
Abstract
Background
Malaria is one of the most severe global public health problems worldwide, particularly in Africa, where Nigeria has the greatest number of malaria cases. This community-based study was designed to investigate the prevalence and risk factors of malaria and to evaluate the knowledge, attitudes, and practices (KAP) regarding malaria among rural Hausa communities in Kano State, Nigeria.
Methods
A cross-sectional community-based study was conducted on 551 participants from five local government areas in Kano State. Blood samples were collected and examined for the presence of Plasmodium species by rapid diagnostic test (RDT), Giemsa-stained thin and thick blood films, and PCR. Moreover, demographic, socioeconomic, and environmental information as well as KAP data were collected using a pre-tested questionnaire.
Results
A total of 334 (60.6 %) participants were found positive for Plasmodium falciparum. The prevalence differed significantly by age group (p < 0.01), but not by gender or location. A multivariate analysis showed that malaria was associated significantly with being aged 12 years or older, having a low household family income, not using insecticide treated nets (ITNs), and having no toilets in the house. Overall, 95.6 % of the respondents had prior knowledge about malaria, and 79.7, 87.6 and 95.7 % of them knew about the transmission, symptoms, and prevention of malaria, respectively. The majority (93.4 %) of the respondents considered malaria a serious disease. Although 79.5 % of the respondents had at least one ITN in their household, utilization rate of ITNs was 49.5 %. Significant associations between the respondents’ knowledge concerning malaria and their age, gender, education, and household monthly income were reported.
Conclusions
Malaria is still highly prevalent among rural Hausa communities in Nigeria. Despite high levels of knowledge and attitudes in the study area, significant gaps persist in appropriate preventive practices, particularly the use of ITNs. Innovative and Integrated control measures to reduce the burden of malaria should be identified and implemented in these communities. Community mobilization and health education regarding the importance of using ITNs to prevent malaria and save lives should be considered.
Similar content being viewed by others


Background
Malaria continues to be a major public health problem in 97 countries and territories in the tropics and subtropics. Globally, approximately 214 million cases of malaria occur annually and 3.2 billion people are at risk of infection [1]. Approximately 438,000 deaths were attributed to malaria in 2015, particularly in sub-Saharan Africa, where an estimated 90 % of all malaria deaths occur [1]. As a critical target of the Millennium Development Goals, in 2005, the World Health Assembly established a goal of reducing malaria cases and deaths by 75 % between 2005 and 2015 [2]. Hence, over the past decade, there has been greatly renewed interest in research and innovations in diagnostic methods, drugs and vaccines, and the development of control measures to eradicate malaria [3]. As a result, between 2000 and 2013, the incidence rates of malaria fell by 30 % globally, and by 34 % in Africa [4].
Nigeria suffers the world’s greatest malaria burden, with approximately 51 million cases and 207,000 deaths reported annually (approximately 30 % of the total malaria burden in Africa), while 97 % of the total population (approximately 173 million) is at risk of infection [5]. Moreover, malaria accounts for 60 % of outpatient visits to hospitals and led to approximately 11 % maternal mortality and 30 % child mortality, especially among children less than 5 years [5, 6]. Malaria is caused by Plasmodium falciparum, and the mosquitoes Anopheles gambiae, Anopheles funestus, Anopheles arabiensis, and Anopheles moucheti are the major vectors that cause year-round transmission; artemether-lumefantrine (AL) or artesunate + amodiaquine (AS + AQ) is the treatment regime adopted in 2004 [1, 7]. This devastating disease affects the country’s economic productivity, resulting in an estimated monetary loss of approximately 132 billion Naira (~700 million USD), in treatment costs, prevention, and other indirect costs [8, 9].
Since 2008, the National Malaria Control Programme (NMCP) in Nigeria has adopted a specific plan, the goal of which is to reduce 50 % of the malaria burden by 2013 by achieving at least 80 % coverage of long-lasting impregnated mosquito nets (LLINs), together with other measures, such as 20 % of houses in targeted areas receiving indoor residual spraying (IRS), and treatment with two doses of intermittent preventative therapy (IPT) for 100 % of pregnant women who visit antenatal care clinics [10–12]. Because of these measures, the percentage of households with at least one LLIN increased to over 70 % by 2010, compared to only 5 % in 2008 [13–15]. Although previous studies have documented a high prevalence of malaria throughout Nigeria [16–21], there remains a paucity of research on people’s knowledge, attitudes, and practices (KAP) towards malaria in the majority of the federation, particularly in Northern Nigeria, including Kano State. This information is imperative in order to identify and implement effective control measures, and plan for the participation of the targeted communities in the control, which is one of the cardinal tools for the success and sustainability of disease control programmes [22–24]. Therefore, this study was designed to investigate the current prevalence and risk factors of malaria and to evaluate the people’s KAP regarding malaria in Kano State, North Central Nigeria.
Methods
Study design
A cross-sectional, community-based study was carried out between May and June 2013 among inhabitants aged 1–90 years in the five rural communities. Primary healthcare personnel and community leaders were involved in the study, and discussions were held with the households’ heads at the community leaders’ hall to explain the rationale and importance of the study.
Study area
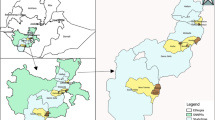
Kano State is located in the North Central part of the country between longitude 8.500°E and latitude 11.500°N; it occupies a total surface area of 20,131 km2 (77,773 m2) and has a total population of approximately 11 million. Kano State is a commercial and agricultural region known for the production of groundnuts and cotton. It is also the second largest industrial center in Nigeria, with textile, tanning, footwear, cosmetics, plastic, and other industries. The state consists primarily of Sudan savanna type vegetation, with an annual mean rainfall of 800-900 mm, a temperature that ranges between 25–40 °C (mean approximately 26 °C), and a relative humidity of 47.43 %. The climate of the study area is a tropical dry-and-wet season type typical of West African savannah. The wet season lasts from May to October, while the dry season extends from November to April [25].
The ecology of Nigeria varies from mangrove swamps and tropical rain forest belts in the coastal areas to open savannah woodland on the low plateau—which extends through much of the central part of the country—to semi-arid plains and Sahel grassland in the north and the eastern highlands. The seasonality, intensity, and duration of malaria transmission vary according to the different ecological strata [26]. The duration of malaria transmission increases from approximately 3 months in the north to year-round in the south. Moreover, the highest anthropophagic index and sporozoite positivity for the major malaria vectors was reported in the savanna forest region [27].
In collaboration with primary healthcare personnel and traditional rulers in each local government area, five districts were selected randomly from the available district list. The districts included were Kura (8.429°E, 11.774°N), Bebeji (8.400°E, 12.366°N), Gwarzo (7.932°E, 11.915°N), Shanono (7.983°E, 12.049°N), and Minjibir (8.530°E, 12.226°N).
Study population
Residents of Kano State are predominantly farmers and merchants, and the districts selected have a homogenous nature with respect to sociocultural and daily economic activities. In the selected areas, primary healthcare staff and leaders of the communities were informed about the objectives and procedures of the study in order to obtain their permission to conduct the study and established a station. Then, the community leaders asked all residents to gather at the station (community leader’s hall) where they received explanation about the objectives of the study and their involvement. All residents who agreed voluntarily to participate were included in this study (universal sampling). A total of 609 individuals volunteered to participate in this study; however, 551 (90.5 %) individuals, aged 1–90 years, met the inclusion criteria (written signed consent, completed questionnaire, and blood samples for examination).
Ethical considerations
Ethical approval for the study protocol was obtained from the Medical Ethics Committee of the University of Malaya Medical Centre, Kuala Lumpur as well as from Kano State’s Ministry of Health, Kano State Hospitals Management Board, the respective local government authorities, and the district heads of the communities. When seeking consent from the volunteers in each village, the objectives and procedures of the study were explained clearly to them in the local language, Hausa. Participants were also informed that they could withdraw from the study at any time without consequences. Thus, written and signed or thumb-printed informed consents were obtained from all adult participants and guardians/parents on behalf of their children before starting the survey; the ethics committees approved these procedures as well. All malaria-positive individuals were treated with the standard medication according to national malaria drug policy.
Questionnaire survey
A pre-tested questionnaire was administered to the participants in order to collect information on their demographic, socioeconomic, and environmental factors, and the health status, as well as their KAP towards malaria. Information was collected from the respondents via face-to-face interviews conducted by trained research assistants. Both assistants were aware of the purpose of the study and the way in which to administer the questionnaire.
The survey gathered information offered both spontaneously and in response to specific questions that addressed their knowledge about malaria. Questions about knowledge were open-ended to avoid guessing about the answers to multiple-choice questions, which might give a false impression concerning the participants’ knowledge. However, questions pertaining to practices were multiple-choice to assess the frequency with which participants’ performed the various activities and actions. At the end of each interview, the interviewers probed for further knowledge related to malaria that the respondents did not mention spontaneously. However, this was done only for selected variables, specifically their source(s) of information about the disease, history, and reasons for previous visits to clinics or hospitals, as well as the availability, condition, and use of ITNs. During the survey, direct observations were made concerning the use of ITNs, as well as housing conditions and cleanliness (including the availability of functioning toilets, indoor plumbing, water containers, and cisterns), and status of windows.
Blood sampling and examination
Approximately 2–3 ml of venous blood was drawn from each participant into an EDTA tube. Thick and thin blood films were prepared and a drop of the blood was used with an RDT kit, the “CareStart Malaria HRP2 from Access Bio, Inc.” Moreover, 2–3 drops were collected on 3 MM Whatman® filter paper (Whatman International Ltd., Maidstone, England) and kept in individual sealed plastic bags at room temperature until use. At Aminu Kano Teaching Hospital, Kano State, the blood films were stained with diluted Giemsa and then examined microscopically for the presence of malaria parasites; 200 fields under 1000× magnification were examined from the thick film before the slide was considered negative.
For positive slides, parasite species and stages were assessed and parasitaemia (parasite density) was determined by counting only the asexual stages against 300 white blood cells (WBC) and then multiplying by 25, assuming the mean total WBC count of individuals is 7500 cells per μl of blood [28]. The level of parasitaemia was recorded as low (<1000 parasites/μl of blood), moderate (1000–9999 parasites/μl of blood), and severe (≥10,000 parasites/μl of blood).
Molecular identification and genotyping
All malaria microscopy-positive slides and a random selection of 20 % of the negative slides were re-examined by another senior specialist at the Department of Parasitology, Faculty of Medicine, University of Malaya, Kuala Lumpur. Afterwards, all those samples were confirmed by PCR. Genomic DNA was extracted using the Qiagen blood and tissue kit (QIAGEN, DNeasy® Blood & Tissue Kit, Cat. no. 69506, Germany); the filter paper blood spot was cut using an ethanol flame–sterilized hole-punch, put into a new 1.5 ml microcentrifuge tube, and then extraction was conducted according to the manufacturer’s instructions. DNA was eluted using 50 µl AE (10 mM Tris–Cl; 0.5 mM EDTA; pH 9.0) elution buffer (included in the kit) and maintained at −20 °C until PCR analysis. Plasmodium species were identified by 18s rRNA-based nested PCR using genus- and species-specific nucleotides primer sets, as described previously [29].
During the survey, all RDT-positive individuals were treated for malaria according to the national malaria drug policy. Afterward, study participants were considered to have falciparum malaria if the positive RDT results were confirmed by blood smears microscopy or PCR. Participants with positive PCR results but negative blood smears microscopy were considered to harbour sub-microscopic parasitaemias and were recorded as positive. Moreover, those who were positive by RDT but negative by microscopy and PCR were considered negative as RDT may give false positive results in individuals with a recent history of malaria infection or due to other infections such as trypanosomiasis, toxoplasmosis, hepatitis C, schistosomiasis, dengue and leishmaniasis [30]. Overall, none of the RDT-negative cases was identified as positive by microscopy or PCR and this is consistent with a recent evaluation for RDT conducted in Nigeria [31].
Statistical analysis
Data were double entered by two different researchers into spreadsheets of SPSS, v. 20 (IBM Corporation, NY, USA). Then, a third researcher crosschecked the two datasets for accuracy and created a single dataset for analysis. The demographic, socioeconomic, environmental, and behavioural characteristics of the respondents, as well as the KAP variables were treated as categorical variables and presented as frequencies and percentages.
Pearson’s Chi squared test and Fisher’s exact test were used to test the associations between malaria prevalence and KAP items as the dependent variables, with the demographic (age, gender, and family size) and socioeconomic factors (educational and employment status, household monthly income, living near water sources, presence of functioning toilet in the house, housing conditions, using ITNs and insecticide, history of infection, and presence of domestic animals in the households) as the explanatory variables. All variables were coded as binary dummy variables. For example, malaria (positive = 1, negative = 0); gender (males = 1, females = 0), and so on. Odds ratios (OR) and 95 % confidence intervals (CI) were also computed for the explanatory variables. Moreover, participants were categorized into three age groups (<12, 12–17 and 18 years and older); however, they were re-categorized into two groups (children <18 years and adults 18 years and older) for analysis of the KAP variables. ORs at 95 % CIs were also computed. Multivariable logistic regression was conducted to identify the risk factors associated significantly with infection. To retain all possible significant associations, all variables that showed an association with p ≤ 0.25 were used in the multiple logistic regression model, as suggested by Bendel and Afifi [32]. A p < 0.05 was considered statistically significant.
Results
A total of 551 individuals participated in the study; 340 (61.7 %) were male, 211 (38.3 %) were female, and 64.1 % were adults aged 18 years and older. Table 1 shows the general demographic, socioeconomic, and environmental characteristics of the study participants. Among these, 23.0 % were inhabitants of Kura, 21.6 % of Bebeji, 17.6 % of Gwarzo, 18.0 % Shanono, and 19.9 % of Minjibir rural areas. Generally, the state government’s minimum wage is N18,000 (112.5 USD) per head; however, only 41.9 % of the respondents had a household monthly income of N32,000 (200 USD). In these communities, the houses were predominantly of traditional construction, with mud walls, but zinc roofing. The water supply was unstable; nevertheless, 64.6 % had drinking water, and 63.2 % used safe water for other domestic chores as well. The majority of the participants had LLIN distributed freely by the NMCP.
Prevalence and distribution of malaria
The prevalence of malaria infection was 60.6 % (334/551: Table 2). Overall, 15 RDT-positive cases were found negative by microscopy; however, five of them were confirmed positive by PCR. All infections were of P. falciparum and the majority (70.1 %) constituted low parasitaemia (<1000 parasites/μl of blood). Moreover, 10 (3.0 %) and 90 (26.9 %) cases were severe (≥10,000 parasites/μl of blood) and moderate (1000–9999 parasites/μl of blood), respectively. The asexual P. falciparum parasitaemia from the samples collected ranged from 50–12,500 parasites/μl of blood, with a geometric mean of 1023 parasites/μl. Overall, the prevalence of malaria was similar between males and females (61.2 vs 59.7 %; Chi square (χ2) = 0.12, p > 0.05). Similarly, there was no significant difference in prevalence according to location (χ2 = 2.31, p > 0.05). However, the prevalence differed significantly (χ2 = 9.40; p < 0.01) among age groups, with those aged 12–17 years having the highest prevalence (66.7 %). Among those aged less than 12 years, the overall prevalence was 42.9 % with those aged below 5 years having a prevalence of 37.5 %.
With regard to history of infection, approximately one-third (33.2 %) of the participants had experienced a recent malaria episode. A significant association was found between this history of infection and location (χ2 = 13.03, p < 0.05); Bebeji had the highest percentage (42.9 %) and Shanono the lowest (24.2 %). Approximately half of the respondents (49.5 %; 273/551) reported that they used ITNs, and there was a significant difference in use between age groups (p < 0.01) and location (p < 0.001), with participants aged 12–17 years (37.0 %), and those from Gwarzo (25.8 %) having the lowest percentage of use; there was no significant difference between males and females (p > 0.5).
Risk factors of malaria
Table 3 shows the results of the univariate analysis of the association between malaria and the potential explanatory variables. The results showed that age group, low family monthly income, and use of ITNs were associated significantly with malaria prevalence. A significantly higher prevalence was reported among participants aged 12 years and above (p < 0.01), those from families with low monthly income (<NGN 32,000) compared to their counterparts (67.1 vs 55.9 %; p < 0.05), and those who did not use ITNs compared to those who did (66.5 vs 54.6 %; p < 0.01).
The multiple logistic regression showed that participants aged 12 years and older were approximately twice as likely to have malaria compared to those younger than 12 years (adjusted OR = 2.23; 95 % CI = 1.19, 4.17). Similarly, low household monthly income (<NGN 32,000) was retained as a significant risk factor and was found to increase the odds of infection by 1.61 times (95 % CI = 1.14, 2.29). Moreover, it was found that not using ITNs increased participants’ odds for malaria by 1.57 times (95 % CI = 1.10, 2.24) when compared to those who used them. Interestingly, the type of toilet was considered in the regression model, based on the p < 0.25 [30], and was retained as the fourth significant risk factor of malaria (OR = 1.70; 95 % CI = 1.00, 2.88; p = 0.049).
Knowledge, attitudes, and practices regarding malaria
Knowledge of the cause, transmission, symptoms, and prevention of malaria, as well as the perception of its seriousness, is presented in Table 4. Generally, the respondents were well informed about malaria; 483 (95.6 %) knew about malaria (excluding children less than 10 years; thus n = 505). Knowledge about malaria was obtained primarily through personal/relatives’ experiences (48.9 %) or the media (27.3 %). Approximately one-fifth of the respondents (20.3 %) did not know the cause of malaria, but the majority (77.8 %) ascribed it to mosquitoes. Approximately three-quarters (77.8 %) of the respondents mentioned fever and slightly less than half mentioned weakness (48.2 %) as symptoms of malaria. Moreover, 69.6 % of the respondents indicated that they avoided mosquitoes by using bed nets or insecticide, while only 4.3 % replied that they did not know how to prevent malaria.
With respect to attitudes, most subjects (93.4 %) regarded malaria as a serious infection. The distribution of ITNs was high in the study area, and 78.2 % of the respondents had at least one ITN in their homes. However, only 48.3 % of the 505 respondents used ITNs, and only one-third (37.4 %) of the respondents used insecticide. With regard to treatment seeking behaviour, a considerable number of the respondents (375, 74.3 %) mentioned that they went to hospitals or clinics when they had an episode of fever, while 19.2 % of the respondents self-medicated as a first-line of treatment for fever; 3.8 % of the respondents did not treat malaria infection.
Tables 5 and 6 show the association between the respondents’ knowledge and attitudes about malaria and their age, gender, educational status, and household monthly income. The results showed significantly higher levels of knowledge of malaria symptoms, particularly weakness, vomiting, and abdominal pain among adult respondents than children. Adult participants had significantly lower levels of knowledge about mosquito bites (72.6 vs 81.8 %) as a cause of malaria, as well as using bed nets/insecticide (65.9 vs 78.3 %) as a preventive measure. Overall, the adults had better attitudes about the seriousness of malaria compared to those younger than 18 (95.6 vs 88.1 %).
With respect to gender, male respondents showed significantly higher levels of knowledge about malaria, particularly mosquito bites (82.6 vs 63.6 %) as a cause; fever as a symptom (83.3 vs 69.0 %); using bed nets/insecticide (79.9 vs 52.7 %); improved personal hygiene (27.8 vs 10.9 %), and medication (10.4 vs 1.6 %) as preventive measures. Moreover, significantly higher levels of knowledge of the role of mosquitoes in malaria transmission (81.6 vs 50.8 %) as well as fever (79.7 vs 66.2 %) and vomiting (23.4 vs 9.2 %) as symptoms of malaria, and using bed nets/insecticide to prevent infection (73.2 vs 46.2 %) were reported among educated respondents compared to their non-educated counterparts (Table 6). In addition, respondents who had household monthly incomes of ≥NGN 32,000 had significantly lower levels of knowledge about the role of mosquitoes in disease transmission (73.3 vs 83.0 %) compared to those having low household monthly incomes.
Discussion
This study reported high prevalence of malaria in Kano State as, where 60.6 % of the participants were found positive for P. falciparum. This is consistent with previous studies conducted in Kano and other Nigerian states. Moreover, recent malaria risk maps estimated that malaria prevalence in Nigeria varied from less than 20 % in certain areas to over 70 % in others [21]. This variation can be attributed to different climatic conditions, less rainfall, and surface water that serve as mosquito breeding sites. Previous studies from Kano State showed that 62.5 % (250/400) of the patients attending two hospitals in Kano Metropolis and 51.7 % (155/300) of the pregnant women attending antenatal clinic at a specialist hospital were malaria-positive [33, 34]. A similar high prevalence (61.3 %) was reported recently among pregnant women attending Aminu Kano Teaching Hospital [35]. In the same vein, over 22,000 deaths from malaria infection were reported in Kano State during 2015 [36]. These findings revealed that malaria continues to be a leading cause of morbidity and mortality in Kano, and suggested that innovative and effective interventions to control malaria should be identified and implemented in these communities.
Consistent with the present findings, previous studies among children in Kebbi, Awka, and Abuja States reported prevalence rates of 64.0 % (128/200), 59.6 % (118/198), and 58.0 % (233/400), respectively [20, 37, 38]. Similarly, previous studies reported P. falciparum prevalence rates of 62.4 and 57.1 % among pregnant women in Ogun and Niger Delta States, respectively [39, 40]. Nonetheless, higher prevalence rates were reported among pregnant women who visit primary healthcare facilities in Imo, Ogun, Gboko, Osun, and Benue States, where the prevalence rates were 80.1, 78.9, 76.9, 72 and 68.3 %, respectively [41–45]. Moreover, an extraordinary population-based prevalence rate (99.2 %) was reported among 2069 pregnant women in Enugu State, Southeastern Nigeria [46]. Similarly, a high prevalence rate (80 %) was reported among other populations in Southern Nigeria [16, 47].
In contrast, other previous studies reported lower prevalence rates: 39.2 % of 360 antenatal clients who visit primary healthcare facilities in Kano State [17], 29.4 % of 160 blood donors in Zaria State [18], 26 % of 400 pregnant women in Port-Harcourt, Rivers State [48], 35 % of 100 long distance truck drivers in Niger Delta State [49], 42.3 % in Otukpo, Benue state, 36.1 % (1060/2936) [50], and 36.6 % (1540/4209) in Abia and Plateau States, and 41.6 % (106/255) in pregnant women in a semi-urban community of Argungu, Kebbi State [51]. When compared to other sub-Saharan countries endemic for malaria, the prevalence reported in this study was higher than the 48.2, 47.8, 49.3 and 42.9 % reported in the Democratic Republic of the Congo [52], Mozambique [53], Burkina Faso [54], and Sierra Leone [55], respectively. Led by Nigeria, these countries are considered the top six among countries affected by malaria [56]. Similarly, a recent study revealed that 42.0 % of 2346 schoolchildren living in a high transmission area in Western Kenya were positive for P. falciparum [57].
Findings of the present study showed a similar prevalence rate among the male and female participants, which is consistent with previous studies in Nigeria, Kenya, and Mozambique, which suggests that the distribution of malaria risk is heterogeneous [19, 53, 58]. However, males were at higher risk of malaria infection due to exposure, and inherent and cultural determinants [59–62]. Coinciding with this, greater and repeated exposure to malaria among males may result in development of partial immunity that renders them at lower risk of clinical malaria compared to females [63], a situation reported in Western Kenya as well [57].
With respect to location, there were no significant differences in the prevalence of malaria among the districts studied; however, an obvious correspondence between a history of recent malaria and use of ITNs was observed, with the lowest percentage of history of recent malaria reported in Shanono (24.2 %), which also has the highest percentage of ITNs use (62.6 %). Due to the specific characteristics of populations that may facilitate human–mosquito contact, malaria risk can vary widely among districts, villages, and even households [64]. A recent study among children in Zambezia province, Mozambique showed that malaria prevalence varied among villages within the same province and ranged from 22.1 to 87.2 % [53].
The present study demonstrated that age, household monthly income, ITNs use and type of toilets were the significant risk factors associated with malaria among these participants. The present findings showed that prevalence was significantly higher among those aged 12–17 years (66.7 %) and ≥18 years (61.5 %) compared to those younger than 12 years (42.9 %). Interestingly, this difference could be explained by the reported age-specific use of ITNs; 60.3 % of those younger than 12 years compared to only 37.0 % of those aged 12–17 years used ITNs. Moreover, individuals aged 12 years and older are expected to have a higher exposure to mosquito bites because they engage in more outdoor activities compared to younger children, particularly at night. These findings are consistent with recent reports that rates of ITNs use were significantly higher among the youngest children, particularly those less than 5 years, and heads of the family, and this might be attributed to the inadequate ITNs per household [65]. Hence, these findings imply that the number of ITNs available to households should be increased to achieve universal coverage in these communities. Similarly, another study revealed that adolescent boys were least likely to use ITNs [15], while a recent study in Abia and Plateau States found that the prevalence of Plasmodium infection was associated significantly with age, with the highest prevalence among children 5–9 years [19]. In contrast, a recent study among Kenyan schoolchildren found that P. falciparum infection reduced with increasing age, and those aged 11–15 years had a 0.78 odds of infection compared to those aged 5–10 years [57].
The present study also showed that low household monthly income (<NGN 32,000) increased the odds of malaria among these children by approximately 1.5 times. This is consistent with previous reports from other African countries that showed malaria is more common among people of lower socioeconomic status who often live in poor housing conditions that increase their exposure to infection [57, 62, 66, 67]. Malaria and poverty are connected intimately, as malaria primarily affects low- and lower-middle income countries, where the poorest communities are affected most severely by malaria due to their poor socioeconomic and environmental status, and inadequate services for prevention, diagnosis, and treatment [5]. Hence, these endemic communities are trapped in a vicious cycle of poverty, underdevelopment, and disease [68]. Despite high IRS coverage and equitable ITN distribution, poverty at both the community and household levels was a significant risk factor for malaria in Northwestern Tanzania [69].
Use of ITNs is considered one of the most cost-effective interventions against malaria in endemic areas, and is associated with significant reductions in malaria morbidity and mortality, particularly among pregnant women and children less than 5 years [70]. The current study showed that failure to use ITNs was a significant risk factor for malaria among the population studied, which is consistent with previous studies in Nigeria and Ethiopia [51, 62].
Despite the high number of participants who had ITNs (79.5 %), only half of the participants stated that they used them, and were found to do so (49.5 %). This unsatisfactory compliance is consistent with previous studies in Nigeria [14, 19, 71–73] and other countries [74, 75]. A recent national study in Nigeria demonstrated a notable gap between ownership and use of ITNs and showed that, at the national level, only 28.7 % of the population had one in the household; this rate increased to 50.0 % in areas with a recent campaign (including Kano State) [72].
Interestingly, the present study showed that approximately one-third (30 %) of those who had ITNs and stated that they used them were found to misuse the nets; hence, they were considered non-users. The improper uses of the ITNs observed included employing bed covers, blankets, window curtains, and door curtains rather than actual ITNs. Moreover, some participants declared that they washed the ITNs before using them to remove the chemicals, which either have an unpleasant smell or induce allergies in some individuals. In addition, some of the ITNs were old and were not re-treated, while others were in poor condition. Similar misuse has been reported in different malaria-endemic African countries, including Nigeria, Uganda, Tanzania, Kenya, Zambia, Sierra Leone, and the Democratic Republic of Congo [76–81]. In addition to the misuses observed, a previous report indicated that some individuals who receive free ITNs frequently sell them on the open market, while many communities refuse to use them because of a misconception that they are purely a Western intervention that has been forced on African communities, with little regard for local norms or cultures [78]. Moreover, people do not use the ITNs because of a perception that malaria or mosquitoes are not a serious problem [76].
The present study also found that the type of toilet in the house was a significant risk factor for malaria in the communities studied, as those living in houses with pit or ground dug latrines were 1.7 times more likely to be infected with malaria than were those who have toilets in their houses with a pour/flush system. The lack of availability of in-home toilets has been reported to be a significant predictor of malaria in Ethiopia and Yemen [82, 83].
With respect to respondents’ KAP, findings the current study indicated that general awareness of malaria was high among Hausa communities in Kano State and almost all of them (95.6 %) had heard about malaria. This is expected, as malaria is considered the primary health problem in these communities [84–86]. Most of the respondents in the present study were well acquainted with malaria symptoms, and 77.8 % of them recognized fever as a detrimental consequence of malaria. Moreover, the present findings showed that the majority of the respondents had received information about malaria prevention, and using bed nets and/or insecticide, improving personal hygiene, and taking medication were the three main preventive measures they cited. This agrees with previous studies in other parts of Nigeria [87, 88], and other malaria-endemic countries [84, 86, 89]. However, a previous study among pregnant women from Ogun State in Southwest Nigeria showed that knowledge of malaria transmission and prevention was generally poor, in that only 36.3 % of the women associated malaria infection with mosquito bites, and none mentioned using ITNs as a preventive measure [39]. Similarly, a previous study among rural farming communities in Oyo State, Southwestern Nigeria, reported that only 12.4 % respondents were aware of the role of mosquito bites in transmitting the disease and less than half (46.7 %) were able to state at least one symptom of malaria [90]. Recent studies from Southwest Nigeria also revealed that knowledge of malaria remains low among caregivers of children less than five, pregnant women and mothers [80, 91].
The present study showed that the majority of the respondents (93.4 %) indicated that malaria is a serious disease, which is consistent with previous studies in Nigeria and other countries [84, 85, 88]. Moreover, this study showed that only a very small percentage (2.3 %) believed that malaria is not harmful. They claimed, “Malaria is not so serious because everyone has it, and cannot be cured.” Some said, “It sometimes causes fever, when one takes medication the fever goes away but the malaria does not, we are born with it.” Others stated, “Malaria cannot be cured, it always comes back,” and “Malaria is in our blood, it is always there, just avoid going down with fever by avoiding stress and always eat good food.” A few were indifferent, and believed that mosquito bites are simply a nuisance; it is good if they can be avoided, but otherwise they have no consequences. However, findings of the current study contradicted those of a recent study in Osun State, Southwest Nigeria, which demonstrated that the majority of the mothers believed that malaria is a simple disease for which they can comfortably apply home remedies [91]. Another hospital-based study about awareness of ITN use in Abeokuta State, Southwest Nigeria reported low awareness among the pregnant women interviewed [92].
Notwithstanding the high prevalence of attitudes that the disease is serious, approximately 20 % of the respondents tended to begin treatment at home and sought help from professionals only when it failed. Home treatment usually involved self-medication or unqualified prescription by family members, friends, and unauthorized shops. This behaviour did not different with malaria fever, wherein people began treatment with analgesics and then anti-malarial drugs if symptoms persisted. The same behaviour has been reported elsewhere in Nigeria [85, 93–95], and from other parts of Africa [96, 97]. Intriguingly, a previous study in Oyo state, Southwest Nigeria, showed that approximately 90 % of suspected malaria cases were self-treated first at home with traditional herbs or drugs purchased from medicine stores [85]. Moreover, a significant difference in treatment-seeking behaviour was reported between rural and urban mothers in Southeast Nigeria, in that two-thirds of urban mothers preferred private/government health facilities, while two-thirds of their rural counterparts preferred self-treatment with drugs bought over-the-counter from patent medicine vendors [94].
This study found that age, gender, educational level, and household monthly income had significant influences on having adequate knowledge about malaria. Younger respondents showed a greater level of knowledge about malaria transmission and prevention than did adults (aged 18 and older), which could be attributed to schools or media, especially television. Similarly, males had substantially higher levels of knowledge about malaria transmission, symptoms, and prevention, which could be because of their higher exposure, as well as certain behavioural and cultural factors. In Nigeria, the prevalence of malaria is highest among pregnant women compared to other groups [41, 42, 46]. Therefore, a health education programme about the disease that targets those women will result in a significant reduction in malaria in the country.
Similar high levels of knowledge about malaria transmission, and prevention were also reported among those having household monthly incomes below NGN 32,000 compared to their counterparts, which is inconsistent with the higher prevalence reported among those respondents. This suggests that the higher prevalence rate among this group is more related to the practices but not the knowledge. This finding also is consistent with previous studies in Nigeria [80, 90, 91]. Obviously, poverty hinders the efforts of malaria control programmes in the study area and other parts of Nigeria, which is worth noting, in that it can help policymakers target these specific populations and implement control measures. Previous studies in Nigeria have shown that the level of education was a strong predictor of positive malaria-related KAP [73, 85, 98]. Similarly, the choice of going to hospital on time depends on the level of education, as non-educated respondents are more likely to patronize unauthorized practitioners or buy medication from street vendors. This practice, combined with the poor quality of anti-malarial drugs in Africa, has led to the emergence and wide distribution of chloroquine-resistant malaria among the population [95, 99]. Therefore, policymakers should recognize that proper training of medical and paramedical personnel in malaria treatment and management must include those “shop operators,” as they are associated most closely with the population, and attitudes about the efficacy of treatment with their remedies cannot be altered immediately.
Conclusions
This study revealed that Nigeria’s battle against malaria has a long way to go. A high prevalence of falciparum malaria was reported among rural populations in Kano State. Hence, there is an urgent need to identify innovative and integrated control measures to reduce malaria prevalence significantly in these communities. Age, household monthly income, use of ITNs, and availability of in-house toilets were the significant predictors of malaria in this population. The study demonstrated that respondents had good levels of knowledge and attitudes regarding malaria transmission, symptoms, and prevention; however, these did not translate into improved preventive practices. The present study found that, despite the high level of ITNs ownership, their use still fell short of the national target. Hence, additional strategies, including community mobilization and more focused health education on the importance of using ITNs to control malaria and save lives, are required to increase use and improve current levels of ownership. That said, the number of ITNs distributed to households should be increased to ensure that populations living in malaria-risk areas have enough ITNs for all households members. Moreover, long-term interventions, such as providing job opportunities and improving the level of education to reduce poverty and improve the quality of life of these vulnerable communities also should be considered in order to achieve a breakthrough in the fight against malaria in Nigeria.
Abbreviations
- KAP:
-
knowledge, attitudes and practices
- ITNs:
-
insecticide-treated nets
- WHO:
-
World Health Organization
- NMCP:
-
National Malaria Control Programme
- RDT:
-
rapid diagnostic test
- NGN:
-
Nigerian Naira
References
WHO. World malaria report 2015. Geneva: World Health Organization; 2015.
WHO. 58th World health assembly. Technical document. Geneva: World Health Organization; 2005. http://www.who.int/nutrition/topics/WHA58.24_idd_en.pdf. Accessed 12 Jan 2016.
Korenromp EL, Hosseini M, Newman RD, Cibulskis RE. Progress towards malaria control targets in relation to national malaria programme funding. Malar J. 2013;12:18. doi:10.1186/1475-2875-12-18.
Murray CJ, Ortblad KF, Guinovart C, Lim SS, Wolock TM, Roberts DA, et al. Global, regional, and national incidence and mortality for HIV, tuberculosis, and malaria during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:1005–70. doi:10.1016/S0140-6736(14)60844-8.
WHO. World malaria report 2014. Geneva: World Health Organization; 2014.
Nigeria Federal Ministry of Health, National Malaria Control Programme. Strategic plan 2009–2013: “a road map for malaria control in Nigeria”, abridged version. Abuja: Yaliam Press Ltd, Federal Ministry of Health; 2009.
Kar NP, Kumar A, Singh OP, Carlton JM, Nanda N. A review of malaria transmission dynamics in forest ecosystems. Parasit Vectors. 2014;7:265. doi:10.1186/1756-3305-7-265.
Federal Ministry of Health. Malaria advocacy brief for policy makers. Abuja: Federal Ministry of Health; 2012.
WHO. Progress and impact series: focus on Nigeria. Geneva: World Health Organization; 2012.
Ye Y, Patton E, Kilian A, Dovey S, Eckert E. Can universal insecticide-treated net campaigns achieve equity in coverage and use? the case of northern Nigeria. Malar J. 2012;11:32. doi:10.1186/1475-2875-11-32.
USAID. Nigeria 2013 demographic and health final report. Rockville: United States Agency for International Development; 2013.
Adigun AB, Gajere EN, Oresanya O, Vounatsou P. Malaria risk in Nigeria: Bayesian geostatistical modelling of 2010 malaria indicator survey data. Malar J. 2015;14:156. doi:10.1186/s12936-015-0683-6.
WHO. World malaria report 2010. Geneva: World Health Organization; 2010.
Oyeyemi AO, Alawode A, Sogunro R. Ownership and utilization of LLIN after LLIN distribution campaign in a South Western state of Nigeria. Malar J. 2010;9(Suppl 2):P34. doi:10.1186/1475-2875-9-S2-P34.
Garley AE, Ivanovich E, Eckert E, Negroustoueva S, Ye Y. Gender differences in the use of insecticide-treated nets after a universal free distribution campaign in Kano State, Nigeria: post-campaign survey results. Malar J. 2013;12:119. doi:10.1186/1475-2875-12-119.
Ibekwe AC, Okonko IO, Onunkwo AI, Ogun AA, Udeze AO, Ejembi J. Comparative prevalence level of Plasmodium in freshmen (first year students) of Nnamdi Azikwe University in Awka, South-Eastern, Nigeria. Malays J Microbiol. 2009;5:51–4.
Gajida AU, Iliyasu Z, Zoakah AI. Malaria among antenatal clients attending primary health care facilities in Kano state, Nigeria. Ann Afr Med. 2010;9:188–93. doi:10.4103/1596-3519.68352.
Oche AO, Aminu M. The prevalence of malarial parasitaemia among blood donors in Ahmadu Bello University Teaching Hospital, Shika, Zaria, Nigeria. Niger J Med. 2012;21:445–9.
Noland GS, Graves PM, Sallau A, Eigege A, Emukah E, Patterson AE, et al. Malaria prevalence, anemia and baseline intervention coverage prior to mass net distributions in Abia and Plateau States, Nigeria. BMC Infect Dis. 2014;14:168. doi:10.1186/1471-2334-14-168.
Nmadu PM, Peter E, Alexander P, Koggie AZ, Maikenti JI. The prevalence of malaria in children between the ages 2-15 visiting Gwarinpa General Hospital life-camp, Abuja, Nigeria. J Health Sci. 2015;5:47–51. doi:10.5923/j.health.20150503.01.
Onyiri N. Estimating malaria burden in Nigeria: a geostatistical modelling approach. Geospat Health. 2015;10:306. doi:10.4081/gh.2015.306.
Ekeh HE, Adeniyi JD. Health education strategies for tropical disease control in school children. J Trop Med Hyg. 1988;91:55–9.
Govere J, Durrheim D, Grange KI, Mabuza A, Booman M. Community knowledge and perceptions about malaria and practices influencing malaria control in Mpumalanga province, South Africa. S Afr Med J. 2000;90:611–6.
Salam RA, Das JK, Lassi ZS, Bhutta ZA. Impact of community-based interventions for the prevention and control of malaria on intervention coverage and health outcomes for the prevention and control of malaria. Infect Dis Poverty. 2014;3:25. doi:10.1186/2049-9957-3-25.
Olofin EA, Nabegu AB, Dambazau AM. Wudil within Kano region: a geographical synthesis. Wudil: The Department of Geography, Kano University of Science and Technology; 2008.
National Malaria Control Programme (NMCP). Nigeria MIS final report. Abuja: Federal Republic of Nigeria; 2010.
Okwa OO, Akinmolayan FI, Carter V, Hurd H. Transmission dynamics of malaria in four selected ecological zones of Nigeria in the rainy season. Ann Afr Med. 2009;8:1–9. doi:10.4103/1596-3519.55756.
Dicko A, Sagara I, Djimde AA, Toure SO, Traore M, Dama S, et al. Molecular markers of resistance to sulphadoxine-pyrimethamine one year after implementation of intermittent preventive treatment of malaria in infants in Mali. Malar J. 2010;9:9. doi:10.1186/1475-2875-9-9.
Singh B, Bobogare A, Cox-Singh J, Snounou G, Abdullah MS, Rahman HA. A genus- and species-specific nested polymerase chain reaction malaria detection assay for epidemiological studies. Am J Trop Med Hyg. 1999;60:687–92.
Maltha J, Gillet P, Jacobs J. Malaria rapid diagnostic tests in endemic settings. Clin Microbiol Infect. 2013;19:399–407. doi:10.1111/1469-0691.
Ajumobi O, Sabitu K, Nguku P, Kwaga J, Ntadom G, Gitta S, et al. Performance of an HRP-2 rapid diagnostic test in Nigerian children less than 5 years of age. Am J Trop Med Hyg. 2015;92:828–33. doi:10.4269/ajtmh.13-0558.
Bendel RB, Afifi AA. Comparison of stopping rules in forward “stepwise” regression. J Am Stat Assoc. 1977;72:46–53.
Oyeyi TI, Hamidu MR, Dakata MA. Slide positivity rate of malaria among patients attending two hospitals in Kano Metropolis. Bayero J Pure Appl Sci. 2009;2:194–6.
Taura DW, Oyeyi TI. Prevalence of malarial parasites in pregnant women attending Sir Muhammad Sunusi Specialist Hospital, Kano, Nigeria. Bayero J Pure Appl Sci. 2009;2:186–8.
Isah MA, Darma AI, Sani I. Prevalence of malarial parasites in pregnant women attending Aminu Kano Teaching Hospital, Kano, Nigeria. Asian J Adv Basic Sci. 2014;3:117–21.
Health reporters, Africa’s online health newspaper. 2016. http://www.healthreporters.info/2016/04/27/kano-records-22000-malaria-deaths-in-2015. Accessed 8 Jun 2016.
Mbanugo JI, Ejims DO. Plasmodium infections in children aged 0–5 years in Awka Metropolis, Anambra State, Nigeria. Niger J Parasitol. 2000;21:55–9.
Singh R, Godson II, Singh S, Singh RB, Isyaku NT, Ebere UV. High prevalence of asymptomatic malaria in apparently healthy schoolchildren in Aliero, Kebbi state, Nigeria. J Vector Borne Dis. 2014;51:128–32.
Idowu OA, Mafiana CF, Sotiloye D. Traditional birth home attendance and its implications for malaria control during pregnancy in Nigeria. Trans R Soc Trop Med Hyg. 2008;102:679–84. doi:10.1016/j.trstmh.2008.03.020.
Madukaku CU, Nosike DI, Nneoma CA. Malaria and its burden among pregnant women in parts of the Niger Delta area of Nigeria. Asia Pac J Reprod. 2012;1:147–51. doi:10.1016/S2305-0500(13)60066-4.
Ohalete CN, Dozie IN, Nwachukwu MI, Obiukwu CE. Epidemiology and socio-economic consequences of malaria in pregnant women in Imo State Nigeria. Afr J Microbiol Res. 2011;5:3895–900.
Oladeinde BH, Omoregie R, Odia I, Oladeinde OB. Prevalence of malaria and anemia among pregnant women attending a traditional birth home in Benin City, Nigeria. Oman Med J. 2012;27:232–6. doi:10.5001/omj.2012.52.
Houmsou RS, Amuta EU, Sar TT, Adie AA. Malarial infection in pregnant women attending antenatal clinics in Gboko, Benue State, Nigeria. Int J Acad Res. 2010;2:33–6.
Adefioye OA, Adeyeba OA, Hassan WO, Oyeniran OA. Prevalence of malaria parasite infection among pregnant women in Osogbo, Southwest, Nigeria. Am Eur J Sci Res. 2007;21:43–5.
Amuta E, Houmsou R, Wama E, Ameh M, et al. Malarial infection among antenatal and maternity clinics attendees at the Federal Medical Centre, Makurdi, Benue State, Nigeria. Infect Dis Rep. 2014;6(1):5050. doi:10.4081/idr.2014.5050.
Gunn JK, Ehiri JE, Jacobs ET, Ernst KC, Pettygrove S, Kohler LN, et al. Population-based prevalence of malaria among pregnant women in Enugu State, Nigeria: the healthy beginning initiative. Malar J. 2015;14(1):438. doi:10.1186/s12936-015-0975-x.
Okonko IO, Soleye FA, Amusan TA, Ogun AA, Udeze AO, Nkang AO, et al. Prevalence of malaria plasmodium in Abeokuta,Nigeria. Malays J Microbiol. 2009;5:113–8.
Wogu MN, Nduka FO, Wogu MD. Prevalence of malaria parasite infection among pregnant women attending antenatal clinics in Port Harcourt, Rivers State, Nigeria. Int J Trop Dis Health. 2013;3:126–32.
Erhabor O, Azuonwu O, Frank-Peterside N. Malaria parasitaemia among long distance truck drivers in the Niger delta of Nigeria. Afr Health Sci. 2012;12:98–103. doi:10.4314/ahs.v12i2.4.
Jombo GTA, Mbaawuaga EM, Ayegba AS, Enenebeaku MNO, Okwori EE, Peters EJ, et al. How far have we rolled back malaria on the African continent nine years down? The burden of malaria among pregnant women in a semi-urban community of northern Nigeria. J Med Med Sci. 2010;1:235–41.
Fana SA, Bunza MD, Anka SA, Imam AU, Nataala SU. Prevalence and risk factors associated with malaria infection among pregnant women in a semi-urban community of north-western Nigeria. Infect Dis Poverty. 2015;4:24. doi:10.1186/s40249-015-0054-0.
Mvumbi DM, Bobanga TL, Melin P, de Mol P, Kayembe JN, Situakibanza HN, et al. High prevalence of Plasmodium falciparum infection in asymptomatic individuals from the Democratic Republic of the Congo. Malar Res Treat. 2016; 5405802. doi: 10.1155/2016/5405802.
Temu EA, Coleman M, Abilio AP, Kleinschmidt I. High prevalence of malaria in Zambezia, Mozambique: the protective effect of IRS versus increased risks due to pig-keeping and house construction. PLoS One. 2012;7:e31409. doi:10.1371/journal.pone.0031409.
Geiger C, Agustar HK, Compaoré G, Coulibaly B, Sié A, Becher H, et al. Declining malaria parasite prevalence and trends of asymptomatic parasitaemia in a seasonal transmission setting in North-Western Burkina Faso between 2000 and 2009–2012. Malar J. 2013;12:27. doi:10.1186/147-2875-12-27.
National Malaria Control Programme (Sierra Leone). Sierra Leone, Malaria indicator survey (MIS) 2013. https://www.dhsprogram.com/pubs/pdf/MIS15/MIS15.pdf. Accessed 13 Mar 2016.
WHO. Achieving the malaria MDG target: reversing the incidence of malaria 2000–2015. Geneva: World Health Organization and the United Nations Children’s Fund; 2015.
Kepha S, Nikolay B, Nuwaha F, Mwandawiro CS, Nankabirwa J, Ndibazza J, et al. Plasmodium falciparum parasitaemia and clinical malaria among school children living in a high transmission setting in western Kenya. Malar J. 2016;15:157. doi:10.1186/s12936-016-1176-y.
Brooker S, Clarke S, Njagi JK, Polack S, Mugo B, Estambale B, et al. Spatial clustering of malaria and associated risk factors during an epidemic in a highland area of western Kenya. Trop Med Int Health. 2004;9:757–66.
Bates I, Fenton C, Gruber J, Lalloo D, Medina LA, Squire SB, et al. Vulnerability to malaria, tuberculosis, and HIV/AIDS infection and disease. Part 1: determinants operating at individual and household level. Lancet Infect Dis. 2004;4:267–77.
Al-Mekhlafi AM, Al-Mekhlafi HM, Mahdy MA, Azazy AA, Fong MY. Human malaria in the highlands of Yemen. Ann Trop Med Parasitol. 2011;105:187–95. doi:10.1179/136485911X12987676649421.
Winskill P, Rowland M, Mtove G, Malima RC, Kirby MJ. Malaria risk factors in north-east Tanzania. Malar J. 2011;10:98. doi:10.1186/1475-2875-10-98.
Loha E, Lindtjørn B. Predictors of Plasmodium falciparum malaria incidence in Chano Mille, South Ethiopia: a longitudinal study. Am J Trop Med Hyg. 2012;87:450–9. doi:10.4269/ajtmh.2012.12-0155.
Smith T, Felger I, Tanner M, Beck HP. Premunition in Plasmodium falciparum infection: insights from the epidemiology of multiple infections. Trans R Soc Trop Med Hyg. 1999;93(Suppl 1):59–64.
Carter R, Mendis KN, Roberts D. Spatial targeting of interventions against malaria. Bull World Health Organ. 2000;78:1401–11.
Ferrari G, Ntuku HM, Schmidlin S, Diboulo E, Tshefu AK, Lengeler C. A malaria risk map of Kinshasa, Democratic Republic of Congo. Malar J. 2016;15:27. doi:10.1186/s12936-015-1074-8.
Noor AM, Gething PW, Alegana VA, Patil AP, Hay SI, Muchiri E, et al. The risks of malaria infection in Kenya in 2009. BMC Infect Dis. 2009;9:180. doi:10.1186/1471-2334-9-180.
Pullan RL, Bukirwa H, Staedke SG, Snow RW, Brooker S. Plasmodium infection and its risk factors in eastern Uganda. Malar J. 2010;9:2. doi:10.1186/1475-2875-9-2.
Gallup JL, Sachs JD. The economic burden of malaria. Am J Trop Med Hyg. 2001;64(1–2 Suppl):85–96.
West PA, Protopopoff N, Rowland M, Cumming E, Rand A, Drakeley C, et al. Malaria risk factors in North West Tanzania: the effect of spraying, nets and wealth. PLoS One. 2013;8:e65787. doi:10.1371/journal.pone.0065787.
Gamble C, Ekwaru JP, ter Kuile FO. Insecticide-treated nets for preventing malaria in pregnancy. Cochrane Database Syst Rev. 2006;2:CD003755.
Afolabi BM, Sofola OT, Fatunmbi BS, Komakech W, Okoh F, Saliu O, et al. Household possession, use and non-use of treated or untreated mosquito nets in two ecologically diverse regions of Nigeria-Niger Delta and Sahel Savannah. Malar J. 2009;8:30. doi:10.1186/1475-2875-8-30.
Kilian A, Koenker H, Baba E, Onyefunafoa EO, Selby RA, Lokko K, et al. Universal coverage with insecticide-treated nets—applying the revised indicators for ownership and use to the Nigeria 2010 malaria indicator survey data. Malar J. 2013;12:314. doi:10.1186/1475-2875-12-314.
Eteng M, Mitchell S, Garba L, Ana O, Liman M, Cockcroft A, et al. Socio-economic determinants of ownership and use of treated bed nets in Nigeria: results from a cross-sectional study in Cross River and Bauchi States in 2011. Malar J. 2014;13:316. doi:10.1186/1475-2875-13-316.
Al-Taiar A, Chandler C, Al-Eryani S, Whitty CJ. Knowledge and practices for preventing severe malaria in Yemen: the importance of gender in planning policy. Health Policy Plan. 2009;24:428–37.
Atieli HE, Zhou G, Afrane Y, Lee MC, Mwanzo I, Githeko AK, et al. Insecticide-treated net (ITN) ownership, usage, and malaria transmission in the highlands of western Kenya. Parasit Vectors. 2011;4:113. doi:10.1186/1756.3305.4-113.
Minakawa N, Dida GO, Sonye GO, Futami K, Kaneko S. Unforeseen misuses of bed nets in fishing villages along Lake Victoria. Malar J. 2008;7:165. doi:10.1186/1475-2875-7-165.
Baume C, Reithinger R, Woldehanna S. Factors associated with use and non-use of mosquito nets owned in Oromia and Amhara Regional States, Ethiopia. Malar J. 2009;8:264. doi:10.1186/1475-2875-8-264.
Eisele TP, Thwing J, Keating J. Claims about the misuse of insecticide-treated mosquito nets: are these evidence-based? PLoS Med. 2011;8:e1001019. doi:10.1371/journal.pmed.1001019.
Lowassa A, Mazigo HD, Mahande AM, Mwang’onde BJ, Msangi S, Mahande MJ, et al. Social economic factors and malaria transmission in Lower Moshi, Northern Tanzania. Parasit Vectors. 2012;5:129. doi:10.1186/1756-3305-5-129.
Adebayo AM, Akinyemi OO, Cadmus EO. Knowledge of malaria prevention among pregnant women and female caregivers of under-five children in rural southwest Nigeria. PeerJ. 2015;3:e792. doi:10.7717/peerj.792.
Kilian A, Koenker H, Obi E, Selby RA, Fotheringham M, Lynch M. Field durability of the same type of long-lasting insecticidal net varies between regions in Nigeria due to differences in household behaviour and living conditions. Malar J. 2015;14:123. doi:10.1186/s12936-015-0640-4.
Ayele DG, Zewotir TT, Mwambi HG. Prevalence and risk factors of malaria in Ethiopia. Malar J. 2012;11:195. doi:10.1186/1475-2875-11-195.
Bamaga O, Mahdy M, Mahmud R, Lim Y. Malaria in Hadhramout, a southeast governorate of Yemen: prevalence, risk factors, knowledge, attitude and practices (KAPs). Parasit Vectors. 2014;7:351. doi:10.1186/1756-3305-7-351.
Isah EC, Ofili AN, Ogbebor CE, Obahiagbon I, Isah AO. Knowledge of malaria and the practices towards its control among urban dwellers in Benin City. Niger Postgrad Med J. 2007;14:125–8.
Adedotun AA, Morenikeji OA, Odaibo AB. Knowledge, attitudes and practices about malaria in an urban community in south-western Nigeria. J Vector Borne Dis. 2010;47:155–9.
Kimbi HK, Nkesa SB, Ndamukong-Nyanga JL, Sumbele IU, Atashili J, Atanga MB. Knowledge and perceptions towards malaria prevention among vulnerable groups in the Buea Health District, Cameroon. BMC Public Health. 2014;14:883. doi:10.1186/1471-2458-14-883.
Erhun WO, Agbani EO, Adesanya SO. Malaria prevention: knowledge, attitude and practice in a South Western Nigerian community. Afr J Biomed Res. 2005;8:25–9.
Singh R, Musa J, Singh S, Ebere UV. Knowledge, attitude and practices on malaria among the rural communities in Aliero, northern Nigeria. J Fam Med Prim Care. 2014;3:39–44. doi:10.4103/2249-4863.130271.
Al-Adhroey AH, Nor ZM, Al-Mekhlafi HM, Mahmud R. Opportunities and obstacles to the elimination of malaria from Peninsular Malaysia: knowledge, attitudes and practices on malaria among aboriginal and rural communities. Malar J. 2010;9:137. doi:10.1186/1475-2875-9-137.
Oladepo O, Tona GO, Oshiname FO, Titiloye MA. Malaria knowledge and agricultural practices that promote mosquito breeding in two rural farming communities in Oyo State, Nigeria. Malar J. 2010;9:91. doi:10.1186/1475-2875-9-91.
Bello IS, Rehal S. A qualitative study exploring health seeking behaviour and cultural beliefs of mothers in paediatric malaria treatment decision-making process in Ile-Ife, South-West Nigeria. Malar J. 2014;13(Suppl 1):P9. doi:10.1186/1475-2875-13-S1-P9.
Runsewe-Abiodun T, Iyabo IA, Christy SA. Awareness and knowledge about insecticide treated nets (ITNs) amongst pregnant mothers in Ogun State, Western-Nigeria: a descriptive cross sectional study. Educ Res J. 2012;2:138–45.
Idowu OA, Mafiana CF, Luwoye IJ, Adehanloye O. Perceptions and home management practices of malaria in some rural communities in Abeokuta, Nigeria. Travel Med Infect Dis. 2008;6:210–4. doi:10.1016/j.tmaid.2007.10.007.
Okeke TA, Okeibunor JC. Rural-urban differences in health-seeking for the treatment of childhood malaria in south-east Nigeria. Health Policy. 2010;95:62–8. doi:10.1016/j.healthpol.2009.11.005.
Oladipo OO, Wellington OA, Sutherland CJ. Persistence of chloroquine-resistant haplotypes of Plasmodium falciparum in children with uncomplicated malaria in Lagos, Nigeria, four years after change of chloroquine as first-line antimalarial medicine. Diagn Pathol. 2015;10:41. doi:10.1186/s13000-015-0276-2.
Thera MA, D’Alessandro U, Thiero M, Ouedraogo A, Packou J, Souleymane OA, et al. Child malaria treatment practices among mothers in the district of Yanfolila, Sikaso region,Mali. Trop Med Int Health. 2000;5:876–81.
Deressa W, Ali A, Enqusellassie F. Self-treatment of malaria in rural communities, Butajira, southern Ethiopia. Bull World Health Organ. 2003;81:261–8.
Russell CL, Sallau A, Emukah E, Graves PM, Noland GS, Ngondi JM, et al. Determinants of bed net use in Southeast Nigeria following mass distribution of LLINs: implications for social behavior change interventions. PLoS One. 2015;10:e0139447. doi:10.1371/journal.pone.0139447.
Sawadogo CW, Amood Al-Kamarany M, Al-Mekhlafi HM, Elkarbane M, Al-Adhroey AH, et al. Quality of chloroquine tablets available in Africa. Ann Trop Med Parasitol. 2011;105:447–53. doi:10.1179/1364859411Y.0000000030.
Authors’ contributions
II, HMA, JI and YLL designed and supervised the study. SD, AUA and SIY conducted the sampling and field survey. SD and HMA analysed the data. SD, HMA and II wrote the paper. WMA, AMA, NAN, HS, FNE, MAA and LRS were involved in the laboratory examination of samples. AA supervised the sampling and field work activities. All authors read and approved the final manuscript.
Acknowledgements
The authors gratefully acknowledge the Ministry of Health, Kano State, Nigeria for their generous cooperation during this study. Thanks also are indebted to the participants for their voluntary participation in this study.
Competing interests
The authors declare that they have no competing interests.
Availability of data and material
Data will not be shared.
Ethics approval and consent to participate
The study was approved by the Medical Ethics Committee of the University of Malaya Medical Centre, Kuala Lumpur. All participants gave a written signed or thumb-printed consent to take part in the study.
Funding
This study was funded by the University of Malaya High Impact Research Grant UM-MOHE (UM.C/625/1/HIR/MOHE/MED/16) from the Ministry of Higher Education Malaysia, and also by the University of Malaya Research Grants; RG510-13HTM and RG331-15AFR. The funding bodies have no role in the study and publication process.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Dawaki, S., Al-Mekhlafi, H.M., Ithoi, I. et al. Is Nigeria winning the battle against malaria? Prevalence, risk factors and KAP assessment among Hausa communities in Kano State. Malar J 15, 351 (2016). https://doi.org/10.1186/s12936-016-1394-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-016-1394-3