
Abstract
Background
Maximal mid-expiratory flow (MMEF) is an earlier predictor of chronic obstructive pulmonary disease (COPD) development than forced expiratory volume in 1 s (FEV1). Changes of lung structure in patients with MMEF impairment only is still not clear. Therefore, this study aimed to investigate the structural features of patients with decreased MMEF by quantitative computed tomography (QCT) and develop a predictive model for predicting patients with reduced MMEF in normal lung function population.
Methods
In this study, 131 patients with normal spirometry results and available volumetric chest CT images were enrolled and divided into the reduced MMEF group (FEV1/forced expiratory vital capacity (FEV1/FVC) > 0.7, FEV1% predictive values (FEV1%pred) > 80%, MMEF%pred < 80%, n = 52) and the normal MMEF group (FEV1/FVC > 0.7, FEV1%pred > 80%, MMEF%pred ≥ 80%, n = 79). The emphysema, small airway disease and medium-size airway parameters were measured by a commercial software. The differences were investigated in clinical features, spirometrical parameters and QCT parameters between the two groups. A nomogram model was constructed based on the results of the multivariable logistic regression model. Spearman’s correlation coefficients were calculated between QCT measurements and spirometrical parameters.
Results
There were more males in reduced MMEF group than normal group (P < 0.05). Lung parenchyma parameter (PRMEmph) and airway-related parameters (functional small airway disease (PRMfSAD), luminal area of fifth- and sixth- generation airway (LA5, LA6) were significantly different between the reduced MMEF group and the normal group (20.2 ± 17.4 vs 9.4 ± 6.7, 3.4 ± 3.5 vs 1.9 ± 2.0, 12.2 ± 2.5 vs 13.7 ± 3.4, 7.7 ± 2.4 vs 8.9 ± 2.8, respectively, all P < 0.01). After multivariable logistical regression, only sex (odds ratio [OR]: 2.777; 95% confidence interval [CI]:1.123–3.867), PRMfSAD (OR:1.102, 95%CI:1.045–1.162) and LA6 (OR:0.650, 95%CI:0.528–0.799) had significant differences between the two groups (P < 0.05) and a model incorporating with the three indicators was constructed (area under curve, 0.836). Correlation analysis showed MMEF%pred had mild to moderate correlation with airway-related measurements.
Conclusion
In normal lung function population, patients with reduced MMEF have potential medium-size and small airway changes, and MMEF%pred is significantly associated with airway-related CT parameters. The nomogram incorporating with sex, PRMfSAD and LA6 has good predictive value and offers more objective evidences in a group with reduced MMEF.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Chronic obstructive pulmonary disease (COPD) is a type of progressively obstructive lung disease that is characterized by persistent respiratory symptoms and airflow limitation due to airways and alveolar abnormalities [1,2,3]. Forced expiratory volume in 1 s (FEV1) to forced expiratory vital capacity (FVC) of less than 0.7 is the gold standard to confirm the diagnosis of COPD [4], and a decrease in FEV1 is considered to be a predictor of COPD development [5]. However, recent studies suggest that maximal mid-expiratory flow (MMEF) values has been shown to occur before a decrease in FEV1, and could be an indicator of early disease [6, 7]. MMEF, also referred to as FEF25-75, defined by the the American Thoracic Society (ATS) and European Respiratory Society (ERS) as the mean forced expiratory flow between the 25% and 75% of the FVC [8], is widely accepted as a measure of small airways (diameter < 2 mm) obstruction. A 10-year follow-up study reported that MMEF is an earlier predictor of COPD development than FEV1 in normal lung function population [9]. Furthermore, a recent work reveals smokers with a decreased MMEF are approximately eight times more likely to develop COPD than patients with a normal MMEF, despite having FEV1% predicted (FEV1%pred) > 80% [10]. Indeed, MMEF rates have been considered a sensitive way to detect early stages of obstructive airway disease since the 1970s [11]. But MMEF has recently been found to be associated not only with small airway abnormalities, but also with lung parenchyma changes. Small airways abnormalities and destruction of lung parenchyma (emphysema) are major pathological hallmarks of COPD, which would contribute to airflow limitation via distinct mechanisms [12]. However, MMEF rates could not provide anatomic localization and quantitative characteristics of either of the two major disease. Computed tomography (CT) can serve as a complementary tool for pulmonary function test (PFT) by providing anatomic localization, differentiating airway disease from emphysema and characterizing emphysema subtypes [13]. Small airway disease can be inferred from an indirect measure of air trapping on CT images, and emphysema are the voxels with CT attenuation less than -950 Hounsfield unit (HU) on inspiration.
Therefore, the purpose of this study was to investigate the imaging features of patients with MMEF abnormalities and develop a predictive model for predicting patients with abnormal MMEF by CT images.
Methods
Study subjects
This prospective study was approved by the Ethics Committee of Huadong Hospital Affiliated to Fudan University (No. 2021K018), and informed consents were obtained from all patients. The study is based on a retrospective interpretation of prospectively acquired data. From July 2020 to May 2021, 312 participants who came for annual health screening without respiratory symptoms at our hospital were enrolled in the study. Subjects who met any of following criteria were considered for inclusion from the analysis with normal lung function results (FEV1/FVC > 0.7 and FEV1%pred > 80%), age > 40 years, no history of asthma or interstitial lung disease, and no history of lung surgery. Forty-one out of 184 eligible subjects were excluded because of incomplete data or poor CT scan quality (CT image quality evaluation detailed in CT examination). Finally, we remain 131 patients with normal PFT results and grouped them according to the MMEF predictive values (Fig. 1).

Flowchart of this study population
Clinical parameters
Clinical parameters, included the body-mass index (BMI), age, gender and smoking status, were collected to estimate differences between the two groups. BMI was calculated by dividing weight by height squared (kg/m2). Smoking status was classified as current-smoker, former-smoker and never-smoker according to the total number of smoked cigarettes, in accordance with previous studies [14, 15]. Current-smokers were considered to have smoked at least 100 cigarettes during their lifetime and currently smoked on a few days or every day. Former-smoker had smoked at least 100 cigarettes, but is current non-smoker. Never-smoker had never smoked or smoked less than 100 cigarettes in their life.
PFTs
All spirometry tests were performed within 1 month before or after CT scanning. The procedures were conducted on a Jaeger MasterScreen Pro lung function system (Jaeger Ltd, Hochberg, Germany) according to the ATS/ERS standardization of spirometry [16]. Baseline FEV1, FVC, FEV1/FVC, MMEF, residual volume (RV), total lung capacity (TLC), and RV/TCL values were obtained for the study. FEV1 and FVC were expressed as percentage of normal predicted values. In current study, to reduce the variability of MMEF and the influence of aging-related decline in lung function, MMEF was expressed as % predicted. Below 80% of predicted value was considered as MMEF abnormalities, as reported in previous studies [17, 18].
CT scanning
Prior to the examination, all patients had been previously instructed on how to perform the respiratory maneuvers while lying in the CT scanner acquisition bed. Patients underwent volumetric thin-section chest CT at both full inspiration and full expiration in the supine position. Scans were performed with a dual-source CT system (Somatom Definition Flash, Siemens Healthcare, Forchheim, Germany) in the caudocranial direction using the following parameters: tube voltage, 140 kVp; effective tube current, 100 mAs; slice thickness, 0.6 mm; picth, 1.0; and gantry rotation time, 0.5 s. The acquired data from the thoracic inlet to the lung base were reconstructed using B30f kernel. All the images were subjectively general evaluated by a radiologist (with 20 years of experience) according to the European Guidelines on Quality Criteria for Computed Tomography [19]. Diagnostic acceptability was evaluated with a four-point scale (1 = fully acceptable, 2 = probable acceptable, 3 = acceptable only in limited conditions, 4 = diagnostically unacceptable). Image noise was evaluated with a three-point scale (1 = too little or less than usual noise, 2 = acceptable noise, 3 = excessive noise). Images with diagnostic acceptability or image noise scores of 3 and above will be excluded for software analysis.
Quantitative image analysis
All CT images were evaluated using a commercial software (Aview, Coreline Soft, Seoul, Korea). Both lungs as well as each lung lobe were automatically segmented with manual edits as necessary by a professional radiographer. Emphysema was quantitated using the percentage of low-attenuation units less than -950HU at maximal inspiration, and recorded as emphysema index (EI). Small airway disease was quantified by Parametric response mapping (PRM) which utilizes image matching by deformed co-registered inspiratory and expiratory CT images and classifies based on a voxel-by-voxel comparison of lung attenuation changes: (1) functional small airway disease (PRMfSAD), are voxels greater than -950HU on inspiratory CT and less than -856HU on expiratory CT, (2) emphysema (PRMEmph), are voxels less than -950HU on inspiratory CT and less than -856HU on expiratory CT, (3) normal (PRMNormal), are voxels greater than -950HU on inspiratory CT and greater than -856HU on expiratory CT (Fig. 2). PRM data were expressed as percentage of total lung volume. Airways were automatically segmented and airway level was detected, and the airway parameters were recorded in medium-size airways, including Pi10, wall thickness (WT), airway wall area percent (%WA) and luminal area (LA). Pi 10 was the square root of the wall area of a hypothetical airway with 10 mm internal perimeter, which was a useful measure of airway wall thickness obtained by calculating a regression line that was plotted from the square root of the wall area of internal perimeters of multiple airways at different locations [20,21,22]. Wall thickness, airway wall area percent and luminal area were calculated from the average of whole lung fifth and sixth generation whole lung bronchial values. The software magnified the images tenfold to automatically detect airways lumens and to measure wall area and luminal area. The wall thickness was calculated using full-width-half-maximum (FWHM) measurement algorithm by detecting the inner and outer boundaries of the airway wall, as early study described [23]. Airway wall area percent was calculated as follows: WA / (WA + LA) *100.

Images of lung parameters in two patients. Notes: The first column shows the distribution of emphysema (displayed in blue). The second and third columns illustrate the distribution of voxels corresponding to PRM class (PRMfSAD voxels in yellow, PRMEmph voxels in red, and normal voxels in green). The last column shows the tracheobronchial tree generated by three-dimensional reconstruction; a A 61-year old male with reduced MMEF (FEV1/FVC = 0.84, FEV1%pred = 91.6%, MMEF%pred = 67.0%). The emphysema index is 5%. PRMfSAD, PRMEmph and PRMNormal are 16%, 4% and 78% respectively. The luminal area of the fifth- and sixth- bronchi are 10.4 mm2 and 5.2 mm2 respectively; b A 58-year old female with normal pulmonary function (FEV1/FVC = 0.96, FEV1%pred = 99.0%, MMEF%pred = 121.1%). The emphysema index is 3%. PRMfSAD, PRMEmph and PRMNormal are 1%, 1% and 97% respectively. The luminal area of the fifth- and sixth- bronchi are 14.3 mm2 and 6.6 mm2 respectively. PRM, Parametric response mapping; PRMEmph, emphysema by PRM; RPMfSAD, functional small airway disease; PRMNormal, normal lung parenchyma by PRM
Finally, the quantitative computed tomography (QCT) measurements used in this study included EI, PRM (PRMfSAD, PRMEmph, PRMNormal), Pi10, mean %WA of the 5th and 6th generation bronchi, mean WT of the 5th and 6th generation bronchi and LA of the 5th and 6th generation bronchi.
Statistical analysis
All statistical analyses were performed using R software (version 3.5.1; http://www.Rproject) and MedCalc Software (version 16.8.4, http://www.medcalc.org). Parametric data were expressed as mean ± standard deviation, and nonparametric data were expressed as numbers and percentages. Student’s t test was used for continuous variables, Pearson’s chi-squared test and Fisher’s exact test was used for categorical variables. Clinical and imaging variables with a P value < 0.1 on univariable analysis were selected as input variables for multivariable logistic regression analysis with a backward stepwise selection mode. A nomogram model was constructed based on the results of the multivariable logistic regression model to make the result of this research feasible to clinicians. Calibration curve was plotted to assess the fitting efficiency of the nomogram.
The receiver operating characteristic (ROC) curve and area under the ROC curve (AUC) were used to evaluate the predictive nomogram. Spearman’s correlation coefficients were calculated between QCT measurements and pulmonary function parameters. Correlation coefficients were interpreted according to the following categories: r < 0.3, mild correlation; 0.3 < r < 0.7, moderate correlation; and r > 0.7, strong correlation. Two-sided P-value less than 0.05 was considered statistically significant.
Results
Patients’ characteristics
The final cohort compromised 131 subjects with normal pulmonary function test and evaluable quantitative CT, and patients were divided into two groups based on the predictive MMEF%: 52 cases of the reduced MMEF group (FEV1/FVC > 0.7, FEV1%pred > 80%, MMEF%pred < 80%), 79 cases of the normal MMEF group (FEV1/FVC > 0.7, FEV1%pred > 80%, MMEF%pred ≥ 80%). The clinical characteristics, pulmonary function results and QCT parameters are presented in Table 1. There was a greater proportion of males in reduced MMEF group than that in the normal group (63.5% vs 41.8%, P = 0.015). But the smoking status was not significantly different between the two groups (P = 0.085). Compared with PFT results between the two groups, FEV1%pred values in the reduced MMEF group were significantly lower than those in the normal MMEF group, while there was no significant difference in actual measurements of FEV1 between the two groups. Although FEV1/FVC was significantly different between the two groups, these values were all within the normal ranges. There was no significant difference in EI value between the reduced MMEF group and normal group (5.7 ± 5.5 vs 4.0 ± 4.1, P = 0.051). The average values of PRMfSAD, PRMEmph and PRMNormal were significantly different between the reduced MMEF group and the normal group (20.2 ± 17.4 vs 9.4 ± 6.7, 3.4 ± 3.5 vs 1.9 ± 2.0, 73.8 ± 19.7 vs 85.3 ± 10.0, respectively, all P < 0.05). The average the luminal area of fifth generation bronchi (LA5) and the luminal area of sixth generation bronchi (LA6) value were significantly smaller in reduced MMEF group than that in normal MMEF group (12.2 ± 2.5 vs 13.7 ± 3.4, 6.9 ± 2.0 vs 8.9 ± 2.8, respectively, all P < 0.05). Pi10, airway wall thickness and wall area percent showed no significant difference between reduced MMEF group and normal MMEF group (all P > 0.05).
Association of CT parameters with spirometrical results
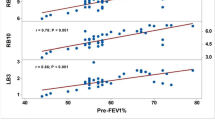
The quantitative CT parameters with significant differences were selected for the correlation analysis to evaluate the pulmonary function parameters, and the results are presented in Supplementary Table S1. Most of the quantitative CT parameters has significant correlation with PFT results. MMEF %pred has significant correlation with small airway parameter (PRMfSAD), medium airway parameters (LA5, LA6), with stronger correlation with LA6 than other QCT parameters (r = 0.338, P < 0.001). FEV1%pred was significantly correlated with the luminal area of the 6th generation bronchi only and not correlated with luminal area of the 5th generation bronchi.
Nomogram and calibration curve
Sex, smoking status, EI, PRM parameters, Pi10, LA5 and LA6 were used as input variables for the multivariable regression analysis. Sex, PRMfSAD and LA6 remained significantly different between the two groups after multivariable regression analysis, and other parameters showed no significance (all P > 0.05). Subsequently, the three parameters were selected to establish the model (Table 2), and nomogram of the model shows in Fig. 3A. Calibration plots were used to visualize the performance of the nomogram (Fig. 3B). To demonstrate the clinical advantages of the nomogram, we compared the receiver operating characteristic (ROC) curves of the single variables against the model (Fig. 4). It was revealed that the area under the curve (AUC) values of sex, PRMfSAD and LA6 were 0.608 (95% confidence interval (CI):0.519–0.693), 0.709 (95% CI: 0.624–0.785) and 0.705 (95% CI: 0.619–0.782) respectively, while the AUC value of nomogram was 0.836 (95% CI: 0.762–0.895). DeLong’s test was used to compare the difference in the ROC curves and showed that the nomogram performed better than sex, PRMfSAD and LA6 alone (all P < 0.05).

Construction of the nomogram. Notes: 1 for female, 0 for male. a Nomogram predicting MMEF reduction; b Calibration curves for the nomogram. fSAD, functional small airway disease; L6, luminal area of 6th-genneration bronchi

The ROC curves of the nomogram and the single variables. Notes: Combined was the model incorporating with sex, fSAD and LA6. fSAD, functional small airway disease; LA6, luminal area of 6th-genneration bronchi
Discussion
In the present study, we investigated the CT image characteristics of patients with decreased MMEF in a normal lung function population, analyzed the correlations between the quantitative CT parameters and lung function parameters, and developed a predictive model for predicting patients with reduced MMEF.
A study found that patients with reduced MMEF had a greater proportion of males than normal subjects but it is not clear whether sex is a risk factor for MMEF reduction [9]. Stockly et al. [18] analyzed a cohort of α1-antitrypsin deficiency (AATD) non-smokers and found that most of the patients in whom MMEF decreased were females. The population of the present study differs from that of the Stockly et al.’s study and includes both smokers and nonsmokers without AATD. In this study, there was a significant difference in sex between reduced MMEF group and normal group and sex was found to be a predictor for distinguishing between the two groups. Additionally, no significant difference in EI was found between the reduced MMEF group and normal group, while difference in PRMEmph was found between the two groups. Both the emphysema parameters, EI and PRMEmph, which reflect pulmonary parenchyma destruction, were less than 6%, indicates that there was no emphysema in the reduced MMEF group, since the Fleischner Society guidelines define emphysema as present only when pixels less than -950HU at quantitative CT are more than 6% [24]. This result is in line with previous studies [18, 25]. Besides, Burgel [26] suggested the key factor leading to airflow limitation in early COPD is small airway disease rather than emphysema. However, changes in the small airways cannot be visualized with current CT capabilities. Investigators have explored measuring air trapping to quantify small airway disease in CT, including measurements of LAA-856exp (lung voxels with CT attenuation less than or equal to -856 HU measured on expiratory CT scan), E/I (ratio of mean lung attenuation on expiratory and inspiratory scans) and PRM [27,28,29]. However, E/I is not able to provide spatial information related to disease distribution and LAA-856exp do not discriminate between air trapping as a result from emphysema or air trapping as a result from small airway disease. PRM uses digitally co-registered inspiratory and expiratory CT scans to compare individual voxel lung attenuation changes allowing differentiation of emphysematous from non-emphysematous air trapping within the lung parenchyma [30]. This non-emphysematous air trapping could reflect the functional changes of small airways, so it is called "functional small airway disease (PRMfSAD)". Vasilescu and colleagues [31] performed CT and micro-CT examinations of lung tissue and have confirmed the PRMfSAD correlated well with pathological small airway disease. Lu et al. [32] showed that among patient with abnormal lung function (FEV1predicted % < 80% or FEV1/FVC < 0.70), air trapping on CT images in patients with reduced MMEF was more severe in than subjects without MMEF reduction, a result is similar to that of Arakawa and colleagues [33]. However, in the studies by Lu et al. and Arakawa et al., they all used air trapping as a proxy for small airway disease, which may exaggerate the extent of small airway disease in patients with decreased MMEF owing to the effects of emphysematous air trapping and overestimate the correlation between MMEF and small airways overestimate the correlation between MMEF and small airways. In this paper, small airway disease was assessed by using PRMfSAD from dual gas phase CT image analysis, which may be more helpful in accurately evaluating the relationship between MMEF impairment and small airway disease. Additionally, the current study found that functional small airway disease, which is a prominent predictor of the model, was significantly higher in MMEF impairment group than in normal group. PRM parameters have been found to be strongly correlated with MMEF%pred, but PRMfSAD was more strongly associated with MMEF%pred than the other two PRM parameters. The result is similar to a smoker study from SPIROMICS cohort [34] in which an increase in PRMfSAD is significantly associated with lower MMEF%pred even adjusted FEV1%pred and FVC%pred. Therefore, our analysis supports that patients with MMEF%pred reduction have no destruction to lung parenchyma but changes in small airways, and PRMfSAD also has a good differentiation for normal and reduced MMEF.
In addition, the medium-size airway measurement parameters also need to be noted. We found no evidence for differences in airway wall thickness measurements, including Pi10 and WT, between subjects with and without MMEF reduction. Nambu et al. [35] concluded that CT images of patients with reduced MMEF showed thicker airway walls, which is inconsistent with our results. However, their research included all COPD patients and not adjusted for the effects of airway remodeling due to other apparently abnormal spirometrical parameters. Airway wall thickening could be due to airflow obstruction [36], whereas none of the patients enrolled in this study had evidence of respiratory airflow obstruction. Qin and colleagues [25] studies smokers and found there was no difference in percentage of the third-, fifth- and ninth-generation bronchial wall area between normal subjects and patients with MMEF reduction. Similarly, in the study, through the analysis of normal and decreased MMEF populations, we found no significant difference in fifth- and sixth-generation bronchial wall area percent between the two groups. Nevertheless, the CT scan lumen area in fifth- and sixth-generation airways was significantly reduced in patients with reduced MMEF compared with health controls and reduced luminal area in fifth- and sixth-generation airway was associated with a reduced MMEF%pred. Previous study of asthmatics has also shown that the smaller airway lumen in patient with decreased MMEF%pred, which the researchers believe that may the mucus accumulation reduce the airway luminal area [37], the but it needs to be further studied.
In the current study, we performed a quantitative analysis on patients with MMEF reduction, and found no lung parenchyma destruction but potential medium and small airway changes in these patients compared to subjects without decrease MMEF. Furthermore, a predictive model was developed based on sex, PRMfSAD and LA6 for predicting patients with MMEF impairment with AUC of 0.836. Besides, correlation analysis revealed a strong correlation between MMEF and airway-related CT parameters. MMEF impairment has been commonly reported to be associated with some respiratory cdisease, such as allergic rhinitis, asthma and bronchiolitis obliterans [38,39,40], and other systemic disease associated with decreased MMEF has been rarely reported [41, 42]. This article only discusses the structural lung abnormalities associated with decreased MMEF, but does not explore whether other systemic abnormalities are also correlated with decreased MMEF, which will require further study in the future.
This study also has some limitations. First, parametric response mapping analysis needs dual-phase CT scanning which increase the expose of radiation dose. Second, due to the limited resolution of CT, the wall thickness of airway with diameter less than 2 mm may be overestimated and luminal area can be underestimated. However, an optical coherence tomography study revealed airways with diameter less than 2 mm located at the seventh (or higher) airway generation [43]. Therefore, resolution has little influence on the evaluation accuracy of direct airway parameters from 5th- and 6th-genneration bronchi in the current study. Third, the correlation between pulmonary function test results and CT parameters are not as strong as previous studies, possibly due to the relatively small sample size. Last, the study is a cross-sectional research about patients with MMEF reduction and it is unclear whether these patients will develop COPD later in life. Further studies will enroll more subjects and follow them longitudinally to observe if they will develop COPD.
Conclusions
In summary, our study shows that in normal lung function population, patients with reduced MMEF have potential medium-size and small airway changes, and MMEF is significantly associated with airway-related CT parameters. The nomogram incorporating with sex, PRMfSAD and LA6 can has good predictive value. The present study offers new insight into the pathologic changes captured by CT scan in a group with reduced MMEF and potentially assists clinicians to take early interventions in these patients.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- COPD:
-
Chronic obstructive pulmonary disease
- FEV1 :
-
Forced expiratory volume in 1 s
- FVC:
-
Forced vital capacity
- MMEF:
-
Maximal mid-expiratory flow
- PFT:
-
Pulmonary function test
- PRM:
-
Parametric response mapping
- QCT:
-
Quantitative computed tomography
- RV:
-
Residual volume
- TLC:
-
Total lung capacity
- WA:
-
Wall area
- WT:
-
Wall thickness
- LA:
-
Luminal area
- PRMEmph :
-
Emphysema by PRM
- PRMfSAD :
-
Functional small airway disease
- PRMNormal :
-
Normal lung parenchyma by PRM
- EI:
-
Emphysema index
References
Cosio MG, Guerassimov A. Chronic obstructive pulmonary disease. Inflammation of small airways and lung parenchyma. Am J Respir Crit Care Med. 1999;160:S21-5.
Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138:16–27.
Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2022 Report.Global Initiative for Chronic Obstructive Lung Disease. Available at:http://goldcopd.org/2022-gold-reports/. Accessed February 9, 2022.
Laucho-Contreras ME, Cohen-Todd M. Early diagnosis of COPD: myth or a true perspective. Eur Respir Rev. 2020;29:200131.
Park HJ, Byun MK, Rhee CK, Kim K, Kim HJ, Yoo KH. Significant predictors of medically diagnosed chronic obstructive pulmonary disease in patients with preserved ratio impaired spirometry: a 3-year cohort study. Respir Res. 2018;19:185.
Niimi A, Matsumoto H, Amitani R, Nakano Y, Mishima M, Minakuchi M, Nishimura K, Itoh H, Izumi T. Airway wall thickness in asthma assessed by computed tomography. Relation to clinical indices. Am J Respir Crit Care Med. 2000;162:1518–23.
Siroux V, Boudier A, Dolgopoloff M, Chanoine S, Bousquet J, Gormand F, Just J, Le Moual N, Nadif R, Pison C, et al. Forced midexpiratory flow between 25% and 75% of forced vital capacity is associated with long-term persistence of asthma and poor asthma outcomes. J Allergy Clin Immunol. 2016;137:1709-16.e1706.
Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, Crapo R, Enright P, van der Grinten CP, Gustafsson P, et al. Standardisation of spirometry. Eur Respir J. 2005;26:319–38.
Kwon DS, Choi YJ, Kim TH, Byun MK, Cho JH, Kim HJ, Park HJ. FEF(25–75%) Values in Patients with Normal Lung Function Can Predict the Development of Chronic Obstructive Pulmonary Disease. Int J Chron Obstruct Pulmon Dis. 2020;15:2913–21.
Bazzan E, Semenzato U, Turato G, Biondini D, Cubero P, Marin-Oto M, Forner M, Tinè M, Casara A, Baraldo S, et al. Symptomatic smokers without COPD have physiological changes heralding the development of COPD. ERJ Open Res. 2022;8:00202–2022.
Riley CM, Wenzel SE, Castro M, Erzurum SC, Chung KF, Fitzpatrick AM, Gaston B, Israel E, Moore WC, Bleecker ER, et al. Clinical Implications of Having Reduced Mid Forced Expiratory Flow Rates (FEF25-75), Independently of FEV1, in Adult Patients with Asthma. PLoS ONE. 2015;10:e0145476.
Han MK, Agusti A, Calverley PM, Celli BR, Criner G, Curtis JL, Fabbri LM, Goldin JG, Jones PW, Macnee W, et al. Chronic obstructive pulmonary disease phenotypes: the future of COPD. Am J Respir Crit Care Med. 2010;182:598–604.
Bhatt SP, Washko GR, Hoffman EA, Newell JD Jr, Bodduluri S, Diaz AA, Galban CJ, Silverman EK. San José Estépar R, Lynch DA: imaging advances in chronic obstructive pulmonary disease. Insights from the genetic epidemiology of chronic obstructive pulmonary disease (COPDGene) Study. Am J Respir Crit Care Med. 2019;199:286–301.
Buist AS, McBurnie MA, Vollmer WM, Gillespie S, Burney P, Mannino DM, Menezes AM, Sullivan SD, Lee TA, Weiss KB, et al. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet. 2007;370:741–50.
Wheaton AG, Liu Y, Croft JB, VanFrank B, Croxton TL, Punturieri A, Postow L, Greenlund KJ. Chronic Obstructive Pulmonary Disease and Smoking Status - United States, 2017. MMWR Morb Mortal Wkly Rep. 2019;68(24):533–8.
Graham BL, Steenbruggen I, Miller MR, Barjaktarevic IZ, Cooper BG, Hall GL, Hallstrand TS, Kaminsky DA, McCarthy K, McCormack MC, et al. Standardization of Spirometry 2019 Update. An official American thoracic society and European respiratory society technical statement. Am J Respir Crit Care Med. 2019;200:e70–88.
Marseglia GL, Cirillo I, Vizzaccaro A, Klersy C, Tosca MA, La Rosa M, Marseglia A, Licari A, Leone M, Ciprandi G. Role of forced expiratory flow at 25–75% as an early marker of small airways impairment in subjects with allergic rhinitis. Allergy Asthma Proc. 2007;28:74–8.
Stockley JA, Ismail AM, Hughes SM, Edgar R, Stockley RA, Sapey E. Maximal mid-expiratory flow detects early lung disease in α(1)-antitrypsin deficiency. Eur Respir J. 2017;49:1602055.
European guidelines on quality criteria for computed tomography. EUR 16262. http://www.drs.dk/guidelines/ct/quality/index.htm. Accessed February 9, 2022.
Bhatt SP, Bodduluri S, KizhakkePuliyakote AS, Oelsner EC, Nakhmani A, Lynch DA, Wilson CG, Fortis S, Kim V. Structural airway imaging metrics are differentially associated with persistent chronic bronchitis. Thorax. 2021;76:343–9.
Nakano Y, Wong JC, de Jong PA, Buzatu L, Nagao T, Coxson HO, Elliott WM, Hogg JC, Paré PD. The prediction of small airway dimensions using computed tomography. Am J Respir Crit Care Med. 2005;171:142–6.
Grydeland TB, Dirksen A, Coxson HO, Eagan TM, Thorsen E, Pillai SG, Sharma S, Eide GE, Gulsvik A, Bakke PS. Quantitative computed tomography measures of emphysema and airway wall thickness are related to respiratory symptoms. Am J Respir Crit Care Med. 2010;181:353–9.
Park HJ, Lee SM, Choe J, Lee SM, Kim N, Lee JS, Oh YM, Seo JB. Prediction of Treatment Response in Patients with Chronic Obstructive Pulmonary Disease by Determination of Airway Dimensions with Baseline Computed Tomography. Korean J Radiol. 2019;20:304–12.
Lynch DA, Austin JH, Hogg JC, Grenier PA, Kauczor HU, Bankier AA, Barr RG, Colby TV, Galvin JR, Gevenois PA, et al. CT-Definable Subtypes of Chronic Obstructive Pulmonary Disease: A Statement of the Fleischner Society. Radiology. 2015;277:192–205.
Qin S, Yu X, Ma Q, Lin L, Li Q, Liu H, Zhang L, Leng S, Han W. Quantitative CT Analysis of Small Airway Remodeling in Patients with Chronic Obstructive Pulmonary Disease by a New Image Post-Processing System. Int J Chron Obstruct Pulmon Dis. 2021;16:535–44.
Burgel PR. The role of small airways in obstructive airway diseases. Eur Respir Rev. 2011;20:23–33.
Galbán CJ, Han MK, Boes JL, Chughtai KA, Meyer CR, Johnson TD, Galbán S, Rehemtulla A, Kazerooni EA, Martinez FJ, Ross BD. Computed tomography-based biomarker provides unique signature for diagnosis of COPD phenotypes and disease progression. Nat Med. 2012;18:1711–5.
Jain N, Covar RA, Gleason MC, Newell JD Jr, Gelfand EW, Spahn JD. Quantitative computed tomography detects peripheral airway disease in asthmatic children. Pediatr Pulmonol. 2005;40:211–8.
Hersh CP, Washko GR, Estépar RS, Lutz S, Friedman PJ, Han MK, Hokanson JE, Judy PF, Lynch DA, Make BJ, et al. Paired inspiratory-expiratory chest CT scans to assess for small airways disease in COPD. Respir Res. 2013;14:42.
Pompe E, Galbán CJ, Ross BD, Koenderman L, Ten Hacken NH, Postma DS, van den Berge M, de Jong PA, Lammers JJ, Mohamed Hoesein FA. Parametric response mapping on chest computed tomography associates with clinical and functional parameters in chronic obstructive pulmonary disease. Respir Med. 2017;123:48–55.
Vasilescu DM, Martinez FJ, Marchetti N, Galbán CJ, Hatt C, Meldrum CA, Dass C, Tanabe N, Reddy RM, Lagstein A, et al. noninvasive imaging biomarker identifies small airway damage in severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2019;200:575–81.
Lu L, Peng J, Zhao N, Wu F, Tian H, Yang H, Deng Z, Wang Z, Xiao S, Wen X, et al. Discordant Spirometry and Impulse Oscillometry Assessments in the Diagnosis of Small Airway Dysfunction. Front Physiol. 2022;13:892448.
Arakawa H, Fujimoto K, Fukushima Y, Kaji Y. Thin-section CT imaging that correlates with pulmonary function tests in obstructive airway disease. Eur J Radiol. 2011;80(2):e157-163.
Ronish BE, Couper DJ, Barjaktarevic IZ, Cooper CB, Kanner RE, Pirozzi CS, Kim V, Wells JM, Han MK, Woodruff PG, et al. Forced Expiratory Flow at 25%-75% Links COPD Physiology to Emphysema and Disease Severity in the SPIROMICS Cohort. Chronic Obstr Pulm Dis. 2022;9:111–21.
Nambu A, Zach J, Schroeder J, Jin G, Kim SS, Kim YI, Schnell C, Bowler R, Lynch DA. Quantitative computed tomography measurements to evaluate airway disease in chronic obstructive pulmonary disease: Relationship to physiological measurements, clinical index and visual assessment of airway disease. Eur J Radiol. 2016;85(11):2144–51.
Nakano Y, Muro S, Sakai H, Hirai T, Chin K, Tsukino M, Nishimura K, Itoh H, Paré PD, Hogg JC, Mishima M. Computed tomographic measurements of airway dimensions and emphysema in smokers. Correlation with lung function. Am J Respir Crit Care Med. 2000;162:1102–8.
Thomson NC, Chaudhuri R, Spears M, Messow CM, MacNee W, Connell M, Murchison JT, Sproule M, McSharry C. Poor symptom control is associated with reduced CT scan segmental airway lumen area in smokers with asthma. Chest. 2015;147(3):735–44.
Naderi M, Sabour S. Diagnostic value of FeNO and MMEF for predicting cough variant asthma in chronic cough patients: methodological issues. J Asthma. 2021;58(6):791–2.
Ciprandi G, Cirillo I, Klersy C, Marseglia GL, Vizzaccaro A, Pallestrini E, Tosca M. Role of FEF25-75 as an early marker of bronchial impairment in patients with seasonal allergic rhinitis. Am J Rhinol. 2006;20(6):641–7.
Patterson GM, Wilson S, Whang JL, Harvey J, Agacki K, Patel H, Theodore J. Physiologic definitions of obliterative bronchiolitis in heart-lung and double lung transplantation: a comparison of the forced expiratory flow between 25% and 75% of the forced vital capacity and forced expiratory volume in one second. J Heart Lung Transplant. 1996;15(2):175–81.
Pelucchi A, Lomater C, Gerloni V, Foresi A, Fantini F, Marazzini L. Lung function and diffusing capacity for carbon monoxide in patients with juvenile chronic arthritis: effect of disease activity and low dose methotrexate therapy. Clin Exp Rheumatol. 1994;12(6):675–9.
van der Doef HP, Arets HG, Froeling SP, Westers P, Houwen RH. Gastric acid inhibition for fat malabsorption or gastroesophageal reflux disease in cystic fibrosis: longitudinal effect on bacterial colonization and pulmonary function. J Pediatr. 2009;155(5):629–33.
Su ZQ, Guan WJ, Li SY, Feng JX, Zhou ZQ, Chen Y, Zhong ML, Zhong NS. Evaluation of the Normal Airway Morphology Using Optical Coherence Tomography. Chest. 2019;156:915–25.
Acknowledgements
Not applicable.
Funding
This study was funded by National Natural Science Foundation of China61976238 (Ming Li) and Science and Technology Planning Project of Shanghai Science and Technology Commission (20Y11902900, 21Y11910500, 22Y11901200); Excellent Academic Leaders of Shanghai (2022XD042); Emerging Talent Program (XXRC2213); Leading Talent Program (LJRC2202) of Huadong hospital; Special clinical research and Shanghai “Rising Stars of Medical Talent” Youth Development Program “Outstanding Youth Medical Talents” sponsored by Shanghai Municipal Health Commission (20204Y029, 202140036, SHWJRS [2021]-99).
Author information
Authors and Affiliations
Contributions
Yuling Yang and Haiyan Ge contributed to study design, manuscript writing and data analysis. Jinjuan Lu contributed to data acquisition and analysis. Xuemei Huang and Kun Wang contributed to study design and data interpretation. Liang Jin contributed to data acquisition and interpretation. Ming Li and Lin Qi contributed to study design and manuscript revision. All authors have read and approved the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Huadong Hospital affiliated to Fudan University (approval number: 2021K018). Written informed consent was obtained from all participants. All methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yang, Y., Ge, H., Lu, J. et al. Structural features on quantitative chest computed tomography of patients with maximal mid-expiratory flow impairment in a normal lung function population. BMC Pulm Med 23, 86 (2023). https://doi.org/10.1186/s12890-023-02380-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-023-02380-0