
Abstract
Background
Malaria among school children is increasingly receiving attention, yet the burden of malaria in this age group is poorly defined. This study presents data on malaria morbidity among school children in Bungoma county, western Kenya.
Method
This study investigated the burden and risk factors of Plasmodium falciparum infection, clinical malaria, and anaemia among 2346 school children aged 5–15 years, who were enrolled in an individually randomized trial evaluating the effect of anthelmintic treatment on the risks of malaria. At baseline, children were assessed for anaemia and nutritional status and information on household characteristics was collected. Children were followed-up for 13 months to assess the incidence of clinical malaria by active detection, and P. falciparum infection and density evaluated using repeated cross-sectional surveys over 15 months.
Results
On average prevalence of P. falciparum infection was 42 % and ranged between 32 and 48 % during the five cross-sectional surveys. Plasmodium falciparum prevalence was significantly higher among boys than girls. The overall incidence of clinical malaria was 0.26 episodes per person year (95 % confidence interval, 0.24–0.29) and was significantly higher among girls (0.23 versus 0.31, episodes per person years). Both infection prevalence and clinical disease varied by season. In multivariable analysis, P. falciparum infection was associated with being male, lower socioeconomic status and stunting. The risk of clinical malaria was associated with being female.
Conclusion
These findings show that the burden of P. falciparum parasitaemia, clinical malaria and anaemia among school children is not insignificant, and suggest that malaria control programmes should be expanded to include this age group.
Similar content being viewed by others

Background
Significant progress in malaria control has been realized in the last decade with a number of countries, including Kenya, reporting decline in malaria transmission and hospital admission [1, 2]. The progress observed is largely due to the increase in access and use of proven malaria control interventions, combined with social and economic development [3–7]. Despite this reduction, malaria remains an important public health problem worldwide with endemicity in over 100 countries in the tropics and subtropics [8, 9].
Malaria prevention typically targets the highest risk groups; pregnant women and children under five who are most affected by the severe forms of the disease. However, there is increasing evidence suggesting that school-aged children (5–15 years) bear the highest burden of asymptomatic malaria irrespective of the transmission setting with a prevalence range between 14 and 64 % [10–14], and constitute nearly half of the population at risk of malaria [8]. Moreover, due to a decline in transmission and exposure in some areas, the peak age of clinical attacks of malaria is shifting from very young (under five) to older children [3, 15].
Both asymptomatic and clinical malaria have been shown to have a negative impact on the health and cognitive development of school children [16–22]. Although, school children are included in standard malaria intervention strategies, often they have the lowest coverage of malaria preventive measures, such as bed nets use [23, 24]. While reduction of infections is observed in younger age groups that are targeted by interventions, parasite prevalence among school aged children may even increase, as observed after the national distribution of bed nets in Kenya [25, 26]. In addition, as school children are rarely treated for these asymptomatic infections, they may contribute significantly to the infectious reservoirs of malaria [27, 28].
In order to adapt malaria control strategies to changes in transmission patterns, there is urgent need for data on asymptomatic and clinical malaria among different age groups. The present study aimed to describe patterns of Plasmodium falciparum infection and clinical malaria among school children living in an area of high malaria transmission in western Kenya. Specifically, this study investigated the burden of P. falciparum infection, clinical malaria, and anaemia, as well as associated risk factors.
Methods
Study area and participants
The study presents secondary analysis of longitudinal data arising from an individually randomized clinical trial evaluating the impact of repeated (every 4 months) anthelmintic treatment with albendazole on clinical malaria and malaria parasitaemia among school children [29]. The trial was conducted between February 2013 and October 2014 in Bumula District, Bungoma County, western Kenya. Malaria transmission is intense and perennial, with two seasonal peaks (May–August and November–December) associated with an increase in rainfall and predominantly caused by P. falciparum. A school survey conducted in 2009 reported that the prevalence of P. falciparum among school children in western Kenya was 21.6 % and with only 19.0 % of school children sleeping under a bed net the previous night [30]. The most recent Malaria Indicator Survey conducted in 2010 reported a slightly higher proportion of children sleeping under a bed net (28.0 %) in western Kenya and a compared to national use of 20 % [26]. There was a mass net distribution campaign that was conducted in 2011, that is reported to have increased the average net ownership from 1.0 per household to 2.6 as had been earlier [31].
The trial recruited 2346 children aged 5–15 years from 23 day schools [29]. The schools were recruited purposively based on their accessibility, all children in the selected schools were invited to be part of the study. Children with signs of severe malaria, aged >15 years, or suspected sickle-cell trait were excluded from the trial. For the purpose of the trial, children were selected based on soil transmitted helminths (STH) infection status and complemented by non-infected children to reach the required sample size, so that 1505 (64 %) had detectable STH infection. There was no difference between STH infected and uninfected children in terms of demographic parameters. However, children who did not have detectable STH infection were more likely to have P. falciparum infection, while parasite density was not significantly different between the two groups (Additional file 1). After 15 months of follow up, there was no difference in either the incidence of clinical malaria or prevalence of P. falciparum between the two treatment groups [29], therefore, all the children are combined in a single analysis in the present paper.
Baseline assessments and follow-up of children
Prior to the trial, a baseline household survey was conducted to collect information on socioeconomic characteristics, and children’s use of malaria prevention measures. During the baseline health survey, haemoglobin concentration was assessed from a finger prick blood sample using a HemoCue haemoglobin photometer (Hb 201 + , Ångelholm, Sweden), weight and height were recorded. Follow-up cross-sectional surveys at schools were conducted at 3, 7, 11, and 15 months (Fig. 1) when a finger-prick blood sample was collected from all children, irrespective of whether they had fever or not, thick and thin blood smears prepared. Active malaria case detection surveillance was conducted over 13 months of follow-up. School visits were conducted on a weekly basis, with absent children followed-up at home. Axillary temperature was measured using a digital thermometer. Children with documented fever (axillary temperature ≥37.5 °C) or who reported fever or any other signs and symptoms (headache, rigors, fevers, vomiting and chills) of malaria within the past 24 h were asked to provide a finger-prick blood sample, which was used to perform a malaria rapid diagnostic test (RDT) (Bioline Malaria Ag P.f/Pan, BD Biosciences, SanDiego, CA) and to prepare thick and thin blood smears. Children diagnosed with uncomplicated clinical malaria (fever or other malaria signs plus a positive RDT result) were treated using Coartem® (20 mg artemether/120 mg lumefantrine) in accordance with national guidelines. No cases of complicated malaria were encountered.

Timeline of the surveys conducted and active case detection during the 15 month follow-up period, among school children in Bumula district, western Kenya
Household and school locations of all enrolled children were mapped using a hand held GPS device (eTrex 20 Garmin Ltd., Olathe, KS, USA). Estimates of land surface temperature (LST), enhanced vegetation index (EVI), elevation and normalized difference vegetation index (NDVI) were extracted for each school after averaging the values of covariates within a 1-km catchment area around each school and household. Permanent water bodies were identified through intersecting gridded surfaces of the normalized difference water index (NDWI) for rainy and dry season. Those water areas which remain throughout the year were considered potential permanent breeding sites for mosquitoes. Straight-line distance (Euclidean distance) from schools to the nearest permanent body was calculated. A detailed description on how the data was obtained and extracted is provided in an additional file enclosed (Additional file 2).
Microscopy and laboratory techniques
Blood smears were air dried and stained with 3 % Giemsa for 45 min. Parasite density was defined as number of Plasmodium parasites per μL of blood, counted against 200 leukocytes assuming a leukocyte count of 8000/μL of blood. If fewer than 10 asexual parasites were detected in the first 200 leukocytes, counting was continued against 500 leukocytes. A blood smear was considered negative when the examination of 200 high power fields failed to reveal asexual parasites. Thin smears were used for species identification. All blood slides were read by two independent microscopists with discrepancies resolved by a third microscopist.
Ethical consideration
Written informed consent was obtained from a parent or guardian and assent was sought from children before enrollment into the study. The study was approved by the Kenya Medical Research Institute and KEMRI Ethics Review Committee (SSC no.2242), the London School of Hygiene and Tropical Medicine (LSHTM) Ethics Committee (6210), and the Makerere School of Public Health, Institutional Review Board (IRB00005876). The study was registered with the Clinical trial.gov NCT01658774.
Definition of variables
Three malariometric outcomes were considered; (1) malaria parasitaemia defined as P. falciparum infection at any density irrespective of presence fever as diagnosed by expert microscopy, (2) P. falciparum parasite density categorized in two groups: light (1–999 parasites/μL), and heavy (≥1000 parasites/μL), and (3) clinical malaria, defined as the presence of asexual P. falciparum parasitaemia as determined by microscopy plus either an axillary temperature >37.5 °C or a reported history of fever during the preceding 24 h. Children were considered at risk from their date of entry into the study until completing follow-up at 13 months. Children with documented or reported clinical malaria or known to have received medical attention from any source other than the survey team were censored for 28 days and those children who were absent from school for ≥10 days were censored for the time of absence [29]. Anaemia was defined using age and sex corrected WHO threshold adjusted by altitude [32] with a mid-point age assumed for the self-reported age for each child as there were doubts over the correctness of the age. Patterns of P. falciparum infection and clinical malaria were investigated by season: wet season (May–August and November–December) and dry season (January–April and September–October).
Individual and household-related variables
Principal component analysis was used to construct a household wealth index based on information on wall, floor, and roof construction materials, source of fuel, and education level of household head. The wealth index was then divided into two groups (termed poor and less poor) based on the median. Z-scores of height-for-age (HAZ), weight-for-age (WAZ) and body mass index for age (BMIZ) were calculated using the AnthroPlus software that uses the new 2006 WHO growth Ref. [33]. Children were classified as stunted, underweight, and thin if their HAZ, WAZ, and BMIZ, respectively, were less than −2 standard deviations (SDs) from the reference medium. Based on observed distribution, age was considered as categorical variable (5–10 years and 11–15 years). Three categories were generated to determine the consistency of bed net use; never (reported none use), sometimes (reported use at least once), and always (reported use at each survey) based on bed net use information collected during the five cross-sectional surveys.
Statistical analysis
Data were analysed using Stata version 13 (Statacorp, College Station). Summary statistics were calculated for all baseline data. Proportion of children with P. falciparum infection and anaemia together with their 95 % confidence interval (CI) was calculated using binomial regression analysis, adjusted for clustering by school. To allow for over dispersion in the distribution of parasites, arithmetic mean parasite counts with their 95 % CIs were estimated using a negative binomial regression model taking into account school clustering. Estimates of prevalence and density of P. falciparum infection were calculated by sex and survey. Incidence rates were calculated as number of events divided by person years at risk using survival analysis, and were estimated for each calendar month, stratified by sex and age group. Survival analysis for clinical malaria was presented using Kaplan–Meier curves. Prevalence rate ratios (P. falciparum infection and anaemia) and incidence rate ratios were calculated adjusting for clustering in schools. Most of the infections were of low parasite density and preliminary analysis indicated little variation and therefore no further analysis was undertaken of this outcome.
Risk factors of P. falciparum infection were identified using mixed effects logistic regression modelling, where P. falciparum infection status was treated as repeated measures (child random intercept), with additional random intercepts to adjust for clustering of children within schools and households. As most households had a single child, the study area was divided into 191 hexagons of 1 km diameter to which households were assigned based on their geographic location (1–66 children per hexagon). Hexagon defined clusters were favored over actual household clusters due to model convergence. All univariable and multivariable models for P. falciparum infection included a fixed term for survey round; this adjusted for the number of times a child contributed to the analysis, even if there was missing data at a particular follow-up survey. Univariable analysis was first performed including one covariate at a time and significant variables (P ≤ 0.05, based on likelihood ratio test) were included in multivariable analysis. Parsimonious regression models were developed using a backwards variable selection approach, eliminating one variable at a time based on the highest P value and retaining only variables with P ≤ 0.05.
Risk factors for incidence of clinical malaria were investigated using mixed effects Poisson regression. The models included a random intercept for children, however they failed to converge when clustering at both school and household level was considered. Hence models were adjusted only for clustering at household, as this is where infection is more likely to occur. Anaemia was not included in the variable selection procedure, because of potential reverse causality. The association of P. falciparum infection and anaemia was however subsequently tested adjusting for variables included in the minimum model. To investigate any potential effect of previous P. falciparum infections on incidence of clinical malaria, the final model was further tested including the number of P. falciparum infections experienced by a child as a fixed term.
Factors associated with baseline anaemia prevalence were identified using mixed effects logistic regression modelling with a random intercept to adjust for clustering within schools. Model selection procedures were followed as described above.
Results
Baseline child characteristics
In total, 2346 children aged 5–15 years from 1712 households were included in the study. Baseline characteristics of children are presented in Table 1. At baseline, the mean age was 10.4 years [standard deviation (SD): 2.5] and 47.5 % of children were female. A total of 1853 (79 %) children reported sleeping under a bed net the previous night and the proportion did not vary between boys and girls.
Plasmodium falciparum infection
The overall prevalence of P. falciparum infection was 42 % and was significantly higher among boys (45 vs 39 %, P < 0.001) and among younger (5–10 years) compared to older children (11–15 years) irrespective of sex (53.9 vs 46.1 %, P < 0.001) (Table 2). The prevalence of P. falciparum was significantly higher during wet season compared to the dry season (42.6 vs 40.6 %, P = 0.042). The majority (68 %) of the infections were light, having parasite densities < 1000 parasites/µl of blood. Densities did not vary by sex, but varied significantly by season (P < 0.001).
In univariable and multivariable analysis the odds of P. falciparum infection reduced with increasing age of children (P < 0.001). Additionally, P. falciparum infection was more common among boys, in children from households with lower socioeconomic status and who were anaemic (Table 3). Additionally, stunting was associated with increased odds of infection in multivariable analysis. However, there was no evidence for a lower risk of P. falciparum infection among children who slept under a bed net the previous night.
Incidence of clinical malaria
The total observation time during the 13 months of active case detection was 2310.8 person years, which was 85 % of the potential follow-up time. During the 13 months follow-up, 606 cases of malaria were recorded, corresponding to an overall incidence rate of 0.26 (95 % CI, 0.24–0.29) episodes per person-year. Of the 2346 children enrolled into the study, 1815 (77.4 %) did not experience any episode of clinical malaria during the follow-up period, 405 (17.3 %) children had only one episode and 93 (4 %) had two or more episodes of malaria. Having any episode and repeated episodes of clinical malaria was significantly higher among girls than boys (0.31 vs 0.23 episodes per person-year, P < 0.001) (Table 2; Fig. 2a) and girls were more likely to have repeated episodes of clinical malaria (P = 0.03). However, using alternative case definition with a parasite density cutoff of >2500 parasites/μL as used in previous studies [34], the incidence rate did not vary by sex (Table 2). Younger children (5–10 years) were 20 times more likely to have an episode of clinical malaria compared to the older age group (11–15 years) (P = 0.038). Although there were more girls in the younger age groups compared to boys, the incidence of malaria was higher in the older girls as shown in Fig. 2b with a higher cumulative risk of developing an episode of clinical malaria P < 0.001.

a Incidence rate of clinical malaria by sex and calendar month. b Cumulative risk of developing an episode of malaria by sex and age group over the 13 months follow-up among school children in Bumula District, western Kenya. Younger children (5–10 years), older children (11–15 years)
Incidence of malaria varied considerably by calendar month ranging from (0.00 to 0.80) episodes per person year with the peak corresponding with the wet season. When stratified by season and sex, the incidence rate varied among boys and girls between the seasons with broadly similar trends, (Table 2; Fig. 2a). In total, 361 (99 %) blood smears done during the wet season were confirmed as clinical malaria cases, compared to 248 (38 %) of the blood smears during the dry season.
In univariable analysis with season as a fixed term, clinical malaria was associated with being female (Incidence rate ratio 1.33, 95 % CI: 1.11–1.62), (Additional file 3). None of the other investigated factors were significant after adjusting for season and sex in multivariable analysis.
Geographic distribution of P. falciparum infection and clinical malaria
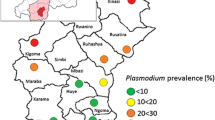
A map showing the location of households in the study area is provided in Fig. 3. Household GPS coordinates were missing for 408 children and sensitivity analysis showed that P. falciparum infection prevalence was higher among children with missing coordinates. Figure 3 shows the geographic distribution of clinical malaria and P. falciparum infection by households and survey round. P. falciparum infection occurred across the study area, but a subset of households in the west appeared to exhibit repeated P. falciparum infection with children from these households having 4–5 detected infections. Clustering of both P. falciparum infection and clinical malaria was more evident at school level, and followed a similar pattern to what was observed at household level (Fig. 4).

a Map of household locations, geographic distribution of b Plasmodium falciparum infection and c clinical malaria by household, during the 15 month follow-up period in Bumula district, western Kenya

Geographic distribution of Plasmodium falciparum infection by survey and clinical malaria as identified by active case detection, by school
Distribution of clinical malaria was skewed with majority of the children not experiencing any episode of clinical malaria (Fig. 4). Children with a single or no infection of P. falciparum during cross-sectional surveys had a higher cumulative risk for developing clinical malaria compared to children with repeated P. falciparum infection with a divergence of the survival curves occurring after 4 months as shown in Fig. 5 (P = 0.012). Only 11 % (364) of children did not experience any clinical malaria episode or P. falciparum infection.

Cumulative risk of developing an episode of clinical malaria, over the 13 months follow, by Plasmodium falciparum infection during the cross-sectional survey among school children. Abbreviations: Pf Plasmodium falciparum; Pf = 0 no P. falciparum infection; Pf = 1 single P. falciparum infection; Pf = 2 repeated (more than once) P. falciparum infections during the five surveys conducted
Anaemia
Overall, 834 children (38 %) were anaemic and anaemia was most common among 11–15 year-olds and among boys (Table 1). Among boys, anaemia was higher in the older age group (11–15 years) compared to 5–10 year-olds (P = 0.009), while in girls, although not significant, anaemia was higher among the younger age group (5–10 years) (P = 0.085). In univariable and multivariable analysis, anaemia was associated with being male, thinness, and presence of P. falciparum infection irrespective of number of times infected (Table 4).
Discussion
The epidemiology of malaria among school children has previously received little attention, with few studies looking at factors associated with the risk among African school children [12, 35]. However there is a renewed interest because of the shift from malaria control that targets high risk groups to a more inclusive approach and targets community-wide transmission [36]. There is, therefore, need for robust data for all age-groups on the burden of malaria to inform planning of control programmes. These results show that malaria burden among school children was considerable, with at least 30 % of children being infected with P. falciparum at any one of five surveys and one in five children experiencing an attack of clinical malaria. The current study showed that asymptomatic malaria was common among boys, stunted and anaemic children from households of lower socioeconomic status, while the incidence of clinical malaria was associated with being female.
The sex difference in P. falciparum infection has previously been reported in Africa [37–40]. Although studies on sexual dimorphism have been inconclusive and warrant further investigation, hypotheses of underlying reasons for such sex differences include estrogen or testosterone specific modulation of antiplasmodial immune [41]. Moreover, the lower risk of clinical malaria among boys may be attributed to development of partial immunity as a result of repeated exposure [42]. This is further supported by the observed lower cumulative risk in children with repeated detections of P. falciparum infection, as it was boys who were more likely to have P. falciparum infection at any one of the surveys. Even though the reported sex differences are interesting from an epidemiological perspective, the programmatic significance of these findings are comparably low. P. falciparum infection prevalence was high among boys and girls and, therefore, both should be equally considered in malaria control strategies.
Furthermore, in this study anaemia was prevalent (two in five children), and was shown to be associated with P. falciparum infection. Similar findings have been consistently reported among school-aged populations in Africa [17, 22, 43–46]. The mechanism through which Plasmodium infection causes anaemia is multifactorial and includes direct destruction of infected red blood cells (RBCs), rupturing of RBCs, hypersplenism, and reduced RBC production in the bone marrow [47, 48]. Both anaemia and P. falciparum infection were associated with poor nutritional status: thinness and stunting, respectively. Malnourished children have previously been shown to have increased risk of malaria [46]. As micronutrient deficiency is common in many malaria endemic areas, it is plausible that these children may have been anaemic initially and P. falciparum infection further added to the strain of anaemia [49]. In addition, intestinal helminth infections are common in Bumula [50] and may also contribute to the observed prevalence of anaemia, although no association was observed between anaemia and hookworm infection in the baseline survey.
The observed association of P. falciparum with low socioeconomic status is in agreement with previous studies that show malaria is more common among people of lower socioeconomic status who often live in poorly constructed houses increasing their exposure to infection [4, 24, 30, 51]. Bumula is one of the poorest districts in Kenya, with 79 % of the households having their floors and walls made of mud and 40 % having a grass thatched roof [52]. In this study 95 % of the children came from houses with walls and floors made of mud and 10 % had thatched roofs. Such house constructions have been found associated with higher malaria prevalence and indoor vector density [53, 54] while improved house structure and quality of construction material was associated with lower incidence of malaria [55]. Modern housing is suggested to offer protection by obstructing mosquito vector entry and reducing their density in the houses, as compared to traditional houses that have thatched roofs, walls and floors made of mud [56, 57]. Improvement of socioeconomic development has been shown to be an effective intervention against malaria [58].
In contrast to cross sectional studies conducted in various parts of Africa, where bed net use has been shown to be lowest among school children [23], 89 % of the children reported sleeping under a bed net the previous night at the baseline survey. Moreover, bed net use was not associated with reduced risk of P. falciparum infection or clinical malaria as would be expected, however the finding is agreement with the last malaria indicator survey that did not show an association of bed net use and Plasmodium infection in Lake Victoria region [31]. It is possible, although children reported ownership of a bed net, they do not consistently use it, as only 22 % stated to consistently sleep under a bed net. Additionally, most school children in rural parts of Africa sleep on the floor and therefore hanging the net may be a challenge [24, 30]. An alternative explanation for the lack of protective effect of bed nets in this study may relate to development of insecticide resistance among Anopheles spp. mosquitoes as previously has been reported in western Kenya [59].
As expected, the prevalence parasitaemia and incidence of clinical malaria fluctuated depending on the rainfall patterns. Western Kenya is a high malaria transmission area with a annual precipitation ranging 1200–1800 mm [60]. Higher prevalence of infection and incidence of clinical malaria were observed during the wet season, consistent, with what is known, transmission intensity varies with rainfall patterns [61]. Despite this seasonal variation, observed P. falciparum infection prevalence was important also during the dry season suggesting that transmission control interventions should not only be targeted to the wet season. Mapping of P. falciparum infection and clinical malaria by survey at school and household level showed pronounced spatial clustering in the western part of the study area. This may be explained by an insufficient spatial resolution of the environmental data used according to the size of the study area. It is well known that the major malaria vectors in the area (Anopheles gambiae s.s.) has greater affinity for small breeding sites such as animal footprints and small ponds formed during rainy season [62] which is hardly detected by medium resolution satellite imagery, such as those used in this study. Clustering was more evident at school level compared to households, suggesting that school based surveys may provide valuable insight into community transmission dynamics. School based surveys have been previously shown to provide a more cost-effective framework for the planning and evaluation of malaria control programmes [10]. It is more effective to survey children at schools compared to community based surveillance which often misses them [13].
The major strength of this study was the temporal dimension afforded by examination of a cohort over 1½ years, with 85 % follow-up rate. The study had a number of limitations. First, the children included in the main trial were from schools that were purposively selected based on accessibility, and therefore may not necessarily be representative of all school-aged children in the study area. However, these findings are similar to a study based on a representative sample of schools conducted in western Kenya [63]. Second, diagnosis was based on routine parasitological procedures and expert malaria microscopy may miss light infections when compared to more sensitive molecular methods [28]. School children have been shown in previous studies, to contribute substantially to sub microscopic infection and therefore the true prevalence may have been under estimated [13, 28]. Third, clinical malaria episodes were missed out if treatment was sought outside the study. Fourth, the age or quality of the bed net and relied on self-reported use. Bed nets may have been of poor condition or torn and therefore fail to provide adequate protection as has been previously reported in Kenya [64–66]. Fifth, haemoglobin level was only measured at baseline; a better assessment of the association of anaemia and clinical malaria could have been made by measuring haemoglobin levels for each suspected case.
Conclusion
The results show that the burden of clinical malaria, P. falciparum infection and anaemia was high among school children in Bumula district, western Kenya. Although reported bed net ownership was high, consistent use was low. Therefore, promoting bed net use among this age group may help to achieve the desired protective effect of this intervention. The study demonstrated the need to include school children in standard malaria interventions, which may alleviate the observed high anaemia burden.
References
Malaria atlas project. 2015. http://www.map.ox.ac.uk/ Accessed on 29 Sep 2015.
WHO. World Malaria Report 2014. Geneva: World Health Organization; 2014. http://www.who.int/malaria/publications/world_malaria_report_2014/wmr-2014-no-profiles.pdf.
Ceesay SJ, Casals-Pascual C, Erskine J, Anya SE, Duah NO, Fulford AJ, et al. Changes in malaria indices between 1999 and 2007 in The Gambia: a retrospective analysis. Lancet. 2008;372:1545–54.
Hay SI, Guerra CA, Tatem AJ, Atkinson PM, Snow RW. Urbanization, malaria transmission and disease burden in Africa. Nat Rev Microbiol. 2005;3:81–90.
WHO. Guidelines for the treatment of malaria. Geneva, Switzerland: World Health Organization; http://www.who.int/malaria/publications/world_malaria_report_2012/wmr2012_no_profiles.pdf 2012.
Noor AM. Measurement of the subnational effect of vector control interventions on malaria infection. Lancet Glob Health. 2014;2:e559–60.
O’Meara WP, Mangeni JN, Steketee R, Greenwood B. Changes in the burden of malaria in sub-Saharan Africa. Lancet Infect Dis. 2010;10:545–55.
Gething PW, Patil AP, Smith DL, Guerra CA, Elyazar IR, Johnston GL, et al. A new world malaria map: Plasmodium falciparum endemicity in 2010. Malar J. 2011;10:378.
Hay SI, Guerra CA, Gething PW, Patil AP, Tatem AJ, Noor AM, et al. A world malaria map: Plasmodium falciparum endemicity in 2007. PLoS Med. 2009;6:e1000048.
Brooker S, Kolaczinski JH, Gitonga CW, Noor AM, Snow RW. The use of schools for malaria surveillance and programme evaluation in Africa. Malar J. 2009;8:231.
Yeka A, Nankabirwa J, Mpimbaza A, Kigozi R, Arinaitwe E, Drakeley C, et al. Factors associated with malaria parasitemia, anemia and serological responses in a spectrum of epidemiological settings in Uganda. PLoS One. 2015;10:e0118901.
Nankabirwa J, Brooker SJ, Clarke SE, Fernando D, Gitonga CW, Schellenberg D, et al. Malaria in school-age children in Africa: an increasingly important challenge. Trop Med Int Health. 2014;19:1294–309.
Walldorf JA, Cohee LM, Coalson JE, Bauleni A, Nkanaunena K, Kapito-Tembo A, et al. School-age children are a reservoir of malaria infection in Malawi. PLoS One. 2015;10:e0134061.
Yapi RB, Hurlimann E, Houngbedji CA, Ndri PB, Silue KD, Soro G, et al. Infection and co-infection with helminths and Plasmodium among school children in Cote d’Ivoire: results from a national cross-sectional survey. PLoS Negl Trop Dis. 2014;8:e2913.
O’Meara WP, Mwangi TW, Williams TN, McKenzie FE, Snow RW, Marsh K. Relationship between exposure, clinical malaria, and age in an area of changing transmission intensity. Am J Trop Med Hyg. 2008;79:185–91.
Clarke SE, Jukes MC, Njagi JK, Khasakhala L, Cundill B, Otido J, et al. Effect of intermittent preventive treatment of malaria on health and education in schoolchildren: a cluster-randomised, double-blind, placebo-controlled trial. Lancet. 2008;372:127–38.
Kassebaum NJ, Jasrasaria R, Naghavi M, Wulf SK, Johns N, Lozano R, et al. A systematic analysis of global anemia burden from 1990 to 2010. Blood. 2014;123:615–24.
Fernando D, de Silva D, Carter R, Mendis KN, Wickremasinghe R. A randomized, double-blind, placebo-controlled, clinical trial of the impact of malaria prevention on the educational attainment of school children. Am J Trop Med Hyg. 2006;74:386–93.
Kihara M, Carter JA, Newton CR. The effect of Plasmodium falciparum on cognition: a systematic review. Trop Med Int Health. 2006;11:386–97.
Kurtzhals JA, Akanmori BD, Goka BQ, Adabayeri V, Nkrumah FK, Behr C, et al. The cytokine balance in severe malarial anemia. J Infect Dis. 1999;180:1753–5.
Nankabirwa J, Wandera B, Kiwanuka N, Staedke SG, Kamya MR, Brooker SJ. Asymptomatic Plasmodium infection and cognition among primary schoolchildren in a high malaria transmission setting in Uganda. Am J Trop Med Hyg. 2013;88:1102–8.
Nankabirwa JI, Wandera B, Amuge P, Kiwanuka N, Dorsey G, Rosenthal PJ, et al. Impact of intermittent preventive treatment with dihydroartemisinin-piperaquine on malaria in Ugandan schoolchildren: a randomized, placebo-controlled trial. Clin Infect Dis. 2014;58:1404–12.
Noor AM, Kirui VC, Brooker SJ, Snow RW. The use of insecticide treated nets by age: implications for universal coverage in Africa. BMC Public Health. 2009;9:369.
Pullan RL, Bukirwa H, Staedke SG, Snow RW, Brooker S. Plasmodium infection and its risk factors in eastern Uganda. Malar J. 2010;9:2.
Zhou G, Afrane YA, Vardo-Zalik AM, Atieli H, Zhong D, Wamae P, et al. Changing patterns of malaria epidemiology between 2002 and 2010 in western Kenya: the fall and rise of malaria. PLoS One. 2011;6:e20318.
DOMC. Division of Malaria Control [Ministry of Public Health and Sanitation], Kenya National Bureau of Statistics, and ICF Macro. 2010 Kenya Malaria Indicator Survey. Nairobi: DOMC, KNBS and ICF Macro; 2011. p. 2011.
Okell LC, Bousema T, Griffin JT, Ouedraogo AL, Ghani AC, Drakeley CJ. Factors determining the occurrence of submicroscopic malaria infections and their relevance for control. Nat Commun. 2012;3:1237.
Okell LC, Ghani AC, Lyons E, Drakeley CJ. Submicroscopic infection in Plasmodium falciparum-endemic populations: a systematic review and meta-analysis. J Infect Dis. 2009;200:1509–17.
Kepha S, Nuwaha F, Nikolay B, Gichuki P, Mwandawiro CS, Mwinzi PN, et al. Effect of repeated anthelminthic treatment on malaria in school children in Kenya: a randomized, open-label, equivalence trial. J Infect Dis. 2016;213:266–75.
Gitonga CW, Edwards T, Karanja PN, Noor AM, Snow RW, Brooker SJ. Plasmodium infection, anaemia and mosquito net use among school children across different settings in Kenya. Trop Med Int Health. 2012;17:858–70.
DOMC. Division of malaria control. Evaluation of the 2011 mass long-lasting insecticide treated net (LLIN) distribution campaign phase 1 and 2 report. 2011.
Benoist BME, Egli I, Cogswell M. Worldwide prevalence of anaemia 1993–2003: WHO global database on anaemia. Geneva: World Health Organization; 2008.
WHO. Anthroplus: growth reference 5–19 years. Geneva: World Health Organization; 2007.
Mwangi TW, Ross A, Snow RW, Marsh K. Case definitions of clinical malaria under different transmission conditions in Kilifi district, Kenya. J Infect Dis. 2005;191:1932–9.
Brooker S, Guyatt H, Omumbo J, Shretta R, Drake L, Ouma J. Situation analysis of malaria in school-aged children in Kenya—what can be done? Parasitol Today. 2000;16:183–6.
Delacollette C, Rietveld A. WHO/GMP-informal consultation on malaria elimination: setting up the WHO agenda. Tunis: World Health Organization; 2006.
Houngbedji CA, N’Dri PB, Hurlimann E, Yapi RB, Silue KD, Soro G, et al. Disparities of Plasmodium falciparum infection, malaria-related morbidity and access to malaria prevention and treatment among school-aged children: a national cross-sectional survey in Côte d’Ivoire. Malar J. 2015;14:7.
Loha E, Lindtjorn B. Predictors of Plasmodium falciparum malaria incidence in Chano Mille, South Ethiopia: a longitudinal study. Am J Trop Med Hyg. 2012;87:450–9.
Winskill P, Rowland M, Mtove G, Malima RC, Kirby MJ. Malaria risk factors in north-east Tanzania. Malar J. 2011;10:98.
Sarpong N, Owusu-Dabo E, Kreuels B, Fobil JN, Segbaya S, Amoyaw F, et al. Prevalence of malaria parasitaemia in school children from two districts of Ghana earmarked for indoor residual spraying: a cross-sectional study. Malar J. 2015;14:260.
Cernetich A, Garver LS, Jedlicka AE, Klein PW, Kumar N, Scott AL, et al. Involvement of gonadal steroids and gamma interferon in sex differences in response to blood-stage malaria infection. Infect Immun. 2006;74:3190–203.
Smith T, Felger I, Tanner M, Beck HP. Premunition in Plasmodium falciparum infection: insights from the epidemiology of multiple infections. Trans R Soc Trop Med Hyg. 1999;93(Suppl 1):59–64.
Halliday KE, Okello G, Turner EL, Njagi K, McHaro C, Kengo J, et al. Impact of intermittent screening and treatment for malaria among school children in Kenya: a cluster randomised trial. PLoS Med. 2014;11:e1001594.
Koukounari A, Estambale BB, Njagi JK, Cundill B, Ajanga A, Crudder C, et al. Relationships between anaemia and parasitic infections in Kenyan schoolchildren: a Bayesian hierarchical modelling approach. Int J Parasitol. 2008;38:1663–71.
Mathanga DP, Halliday KE, Jawati M, Verney A, Bauleni A, Sande J, et al. The high burden of malaria in primary school children in southern Malawi. Am J Trop Med Hyg. 2015;93:779–89.
Pullan RL, Gitonga C, Mwandawiro C, Snow RW, Brooker SJ. Estimating the relative contribution of parasitic infections and nutrition for anaemia among school-aged children in Kenya: a subnational geostatistical analysis. BMJ Open. 2013;3:e001936. doi:10.1136/bmjopen-2012-001936.
Akinosoglou KS, Solomou EE, Gogos CA. Malaria: a haematological disease. Hematology. 2012;17:106–14.
Menendez C, Fleming AF, Alonso PL. Malaria-related anaemia. Parasitol Today. 2000;16:469–76.
Nussenblatt V, Semba RD. Micronutrient malnutrition and the pathogenesis of malarial anemia. Acta Trop. 2002;82:321–37.
Kepha S, Nuwaha F, Nikolay B, Gichuki P, Edwards T, Allen E, et al. Epidemiology of coinfection with soil transmitted helminths and Plasmodium falciparum among school children in Bumula District in western Kenya. Parasit Vectors. 2015;8:314.
Noor AM, Gething PW, Alegana VA, Patil AP, Hay SI, Muchiri E, et al. The risks of malaria infection in Kenya in 2009. BMC Infect Dis. 2009;9:180.
KNBS. Kenya National Bureau of Statistics and Society for International Development (SID): exploring Kenya’s Inequality; pulling apart of pooling together. 2013.
Ghebreyesus TA, Haile M, Witten KH, Getachew A, Yohannes M, Lindsay SW, et al. Household risk factors for malaria among children in the Ethiopian highlands. Trans R Soc Trop Med Hyg. 2000;94:17–21.
Lwetoijera DW, Kiware SS, Mageni ZD, Dongus S, Harris C, Devine GJ, et al. A need for better housing to further reduce indoor malaria transmission in areas with high bed net coverage. Parasit Vectors. 2013;6:57.
Liu JX, Bousema T, Zelman B, Gesase S, Hashim R, Maxwell C, et al. Is housing quality associated with malaria incidence among young children and mosquito vector numbers? Evidence from Korogwe, Tanzania. PLoS One. 2014;9:e87358.
Animut A, Balkew M, Lindtjorn B. Impact of housing condition on indoor-biting and indoor-resting Anopheles arabiensis density in a highland area, central Ethiopia. Malar J. 2013;12:393.
Njie M, Dilger E, Lindsay SW, Kirby MJ. Importance of eaves to house entry by anopheline, but not culicine, mosquitoes. J Med Entomol. 2009;46:505–10.
Tusting LS, Willey B, Lucas H, Thompson J, Kafy HT, Smith R, et al. Socioeconomic development as an intervention against malaria: a systematic review and meta-analysis. Lancet. 2013;382:963–72.
Wanjala CL, Zhou G, Mbugi J, Simbauni J, Afrane YA, Ototo E, et al. Insecticidal decay effects of long-lasting insecticide nets and indoor residual spraying on Anopheles gambiae and Anopheles arabiensis in western Kenya. Parasit Vectors. 2015;8:588.
Bungoma County, Kenya County Fact Sheets, Commission on Revenue Allocation. 2011.
Hay SI, Snow RW, Rogers DJ. From predicting mosquito habitat to malaria seasons using remotely sensed data: practice, problems and perspectives. Parasitol Today. 1998;14:306–13.
Mulambalah CS, Siamba DN, Ngeiywa MM, Vulule JM. Anopheles species diversity and breeding habitat distribution and the prospect for focused malaria control in the Western Highlands of Kenya. Int J Trop Med. 2011;6:44–51.
Okoyo C, Mwandawiro C, Kihara J, Simiyu E, Gitonga CW, Noor AM, et al. Comparing insecticide-treated bed net use to Plasmodium falciparum infection among schoolchildren living near Lake Victoria, Kenya. Malar J. 2015;14:515.
Atieli HE, Zhou G, Afrane Y, Lee MC, Mwanzo I, Githeko AK, et al. Insecticide-treated net (ITN) ownership, usage, and malaria transmission in the highlands of western Kenya. Parasit Vectors. 2011;4:113.
Mutuku FM, Khambira M, Bisanzio D, Mungai P, Mwanzo I, Muchiri EM, et al. Physical condition and maintenance of mosquito bed nets in Kwale County, coastal Kenya. Malar J. 2013;12:46.
Githinji S, Herbst S, Kistemann T, Noor AM. Mosquito nets in a rural area of Western Kenya: ownership, use and quality. Malar J. 2010;9:250.
Authors’ contributions
SK, FN and SJB designed the study, SK and BN performed the analysis while RLP and EA contributed to the statistical aspects of the trial. All other authors played an important role in finalizing the study protocol and data interpretation (CSM, JNA JND JC, DM, KEH). SK, BN and SJB drafted the manuscript. All authors read and approved the final manuscript.
Acknowledgements
We thank children and parents who participated in this study, the cross-sectional survey, surveillance teams and technicians from KEMRI and Division of Vector Borne Diseases for working tirelessly. We acknowledge the ministries of Education and Health for support provided both at national and district level and the Bumula District hospital, in particular Belinda Kipsoi and Ruth Nyaudi. We thank Jimmy Kihara, Paul Gichuki, Samuel Oniare, Patrick Muteti, Julius Mayunga, and KEMRI (Center of Biotechnology Research and Development) for their support and contributions. This study is published with the permission of Director KEMRI.
Financial support
The trial was supported by the Dissecting the Immunological Interplay between Poverty Related Diseases and Helminth Infections: An African-European Research Initiative (IDEA) consortium, which is funded by the European Union through its FP7-HEALTH-2009 programme. SK is supported by a PhD training fellowship from THRiVE (Training Health Researchers into Vocational Excellence in East Africa) consortium, which is funded by the Wellcome Trust (087540), J. Nankabirwa and J. Ndibazza supported by the Malaria Capacity Development Consortium (WT084289MA) and the Bill & Melinda Gates Foundation (51941) and SJB is supported by a Wellcome Trust Senior Fellowship in Basic Biomedical Science (098045) which also supports RLP.
Competing interests
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Additional files
12936_2016_1176_MOESM1_ESM.doc
Additional file 1. Baseline characteristics among school children who were infected with any STH versus those who were uninfected in Bumula district. The table compares baseline characteristics of study children who were infected with any soil transmitted helminth versus those who were uninfected at recruitment.
12936_2016_1176_MOESM2_ESM.doc
Additional file 2. Sources and processing of environmental data. A summary of sources and processing procedures of environmental data is provided.
12936_2016_1176_MOESM3_ESM.doc
Additional file 3. Factors associated with incidence of clinical malaria among school children in Bumula, district. This table shows analysis of risk factors associated with clinical malaria.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kepha, S., Nikolay, B., Nuwaha, F. et al. Plasmodium falciparum parasitaemia and clinical malaria among school children living in a high transmission setting in western Kenya. Malar J 15, 157 (2016). https://doi.org/10.1186/s12936-016-1176-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-016-1176-y