
Abstract
Purpose
The ratio of non-high-density lipoprotein cholesterol (non-HDL-c) to high-density lipoprotein cholesterol (HDL-c) (NHHR) is a novel comprehensive lipid index. The aim of this study was to investigate the relationship between the NHHR and the prevalence of hyperuricaemia (HUA) in the adult population of the U.S.
Methods
This cross-sectional study collected data from the National Health and Nutrition Examination Survey (NHANES) (2007–2018). HUA was defined as a serum uric acid (SUA) concentration ≥ 7 mg/dL in men and ≥ 6 mg/dL in women. Multivariate logistic regression models and the restricted cubic spline (RCS) method were applied to examine the relationship between the NHHR and the risk of developing HUA. Subgroup analyses and interaction tests were also performed.
Results
The prevalence of HUA increased with increasing NHHR values (9.01% vs. 13.38% vs. 17.31% vs. 25.79%, P < 0.001). The NHHR was independently correlated with the risk of developing HUA (OR = 1.10, 95% CI: 1.05–1.16; P < 0.001). Furthermore, the risk of developing HUA was significantly greater among individuals with the highest NHHR quartile than among those with the lowest NHHR quartile (OR = 1.94, 95% CI: 1.62–2.33; P < 0.001). This relationship was consistent across subgroups. According to the RCS analysis, an inverted U-shaped relationship existed between the NHHR and the risk of developing HUA.
Conclusions
The NHHR was closely associated with an increased risk of developing HUA. Further studies on the NHHR could be beneficial for preventing and treating HUA.
Similar content being viewed by others

Introduction
Hyperuricaemia (HUA) is a typical metabolic disorder characterized by an elevated uric acid level in the plasma that exceeds normal limits. HUA not only serves as an early stage indicator and a primary cause of gout but is also considered an important risk factor for the development of cardiovascular diseases, diabetes mellitus, and chronic kidney disease as well as increased mortality rates [1,2,3,4]. Currently, the global incidence of HUA is on the rise, imposing a significant burden worldwide [5, 6]. Despite this, its treatment continues to be less than optimal.
Non-high-density lipoprotein cholesterol (non-HDL-c) refers to all potentially atherogenic cholesterol found in various lipoprotein particles, such as low-density lipoprotein cholesterol (LDL-c), lipoprotein (a), intermediate-density lipoprotein, and remnants of very low-density lipoprotein (VLDL) [7, 8]. On the other hand, high-density lipoprotein cholesterol (HDL-c), which is composed of the smallest and densest lipoprotein particles, prevents atherosclerosis [9]. Therefore, the ratio of non-HDL-c to HDL-c (NHHR) serves as a new and comprehensive index for lipid evaluation to cover the array of lipid particles that either promote or inhibit atherosclerosis [10]. Scholarly research has revealed the superior predictive power of the NHHR over conventional lipid metrics for assessing the risk of atherosclerosis and cardiovascular disorders [11, 12]. Additionally, emerging research has revealed the possibility of using the NHHR as an independent predictive marker for conditions such as diabetes and metabolic syndrome, indicating its invaluable contribution to the assessment of metabolic anomalies [13,14,15].
Despite epidemiological evidence indicating a close correlation between dyslipidaemia marker concentrations and the risk of developing HUA, existing research does not address the potential role of the NHHR in the risk of developing HUA [16, 17]. Using data sourced from the National Health and Nutrition Examination Survey (NHANES), the aim of this study was to uncover the relationship between the NHHR and the risk of developing HUA in U.S. adults. The hypothesis of this study was that there would be a strong correlation between the NHHR and the risk of developing HUA.
Materials and methods
Study population
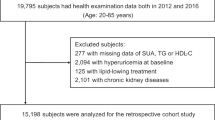
The NHANES is a comprehensive research plan using a complex probability sampling method aimed at the assessment of health and nutritional status among U.S. adult and child populations. Participants in the NHANES engage in health interviews, clinical tests, dietary assessments, and physical examinations [18]. The Ethics Review Board of the National Center for Health Statistics approved the research protocol. More detailed information can be found in the NHANES database. This research ultimately involved 30,937 eligible participants drawn from a pool of 59,842 individuals by merging the NHANES cycles spanning 2007 to 2018. All study participants were aged 20 years or older, were not pregnant, and had complete NHHR and serum uric acid (SUA) data.
Exposure and outcome definitions
In this study, the NHHR, which is the ratio of non-HDL-c to HDL-c, was used as the exposure variable. Using blood samples obtained from fasting individuals, non-HDL-c is determined by deducting HDL-c from total cholesterol (TC) [19, 20]. HUA was defined as SUA levels ≥ 7 mg/dL in men and ≥ 6 mg/dL in women [21].
Covariate definitions
The study considered various potential covariates, including age (years), gender, race, income, education, smoking status, diabetes mellitus status, hypertension status, blood pressure, body mass index (BMI, kg/m2), waist circumference (WC, cm), and biochemical markers such as glycohemoglobin (HbA1c, %), alanine aminotransferase (ALT, U/L) concentrations, aspartate aminotransferase (AST, U/L) concentrations, gamma-glutamyl transferase (GGT, U/L) concentrations, triglyceride (TG, mmol/L) concentrations, LDL-c concentrations, serum creatinine (SCr, µmol/L) concentrations, and the estimated glomerular filtration rate (eGFR, mL/min/1.73 m2). The BMI was categorized as < 25 (normal), 25-29.9 (overweight), or ≥ 30 kg/m2 (obese). The eGFR calculation was based on the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula [22]. Smoking history included both former and current smoking status. Diabetes and hypertension status were indicated by a self-reported history of either condition.
Statistical analysis
Statistical analyses in this research were conducted using Empower software (http://www.empowerstats.com) and R software (http://www.R-project.org) in compliance with the standards prescribed by the Centers for Disease Control and Prevention (CDC). This research involved the application of a complex, tiered cluster sampling method, incorporating sample weights. Continuous data are presented as the means, while categorical data are expressed as percentages. The weighted Student’s t test and chi-squared test were applied for comparisons across various groups. Logistic and linear regression models were applied to examine the associations of the levels of non-HDL-c and HDL-c and the NHHR with the risk of developing HUA, as well as between those factors and the SUA concentration. The variance inflation factor was further applied to detect multicollinearity in regression analyses. Decision curve analysis (DCA) and receiver operating characteristic (ROC) curve analysis were applied to measure the efficacy of using non-HDL-c, HDL-c, and the NHHR to determine the risk of developing HUA. Subgroup analyses were also performed. Finally, restricted cubic spline (RCS) logistic regression with four knots was applied to investigate the nonlinear associations between the NHHR and the risk of developing HUA, using the median values of the NHHR as references (OR = 1). For observed nonlinear relationships, a two-piecewise linear regression model was applied to define intervals and identify threshold effects. A P value (two-sided) < 0.05 was considered to indicate statistical significance.
Results
Baseline characteristics
A total of 30,937 participants, with an average age of 47.78 years, 48.79% of whom were male, were included in this study (Table 1). Compared with the non-HUA group, the HUA group was older and had more males, individuals with an annual income under $20,000, smokers, and individuals with hypertension and diabetes (P < 0.05). Additionally, individuals in this group exhibited increased BMI, WC, systolic blood pressure (SBP), diastolic blood pressure (DBP), HbA1c concentrations, ALT concentrations, AST concentrations, GGT concentrations, TG concentrations, TC concentrations, LDL-c concentrations, non-HDL-c concentrations, SCr concentrations, and SUA concentrations (P < 0.01). Conversely, a greater proportion of individuals with education levels above high school, as well as a reduced eGFR and HDL-c concentration, were observed (P < 0.001). Additionally, differences in race distribution were also observed (P < 0.001). The HUA group exhibited notably greater NHHR values than did the non-HUA group (P < 0.001).
Baseline characteristics based on the quantiles of the NHHR
According to the NHHR, the subjects were categorized into four groups based on quantiles (Table 2). The high-NHHR quantile group exhibited greater proportions of males, individuals with an annual income under $20,000, smokers, and individuals with diabetes and hypertension, as well as variations in racial distribution (P < 0.05). Furthermore, BMI, WC, SBP, DBP, ALT concentrations, AST concentrations, GGT concentrations, HbA1c values, TG concentrations, TC concentrations, LDL-c concentrations, non-HDL-c concentrations, and SCr concentrations were obviously increased (P < 0.001). In contrast, the proportions of individuals with high education levels, high eGFRs, and high HDL-c levels decreased (P < 0.01). Compared to those in the lowest NHHR quartile, individuals in the second and third quartiles were older, and those in the fourth quartile were younger (P < 0.05). Notably, a higher NHHR was related to increased levels of SUA and a greater prevalence of HUA (9.01% vs. 13.38% vs. 17.31% vs. 25.79%, P < 0.001).
Association between the NHHR and the risk of developing HUA
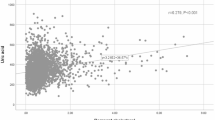
The NHHR is positively correlated with the prevalence of HUA, a statistically significant relationship that persists across unadjusted, preliminarily adjusted, and fully adjusted logistic regression models (Table 3). Upon complete adjustment, each unit increase in the NHHR was associated with a 10% increase in the risk of developing HUA (OR = 1.10, 95% CI: 1.05–1.16, P < 0.001) (Supplementary Tables 1 and 2). When the NHHR was divided into quartiles, participants in the highest quartile clearly faced a greater risk, with a 0.94-fold increase compared to those in the lowest quartile (OR = 1.94, 95% CI: 1.62–2.33, P < 0.001). Using SUA levels as the dependent variable, linear regression analysis revealed a significant correlation between the NHHR and SUA (β = 0.06, 95% CI: 0.04–0.08, P < 0.001) (Table 4). Based on the ROC curve results, the areas under the curve (AUCs) for the NHHR, non-HDL-c, and HDL-c were 61.76%, 56.68%, and 59.59%, respectively. Additionally, DCA showed that compared with non-HDL-c and HDL-c concentrations, the NHHR offers a greater net benefit (Figs. 1 and 2).

DCA results

ROC results
Subgroup analysis and threshold effect
Subgroup analyses were carried out considering factors such as age, gender, race, annual household income, education level, smoking status, BMI, diabetes status, hypertension status, and the eGFR to evaluate the reliability of this relationship between the NHHR and the risk of developing HUA across different populations (Fig. 3). The results indicated that these factors had no significant impact on the relationship (P > 0.05). Interestingly, the RCS results showed a nonlinear, inverted U-shaped relationship between the NHHR and the risk of developing HUA across the entire population (Fig. 4). Further investigation using a two-piecewise linear regression identified a breakpoint at 5.14 (Table 5). To the left of the breakpoint, a positive correlation existed between the NHHR and the risk of developing HUA, as indicated by an OR of 1.25 and a 95% CI ranging from 1.18 to 1.32. To the right of the breakpoint, the NHHR and the risk of developing HUA were inversely correlated, with an OR of 0.77 and a 95% CI of 0.68 to 0.88. There was a significant change across the breakpoint (P < 0.001).

Subgroup analyses

Results of RCS analysis
Discussion
This groundbreaking population-based study explored the connection between the NHHR and the risk of developing HUA. Compared to traditional lipid indicators, a higher NHHR is strongly associated with a greater risk of developing HUA.
Usually, LDL-c is the focus for managing dyslipidaemia [23]. However, non-HDL-c, which includes all plasma lipoproteins except for HDL-c, are recognized as a significant risk factor for cardiovascular diseases [24, 25]. Therefore, non-HDL-c has gradually become a coprimary or primary target in dyslipidaemia management [24]. Several prior studies from China have also established an independent association between the non-HDL-c concentration and the risk of developing HUA [16, 20]. Moreover, some scholars have also reported that a decrease in HDL-c levels is a key risk factor for HUA [26]. Emerging evidence suggests that lipid ratios might be valuable indicators for various diseases, including cardiovascular diseases, diabetes, and metabolic syndrome [13, 27,28,29]. The NHHR was proposed to encompass all information related to pro-atherosclerotic and anti-atherosclerotic lipid particles, representing the balance between lipoproteins [10, 30]. Studies have demonstrated that the NHHR significantly surpasses traditional lipid parameters in the assessment of atherosclerosis [11]. Similarly, in the field of metabolic disorders, past studies have shown that the NHHR has excellent predictive ability for diabetes, metabolic syndrome, and insulin resistance (IR), surpassing individual lipid indicators such as non-HDL-c, HDL-c, and LDL-c [13, 15]. Nevertheless, there has been limited research on the correlation between lipid ratios and the risk of developing HUA, making it unclear whether the NHHR can serve as a useful marker for HUA. This study revealed that compared with the individual measurements of non-HDL-c and HDL-c, the NHHR has superior diagnostic predictive value for the risk of developing HUA. Additionally, further RCS analysis indicated a nonlinear, inverse U-shaped association between the NHHR and the risk of developing HUA, consistent with previous studies on the connection between the NHHR and suicidal ideation [31]. This study extends the use of lipid ratios and fills the gaps in previous research, suggesting that the NHHR might be a promising marker for predicting HUA. Notably, cohort research has confirmed a close relationship between dyslipidaemia and the incidence of HUA [32,33,34]. Hence, from the perspective of lipid management, the prevention and treatment of HUA could offer important clinical benefits. Current research has also attempted to focus on non-HDL-c as a key point in lipid management [24]. Whether NHHR is a novel target for lipid management requires further investigation. Finally, subgroup analyses and interaction tests did not identify specific populations; however, further analysis is warranted for other groups, such as older nonwhite women.
Several plausible factors, such as IR, oxidative stress, inflammation, lifestyle, and the use of lipid-lowering medications, might contribute to revealing the association between dyslipidaemia marker concentrations and the risk of developing HUA. IR, a common factor underlying both conditions, impairs the body’s ability to use insulin efficiently, leading to disrupted lipid metabolism and increased uric acid production [35, 36]. Additionally, an imbalance between free radicals and antioxidants causes oxidative stress, resulting in lipid peroxidation and uric acid accumulation [37, 38]. Chronic inflammation, often observed in individuals with dyslipidaemia, can also stimulate uric acid synthesis and impair its excretion [39]. Researchers have also discovered that patients with hyperlipidaemia and HUA share similar dietary behaviours, such as consuming large amounts of alcohol and fatty foods [40]. Interestingly, the administration of lipid-lowering medications is associated with alterations in SUA levels [41].
Strengths and limitations of the study
This study has several strengths. It was based on data from the National Health and Nutrition Examination Survey (NHANES) database, which is nationally representative and has a relatively large sample size. This study included effective control for potential confounding factors, enhancing the reliability of the results. RCS analysis was also employed to further investigate nonlinear relationships and assess the reliability of the results across different populations through subgroup analysis.
However, there are also some limitations to the current research. First, the use of a cross-sectional design prevents us from inferring causality; therefore, prospective cohort studies and intervention trials are essential to elucidate the causality of these associations. Second, this study did not account for certain potential confounders, including the use of uric acid-lowering and lipid-lowering medications or dietary patterns marked by high consumption of alcohol and fatty foods, which could skew the results. Furthermore, as the sample comes from the US population, the applicability of the results to other populations needs additional verification.
Conclusion
In a nationally representative study conducted among adults aged ≥ 20 years, the NHHR was associated with the risk of developing HUA. Implementing lipid management to improve the NHHR could help in assessing, preventing, and treating HUA.
Data availability
The data are sourced from the NHANES database, which is a publicly accessible and free resource (https://www.cdc.gov/nchs/nhanes).
References
Ndrepepa G. Uric acid and cardiovascular disease. Clin Chim Acta. 2018;484150–163. https://doi.org/10.1016/j.cca.2018.05.046.
Zhu Y, Pandya BJ, Choi HK. Comorbidities of gout and hyperuricemia in the US general population: NHANES 2007–2008. Am J Med. 2012;125(7):679–e6871. https://doi.org/10.1016/j.amjmed.2011.09.033.
Facchini F, Chen YD, Hollenbeck CB, Reaven GM. Relationship between resistance to insulin-mediated glucose uptake, urinary uric acid clearance, and plasma uric acid concentration. JAMA. 1991;266(21):3008–11.
Crawley WT, Jungels CG, Stenmark KR, Fini MA. U-shaped association of uric acid to overall-cause mortality and its impact on clinical management of hyperuricemia. Redox Biol. 2022;51102271. https://doi.org/10.1016/j.redox.2022.102271.
Danve A, Sehra ST, Neogi T. Role of diet in hyperuricemia and gout. Best Pract Res Clin Rheumatol. 2021;35(4):101723. https://doi.org/10.1016/j.berh.2021.101723.
Dehlin M, Jacobsson L, Roddy E. Global epidemiology of gout: prevalence, incidence, treatment patterns and risk factors. Nat Rev Rheumatol. 2020;16(7):380–90. https://doi.org/10.1038/s41584-020-0441-1.
Hodkinson A, Tsimpida D, Kontopantelis E, Rutter MK, Mamas MA, Panagioti M. Comparative effectiveness of statins on non-high density lipoprotein cholesterol in people with diabetes and at risk of cardiovascular disease: systematic review and network meta-analysis. BMJ. 2022;376e067731. https://doi.org/10.1136/bmj-2021-067731.
Blaha MJ, Blumenthal RS, Brinton EA, Jacobson TA. The importance of non-HDL cholesterol reporting in lipid management. J Clin Lipidol. 2008;2(4):267–73. https://doi.org/10.1016/j.jacl.2008.06.013.
Di Bartolo BA, Cartland SP, Genner S, Manuneedhi Cholan P, Vellozzi M, Rye KA, Kavurma MM. HDL improves cholesterol and glucose homeostasis and reduces atherosclerosis in Diabetes-Associated atherosclerosis. J Diabetes Res. 2021;20216668506. https://doi.org/10.1155/2021/6668506.
Wang A, Li Y, Zhou L, Liu K, Li S, Zong C, Song B, Gao Y, Li Y, Tian C, Xing Y, Xu Y, Wang L. Non-HDL-C/HDL-C ratio is associated with carotid plaque stability in general population: a cross-sectional study. Front Neurol. 2022;13875134. https://doi.org/10.3389/fneur.2022.875134.
Zhu L, Lu Z, Zhu L, Ouyang X, Yang Y, He W, Feng Y, Yi F, Song Y. Lipoprotein ratios are better than conventional lipid parameters in predicting coronary heart disease in Chinese Han people. Kardiol Pol. 2015;73(10):931–8. https://doi.org/10.5603/KP.a2015.0086.
Kouvari M, Panagiotakos DB, Chrysohoou C, Georgousopoulou EN, Tousoulis D, Pitsavos AC. Sex-related differences of the Effect of Lipoproteins and apolipoproteins on 10-Year Cardiovascular Disease Risk; insights from the ATTICA Study (2002–2012). Molecules. 2020;25(7). https://doi.org/10.3390/molecules25071506.
Sheng G, Liu D, Kuang M, Zhong Y, Zhang S, Zou Y. Utility of Non-high-density Lipoprotein Cholesterol to high-density lipoprotein cholesterol ratio in evaluating Incident Diabetes Risk. Diabetes Metab Syndr Obes. 2022;151677–1686. https://doi.org/10.2147/dmso.S355980.
Wang D, Wang L, Wang Z, Chen S, Ni Y, Jiang D. Higher non-HDL-cholesterol to HDL-cholesterol ratio linked with increased nonalcoholic steatohepatitis. Lipids Health Dis. 2018;17(1):67. https://doi.org/10.1186/s12944-018-0720-x.
Kim SW, Jee JH, Kim HJ, Jin SM, Suh S, Bae JC, Kim SW, Chung JH, Min YK, Lee MS, Lee MK, Kim KW, Kim JH. Non-HDL-cholesterol/HDL-cholesterol is a better predictor of metabolic syndrome and insulin resistance than apolipoprotein B/apolipoprotein A1. Int J Cardiol. 2013;168(3):2678–83. https://doi.org/10.1016/j.ijcard.2013.03.027.
Fang Y, Mei W, Wang C, Ren X, Hu J, Su F, Cao L, Tavengana G, Jiang M, Wu H, Wen Y. Dyslipidemia and hyperuricemia: a cross-sectional study of residents in Wuhu, China. BMC Endocr Disord. 2024;24(1):2. https://doi.org/10.1186/s12902-023-01528-7.
Basnet TB, Du S, Feng R, Gao J, Gong J, Ye W. Fatty liver mediates the association of hyperuricemia with prediabetes and diabetes: a weighting-based mediation analysis. Front Endocrinol (Lausanne). 2023;141133515. https://doi.org/10.3389/fendo.2023.1133515.
Hoffman HJ, Rawal S, Li CM, Duffy VB. New chemosensory component in the U.S. National Health and Nutrition Examination Survey (NHANES): first-year results for measured olfactory dysfunction. Rev Endocr Metab Disord. 2016;17(2):221–40. https://doi.org/10.1007/s11154-016-9364-1.
Hu H, Fukunaga A, Yokoya T, Nakagawa T, Honda T, Yamamoto S, Okazaki H, Miyamoto T, Sasaki N, Ogasawara T, Gonmori N, Yamamoto K, Hori A, Tomita K, Nagahama S, Konishi M, Katayama N, Morioka H, Kabe I, Mizoue T, Dohi S. Non-high-density Lipoprotein Cholesterol and risk of Cardiovascular Disease: the Japan Epidemiology Collaboration on Occupational Health Study. J Atheroscler Thromb. 2022;29(9):1295–306. https://doi.org/10.5551/jat.63118.
Xu J, Peng H, Ma Q, Zhou X, Xu W, Huang L, Hu J, Zhang Y. Associations of non-high density lipoprotein cholesterol and traditional blood lipid profiles with hyperuricemia among middle-aged and elderly Chinese people: a community-based cross-sectional study. Lipids Health Dis. 2014;13117. https://doi.org/10.1186/1476-511x-13-117.
Feig DI, Kang DH, Johnson RJ. Uric acid and cardiovascular risk. N Engl J Med. 2008;359(17):1811–21. https://doi.org/10.1056/NEJMra0800885.
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, Kusek JW, Eggers P, Van Lente F, Greene T, Coresh J. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–12. https://doi.org/10.7326/0003-4819-150-9-200905050-00006.
Navarese EP, Robinson JG, Kowalewski M, Kolodziejczak M, Andreotti F, Bliden K, Tantry U, Kubica J, Raggi P, Gurbel PA. Association between Baseline LDL-C Level and Total and Cardiovascular Mortality after LDL-C lowering: a systematic review and Meta-analysis. JAMA. 2018;319(15):1566–79. https://doi.org/10.1001/jama.2018.2525.
Raja V, Aguiar C, Alsayed N, Chibber YS, ElBadawi H, Ezhov M, Hermans MP, Pandey RC, Ray KK, Tokgözoglu L, Zambon A, Berrou JP, Farnier M. Non-HDL-cholesterol in dyslipidemia: review of the state-of-the-art literature and outlook. Atherosclerosis. 2023;383117312. https://doi.org/10.1016/j.atherosclerosis.2023.117312.
Yu Y, Lan T, Wang D, Fang W, Tao Y, Li M, Huang X, Zhou W, Wang T, Zhu L, Bao H, Cheng X. The association of lipid ratios with hyperuricemia in a rural Chinese hypertensive population. Lipids Health Dis. 2021;20(1):121. https://doi.org/10.1186/s12944-021-01556-z.
Wang HP, Xu YY, Xu BL, Lu J, Xia J, Shen T, Fang J, Lei T. Correlation between abdominal Fat distribution and serum uric acid in patients recently diagnosed with type 2 diabetes. Diabetes Metab Syndr Obes. 2023;163751–3762. https://doi.org/10.2147/dmso.S430235.
Chen Y, Chang Z, Liu Y, Zhao Y, Fu J, Zhang Y, Liu Y, Fan Z. Triglyceride to high-density lipoprotein cholesterol ratio and cardiovascular events in the general population: a systematic review and meta-analysis of cohort studies. Nutr Metab Cardiovasc Dis. 2022;32(2):318–29. https://doi.org/10.1016/j.numecd.2021.11.005.
Drexel H, Larcher B, Mader A, Vonbank A, Heinzle CF, Moser B, Zanolin-Purin D, Saely CH. (2021) The LDL-C/ApoB ratio predicts major cardiovascular events in patients with established atherosclerotic cardiovascular disease. Atherosclerosis 32944-49. https://doi.org/10.1016/j.atherosclerosis.2021.05.010.
Zhang X, Zhang X, Li X, Feng J, Chen X. Association of metabolic syndrome with atherogenic index of plasma in an urban Chinese population: a 15-year prospective study. Nutr Metab Cardiovasc Dis. 2019;29(11):1214–9. https://doi.org/10.1016/j.numecd.2019.07.006.
Qi X, Wang S, Huang Q, Chen X, Qiu L, Ouyang K, Chen Y. The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and risk of depression among US adults: a cross-sectional NHANES study. J Affect Disord. 2024;344451–457. https://doi.org/10.1016/j.jad.2023.10.064.
Qing G, Deng W, Zhou Y, Zheng L, Wang Y, Wei B. The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and suicidal ideation in adults: a population-based study in the United States. Lipids Health Dis. 2024;23(1):17. https://doi.org/10.1186/s12944-024-02012-4.
Zhang Y, Zhang M, Yu X, Wei F, Chen C, Zhang K, Feng S, Wang Y, Li WD. Association of hypertension and hypertriglyceridemia on incident hyperuricemia: an 8-year prospective cohort study. J Transl Med. 2020;18(1):409. https://doi.org/10.1186/s12967-020-02590-8.
Xu Y, Dong H, Zhang B, Zhang J, Ma Q, Sun H. Association between dyslipidaemia and the risk of hyperuricaemia: a six-year longitudinal cohort study of elderly individuals in China. Ann Med. 2022;54(1):2402–10. https://doi.org/10.1080/07853890.2022.2118368.
He H, Wang S, Xu T, Liu W, Li Y, Lu G, Tu R. Sex-related differences in the hypertriglyceridemic-waist phenotype in association with hyperuricemia: a longitudinal cohort study. Lipids Health Dis. 2023;22(1):38. https://doi.org/10.1186/s12944-023-01795-2.
Vuorinen-Markkola H, Yki-Järvinen H. Hyperuricemia and insulin resistance. J Clin Endocrinol Metab. 1994;78(1):25–9. https://doi.org/10.1210/jcem.78.1.8288709.
Smith DA. Treatment of the dyslipidemia of insulin resistance. Med Clin North Am. 2007;91(6):1185–210. https://doi.org/10.1016/j.mcna.2007.06.008. x.
Rizzo M, Kotur-Stevuljevic J, Berneis K, Spinas G, Rini GB, Jelic-Ivanovic Z, Spasojevic-Kalimanovska V, Vekic J. Atherogenic dyslipidemia and oxidative stress: a new look. Transl Res. 2009;153(5):217–23. https://doi.org/10.1016/j.trsl.2009.01.008.
Gherghina ME, Peride I, Tiglis M, Neagu TP, Niculae A, Checherita IA. Uric acid and oxidative stress-relationship with Cardiovascular, metabolic, and renal impairment. Int J Mol Sci. 2022;23(6). https://doi.org/10.3390/ijms23063188.
Al Shanableh Y, Hussein YY, Saidwali AH, Al-Mohannadi M, Aljalham B, Nurulhoque H, Robelah F, Al-Mansoori A, Zughaier SM. Prevalence of asymptomatic hyperuricemia and its association with prediabetes, dyslipidemia and subclinical inflammation markers among young healthy adults in Qatar. BMC Endocr Disord. 2022;22(1):21. https://doi.org/10.1186/s12902-022-00937-4.
Conen D, Wietlisbach V, Bovet P, Shamlaye C, Riesen W, Paccaud F, Burnier M. Prevalence of hyperuricemia and relation of serum uric acid with cardiovascular risk factors in a developing country. BMC Public Health. 2004;49. https://doi.org/10.1186/1471-2458-4-9.
Deedwania PC, Stone PH, Fayyad RS, Laskey RE, Wilson DJ. Improvement in renal function and reduction in serum uric acid with intensive statin therapy in older patients: a Post Hoc Analysis of the SAGE trial. Drugs Aging. 2015;32(12):1055–65. https://doi.org/10.1007/s40266-015-0328-z.
Acknowledgements
We extend our gratitude to the participants involved in this research and the assistance offered by Jiangsu University and Xuzhou Medical University.
Funding
This study was supported by the Science and Technology Project of Changzhou Health Commission (WZ202226), the Young Talent Development Plan of Changzhou Health Commission (CZQM2022029), the Kunshan Key R & D Program (KS2201), and the Guang Ren Foundation Research Project of the Affiliated Hospital of Jiangsu University (KRY-YN2022017).
Author information
Authors and Affiliations
Contributions
Z.W. and M.W. wrote the manuscript. R.D. and F.T. prepared tables and figures. M.X. and T.G. provided critical feedback and revised the manuscript. Q.Y. supervised the entire project. The final manuscript was reviewed and approved by all the authors.
Corresponding author
Ethics declarations
Ethical approval
This study involving human participants was reviewed and approved by the Ethics Review Board of the National Center for Health Statistics.
Informed consent
Written informed consent was obtained from all participants in the study.
Competing interests
The authors acknowledge that there are no competing interests
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, Z., Wu, M., Du, R. et al. The relationship between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and hyperuricaemia. Lipids Health Dis 23, 187 (2024). https://doi.org/10.1186/s12944-024-02171-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-024-02171-4