
Abstract
Background
The incidence of neoplasia after surgery has not been sufficiently evaluated in patients with ulcerative colitis (UC), particularly in the Japanese population, and it is not clear whether surveillance endoscopy is effective in detecting dysplasia/cancer in the remnant rectum or pouch. The aims of this study were to assess and compare postoperative development of dysplasia/cancer in patients with UC who underwent ileorectal anastomosis (IRA) or ileal pouch-anal anastomosis (IPAA) and to evaluate the effectiveness of postoperative surveillance endoscopy.
Methods
One hundred twenty patients who received postoperative surveillance endoscopy were retrospectively reviewed for development of dysplasia/cancer in the remnant rectal mucosa or pouch.
Results
Three hundred seventy-nine endoscopy sessions were conducted for 30 patients after IRA, while 548 pouch endoscopy sessions were conducted for 90 patients after IPAA. In the IRA group, 5 patients developed dysplasia/cancer during postoperative surveillance and in all cases, neoplasia was detected at an early stage. In the IRA group, no patient developed neoplasia within 10 years of diagnosis; the cumulative incidence of neoplasia after disease onset was 7.2, 12.0, and 23.9 % at 15, 20, and 25 years, respectively. In one case after stapled IPAA, dysplasia was found at the ileal pouch; a subsequent 9 endoscopy sessions in 8 years did not detect any dysplasia. Neoplasia was found more frequently during postoperative surveillance in the IRA group than in the IPAA group (p = .0028). The cumulative incidence of neoplasia after IRA was 3.8, 8.7, and 21.7 % at 10, 15, and 20 years, respectively, and that after IPAA was 1.6 % at 20 years.
Conclusions
The cumulative incidence of neoplasia after IPAA was minimal. Those who underwent IRA had a greater risk of developing neoplasia than those who underwent IPAA, although postoperative surveillance endoscopy was able to detect dysplasia/cancer at an early stage. IRA can be the surgical procedure of choice only in selected cases in which it would be of benefit to the patient, with more careful surveillance.
Similar content being viewed by others


Background
Cancer development in the ileal pouch and the remnant rectum has been the concern after surgical resection for patients with ulcerative colitis (UC) [1, 2]. Patients who underwent ileo-rectal anastomosis (IRA) are known to be at risk for the development of rectal cancer and require surveillance colonoscopy as those who have not received surgery [3]. BSG guidelines suggest the way of pouch surveillance after IPAA with admitting that there is no clear evidence for pouch surveillance [4]. However, the effectiveness of surveillance colonoscopy for patients with UC remains unclear.
Ileorectal anastomosis (IRA) used to be the surgical procedure for UC, which includes a total abdominal colectomy with anastomosis between the ileum and the rectum [5]. The major disadvantage of IRA is that risk of recurrent proctitis and neoplasia transformation remained in the remnant rectum. In 1978, Parks et al. [6] reported conducting a total proctocolectomy with ileal pouch-anal anastomosis (IPAA). Since then, IPAA has become the standard surgical treatment for patients with UC in most cases.
It has been reported that the risk of postoperative neoplasia is lower in patients with UC receiving IPAA due to excision of the rectum than in those receiving IRA [1, 2, 7–12]. However, cases of dysplasia/cancer have been reported even after IPAA; thus, IPAA does not completely eliminate the risk of neoplasia transformation [1, 2, 12–20]. Postoperative neoplasias have been detected at the anal transitional zone (ATZ) or in the pouch. Prior neoplasia was reported to be a risk factor for postoperative dysplasia/cancer development [1, 2, 13, 14, 21].
Kariv et al. [1] reported that the cumulative incidence of pouch neoplasia after IPAA was 1.3 and 4.2 % at 10 and 20 years, respectively, and Derikx et al. [2] reported a cumulative incidence of 2.0 and 6.9 % at 10 and 20 years, respectively. There are two major methods of reconstruction in IPAA: hand-sewn IPAA with mucosectomy and stapled IPAA without mucosectomy. There has been debate regarding the relative oncological risks of these techniques. There have been many reported cases in which stapled IPAA was selected with neoplasia as a surgical indication [1, 2, 19, 20, 22, 23]. On the other hand, Sagayama et al. [21] reported that the incidence of dysplasia in the mucosectomy area was as high as 4.4 %; therefore, they recommended performing hand-sewn IPAA with mucosectomy.
IPAA has replaced IRA for most UC surgeries due to postoperative inflammation and the risk of neoplasia development in the remnant rectum with IRA. However, IRA has several advantages over IPAA in terms of anal and sexual functions and fecundity and thus, IRA is currently considered in selected cases [7–10]. In particular, laparoscopic IRA may decrease postoperative adhesions of the fallopian tubes, increasing the probability of spontaneous pregnancy [24]. In selecting IRA for these patients, it is vital to clarify the risk of neoplasia development after IRA and the effectiveness of postoperative surveillance endoscopy, particularly whether it can detect neoplasia at an early stage. In some studies of IRA, no patient developed dysplasia/cancer within 10 years of diagnosis [9–11, 25, 26], although the risk of neoplasia transformation increased with longer follow-up [9–11]. Most patients who developed cancer after IRA presented at an advanced stage, when the prognosis was poor [9–11, 27]. There are no guidelines regarding surveillance after IRA, and the effectiveness of early detection of neoplasia is unclear.
We previously reported a postoperative surveillance cohort in 2011 with data until 2008 [28] and have updated the data with an additional 6 years of follow-up. We have shown a relatively high incidence of neoplasia in IRA series [29]. The aims of the current study were to assess and compare postoperative development of dysplasia/cancer for patients with UC between the two surgical procedures and to evaluate the effectiveness of postoperative surveillance endoscopy in our series.
Methods
Patients
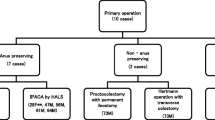
One hundred forty-four patients with UC underwent either IRA or IPAA in our institute between 1965 and 2014. Of these, 24 patients were excluded from the study because they did not receive endoscopy after surgery. For UC patients with coexisting colorectal cancer or dysplasia, hand-sewn IPAA has been preferentially performed in our institution. A total of 120 patients were retrospectively reviewed for development of dysplasia/cancer in the remnant rectal mucosa or pouch, based on endoscopic and pathological findings. This study was carried out with the approval of the Ethical Review Board of The University of Tokyo.
Surveillance endoscopy
Surveillance endoscopy was conducted annually in most cases. In addition to conventional observation, the indigo carmine dye-spraying method was performed for better visualization of mucosal lesions. Targeted biopsy specimens were taken from lesions suggestive of dysplasia, and random biopsy specimens were taken from apparently normal flat mucosa in the remnant rectum after IRA and from those in the ATZ area or pouch after IPAA. Dysplasia was graded according to Riddell’s classification [30] into high-grade dysplasia (HGD) and low-grade dysplasia (LGD).
Statistical analyses
For analysis of clinicopathological variables, unpaired t tests or Wilcoxon rank-sum tests were used for comparison of continuous variables and the Pearson chi-square test and Fisher’s exact test (if expected cell counts were <5) for categorical variables. The cumulative incidence of neoplasia after surgery was calculated using a Kaplan-Meier curve. A log-rank test was used to compare incidences between the surgical procedures. All analyses were performed with JMP 10.0 software (SAS Institute Japan, Tokyo, Japan), and differences were considered statistically significant at p < .05.
Results
A total of 927 endoscopy sessions after surgery were conducted for 120 patients with UC who underwent either IRA or IPAA (median 5 times, range 1–34). These included 379 endoscopy sessions for 30 patients after IRA and 548 pouch endoscopy sessions for 90 patients after IPAA. Patient characteristics are shown in Table 1.
IRA was the surgical procedure of choice before the 1980s in our institute mainly for medically refractory UC. In the only case of IRA performed for colon cancer, bowel obstruction due to the lesion had led to perforation of the ileum and a prior ileostomy, and it was difficult in this case to perform a total proctocolectomy because of the peritoneal adhesion. Most cases of dysplasia/cancer were in the IPAA group, and the disease duration at surgery in this group was longer than that in the IRA group (p = .0017). When cases of dysplasia/cancer were excluded and only refractory cases compared, there was no significant difference in disease duration at surgery between the IPAA and IRA groups (p = .0801). There were no significant differences in gender or age at surgery (p = .83, p = .48, respectively). Postoperative follow-up duration in the IRA group was longer than that in the IPAA group (p < .0001). There was no significant difference in total disease duration between the groups (p = .21).
Five patients who underwent IRA developed dysplasia or cancer during postoperative surveillance (Table 2). HGD was detected in the remnant rectal mucosa in 2 cases and LGD in 3 cases at the time of surveillance colonoscopy. Of these, 4 patients underwent surgical resection, including hand-sewn IPAA in 2 cases, abdominoperineal resection in 1 case, and transanal resection in 1 case. The other patient continued endoscopic follow-up without HGD being detected thereafter and ultimately discontinued surveillance due to age. Final pathological diagnoses for the surgical specimens were carcinoma with submucosal invasion in 2 cases and HGD in 2 cases. In 1 case with stapled IPAA, dysplasia was initially found in the ileal pouch, while subsequent 9 endoscopy sessions over 8 years did not detect dysplasia. In 1 patient who had undergone hand-sewn IPAA due to colitis-associated cancer, HGD was detected in the ileal pouch 2 years after IPAA. This patient underwent pouch excision, and the lesion proved to be a recurrence via dissemination rather than a newly developed neoplasia. In the present study, postoperative development of neoplasia was found mainly in refractory cases, with only 1 case of recurrence of preoperative dysplasia/cancer.
Cumulative incidences of neoplasia by surgical technique are shown in Fig. 1. The cumulative incidence of neoplasia after disease onset in the IRA group was 7.2, 12.0, and 23.9 % at 15, 20, and 25 years, respectively. No patient developed dysplasia/cancer within 10 years of diagnosis. Neoplasias were found more frequently in the IRA group than in the IPAA group (p = .0028). When cases of dysplasia/cancer were excluded and only refractory cases compared, the cumulative incidence of neoplasia after disease onset in the IRA group was 7.4, 12.6, and 24.6 % at 15, 20, and 25 years, respectively, and the difference between the IRA and IPAA group remained the same (p = .0227). The cumulative incidence was also estimated from the point of surgery. The cumulative incidence of neoplasia after IRA was 3.8, 8.7, and 21.7 % at 10, 15, and 20 years, respectively, and that after IPAA was 1.6 % at 20 years.

Cumulative incidence of neoplasia by surgical technique. Cumulative incidence calculated using the Kaplan-Meier method; p value calculated using the log-rank test. IRA ileorectal anastomosis, IPAA ileal pouch-anal anastomosis
Discussion
In the present study, the cumulative incidence of dysplasia/cancer in the Japanese patients with UC who underwent IRA was 7.2, 12.0, and 23.9 % at 15, 20, and 25 years after disease onset, respectively. No patient developed dysplasia/cancer within 10 years of diagnosis. On the other hand, dysplasia was found in only 1 patient out of 90 who underwent IPAA, and only during one surveillance session. Thus, neoplasias were found substantially more frequently in the IRA group than in the IPAA group. All of the neoplasias were successfully detected in early stages (stage 0 or I) with annual surveillance colonoscopy. Although patients with colitis-associated cancer have poorer prognosis than those with sporadic cancer in stage III, the prognosis is comparable in stages I and II [31]. Therefore, we believe that our postoperative surveillance program has effectively detected neoplasia at an early stage among patients who underwent IRA. IPAA is generally recommended for patients with UC based on the risk of cancer in the remnant rectum or ileal pouch. However, these results demonstrate that IRA with vigilant surveillance can be a viable alternative for those who hope to become pregnant or to preserve anal and sexual functions.
Kariv et al. [1] reported that the cumulative incidence of pouch neoplasia after IPAA was 1.3 and 4.2 % at 10 and 20 years, respectively. Derekx et al. [2] reported 2.0 and 6.9 % at 10 and 20 years, respectively. The cumulative incidence of neoplasia in our series was 1.6 % 20 years after IPAA, lower than that in the previous studies. This may reflect the choice of surgical procedure in our institute. Stapled IPAA is sometimes performed for patients with dysplasia/cancer due to the simplicity of its surgical procedure and to preserve postoperative anal function [1, 2, 19, 20, 22, 23]; however, neoplasias have frequently been detected in the ATZ area after stapled IPAA [1, 2, 19, 20]. We have basically performed hand-sewn IPAA with mucosectomy for patients with dysplasia/cancer, which may account for the decreased development of postoperative neoplasia in our series.
In previous reports, no IRA patient developed rectal cancer within 10 years of diagnosis [9–11, 25, 26], although the risk of neoplasia transformation increased with longer follow-up [9–11]. Andersson et al. [10] reported a cumulative cancer risk of 0 % at 10 years, 2.1 % at 20 years, and 8.7 % at 25 years. Similarly, Baker et al. [11] reported 0 % at 10 years, 6 % at 20 years, and 18 % at 35 years, while da Luz Moreira reported 2 % at 10 years and 14 % at 20 years [9]. Our results are consistent with these reports and also confirm that development of neoplasia is significantly more frequent after IRA than after IPAA.
In our series, all dysplasias/cancers were successfully detected at early stages (stages 0 and I) with postoperative surveillance endoscopy and all patients survived without recurrence after additional treatment, although previous studies have reported that patients with cancer after IRA had poor prognosis [9–11, 27]. Notably, postoperative development of neoplasia in the present study was found in refractory cases. Therefore, it is important to conduct surveillance endoscopy after IRA regardless of surgical indication. In recent years, IRA has been performed for selected cases in consideration of anal function, sexual function, and fertility [7–10]. Postoperative surveillance is particularly important in such cases.
There were several limitations of this study. First, the sample size was small. Second, this was a retrospective study. Third, longer follow-up may be needed since patients with UC are young at disease onset. Therefore, further research with a larger number of patients and longer follow-up will be needed to confirm the validity of these results.
Conclusions
The present study demonstrated that the cumulative incidence of neoplasia after IPAA is minimal. Those who underwent IRA had higher risk of neoplasia development than those who underwent IPAA, although postoperative surveillance enabled us to detect dysplasia/cancer at an early stage. IRA can be the surgical procedure of choice in selected cases in which it would be of benefit to the patient, with more careful surveillance.
References
Kariv R, Remzi FH, Lian L, Bennett AE, Kiran RP, Kariv Y, et al. Preoperative colorectal neoplasia increases risk for pouch neoplasia in patients with restorative proctocolectomy. Gastroenterology. 2010;139(3):806–12. doi:10.1053/j.gastro.2010.05.085. 812.e801-802.
Derikx LA, Kievit W, Drenth JP, de Jong DJ, Ponsioen CY, Oldenburg B, et al. Prior colorectal neoplasia is associated with increased risk of ileoanal pouch neoplasia in patients with inflammatory bowel disease. Gastroenterology. 2014;146(1):119–28. doi:10.1053/j.gastro.2013.09.047. e111.
Hata K, Watanabe T, Kazama S, Suzuki K, Shinozaki M, Yokoyama T, et al. Earlier surveillance colonoscopy programme improves survival in patients with ulcerative colitis associated colorectal cancer: results of a 23-year surveillance programme in the Japanese population. Br J Cancer. 2003;89(7):1232–6. doi:10.1038/sj.bjc.6601247.
Mowat C, Cole A, Windsor A, Ahmad T, Arnott I, Driscoll R, et al. Guidelines for the management of inflammatory bowel disease in adults. Gut. 2011;60(5):571–607. doi:10.1136/gut.2010.224154.
Aylett SO. Conservative surgery in the treatment of ulcerative colitis. Br Med J. 1953;2(4850):1348–51.
Parks AG, Nicholls RJ. Proctocolectomy without ileostomy for ulcerative colitis. Br Med J. 1978;2(6130):85–8.
Myrelid P, Oresland T. A reappraisal of the ileo-rectal anastomosis in ulcerative colitis. J Crohns Colitis. 2015;9(6):433–8. doi:10.1093/ecco-jcc/jjv060.
Scoglio D, Ahmed Ali U, Fichera A. Surgical treatment of ulcerative colitis: ileorectal vs ileal pouch-anal anastomosis. World J gastroenterol. 2014;20(37):13211–8. doi:10.3748/wjg.v20.i37.13211.
da Luz MA, Kiran RP, Lavery I. Clinical outcomes of ileorectal anastomosis for ulcerative colitis. Br J Surg. 2010;97(1):65–9. doi:10.1002/bjs.6809.
Andersson P, Norblad R, Soderholm JD, Myrelid P. Ileorectal anastomosis in comparison with ileal pouch anal anastomosis in reconstructive surgery for ulcerative colitis—a single institution experience. J Crohns Colitis. 2014;8(7):582–9. doi:10.1016/j.crohns.2013.11.014.
Baker WN, Glass RE, Ritchie JK, Aylett SO. Cancer of the rectum following colectomy and ileorectal anastomosis for ulcerative colitis. Br J Surg. 1978;65(12):862–8.
Branco BC, Sachar DB, Heimann TM, Sarpel U, Harpaz N, Greenstein AJ. Adenocarcinoma following ileal pouch-anal anastomosis for ulcerative colitis: review of 26 cases. Inflamm Bowel Dis. 2009;15(2):295–9. doi:10.1002/ibd.20609.
Remzi FH, Fazio VW, Delaney CP, Preen M, Ormsby A, Bast J, et al. Dysplasia of the anal transitional zone after ileal pouch-anal anastomosis: results of prospective evaluation after a minimum of ten years. Dis Colon Rectum. 2003;46(1):6–13. doi:10.1097/01.dcr.0000044727.08281.49.
Ziv Y, Fazio VW, Sirimarco MT, Lavery IC, Goldblum JR, Petras RE. Incidence, risk factors, and treatment of dysplasia in the anal transitional zone after ileal pouch-anal anastomosis. Dis Colon Rectum. 1994;37(12):1281–5.
Kayaalp C, Nessar G, Akoglu M, Atalay F. Elimination of mucosectomy during restorative proctocolectomy in patients with ulcerative colitis may provide better results in low-volume centers. Am J Surg. 2003;185(3):268–72.
Vento P, Lepisto A, Karkkainen P, Ristimaki A, Haglund C, Jarvinen HJ. Risk of cancer in patients with chronic pouchitis after restorative proctocolectomy for ulcerative colitis. Colorectal Dis. 2011;13(1):58–66. doi:10.1111/j.1463-1318.2009.02058.x.
Alessandroni L, Kohn A, Capaldi M, Guadagni I, Scotti A, Tersigni R. Adenocarcinoma below stapled ileoanal anastomosis after restorative proctocolectomy for ulcerative colitis. Updat Surg. 2012;64(2):149–52. doi:10.1007/s13304-011-0089-0.
O’Riordan JM, Kirsch R, Mohseni M, McLeod RS, Cohen Z. Long-term risk of adenocarcinoma post-ileal pouch-anal anastomosis for ulcerative colitis: report of two cases and review of the literature. Int J Color Dis. 2012;27(3):405–10. doi:10.1007/s00384-011-1243-3.
Block M, Borjesson L, Willen R, Bengtson J, Lindholm E, Brevinge H, et al. Neoplasia in the colorectal specimens of patients with ulcerative colitis and ileal pouch-anal anastomosis—need for routine surveillance? Scand J Gastroenterol. 2015;50(5):528–35. doi:10.3109/00365521.2015.1004364.
Kuiper T, Vlug MS, van den Broek FJ, Tytgat KM, van Eeden S, Fockens P, et al. The prevalence of dysplasia in the ileoanal pouch following restorative proctocolectomy for ulcerative colitis with associated dysplasia. Colorectal Dis. 2012;14(4):469–73. doi:10.1111/j.1463-1318.2011.02669.x.
Sagayama K, Ikeuchi H, Nishigami T, Nakano H, Uchino M, Nakamura M, et al. Incidence of and risk factors for dysplasia in mucosectomy area in ulcerative colitis patients undergoing restorative proctocolectomy. Int J Color Dis. 2007;22(4):439–43. doi:10.1007/s00384-006-0178-6.
Loffler T, Rossion I, Bruckner T, Diener MK, Koch M, von Frankenberg M, et al. HAnd Suture Versus STApling for Closure of Loop Ileostomy (HASTA Trial): results of a multicenter randomized trial (DRKS00000040). Ann Surg. 2012;256(5):828–35. doi:10.1097/SLA.0b013e318272df97. discussion 835-826.
Al-Sukhni W, McLeod RS, MacRae H, O’Connor B, Huang H, Cohen Z. Oncologic outcome in patients with ulcerative colitis associated with dyplasia or cancer who underwent stapled or handsewn ileal pouch-anal anastomosis. Dis Colon Rectum. 2010;53(11):1495–500. doi:10.1007/DCR.0b013e3181f222d5.
Hata K, Kazama S, Nozawa H, Kawai K, Kiyomatsu T, Tanaka J, et al. Laparoscopic surgery for ulcerative colitis: a review of the literature. Surg Today. 2014. doi:10.1007/s00595-014-1053-7.
Mann CV. Total colectomy and ileorectal anastomosis for ulcerative colitis. World J Surg. 1988;12(2):155–9.
Pastore RL, Wolff BG, Hodge D. Total abdominal colectomy and ileorectal anastomosis for inflammatory bowel disease. Dis Colon Rectum. 1997;40(12):1455–64.
Johnson WR, McDermott FT, Hughes ES, Pihl EA, Milne BJ, Price AB. The risk of rectal carcinoma following colectomy in ulcerative colitis. Dis Colon Rectum. 1983;26(1):44–6.
Shuno Y, Hata K, Sunami E, Shinozaki M, Kawai K, Kojima T, et al. Is surveillance endoscopy necessary after colectomy in ulcerative colitis? ISRN gastroenterology. 2011;2011:509251. doi:10.5402/2011/509251.
Hata K, Ishihara S, Watanabe T. Successful surveillance colonoscopy for patients with ulcerative colitis after ileorectal anastomosis. J Crohns Colitis. 2015. doi:10.1093/ecco-jcc/jjv124.
Riddell RH, Goldman H, Ransohoff DF, Appelman HD, Fenoglio CM, Haggitt RC, et al. Dysplasia in inflammatory bowel disease: standardized classification with provisional clinical applications. Hum Pathol. 1983;14(11):931–68.
Watanabe T, Konishi T, Kishimoto J, Kotake K, Muto T, Sugihara K, et al. Ulcerative colitis-associated colorectal cancer shows a poorer survival than sporadic colorectal cancer: a nationwide Japanese study. Inflamm Bowel Dis. 2011;17(3):802–8. doi:10.1002/ibd.21365.
Funding
This work was supported in part by the Health and Labour Sciences Research Grants for research on intractable diseases from the Ministry of Health, Labour and Welfare of Japan.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
KH conceived the design of the study. HI collected and analyzed the data and drafted the manuscript. KH, SI, and TW participated in the critical revision of the manuscript and study supervision. KH, JK, HA, KO, KY, TN, TT, JT, TK, KK, HN, SK, HY, SI, ES, and JK collected the patients’ data. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Ishii, H., Hata, K., Kishikawa, J. et al. Incidence of neoplasias and effectiveness of postoperative surveillance endoscopy for patients with ulcerative colitis: comparison of ileorectal anastomosis and ileal pouch-anal anastomosis. World J Surg Onc 14, 75 (2016). https://doi.org/10.1186/s12957-016-0833-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12957-016-0833-5