrane leads to necrotic cell death. Cell Res. 2014;24:105–21.
de Vasconcelos NM, van Opdenbosch N, van Gorp H, Parthoens E, Lamkanfi M. Single-cell analysis of pyroptosis dynamics reveals conserved GSDMD-mediated subcellular events that precede plasma membrane rupture. Cell Death Differ. 2019;26:146–61.
Evavold CL, Ruan J, Tan Y, Xia S, Wu H, Kagan JC. The pore-forming protein gasdermin D regulates interleukin-1 secretion from living macrophages. Immunity. 2018;48:35-44.e6.
Heilig R, Dick MS, Sborgi L, Meunier E, Hiller S, Broz P. The Gasdermin-D pore acts as a conduit for IL-1β secretion in mice. Eur J Immunol. 2018;48:584–92.
Russo HM, Rathkey J, Boyd-Tressler A, Katsnelson MA, Abbott DW, Dubyak GR. Active caspase-1 induces plasma membrane pores that precede pyroptotic lysis and are blocked by lanthanides. J Immunol. 2016;197:1353–67.
Devitt A, Marshall LJ. The innate immune system and the clearance of apoptotic cells. J Leukoc Biol. 2011;90:447–57.
Arandjelovic S, Ravichandran KS. Phagocytosis of apoptotic cells in homeostasis. Nat Immunol. 2015;16:907–17.
Birge RB, Boeltz S, Kumar S, Carlson J, Wanderley J, Calianese D, et al. Phosphatidylserine is a global immunosuppressive signal in efferocytosis, infectious disease, and cancer. Cell Death Differ. 2016;23:962–78.
Henson PM. Cell removal: efferocytosis. Annu Rev Cell Dev Biol. 2017;33:127–44.
Hoffmann PR, DeCathelineau AM, Ogden CA, Leverrier Y, Bratton DL, Daleke DL, et al. Phosphatidylserine (PS) induces PS receptor-mediated macropinocytosis and promotes clearance of apoptotic cells. J Cell Biol. 2001;155:649–59.
DeCathelineau AM, Henson PM. The final step in programmed cell death: phagocytes carry apoptotic cells to the grave. Essays Biochem. 2003;39:105–17.
Kumar S, Birge RB. Efferocytosis. Curr Biol. 2016;26:R558–9.
Monks J, Rosner D, Geske FJ, Lehman L, Hanson L, Neville MC, et al. Epithelial cells as phagocytes: apoptotic epithelial cells are engulfed by mammary alveolar epithelial cells and repress inflammatory mediator release. Cell Death Differ. 2005;12:107–14.
Ross GD, Reed W, Dalzell JG, Becker SE, Hogg N. Macrophage cytoskeleton association with CR3 and CR4 regulates receptor mobility and phagocytosis of iC3b-opsonized erythrocytes. J Leukoc Biol. 1992;51:109–17.
Park SY, Jung MY, Lee SJ, Kang KB, Gratchev A, Riabov V, et al. Stabilin-1 mediates phosphatidylserine-dependent clearance of cell corpses in alternatively activated macrophages. J Cell Sci. 2009;122:3365–73.
Anderson CL, Shen L, Eicher DM, Wewers MD, Gill JK. Phagocytosis mediated by three distinct Fc gamma receptor classes on human leukocytes. J Exp Med. 1990;171:1333–45.
Hochreiter-Hufford A, Ravichandran KS. Clearing the dead: apoptotic cell sensing, recognition, engulfment, and digestion. Cold Spring Harb Perspect Biol. 2013;5: a008748.
Green DR, Oguin TH, Martinez J. The clearance of dying cells: table for two. Cell Death Differ. 2016;23:915–26.
Zent CS, Elliott MR. Maxed out macs: physiologic cell clearance as a function of macrophage phagocytic capacity. FEBS J. 2017;284:1021–39.
Fond AM, Ravichandran KS. Clearance of dying cells by phagocytes: mechanisms and implications for disease pathogenesis. Adv Exp Med Biol. 2016;930:25–49.
Overholtzer M, Mailleux AA, Mouneimne G, Normand G, Schnitt SJ, King RW, et al. A nonapoptotic cell death process, entosis, that occurs by cell-in-cell invasion. Cell. 2007;131:966–79.
Flannagan RS, Jaumouillé V, Grinstein S. The cell biology of phagocytosis. Annu Rev Pathol. 2012;7:61–98.
Pauwels AM, Trost M, Beyaert R, Hoffmann E. Patterns, receptors, and signals: regulation of phagosome maturation. Trends Immunol. 2017;38:407–22.
Brewer JM, Pollock KGJ, Tetley L, Russell DG. Vesicle size influences the trafficking, processing, and presentation of antigens in lipid vesicles. J Immunol. 2004;173:6143–50.
Doshi N, Mitragotri S. Macrophages recognize size and shape of their targets. PLoS ONE. 2010;5: e10051.
Champion JA, Mitragotri S. Role of target geometry in phagocytosis. Proc Natl Acad Sci USA. 2006;103:4930–4.
Branzk N, Lubojemska A, Hardison SE, Wang Q, Gutierrez MG, Brown GD, et al. Neutrophils sense microbe size and selectively release neutrophil extracellular traps in response to large pathogens. Nat Immunol. 2014;15:1017–25.
Greenlee-Wacker MC. Clearance of apoptotic neutrophils and resolution of inflammation. Immunol Rev. 2016;273:357–70.
Gude DR, Alvarez SE, Paugh SW, Mitra P, Yu J, Griffiths R, et al. Apoptosis induces expression of sphingosine kinase 1 to release sphingosine-1-phosphate as a “come-and-get-me” signal. FASEB J. 2008;22:2629–38.
Truman LA, Ford CA, Pasikowska M, Pound JD, Wilkinson SJ, Dumitriu IE, et al. CX3CL1/fractalkine is released from apoptotic lymphocytes to stimulate macrophage chemotaxis. Blood. 2008;112:5026–36.
Elliott MR, Chekeni FB, Trampont PC, Lazarowski ER, Kadl A, Walk SF, et al. Nucleotides released by apoptotic cells act as a find-me signal to promote phagocytic clearance. Nature. 2009;461:282–6.
Chekeni FB, Elliott MR, Sandilos JK, Walk SF, Kinchen JM, Lazarowski ER, et al. Pannexin 1 channels mediate “find-me” signal release and membrane permeability during apoptosis. Nature. 2010;467:863–7.
Garris CS, Wu L, Acharya S, Arac A, Blaho VA, Huang Y, et al. Defective sphingosine 1-phosphate receptor 1 (S1P1) phosphorylation exacerbates TH17-mediated autoimmune neuroinflammation. Nat Immunol. 2013;14:1166–72.
Ravichandran KS. Find-me and eat-me signals in apoptotic cell clearance: progress and conundrums. J Exp Med. 2010;207:1807–17.
Elliott MR, Ravichandran KS. The dynamics of apoptotic cell clearance. Dev Cell. 2016;38:147–60.
Idzko M, Ferrari D, Eltzschig HK. Nucleotide signalling during inflammation. Nature. 2014;509:310–7.
Koizumi S, Shigemoto-Mogami Y, Nasu-Tada K, Shinozaki Y, Ohsawa K, Tsuda M, et al. UDP acting at P2Y6 receptors is a mediator of microglial phagocytosis. Nature. 2007;446:1091–5.
Frey B, Rubner Y, Kulzer L, Werthmöller N, Weiss EM, Fietkau R, et al. Antitumor immune responses induced by ionizing irradiation and further immune stimulation. Cancer Immunol Immunother. 2014;63:29–36.
Cekic C, Linden J. Purinergic regulation of the immune system. Nat Rev Immunol. 2016;16:177–92.
Köröskényi K, Duró E, Pallai A, Sarang Z, Kloor D, Ucker DS, et al. Involvement of adenosine A2A receptors in engulfment-dependent apoptotic cell suppression of inflammation. J Immunol. 2011;186:7144–55.
Yamaguchi H, Maruyama T, Urade Y, Nagata S. Immunosuppression via adenosine receptor activation by adenosine monophosphate released from apoptotic cells. Elife. 2014;3: e02172.
Wang Q, Ju X, Zhou Y, Chen K. Necroptotic cells release find-me signal and are engulfed without proinflammatory cytokine production. In Vitro Cell Dev Biol Anim. 2015;51:1033–9.
Atkin-Smith GK. Phagocytic clearance of apoptotic, necrotic, necroptotic and pyroptotic cells. Biochem Soc Trans. 2021;49:793–804.
Chen J, Kuroki S, Someda M, Yonehara S. Interferon-γ induces the cell surface exposure of phosphatidylserine by activating the protein MLKL in the absence of caspase-8 activity. J Biol Chem. 2019;294:11994–2006.
Gong YN, Guy C, Olauson H, Becker JU, Yang M, Fitzgerald P, et al. ESCRT-III acts downstream of MLKL to regulate necroptotic cell death and its consequences. Cell. 2017;169:286-300.e16.
Gerlach BD, Marinello M, Heinz J, Rymut N, Sansbury BE, Riley CO, et al. Resolvin D1 promotes the targeting and clearance of necroptotic cells. Cell Death Differ. 2020;27:525–39.
Yang D, He Y, Muñoz-Planillo R, Liu Q, Núñez G. Caspase-11 requires the pannexin-1 channel and the purinergic P2X7 pore to mediate pyroptosis and endotoxic shock. Immunity. 2015;43:923–32.
Westman J, Papareddy P, Dahlgren MW, Chakrakodi B, Norrby-Teglund A, Smeds E, et al. Extracellular histones induce chemokine production in whole blood ex vivo and leukocyte recruitment in vivo. PLoS Pathog. 2015;11: e1005319.
de Oliveira S, Rosowski EE, Huttenlocher A. Neutrophil migration in infection and wound repair: going forward in reverse. Nat Rev Immunol. 2016;16:378–91.
McDonald B, Pittman K, Menezes GB, Hirota SA, Slaba I, Waterhouse CCM, et al. Intravascular danger signals guide neutrophils to sites of sterile inflammation. Science. 2010;330:362–6.
Honda M, Takeichi T, Hashimoto S, Yoshii D, Isono K, Hayashida S, et al. Intravital imaging of neutrophil recruitment reveals the efficacy of FPR1 blockade in hepatic ischemia-reperfusion injury. J Immunol. 2017;198:1718–28.
Crouser ED, Shao G, Julian MW, MacRe JE, Shadel GS, Tridandapani S, et al. Monocyte activation by necrotic cells is promoted by mitochondrial proteins and formyl peptide receptors. Crit Care Med. 2009;37:2000–9.
Griffith JW, Sokol CL, Luster AD. Chemokines and chemokine receptors: positioning cells for host defense and immunity. Annu Rev Immunol. 2014;32:659–702.
Girbl T, Lenn T, Perez L, Rolas L, Barkaway A, Thiriot A, et al. Distinct compartmentalization of the chemokines CXCL1 and CXCL2 and the atypical receptor ACKR1 determine discrete stages of neutrophil diapedesis. Immunity. 2018;49:1062-1076.e6.
Kienle K, Lämmermann T. Neutrophil swarming: an essential process of the neutrophil tissue response. Immunol Rev. 2016;273:76–93.
Lämmermann T, Afonso PV, Angermann BR, Wang JM, Kastenmüller W, Parent CA, et al. Neutrophil swarms require LTB4 and integrins at sites of cell death in vivo. Nature. 2013;498:371–5.
Afonso PV, Janka-Junttila M, Lee YJ, McCann CP, Oliver CM, Aamer KA, et al. LTB4 is a signal-relay molecule during neutrophil chemotaxis. Dev Cell. 2012;22:1079–91.
Yoo SK, Starnes TW, Deng Q, Huttenlocher A. Lyn is a redox sensor that mediates leukocyte wound attraction in vivo. Nature. 2011;480:109–12.
Hattori H, Subramanian KK, Sakai J, Jia Y, Li Y, Porter TF, et al. Small-molecule screen identifies reactive oxygen species as key regulators of neutrophil chemotaxis. Proc Natl Acad Sci USA. 2010;107:3546–51.
Kuiper JWP, Sun C, Magalhães MAO, Glogauer M. Rac regulates PtdInsP3 signaling and the chemotactic compass through a redox-mediated feedback loop. Blood. 2011;118:6164–71.
Burnstock G, Boeynaems JM. Purinergic signalling and immune cells. Purinergic Signal. 2014;10:529–64.
Wang J, Kubes P. A Reservoir of mature cavity macrophages that can rapidly invade visceral organs to affect tissue repair. Cell. 2016;165:668–78.
Gardai SJ, McPhillips KA, Frasch SC, Janssen WJ, Starefeldt A, Murphy-Ullrich JE, et al. Cell-surface calreticulin initiates clearance of viable or apoptotic cells through trans-activation of LRP on the phagocyte. Cell. 2005;123:321–34.
Park SY, Jung MY, Kim HJ, Lee SJ, Kim SY, Lee BH, et al. Rapid cell corpse clearance by stabilin-2, a membrane phosphatidylserine receptor. Cell Death Differ. 2008;15:192–201.
Rodriguez-Manzanet R, Sanjuan MA, Wu HY, Quintana FJ, Xiao S, Anderson AC, et al. T and B cell hyperactivity and autoimmunity associated with niche-specific defects in apoptotic body clearance in TIM-4-deficient mice. Proc Natl Acad Sci USA. 2010;107:8706–11.
He M, Kubo H, Morimoto K, Fujino N, Suzuki T, Takahasi T, et al. Receptor for advanced glycation end products binds to phosphatidylserine and assists in the clearance of apoptotic cells. EMBO Rep. 2011;12:358–64.
Mazaheri F, Breus O, Durdu S, Haas P, Wittbrodt J, Gilmour D, et al. Distinct roles for BAI1 and TIM-4 in the engulfment of dying neurons by microglia. Nat Commun. 2014;5:4046.
Toda S, Segawa K, Nagata S. MerTK-mediated engulfment of pyrenocytes by central macrophages in erythroblastic islands. Blood. 2014;123:3963–71.
Nepal S, Tiruppathi C, Tsukasaki Y, Farahany J, Mittal M, Rehman J, et al. STAT6 induces expression of Gas6 in macrophages to clear apoptotic neutrophils and resolve inflammation. Proc Natl Acad Sci USA. 2019;116:16513–8.
Rymut N, Heinz J, Sadhu S, Hosseini Z, Riley CO, Marinello M, et al. Resolvin D1 promotes efferocytosis in aging by limiting senescent cell-induced MerTK cleavage. FASEB J. 2020;34:597–609.
Sághy T, Köröskényi K, Hegedűs K, Antal M, Bankó C, Bacsó Z, et al. Loss of transglutaminase 2 sensitizes for diet-induced obesity-related inflammation and insulin resistance due to enhanced macrophage c-Src signaling. Cell Death Dis. 2019;10:439.
Park YJ, Liu G, Lorne EF, Zhao X, Wang J, Tsuruta Y, et al. PAI-1 inhibits neutrophil efferocytosis. Proc Natl Acad Sci USA. 2008;105:11784–9.
Segawa K, Kurata S, Yanagihashi Y, Brummelkamp TR, Matsuda F, Nagata S. Caspase-mediated cleavage of phospholipid flippase for apoptotic phosphatidylserine exposure. Science. 2014;344:1164–8.
Elliott MR, Koster KM, Murphy PS. Efferocytosis signaling in the regulation of macrophage inflammatory responses. J Immunol. 2017;198:1387–94.
Hanayama R, Tanaka M, Miyasaka K, Aozasa K, Koike M, Uchiyama Y, et al. Autoimmune disease and impaired uptake of apoptotic cells in MFG-E8-deficient mice. Science. 2004;304:1147–50.
Hu CY, Wu CS, Tsai HF, Chang SK, Tsai WI, Hsu PN. Genetic polymorphism in milk fat globule-EGF factor 8 (MFG-E8) is associated with systemic lupus erythematosus in human. Lupus. 2009;18:676–81.
Soki FN, Koh AJ, Jones JD, Kim YW, Dai J, Keller ET, et al. Polarization of prostate cancer-associated macrophages is induced by milk fat globule-EGF factor 8 (MFG-E8)-mediated efferocytosis. J Biol Chem. 2014;289:24560–72.
Pulanco MC, Cosman J, Ho M-M, Huynh J, Fing K, Turcu J, et al. Complement protein C1q enhances macrophage foam cell survival and efferocytosis. J Immunol. 2017;198:472–80.
Nishi C, Toda S, Segawa K, Nagata S. Tim4- and MerTK-mediated engulfment of apoptotic cells by mouse resident peritoneal macrophages. Mol Cell Biol. 2014;34:1512–20.
Rantakari P, Patten DA, Valtonen J, Karikoski M, Gerke H, Dawes H, et al. Stabilin-1 expression defines a subset of macrophages that mediate tissue homeostasis and prevent fibrosis in chronic liver injury. Proc Natl Acad Sci USA. 2016;113:9298–303.
Voss OH, Tian L, Murakami Y, Coligan JE, Krzewski K. Emerging role of CD300 receptors in regulating myeloid cell efferocytosis. Mol Cell Oncol. 2015;2: e964625.
Tian L, Choi SC, Lee HN, Murakami Y, Qi CF, Sengottuvelu M, et al. Enhanced efferocytosis by dendritic cells underlies memory T-cell expansion and susceptibility to autoimmune disease in CD300f-deficient mice. Cell Death Differ. 2016;23:1086–96.
Friggeri A, Yang Y, Banerjee S, Park YJ, Liu G, Abraham E. HMGB1 inhibits macrophage activity in efferocytosis through binding to the αvβ3-integrin. Am J Physiol Cell Physiol. 2010;299:C1267–76.
Wang X, Bu HF, Zhong W, Asai A, Zhou Z, di Tan X. MFG-E8 and HMGB1 are involved in the mechanism underlying alcohol-induced impairment of macrophage efferocytosis. Mol Med. 2013;19:170–82.
Banerjee S, de Freitas A, Friggeri A, Zmijewski JW, Liu G, Abraham E. Intracellular HMGB1 negatively regulates efferocytosis. J Immunol. 2011;187:4686–94.
Erwig LP, McPhilips KA, Wynes MW, Ivetic A, Ridley AJ, Henson PM. Differential regulation of phagosome maturation in macrophages and dendritic cells mediated by Rho GTPases and ezrin-radixin-moesin (ERM) proteins. Proc Natl Acad Sci USA. 2006;103:12825–30.
Nakaya M, Tanaka M, Okabe Y, Hanayama R, Nagata S. Opposite effects of Rho family GTPases on engulfment of apoptotic cells by macrophages. J Biol Chem. 2006;281:8836–42.
Moon C, Lee YJ, Park HJ, Chong YH, Kang JL. N-Acetylcysteine inhibits RhoA and promotes apoptotic cell clearance during intense lung inflammation. Am J Respir Crit Care Med. 2010;181:374–87.
Wang Q, Imamura R, Motani K, Kushiyama H, Nagata S, Suda T. Pyroptotic cells externalize eat-me and release find-me signals and are efficiently engulfed by macrophages. Int Immunol. 2013;25:363–72.
Brouckaert G, Kalai M, Krysko DV, Saelens X, Vercammen D, Ndlovu M, et al. Phagocytosis of necrotic cells by macrophages is phosphatidylserine dependent and does not induce inflammatory cytokine production. Mol Biol Cell. 2004;15:1089–100.
Lu J, Shi W, Liang B, Chen C, Wu R, Lin H, et al. Efficient engulfment of necroptotic and pyroptotic cells by nonprofessional and professional phagocytes. Cell Discov. 2019;5:39.
Zargarian S, Shlomovitz I, Erlich Z, Hourizadeh A, Ofir-Birin Y, Croker BA, et al. Phosphatidylserine externalization, “necroptotic bodies” release, and phagocytosis during necroptosis. PLoS Biol. 2017;15: e2002711.
Klöditz K, Fadeel B. Three cell deaths and a funeral: macrophage clearance of cells undergoing distinct modes of cell death. Cell Death Discov. 2019;5:69.
Taefehshokr N, Yin C, Heit B. Rab GTPases in the differential processing of phagocytosed pathogens versus efferocytosed apoptotic cells. Histol Histopathol. 2021;36:123–35.
Nakayama M, Akiba H, Takeda K, Kojima Y, Hashiguchi M, Azuma M, et al. Tim-3 mediates phagocytosis of apoptotic cells and cross-presentation. Blood. 2009;113:3821–30.
Akakura S, Singh S, Spataro M, Akakura R, Kim JI, Albert ML, et al. The opsonin MFG-E8 is a ligand for the αvβ5 integrin and triggers DOCK180-dependent Rac1 activation for the phagocytosis of apoptotic cells. Exp Cell Res. 2004;292:403–16.
Torr EE, Gardner DH, Thomas L, Goodall DM, Bielemeier A, Willetts R, et al. Apoptotic cell-derived ICAM-3 promotes both macrophage chemoattraction to and tethering of apoptotic cells. Cell Death Differ. 2012;19:671–9.
Païdassi H, Tacnet-Delorme P, Garlatti V, Darnault C, Ghebrehiwet B, Gaboriaud C, et al. C1q binds phosphatidylserine and likely acts as a multiligand-bridging molecule in apoptotic cell recognition. J Immunol. 2008;180:2329–38.
Scannell M, Flanagan MB, deStefani A, Wynne KJ, Cagney G, Godson C, et al. Annexin-1 and peptide derivatives are released by apoptotic cells and stimulate phagocytosis of apoptotic neutrophils by macrophages. J Immunol. 2007;178:4595–605.
Poon IKH, Hulett MD, Parish CR. Molecular mechanisms of late apoptotic/necrotic cell clearance. Cell Death Differ. 2010;17:381–97.
Savill J, Dransfield I, Gregory C, Haslett C. A blast from the past: clearance of apoptotic cells regulates immune responses. Nat Rev Immunol. 2002;2:965–75.
Manfredi AA, Rovere P, Heltai S, Galati G, Nebbia G, Tincani A, et al. Apoptotic cell clearance in systemic lupus erythematosus: II. Role of β2-glycoprotein I. Arthritis Rheum. 1998;41:215–23.
Acknowledgements
We acknowledge the financial support from Padjadjaran University and Prodia Clinical Laboratory, Indonesia for this work.
Funding
This work was supported by Prodia Clinical Laboratory for CAP.
Author information
Authors and Affiliations
Contributions
CAP and AM conceived the manuscript. CAP wrote the manuscript and prepared the figures. AM, MIB, and KLD read and edited the manuscript. All authors read and approved the final manuscript.
Authors’ information
Chandra Agung Purnama is a Ph.D. student from Padjajaran University. Melisa Intan Barliana is Professor of Department Biological Pharmacy Biotechnology from Padjadjaran University. Keri Lestari Dandan is Professor of Department Pharmacology and Clinical Pharmacy from Padjadjaran University. Anna Meiliana is lecturer in doctoral program of Department Pharmacology and Clinical Pharmacy and committee in Prodia Education and Research Institute.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent of publication
All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Purnama, C.A., Meiliana, A., Barliana, M.I. et al. Update of cellular responses to the efferocytosis of necroptosis and pyroptosis. Cell Div 18, 5 (2023). https://doi.org/10.1186/s13008-023-00087-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13008-023-00087-6