
Abstract
Background
Uric acid (UA), a liver-derived metabolite, is intimately tied to metabolic disorders. Although ample research underscores its connection with hypertriglyceridemia (HTG), studies focusing on adolescents remain limited. To fill the gaps in epidemiology,this study focused on analyzing the relationship between the levels of uric acid and HTG in a demographic sample comprising adolescents from the United States.
Methods
In this study, a total of 4,435 participants through the National Health and Nutrition Examination Survey (NHANES) from 2011 to 2020. The exposure variable was serum uric acid (SUA), the effect variable was HTG, and the covariates included demographic, questionnaire, physical examination and laboratory indicators. We utilized weighted logistic regression and meticulous subgroup evaluations to discern the intrinsic link between SUA and HTG. Stratified analyses augmented the validation of this association, while smooth curve fitting probed for potential nonlinear correlations.
Results
The study included 4,435 participants. Male adolescents exhibit elevated SUA levels. After adjusting for all variables, the weighted multiple logistic regression model revealed that SUA was positively correlated with HTG risk (OR = 1.006, 95% CI: 1.005–1.007). This relationship was consistent across the three tertiles group of SUA (T1: OR = 1.006 [95% CI: 1.005–1.007]; T2: OR = 1.006 [95% CI: 1.005–1.007]; T3: OR = 1.004 [95% CI: 1.003–1.006]; P for trend < 0.001). Stratified analyses confirmed that the positive correlation between SUA and HTG risk was significant, irrespective of sex, age or race.
Conclusions
In American children and adolescents aged 12 to 18 years, there was a pronounced association between SUA and HTG. SUA could serve as a risk indicator for HTG. It is recommended that children diagnosed with HTG should be regularly tested for SUA levels. In addition, it is recommended that SUA be included in the comprehensive care of children diagnosed with HTG.
Similar content being viewed by others

Introduction
Within the United States (US), the prevalence of hypertriglyceridemia (HTG) is 10.7% among youths aged 12 to 19 years [1]. Pediatric dyslipidemia can increase susceptibility to cardiovascular afflictions later in life—a predominant mortality factor in the nation [2]. Furthermore, HTG not only heightens cardiovascular threats but also exhibits a profound correlation with obesity, diabetes, and nonalcoholic steatohepatitis [3,4,5]. Consequently, vigilant surveillance of lipidemia in young people, discerning dyslipidemia precursors, and preemptively mitigating the inception and advancement of HTG has become paramount.
Serum uric acid (SUA), an end-product of purine catabolism, is linked to noncommunicable ailments, including hypertension, coronary arteriopathy, and metabolic syndrome [6,7,8]. Concurrently, augmented SUA concentrations resonate with an escalated peril of both holistic and cardiovascular demise [9, 10]. In a study of Chinese children and adolescents, SUA levels increased significantly between the ages of 11 and 15 years, with an estimated prevalence of hyperuricemia in children reaching 23.3% [11]. As a pro-oxidant, SUA contributes to pathological responses in humans by amplifying the oxidative stress response, which is typically viewed as one of the primary mechanisms underlying metabolic and cardiovascular diseases [4].
A growing number of studies have shown a correlation between SUA and HTG. Related research has shown that high levels of UA induce mitochondrial oxidative stress and promote the progression of HTG and metabolic syndrome [12, 13]. Other studies have shown that the apolipoprotein e (ApoE) allele is associated with increased SUA levels [14]. SUA affects residue receptors and reduces the level of very low-density lipoprotein (VLDL) in the liver, eventually leading to elevated triglyceride levels [15]. An increasing number of studies have shown that UA can be considered a risk factor for HTG, and it is suggested that monitoring and controlling SUA levels can prevent and treat HTG and its complications [16,17,18]. In a clinical study of the effect of uric acid-lowering therapy on HTG in patients with gout, serum triglycerides were reduced with the use of uric acid-lowering agents such as febuxostat and benzbromarone [16]. A longitudinal population-based epidemiologic study revealed that SUA predicts the occurrence of HTG in a positive and dose-dependent manner. Mechanistically, high UA may inhibit enzymes that catalyze the breakdown of triglycerides and reduce the breakdown of serum triglycerides, leading to a greater incidence of HTG in people with high UA than in healthy people [19]. A number of previous studies have shown that there is a correlation between SUA and various components of metabolic syndrome in children, among which triglycerides and high-density lipoprotein have shown a more significant correlation with UA [20,21,22].
However, the association between SUA and HTG remains ambiguous, particularly in children and adolescents. Consequently, data from the National Health and Nutrition Examination Survey (NHANES) database (2011–2020) were utilized in a cross-sectional study to provide epidemiological evidence.
Methods
Data sources
The data were obtained from the NHANES repository. The National Health Survey (NHANES), a biannual national cross-sectional survey, aims to collect insights into the health and nutritional landscape of American households. The interview segment encompasses demographic, socioeconomic, and dietary nutrition inquiries. The laboratory test segment comprises various examinations [23]. The study protocols were all approved by the ethical review board of the National Center for Health Statistics, and written consent was obtained from all participants before data collection. Relevant published study data are available at https://www.cdc.gov/nchs/nhanes/. This study rigorously adhered to the Strengthening Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies [24].
Study population
The analysis utilized data from four NHANES cycles spanning the years 2011 to 2020. The dataset consisted of a total of 45,462 observations, encompassing 11,364 adolescents aged between 12 and 18 years who underwent screening. The subsequent exclusion of 6,929 children and adolescents with incomplete data on serum triglyceride and SUA levels resulted in a final sample size of 4,435 participants (Fig. 1).

Flowchart of the sample selection for this study
Definition of HTG
This cross-sectional investigation focused on HTG as the principal outcome. HTG was defined as a serum triglyceride level greater than 150 mg/dL (> 17 mmol/L) [25, 26]. The Collaborative Studies Clinical Laboratory at the University of Minnesota Medical Center gauged these levels utilizing the Roche/Hitachi Modular P Chemistry Analyzer. Further pertinent standards are available at http://cdc.gov/nchs/nhanes.
Measurement of SUA
This cross-sectional investigation focused on SUA as the main dependent variable. SUA was determined by the production of colored products from the oxidation of UA through the action of 4-aminophenazone (fluorescence method). The results are reported with one decimal place. Low reported results (< 0.2 mg/dL) were reported. Details are provided on the NHANES website: http://cdc.gov/nchs/nhanes.
Other covariates
Based on prior research concerning factors correlated with HTG in the youthful demographic and cognizant of the pronounced disparities in individual ramifications from potential confounders [27,28,29,30], we incorporated the following variables for comprehensive adjustment: continuous variables: Albumin (g/dL), Alanine Aminotransferase (ALT, u/L), Aspartate Aminotransferase (AST, u/L), Alkaline phosphatase (ALP, U/L), Creatinine (umol/L), Gamma glutamyl transferase (GGT, U/L), Glucose (mmol/L), Lactate dehydrogenase (LDH, U/L), Total protein (g/dL), systolic blood pressure (SBP, mmHg), diastolic blood pressure (DBP mmHg), and dietary data [Total saturated fatty acids (g), Total monounsaturated fatty acids (g) and Total polyunsaturated fatty acids (g)] and categorical variables: sex (male, female) and race (non-Hispanic white, non-Hispanic Black, Mexican American and other).
Statistical analysis
The NHANES weights were incorporated into all calculations to more accurately capture the comprehensive nuances of the data. The purpose of applying weights is to adjust the coefficients of each independent variable in order to reflect the varying degrees of influence that different independent variables have on the dependent variable, thereby enabling research findings to better represent the overall population of the United States [23, 31]. The analytical process was conducted in four stages. Initially, SUA concentrations were divided into three groups based on tertile distinctions. Chi-square assessments were employed for categorical distinctions, while weighted t-tests were used for continuous variables. Subsequently, a weighted multifactorial logistic regression analysis elucidated the discrete correlation between SUA and HTG, controlling for various variables. The initial modulation accounted for sex, age, and ethnicity, while the subsequent one incorporated all covariates. The advantage of utilizing a multivariate logistic regression model lies in its ability to consider the influence of multiple factors on the outcome, thereby yielding more precise prediction results. Moreover, such analytical frameworks are instrumental in assessing the impact of various factors on outcomes, thereby enhancing our comprehension of the dataset. In the third step, a stratified analysis scrutinized the influence of disparate subgroups on the outcomes. In addition, the linear relationship between SUA and HTG was elucidated by smooth curve fitting. The significance threshold was set at P < 0.001. All analysis was performed using R software, version 3.4.3, and EmpowerStats Software (www. empowerstats.com).
Results
Baseline characteristics of the participants
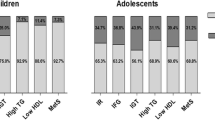
Participants were categorized into three distinct groups based on their SUA tertile rankings. Table 1 provides a comprehensive overview of the fundamental characteristics of the entire cohort consisting of 4,435 subjects, organized according to these SUA tertiles. The characteristics exhibited significant variations across SUA tertiles. In comparison to other participants, males constituted the majority (79.9%) in the highest SUA tertile. There were notable disparities observed between SUA tertiles and ALT, AST, creatinine, GGT, LDH, total protein levels, blood pressure readings, and dietary TMFA intake (P < 0.001).
Associations between SUA levels and HTG
The outcomes of the multifactorial regression assessment are presented in Table 2. Model 1 demonstrates a significant positive association between SUA and the onset of HTG, without considering other factors (OR = 1.006, 95% CI: 1.005–1.007, P < 0.001). The adjusted Model 2, accounting for age, gender, and race, revealed a statistically significant positive association (OR = 1.006, 95% CI: 1.005–1.007, P < 0.001). Moreover, even after comprehensive adjustment for all covariates in Model 3, the levels of SUA still demonstrated a positive correlation with HTG (OR = 1.004, 95% CI: 1.003–1.006, P < 0.001). The relationship between SUA and HTG was comprehensively examined by dividing SUA into tertiles. In the fully adjusted model 3, when comparing the highest tertile (T3) with the lowest tertile (T1), an odds ratio (OR) of 1.941 (95% CI: 1.461–2.579) was obtained, indicating a consistent positive correlation between elevated levels of SUA and HTG. Their interrelation underwent scrutiny via a generalized additive framework and polished curve adaptation (penal spline methodology), yielding congruent revelations (Fig. 2).

The correlation between serum uric acid and hypertriglyceridemia. (Red lines indicate smooth fit curves between variables. The blue lines indicate the 95% confidence intervals of the fits. Age, sex, race, glucose, albumin, ALT, AST, LDH, ALP, total protein, GGT, creatinine, SBP, DBP, TMFA, TPFA and TSFA were adjusted
Subgroup analyses
Further analysis within subgroups, delineated by factors such as age, sex, and ethnicity, consistently revealed a significant correlation between SUA concentrations and the incidence of HTG, as evidenced in Table 3. In addition, the nonlinear association between the two parameters was assessed through smooth curve fitting, which yielded consistent outcomes (Figs. 3, 4, and 5). In addition, from the smooth curve fitting plot, we hypothesize that the risk of HTG is lowest in Non-Hispanic Black and highest in Non-Hispanic White at the same SUA level.

The correlation between serum uric acid and hypertriglyceridemia stratified by age

The correlation between serum uric acid and hypertriglyceridemia stratified by sex

The correlation between serum uric acid and hypertriglyceridemia stratified by race
Discussion
In this study, a higher concentration of SUA was found to be positively associated with an increased prevalence of HTG among adolescents. Subgroup analysis further demonstrated a consistent association between the incidence of HTG in both children and adolescents.
The findings of this study indicated a higher prevalence of elevated levels of UA in men compared to women, which is consistent with previous research [32, 33]. It has been suggested that this disparity may be attributed to the excretory effects of estrogen on UA in the kidneys and the reabsorption effects of androgens on UA in the renal tubules [34, 35]. Additionally, adolescent males are more prone to adopting unhealthy lifestyles and behavioral habits during adolescence, such as smoking, alcohol consumption, and high-fat diets; all of which are potential risk factors for increased serum uric acid levels [36].
To date, numerous studies have investigated the association between SUA and HTG, yet limited attention has been given to the adolescent and pediatric population. A meta-analysis conducted by Goli P et al. demonstrated a robust correlation between SUA concentration and key components of metabolic syndrome in children, including HTG [37]. Consistent with these findings, a previous study in a Chinese community revealed an escalating prevalence of HTG with increasing basal levels of SUA [38]. Civantos Modino S [39] reported that overweight and obese children exhibited elevated average SUA levels, which significantly increased their likelihood of developing metabolic syndrome. Notably, SUA serves as a superior marker for predicting fatty liver risk in adolescents compared to metabolic syndrome itself [40]. In a retrospective analysis of 4,922 children diagnosed with adenoid or tonsil hypertrophy, a one standard deviation increase in serum uric acid (SUA) was associated with a 27% increased risk of dyslipidemia, with an OR of 1.270 and a 95% CI ranging from 1.185 to 1.361. Correspondingly, the incidence of hypertriglyceridemia (HTG) increased, indicating a significant positive correlation between SUA and HTG [41]. Furthermore, a cross-sectional study investigating the relationship between HTG and SUA in adults revealed a positive correlation in the U.S. adult cohort [42], with the association being more pronounced in individuals younger than 60 years, suggesting that the impact of SUA on health is more significant in younger individuals [43].
However, there is no definitive conclusion regarding the mechanism of SUA and HTG. Studies have shown that high UA is closely related to metabolic syndrome, a view further confirmed in the adolescent population [44]. The potential mechanism of action between the two includes the excessive production of reactive oxygen species by UA through the enzymatic action of xanthine oxidase, which causes endothelial dysfunction [45]. Concurrently, when soluble UA impairs nitric oxide production in endothelial cells, it also induces endothelial dysfunction [46]. These findings were confirmed in a population of obese prepubertal children [47]. Previous studies have confirmed that UA enters cells through organic ionophores and induces strong oxidation [48]. This significantly increases the burden of liver metabolism and fat accumulation. As mentioned earlier, oxidative stress responses within the vast majority of cells activate sterol regulatory element-binding proteins, resulting in the production of various lipogenic enzymes [49]. All these lipases promote the production of fat, especially in liver cells, which greatly increases the risk of nonalcoholic fatty liver disease [50]. Moreover, UA induces protein kinase B phosphorylation by mediating mitochondrial oxidative stress, affecting endothelial function [51, 52]. In an animal experiment, UA was observed to upregulate the expression of miR-149-5p and regulate the miR-149-5p/FGF21 axis, resulting in triglyceride accumulation in the liver [53]. Meng et al. [54] first proposed that the CXCL-13 pathway is a key factor that is affected by hyperuricemia and disrupts lipid metabolic processes in vivo and in vitro. Moreover, prevailing conjectures posit that augmented SUA concentrations could attenuate lipase efficacy, thus curbing the catabolism of triglycerides [55]. Contemporary research delineates a salient affirmative association between SUA and triglyceride-abundant lipoprotein cholesterol (TRL-C). This association might be mediated by bridging effects, such as the high expression of angiopoietin-like protein 4 (ANGPTL4) in subcutaneous adipose tissue and the inhibition of lipoprotein lipase activity [56]. These findings indicate that UA, which plays a direct or indirect role in cellular oxidative stress, is implicated in lipid metabolism disorders.
Study strengths and limitations
A significant advantage of this investigation lies in its expansive sample size, comprising 4,435 participants. This extensive collection of data bolsters the study's capacity to delineate a precise correlation between SUA concentrations and the incidence of HTG among children and adolescents. By encompassing a broad demographic, this research provides robust evidence that underscores the relationship between SUA levels and HTG, offering a clearer understanding of metabolic health in the younger population. Second, based on clinical experience and prior data, relevant covariates were chosen to mitigate study bias. Finally, the data are sourced from the NHANES database, which can better represent the population characteristics of the native US after quoting sampling weights.
However, some limitations exist. For example, the included data represent only the U.S. population. Therefore, caution should be exercised when extrapolating findings to other countries or races. Furthermore, the study results may be influenced by unmeasured variables. Additionally, it is important to note that the cross-sectional design of this study limits our ability to establish a causal relationship between UA and hyperlipidemia. These findings suggest that future research should focus on elucidating the underlying mechanisms linking SUA and HTG in order to validate our conclusions.
Conclusions
In conclusion, this investigation has revealed a compelling correlation between SUA concentrations and HTG, indicating that elevated SUA levels contribute to the development of HTG in American youth. Importantly, these findings underscore the significance of effectively managing and controlling SUA levels in children and adolescents with HTG to prevent disease progression. Future research should further explore the underlying mechanisms of this association and validate our assertions.
Availability of data and materials
The datasets presented in this study can be found in the following online repositories: https://www.cdc.gov/nchs/nhanes/.
References
Stewart J, McCallin T, Martinez J, Chacko S, Yusuf S. Hyperlipidemia. Pediatr Rev. 2020;41(8):393–402. https://doi.org/10.1542/pir.2019-0053.
Simental-Mendía LE, Rodríguez-Morán M, Aradillas-García C, Guerrero-Romero F. Hypertriglyceridemia is associated with impaired fasting glucose in normal-weight children. Pediatr Res. 2018;84(3):352–5. https://doi.org/10.1038/s41390-018-0027-7.
Hou X, Guan Y, Tang Y, Song A, Zhao J, Ren L, et al. A correlation study of the relationships between nonalcoholic fatty liver disease and serum triglyceride concentration after an oral fat tolerance test. Lipids Health Dis. 2021;20(1):54. https://doi.org/10.1186/s12944-021-01483-z.
Ndrepepa G. Uric acid and cardiovascular disease. Int J Clin Chem. 2018;484:150–63. https://doi.org/10.1016/j.cca.2018.05.046.
Parhofer KG, Laufs U. The Diagnosis and Treatment of Hypertriglyceridemia. Deutsches Arzteblatt international. 2019;116(49):825–32. https://doi.org/10.3238/arztebl.2019.0825.
Khichar S, Choudhary S, Singh VB, Tater P, Arvinda RV, Ujjawal V. Serum uric acid level as a determinant of the metabolic syndrome: A case control study. Diabetes & metabolic syndrome. 2017;11(1):19–23. https://doi.org/10.1016/j.dsx.2016.06.021.
Kubota M. Hyperuricemia in Children and Adolescents: Present Knowledge and Future Directions. Journal of nutrition and metabolism. 2019;2019:3480718. https://doi.org/10.1155/2019/3480718.
Wei F, Sun N, Cai C, Feng S, Tian J, Shi W, et al. Associations between serum uric acid and the incidence of hypertension: a Chinese senior dynamic cohort study. J Transl Med. 2016;14(1):110. https://doi.org/10.1186/s12967-016-0866-0.
Li B, Chen L, Hu X, Tan T, Yang J, Bao W, et al. Association of Serum Uric Acid With All-Cause and Cardiovascular Mortality in Diabetes. Diabetes Care. 2023;46(2):425–33. https://doi.org/10.2337/dc22-1339.
Zhang S, Wang Y, Cheng J, Huangfu N, Zhao R, Xu Z, et al. Hyperuricemia and Cardiovascular Disease. Curr Pharm Des. 2019;25(6):700–9. https://doi.org/10.2174/1381612825666190408122557.
Rao J, Ye P, Lu J, Chen B, Li N, Zhang H, et al. Prevalence and related factors of hyperuricaemia in Chinese children and adolescents: a pooled analysis of 11 population-based studies. Ann Med. 2022;54(1):1608–15. https://doi.org/10.1080/07853890.2022.2083670.
Copur S, Demiray A, Kanbay M. Uric acid in metabolic syndrome: Does uric acid have a definitive role? Eur J Intern Med. 2022;103:4–12. https://doi.org/10.1016/j.ejim.2022.04.022.
Yang Y, Zhou Y, Cheng S, Sun JL, Yao H, Ma L. Effect of uric acid on mitochondrial function and oxidative stress in hepatocytes. Genet Mol Res. 2016;15(2):10.4238/gmr.15028644. Published 2016 Jun 24. https://doi.org/10.4238/gmr.15028644.
Wang C, Yan W, Wang H, Zhu J, Chen H. APOE polymorphism is associated with blood lipid and serum uric acid metabolism in hypertension or coronary heart disease in a Chinese population. Pharmacogenomics. 2019;20(14):1021–31. https://doi.org/10.2217/pgs-2019-0048.
Marais AD. Apolipoprotein E and Atherosclerosis. Curr Atheroscler Rep. 2021;23(7):34. https://doi.org/10.1007/s11883-021-00933-4.
Wu J, Zhang YP, Qu Y, Jie LG, Deng JX, Yu QH. Efficacy of uric acid-lowering therapy on hypercholesterolemia and hypertriglyceridemia in gouty patients. Int J Rheum Dis. 2019;22(8):1445–51. https://doi.org/10.1111/1756-185X.13652. Epub 2019 Jul 17 PMID: 31317680.
Hou YL, Yang XL, Wang CX, Zhi LX, Yang MJ, You CG. Hypertriglyceridemia and hyperuricemia: a retrospective study of urban residents. Lipids Health Dis. 2019;18(1):81. https://doi.org/10.1186/s12944-019-1031-6.PMID:30935401;PMCID:PMC6444567.
Gonçalves JP, Oliveira A, Severo M, Santos AC, Lopes C. Cross-sectional and longitudinal associations between serum uric acid and metabolic syndrome. Endocrine. 2012;41(3):450–7. https://doi.org/10.1007/s12020-012-9629-8. Epub 2012 Feb 21 PMID: 22350659.
Zheng R, Ren P, Chen Q, Yang T, Chen C, Mao Y. Serum Uric Acid Levels and Risk of Incident Hypertriglyceridemia: A Longitudinal Population-based Epidemiological Study. Ann Clin Lab Sci. 2017;47(5):586–91.
Ságodi L, Fehér V, Kiss-Tóth E, et al. Metabolic complications of obesity during adolescence, particularly regarding elevated uric acid levels. Orv Hetil. 2015;156(22):888–95. https://doi.org/10.1556/650.2015.30140.
Ishiro M, Takaya R, Mori Y, et al. Association of uric acid with obesity and endothelial dysfunction in children and early adolescents. Ann Nutr Metab. 2013;62(2):169–76. https://doi.org/10.1159/000346227.
Koborová I, Gurecká R, Hlavatá A, et al. Association between asymptomatic hyperuricaemia and metabolic syndrome in the adolescents. Vnitr Lek. 2015;61:42–9.
Chen TC, Clark J, Riddles MK, Mohadjer LK, Fakhouri THI. National Health and Nutrition Examination Survey Sample Design and Estimation Procedures. Vital and health statistics Series 2. Data Eval Methods Res. 2020;184:1–35.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. International journal of surgery (London, England). 2014;12(12):1495–9. https://doi.org/10.1016/j.ijsu.2014.07.013.
Hypertriglyceridemia CA. Endocrinol Metab Clin North Am. 2022;51(3):539–55. https://doi.org/10.1016/j.ecl.2022.02.010.
Christian JB, Juneja MX, Meadowcroft AM, Borden S, Lowe KA. Prevalence, characteristics, and risk factors of elevated triglyceride levels in US children. Clin Pediatr. 2011;50(12):1103–9. https://doi.org/10.1177/0009922811414286.
Shi Y, Hu H, Wu Z, Wu J, Chen Z, Cheng X, et al. Associations between dietary copper intake and hypertriglyceridemia among children and adolescents in the US. Nutr Metab Cardiovasc Dis. 2023;33(4):809–16. https://doi.org/10.1016/j.numecd.2023.01.020.
Talbot D, Massamba VK. A descriptive review of variable selection methods in four epidemiologic journals: there is still room for improvement. Eur J Epidemiol. 2019;34(8):725–30. https://doi.org/10.1007/s10654-019-00529-y.
Duan H, Zhang R, Chen X, Yu G, Song C, Jiang Y, et al. Associations ofuric acid with liver steatosis and fibrosis applying vibration controlled transient elastography in the united states: a nationwide cross-section study. Front Endocrinol (Lausanne). 2022;13: 930224. https://doi.org/10.3389/fendo.2022.930224.
Duan H, Zhang R, Chen X, Yu G, Song C, Jiang Y, et al. Associations ofuric acid with liver steatosis and fibrosis applying vibration controlled transient elastography in the united states: a nationwide cross-section study. Front Endocrinol (Lausanne). 2022;13: 930224. https://doi.org/10.3389/fendo.2022.930224.
Chen TC, Parker JD, Clark J, Shin HC, Rammon JR, Burt VL. National Health and Nutrition Examination Survey: Estimation Procedures, 2011–2014. Vital and health statistics Series 2. Data Eval Methods Research. 2018;177:1–26.
Conen D, Wietlisbach V, Bovet P, Shamlaye C, Riesen W, Paccaud F, et al. Prevalence of hyperuricemia and relation of serum uric acid with cardiovascular risk factors in a developing country. BMC Public Health. 2004;4:9. https://doi.org/10.1186/1471-2458-4-9.
Li Y, Tian L, Zheng H, Jia C. Serum uric acid and risk of incident hypercholesterolaemia and hypertriglyceridaemia in middle-aged and older Chinese: a 4-year prospective cohort study. Ann Med. 2020;52(8):479–87. https://doi.org/10.1080/07853890.2020.1795918.
Stone ML, Richardson MR, Guevara L, Rand BG, Churilla JR. Elevated Serum Uric Acid and Self-Reported Heart Failure in US Adults: 2007–2016 National Health and Nutrition Examination Survey. Cardiorenal medicine. 2019;9(6):344–53. https://doi.org/10.1159/000502438.
Tsai EC, Boyko EJ, Leonetti DL, Fujimoto WY. Low serum testosterone level as a predictor of increased visceral fat in Japanese-American men. International journal of obesity and related metabolic disorders : journal of the International Association for the Study of Obesity. 2000;24(4):485–91. https://doi.org/10.1038/sj.ijo.0801183.
Kubota M. Hyperuricemia in Children and Adolescents: Present Knowledge and Future Directions. J Nutr Metab. 2019;2(2019):3480718. https://doi.org/10.1155/2019/3480718.PMID:31192008;PMCID:PMC6525889.
Goli P, Riahi R, Daniali SS, Pourmirzaei M, Kelishadi R. Association of serum uric acid concentration with components of pediatric metabolic syndrome: A systematic review and meta-analysis. J Res Med Sci. 2020;25:43. https://doi.org/10.4103/jrms.JRMS_733_19.
Zhao LJ, Zhao D, Liu J, Wang W, Wu GX, Qin LP, et al. Association between serum uric acid and triglyceride in a Chinese community. Zhonghua nei ke za zhi. 2005;44(9):664–7.
Civantos Modino S, Guijarro de Armas MG, Monereo Mejías S, Montaño Martínez JM, Iglesias Bolaños P, Merino Viveros M, et al. Hyperuricemia and metabolic syndrome in children with overweight and obesity. Endocrinologia y nutricion : organo de la Sociedad Espanola de Endocrinologia y Nutricion. 2012;59(9):533–8. https://doi.org/10.1016/j.endonu.2012.06.010.
Di Bonito P, Valerio G, Licenziati MR, Di Sessa A, Miraglia Del Giudice E, Morandi A, et al. Uric acid versus metabolic syndrome as markers of fatty liver disease in young people with overweight/obesity. Diabetes Metab Res Rev. 2022;38(7): e3559. https://doi.org/10.1002/dmrr.3559.
Yu J, Liu X, Ji H, Zhang Y, Zhan H, Zhang Z, et al. Distribution of serum uric acid concentration and its association with lipid profiles: a single-center retrospective study in children aged 3 to 12 years with adenoid and tonsillar hypertrophy. Lipids Health Dis. 2023;22(1):48. https://doi.org/10.1186/s12944-023-01806-2.
Nagahama K, Inoue T, Kohagura K. Hyperuricemia predicts future metabolic syndrome: a 4-year follow-up study of a large screened cohort in Okinawa. Japan Hypertens Res. 2014;37(3):232–8. https://doi.org/10.1038/hr.2013.137. Epub 2013 Oct 31 PMID: 24173358.
Tan MY, Mo CY, Li F, Zhao Q. The association between serum uric acid and hypertriglyceridemia: evidence from the national health and nutrition examination survey (2007–2018). Front Endocrinol (Lausanne). 2023;18(14):1215521. https://doi.org/10.3389/fendo.2023.1215521.PMID:37534213;PMCID:PMC10392824.
Foster C, Smith L, Alemzadeh R. Excess serum uric acid is associated with metabolic syndrome in obese adolescent patients. J Diabetes Metab Disord. 2020;19(1):535–43. https://doi.org/10.1007/s40200-020-00507-2.
Soltani Z, Rasheed K, Kapusta DR, Reisin E. Potential role of uric acid in metabolic syndrome, hypertension, kidney injury, and cardiovascular diseases: is it time for reappraisal? Curr Hypertens Rep. 2013;15(3):175–81. https://doi.org/10.1007/s11906-013-0344-5.
Khosla UM, Zharikov S, Finch JL, Nakagawa T, Roncal C, Mu W, et al. Hyperuricemia induces endothelial dysfunction. Kidney Int. 2005;67(5):1739–42. https://doi.org/10.1111/j.1523-1755.2005.00273.x.
Valle M, Martos R, Cañete MD, Valle R, van Donkelaar EL, Bermudo F, et al. Association of serum uric acid levels to inflammation biomarkers and endothelial dysfunction in obese prepubertal children. Pediatr Diabetes. 2015;16(6):441–7. https://doi.org/10.1111/pedi.12199.
Yu MA, Sánchez-Lozada LG, Johnson RJ, Kang DH. Oxidative stress with an activation of the renin-angiotensin system in human vascular endothelial cells as a novel mechanism of uric acid-induced endothelial dysfunction. J Hypertens. 2010;28(6):1234–42.
Jia L, Xing J, Ding Y, Shen Y, Shi X, Ren W, et al. Hyperuricemia causes pancreatic β-cell death and dysfunction through NF-κB signaling pathway. PLoS ONE. 2013;8(10): e78284. https://doi.org/10.1371/journal.pone.0078284.
Choi YJ, Shin HS, Choi HS, Park JW, Jo I, Oh ES, et al. Uric acid induces fat accumulation via generation of endoplasmic reticulum stress and SREBP-1c activation in hepatocytes. Journal Tech Methods Pathol. 2014;94(10):1114–25. https://doi.org/10.1038/labinvest.2014.98.
Cai W, Duan XM, Liu Y, Yu J, Tang YL, Liu ZL, et al. Uric Acid Induces Endothelial Dysfunction by Activating the HMGB1/RAGE Signaling Pathway. Biomed Res Int. 2017;2017:4391920. https://doi.org/10.1155/2017/4391920.
Lanaspa MA, Sanchez-Lozada LG, Choi YJ, Cicerchi C, Kanbay M, Roncal-Jimenez CA, et al. Uric acid induces hepatic steatosis by generation of mitochondrial oxidative stress: potential role in fructose-dependent and -independent fatty liver. J Biol Chem. 2012;287(48):40732–44. https://doi.org/10.1074/jbc.M112.399899.
Chen S, Chen D, Yang H, Wang X, Wang J, Xu C. Uric acid induced hepatocytes lipid accumulation through regulation of miR-149-5p/FGF21 axis. BMC Gastroenterol. 2020;20(1):39. https://doi.org/10.1186/s12876-020-01189-z.
Meng J, Lv Q, Sui A, Xu D, Zou T, Song M, et al. Hyperuricemia induces lipid disturbances by upregulating the CXCL-13 pathway. Am J Physiol Gastrointest Liver Physiol. 2022;322(2):G256–67. https://doi.org/10.1152/ajpgi.00285.2021.
Zheng R, Ren P, Chen Q, Yang T, Chen C, Mao Y. Serum Uric Acid Levels and Risk of Incident Hypertriglyceridemia: A Longitudinal Population-based Epidemiological Study. Ann Clin Lab Sci. 2017;47(5):586–91.
Peng Y, Hu D, Luo Q, Peng D. Angiopoietin-Like Protein 4 May Be an Interplay Between Serum Uric Acid and Triglyceride-Rich Lipoprotein Cholesterol. Frontiers in cardiovascular medicine. 2022;9: 863687. https://doi.org/10.3389/fcvm.2022.863687.
Funding
This work was supported by Shandong focused on Research and Development Projects (project number: 2019GSF108157).
Author information
Authors and Affiliations
Contributions
Shang-An Si conceived the idea, researched the literature and wrote the manuscript. Meng-Qi Chen performed the visualization duties. Gui-Ju Zhang reviewed and revised the manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
The studies involving human participants were reviewed and approved by the National Center for Health Statistics (NCHS). The patients/participants provided written informed consent to participate in this study. All authors agreed to participate in the research and writing of the manuscript.
Consent for publication
All authors approved the publication of this manuscript.
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that may affect the work reported herein.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Si, SA., Chen, MQ. & Zhang, GJ. Association of serum uric acid with hypertriglyceridemia in children and adolescents: a cross-sectional study. Lipids Health Dis 23, 195 (2024). https://doi.org/10.1186/s12944-024-02182-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-024-02182-1