
Abstract
Background
Human adenovirus (HAdV) is an important viral agent in children which can lead to severe acute respiratory infection (SARI). Reports on molecular epidemiology of HAdVs in Iran are limited. This case-control study is conducted to compare the HAdV infection rate and molecular epidemiology among two groups of children with and without respiratory symptoms in Tehran, Iran during 2018–2019.
Methods
Nested PCR was performed on 120 oropharyngeal swabs taken from children aged five and younger with SARI who were hospitalized as the case group, and 120 oropharyngeal swabs were collected from children of the same age without respiratory symptoms as the control group. For positive samples Sanger sequencing was done and a phylogenetic tree was drawn afterward.
Results
Out of 120 cases, 8 (6.6%) tested positive for eachHAdV types including 6 (75%) HAdV-B7, 1 (12.5%) HAdV-C2, and 1 (12.5%) HAdV-C6. Among the control group, out of 120 samples, 8 (6.6%) were positive comprising 5 (62.5%) HAdV-C5, 2 (25%) HAdV-F41, and 1 (12.5%) HAdV-C6.
Conclusion
The present study indicated a different viewpoint of HAdV molecular epidemiology in which the genotypes were compared in children with and without respiratory symptoms. HAdV prevalence was equally common in cases and controls but different genotypes were detected in these two groups. HAdV-B7 was the main type among children with SARI, dissimilar to children with no respiratory symptoms where HAdV-C5 was the predominant type. Detecting HAdV-F in oropharyngeal swabs was a rare finding, which requires further investigation.
Similar content being viewed by others


Introduction
Human adenoviruses (HAdVs) are non-enveloped double-stranded linear DNA viruses belonging to the family Adenoviridae and genus Mastadenovirus. HAdVs are classified into seven species (A to G) and more than 90 types, due to their genetic characteristics, tissue tropism, and clinical manifestations. HAdV species C (type 1, 2, 5, and 6) and B (type 3 and 7) are most commonly related to respiratory infections, followed by species E and D, while viruses in species F are assumed to cause gastrointestinal tract infections[1]. The predominant HAdV types detected in association with clinical presentation differ between different geographic regions and may shift over time according to the year of surveillance. HAdVs are crucial viral agents which have been linked to a variety of illnesses, including severe acute respiratory infection (SARI), gastroenteritis, conjunctivitis, hemorrhagic cystitis, hepatitis, myocarditis, nephritis, meningoencephalitis, and nosocomial infection [2]. SARIs (of any viruses) are considered to be serious threats in pediatric patients [2,3,4]. HAdVs as one of the causative agents of SARI can involve all ages, however, their infections occur more frequently in children younger than 5 years old [2]. It is worth mentioning that SARI etiology can be hard to establish due to the frequent detection of HAdV in asymptomatic children [5, 6]. HAdVs account for 5–10% of respiratory tract infections among children [3, 7]. Clinical manifestations of adenoviral respiratory disease may range from asymptomatic infection to fatal [1, 4]. The severity of clinical symptoms depends on the host’s age and immunocompetence status as well as the types of the virus [2, 8]. Almost 80% of HAdV infections in children are related to HAdV types 1 to 7 [9]. HAdV-B7 is highly correlated with severe respiratory infections and high mortality rate [9,10,11]. Since respiratory HAdVs prodominent types alter.
through the years in various countries, evaluation of molecular epidemiology is necessary to recognize the prevalence of circulating HAdVs types in a specific period.
This case-control study is conducted to estimate the HAdV infection rate and its molecular epidemiology in children aged five and younger with respiratory symptoms (as case group) and without respiratory symptoms (as control group) from December 2018 to December 2019.
Method
Study design and samples preparation
A total of 240 oropharyngeal specimens, collected from December 2018 to December 2019, were enrolled in this case-control study, including 120 oropharyngeal swabs from children aged five and younger hospitalized with SARI and referred to the National Influenza Center (NIC), all of which tested negative for influenza A and B viruses, and 120 oropharyngeal swabs which were collected from children with the same age group who had fever and rash due to MMR (Measles, Mumps and Rubella) vaccine and had no respiratory symptoms as the control group. All cases were individually matched to control by age. The presented study was approved by the Ethics Committee of Tehran University of Medical Sciences with the approval code IR.TUMS.SPH.REC.1398.162.
DNA extraction and PCR
DNA extraction was performed using the High Pure Viral Nucleic acid kit (Roche, Germany) according to the manufacturer’s instructions. Nested polymerase chain reaction (PCR) was performed on a hexon conserved region by applying specific primers including, ADH-01 (ACTACAAYATTGGCTACCAGG) and ADH-02 (CAAAACATAAAGAAGKGTGGGC) with 440bp PCR product for the first round and ADH-I1 (AACTTCCAGCCCATGAGCMG) and ADH-I2 (CTCAAAAGTCATGTCBAGCGC) with 330bp PCR product for the second round [12].
The first round of nested PCR was performed in a 50µl reaction. 10µl of extracted DNA was added to 40µl of the reaction mixture containing 5µl 10× PCR buffer,
20 mM MgSo4, 2.5 mM dNTP mixture, 2 units of Taq DNA polymerase (Biobasic, Canada) and 10 pmol of the ADH-01 and ADH-02 primers. The thermal cycling was carried out with the following program: initial denaturation at 94°C for 5min, followed by 40 cycles consisting of denaturation at 94°C for 30s, annealing at 50°C for 30s and extension at 72°C for 30s. The final elongation step was 72°C for 5mins. In the second round of PCR, 5µl of the primary PCR product was added to 45µl of the reaction mixture using ADH-I1 and ADH-I2 primers. The thermal protocol was the same as mentioned in the first round, apart from the annealing temperature which exceeded to 55°C. The final PCR products (330bp) were observed using 2% agarose gel electrophoresis and sequenced by Sanger sequencing in NIC laboratory using 3130 genetic analyzer (Applied Biosystems).
Phylogenetic analysis
The sequence reads were processed using BioEdit (v 7.0.5.3). The final sequences of each read were aligned by the BLAST Tool from NCBI. To draw a phylogenetic tree MEGA X was used based on the Neighbor-joining method, Tamura-Nei model, and bootstrap analyses by 1000 resampling of the datasets.
Statistical analysis
Statistical analyses were done using R version 4.0.3 and SPSS software 16.0 (SPSS Inc, Chicago, IL).
To compare differences between children with and without respiratory symptoms, we used the χ2 test, or McNemar’s exact test were appropriate. A two-sided α value of less than 0.05 was regarded as statistically significant.
Results
The specimens were oropharyngeal swabs from two groups of children aged five and younger with and without any respiratory symptoms as case and control groups, respectively. Each group was divided into 3 age groups: under 1, 1–3 and 4–5 years old. All cases in these two groups were individually matched by age. Hence, age distribution was almost identical in both groups comprising 56 (46.7%) under 1, 54 (45%) 1–3 and 10 (8.3%) 4–5 years old with a mean age of 1.05 years (SD = 1.38). Totally, out of 240 samples 16 (6.6%) were positive for HAdV by nested PCR including 8 (6.7%) positive in the patients and 8 (6.7%) positive in the control group. Out of all 120 individuals in the control group, 51 (42.5%) were female and 69 (57.5%) were male containing 4 (50%) positive females and 4(50%) positive males. 47 (39.1%) of 120 patients were female and 73 (60.9%) were male comprising 5 (62.5%) and 3 (37.5%) positive for HAdV respectively. In the control group, all positive samples belonged to the 1–3 years old age group (p-value = 0.02), while in the case group, out of 8 positive samples 5 (62.5%), 2 (25%) and 1 (12.5%) belonged to under 1, 1–3 and 4–5 years old age groups, respectively (Table1).
Sequencing was performed for all 16 positive samples. Five different HAdV types were identified indicating that HAdV-B7 was the predominant type, followed by HAdV-C5. By phylogenetic analysis (Fig.1) our strains in the control group matched with HAdV-C5 (62.5%), HAdV-F41 (25%) and HAdV-C6 (12.5%). Whereas, in the case group HAdV-B7 comprised 75% of positive cases (6/8, p-value = 0.02), followed by HAdV-C2 (12.5%,1/8) and HAdV-C6 (12.5%, 1/8) (Fig.2).

Phylogenetic tree was inferred by using the Neighbor joining method based on the Tamura-Nei model with 1000 bootstrap analyses. A region with 330 nucleotides length from HAdV hexon was sequenced. The accession numbers for reference strains are written next to their types and 16 strains identified in this study (GenBank accession numbers MW558248-MW558263) are marked with ♦

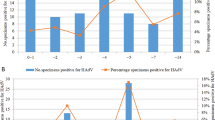
Comparison of adenovirus positive cases based on genotype in two groups: children with SARI(A) and without any respiratory symptoms (B)
The identity between Iranian HAdV strains and reference sequences of the same types is shown in Table2.
Discussion
In the present study, the detection rate and molecular epidemiology of HAdV in oropharyngeal swabs obtained from two groups of children aged five and younger with SARI and without any respiratory symptoms were investigated.
We report that, HAdV-DNA was identified in 8 patients (6.7%) and 8 control samples (6.7%). The predominant type in the case and control groups, were HAdV-B7 and HAdV-C5, respectively. It is known that HAdV-B7 is associated with severe diseases. Within the SARI patients, 56% were < 1 year and also five out of six HAdV-B7 positive cases were < 1 year. This actually indicates that < 1 age group is more important from the SARI point of view.
In a case-control study in Norway, adenoviral infections were detected in 6.1% of children with respiratory tract infections, whereas the control group’s detection rate was 10.5%. The most common types were HAdV-B3, HAdV-C2, and HAdV-C1[13]. Former studies in Iran showed that 14.4% [14], 18.4% [3] and 35.5% [2] of children with SARI were positive for HAdV. In the latter study, the most prevalent species among children with SARI was HAdV-B (80.3%), followed by HAdV-C (15.5%), HAdV-D (2.8%) and HAdV-E (1.4%). Besides, HAdV- B14/55 and HAdV-B3 were the predominant types [2]. Makvandi et al. detected HAdV-5 (86.3%) and HAdV-2 (13.7%) in children diagnosed with SARI [3]. In Egypt, the prevalence rate of HAdV in hospitalized pediatric patients was 35%, in which HAdV-B was the most common (76.2%), followed by HAdV-C (19%) and HAdV-E (4.8%) [15]. Various studies in China have reported different detection rates, for instance 3.72%, in which the common types were HAdV-C2, HAdV-B3, HAdV-B7 [16], 9.4% where the most prevalent type was HAdV-B7 (34%) [9] and another study with 13.3% HAdV prevalence in children with pneumonia which HAdV-B7 was the main serotype [17].
Some serotypes of HAdVs have been reported to be associated with more severe infections. A study in Taiwan has revealed an association between HAdV-B7 and severe pulmonary complications, respiratory failure, longer hospitalization, long-term pulmonary sequel, as well as intensive-care requirements even among children with no symptoms, in comparison to HAdV-C2 and HAdV-B3 [18]. As shown in some studies, the fatality rate of HAdV-B7 and HAdV-3 infections was higher rather than other types [9, 18,19,20,21,22]. Lai et al. showed that out of 45 severe HAdV infected cases 22 (49%) had HAdV-B7 and also 7 (70%) of fatal cases were due to HAdV-B7 which indicated the mortality rate of HAdV-B7 was 32%[23]. As it was reported by Na Zeng et al. HAdV-B7 infection triggers respiratory failure, severe pneumonia, toxic encephalopathy and lower white blood cell and platelets count. They noticed that in cell culture HAdV-B7 replicates more than HAdV-B3 and also induces aggravated cytokine response provoking severe inflammation in the respiratory tract [24].
In numerous studies, the HAdV detection rate in children with SARI has been reported 2–10% [13]. With a detection rate of 6.7%, our data was in agreement with most of the other studies. A noteworthy point is that HAdV detection in respiratory tracts does not necessarily imply that SARI is due to the presence of this virus. It could be a consequence of HAdV latency and sheddingfor a long time. Many studies have indicated that HAdV, specifically HAdV-C, can persist in the lymphocytes of tonsils and adenoids [25]. As mentioned, herein more HAdV-C cases were detected in the control group in comparison to the patients. This may be on the grounds that in the control group, where patients do not have respiratory symptoms, adenovirus-DNA presence in oropharyngeal swabs may be a result of a former infection rather than a recent one. Since we detected HAdV-B7 cases in the patients with SARI, contrary to the control group, this data was also consistent with other studies which indicated that HAdV-B7 leads to more severe conditions. It is noticeable that in this study, two cases of HAdV-F41, which is an enteric HAdV, were found in oropharyngeal swabs in the control group. Previously, in a study in Argentina, out of 26 positive HAdV respiratory samples 2 were identified as HAdV-F. The underlying reason for detecting HAdV-F in the respiratory tract has not been recognized yet. It is assumed that the respiratory tract could either be an entry or replication site for HAdV-F [26]. Further research is needed to justify this phenomenon.
As it is evident, HAdV prevalent types alter through the years in different countries. Thus, monitoring the molecular epidemiology of HAdV in different sites and over the years is of high importance.
This study has some limitations we need to highlight. Clinical data on the study subjects such as days of symptoms, clinical presentations, comorbidities, and socioeconomic status were not available. Besides, there was no access to follow-up data for the controls on developed respiratory symptoms after sampling.
Conclusion
To our knowledge, the present study is the only research which has raised a different viewpoint of HAdV molecular epidemiology where the genotypes were compared in children with and without respiratory symptoms. HAdV prevalence was equally common in cases and controls but different genotypes were detected in these two groups. HAdV-B, which has been associated with a more severe condition, was only identified in the case group. Continued surveillance may be helpful regarding control and treatment of adenoviral infections.
Data availability
The datasets collected and analyzed during this study are not publicly available due to the National Influenza Center policy but are available from the corresponding author on reasonable request.
Abbreviations
- HAdV:
-
Human adenovirus.
- SARI:
-
severe acute respiratory infection.
- NIC:
-
National Influenza Center.
- PCR:
-
polymerase chain reaction.
References
Kosulin K. Intestinal HAdV Infection: Tissue Specificity, Persistence, and Implications for Antiviral Therapy. Viruses 2019, 11(9).
Shafiei-Jandaghi N-Z, Yavarian J, Malekshahi SS, Naseri M, Shadab A, Ghavami N, Mokhtari-Azad T. Identification of adenovirus species in Iranian pediatric population with severe acute respiratory infections. Future Virol. 2019;14(9):577–83.
Ghasemi Y, Makvandi M, Samarbafzadeh AR, Nejati A, Najafifard S, Neisi N, Rasti M, Ahmadi K, Shamsizadeh A, Nikfar R. Serotype determination of adenoviruses in children with respiratory infection. Indian J Pediatr. 2014;81(7):639–43.
Ogunbayo AE, Mogotsi MT, Sondlane H, Nkwadipo KR, Sabiu S, Nyaga MM. Pathogen Profile of Children Hospitalised with Severe Acute Respiratory Infections during COVID-19 Pandemic in the Free State Province, South Africa. Int J Environ Res Public Health 2022, 19(16).
Rhedin S, Lindstrand A, Rotzén-Östlund M, Tolfvenstam T, Ohrmalm L, Rinder MR, Zweygberg-Wirgart B, Ortqvist A, Henriques-Normark B, Broliden K, et al. Clinical utility of PCR for common viruses in acute respiratory illness. Pediatrics. 2014;133(3):e538–45.
O’Brien KL, Baggett HC, Brooks WA, Feikin DR, Hammitt LL, Higdon MM, Howie SRC, Deloria Knoll M, Kotloff KL, Levine OS, et al. Causes of severe pneumonia requiring hospital admission in children without HIV infection from Africa and Asia: the PERCH multi-country case-control study. The Lancet (British edition). 2019;394(10200):757–79.
Williams BG, Gouws E, Boschi-Pinto C, Bryce J, Dye C. Estimates of world-wide distribution of child deaths from acute respiratory infections. Lancet Infect Dis. 2002;2(1):25–32.
Akhil C, Suresha PG, Sabeena S, Hindol M, Arunkumar G. Genotyping of human adenoviruses circulating in Southwest India. Virusdisease. 2016;27(3):266–70.
Xie L, Zhang B, Xiao N, Zhang F, Zhao X, Liu Q, Xie Z, Gao H, Duan Z, Zhong L. Epidemiology of human adenovirus infection in children hospitalized with lower respiratory tract infections in Hunan, China. J Med Virol. 2019;91(3):392–400.
Barnadas C, Schmidt DJ, Fischer TK, Fonager J. Molecular epidemiology of human adenovirus infections in Denmark, 2011–2016. J Clin Virol. 2018;104:16–22.
Callaway Z, Kim SH, Kim JY, Kim DW, Kim C-K. Adenovirus infection with serious pulmonary sequelae in Korean children. Clin Respir J. 2011;5(2):92–8.
Colaizy TT, Morris CD, Lapidus J, Sklar RS, Pillers DA. Detection of ureaplasma DNA in endotracheal samples is associated with bronchopulmonary dysplasia after adjustment for multiple risk factors. Pediatr Res. 2007;61(5 Pt 1):578–83.
Schjelderup Nilsen H-J, Nordbø SA, Krokstad S, Døllner H, Christensen A. Human adenovirus in nasopharyngeal and blood samples from children with and without respiratory tract infections. J Clin Virol. 2019;111:19–23.
Shatizadeh Malekshahi S, Shafiei-Jandaghi NZ, Yavarian J, Shadab A, Naseri M, Mokhtari Azad T. Detection of Respiratory Co-Infections in Children Less Than Five Years With Adenovirus Infection. Arch Pediatr Infect Dis. 2017;5(1):e36953.
Abd-Jamil J, Teoh B-T, Hassan EH, Roslan N, AbuBakar S. Molecular identification of adenovirus causing respiratory tract infection in pediatric patients at the University of Malaya Medical Center. BMC Pediatr. 2010;10(1):46.
Zhao MC, Guo YH, Qiu FZ, Wang L, Yang S, Feng ZS, Li GX. Molecular and clinical characterization of human adenovirus associated with acute respiratory tract infection in hospitalized children. J Clin Virol. 2020;123:104254.
Xie L, Zhang B, Zhou J, Huang H, Zeng S, Liu Q, Xie Z, Gao H, Duan Z, Zhong L. Human adenovirus load in respiratory tract secretions are predictors for disease severity in children with human adenovirus pneumonia. Virol J. 2018;15(1):123.
Lin MR, Yang SL, Gong YN, Kuo CC, Chiu CH, Chen CJ, Hsieh YC, Kuo CY, Fang CW, Tsao KC, et al. Clinical and molecular features of adenovirus type 2, 3, and 7 infections in children in an outbreak in Taiwan, 2011. Clin Microbiol Infect. 2017;23(2):110–6.
Li QG, Zheng QJ, Liu YH, Wadell G. Molecular epidemiology of adenovirus types 3 and 7 isolated from children with pneumonia in Beijing. J Med Virol. 1996;49(3):170–7.
Zhang ZJ, Wang ZL, Cao YP, Zhu ZH, Liu YL, Lin LM, Gao X. Acute respiratory infections in childhood in Beijing: An etiological study of pneumonia and bronchiolitis. Chin Med J (Engl). 1986;99(9):695–702.
Tang L, Wang L, Tan X, Xu W. Adenovirus serotype 7 associated with a severe lower respiratory tract disease outbreak in infants in Shaanxi Province, China. Virol J. 2011;8(1):23.
Ning G, Wang X, Wu D, Yin Z, Li Y, Wang H, Yang W. The etiology of community-acquired pneumonia among children under 5 years of age in mainland China, 2001–2015: A systematic review. Hum Vaccin Immunother. 2017;13(11):2742–50.
Lai CY, Lee CJ, Lu CY, Lee PI, Shao PL, Wu ET, Wang CC, Tan BF, Chang HY, Hsia SH, et al: Adenovirus serotype 3 and 7 infection with acute respiratory failure in children in Taiwan, 2010–2011. PloS one 2013, 8(1):e53614.
Fu Y, Tang Z, Ye Z, Mo S, Tian X, Ni K, Ren L, Liu E, Zang N. Human adenovirus type 7 infection causes a more severe disease than type 3. BMC Infect Dis. 2019;19(1):36.
Proenca-Modena JL, de Souza Cardoso R, Criado MF, Milanez GP, de Souza WM, Parise PL, Bertol JW, de Jesus BLS, Prates MCM, Silva ML, et al. Human adenovirus replication and persistence in hypertrophic adenoids and palatine tonsils in children. J Med Virol. 2019;91(7):1250–62.
Echavarria M, Maldonado D, Elbert G, Videla C, Rappaport R, Carballal G. Use of PCR to demonstrate presence of adenovirus species B, C, or F as well as coinfection with two adenovirus species in children with flu-like symptoms. J Clin Microbiol. 2006;44(2):625–7.
Acknowledgements
We express our thanks to our colleagues in NIC, Virology Department, School of Public Health, Tehran University of Medical Sciences. This study was supported by Tehran University of Medical Sciences.
Funding
This work was funded and supported by Tehran University of Medical Sciences (Grant No. 1400-1-99-52579).
Author information
Authors and Affiliations
Contributions
SZ, ZH, KS contributed in tests performing, NGH and SZ performed the extraction, JY, SSM and AN contributed in reviewing the paper critically, the comments were included. NZ-SJ and SZ contributed in drafting the manuscript. TMA and NZ-SJ designed and supervised the study. All authors have approved the final version of the article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Tehran University of Medical Sciences with the approval code IR.TUMS.SPH.REC.1398.162. All methods were performed in accordance with the relevant guidelines and regulations. All specimens included in this study were collected by Iran Ministry of Health for national influenza surveillance. No extra sample was collected for this study. We sought permission from Tehran University of Medical Sciences (TUMS) review board for using the samples and informed consent is exempted.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zadheidar, S., Yavarian, J., Heydarifard, Z. et al. Molecular epidemiology of human adenoviruses in children with and without respiratory symptoms: Preliminary findings from a case-control study. BMC Pediatr 22, 583 (2022). https://doi.org/10.1186/s12887-022-03625-3
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-022-03625-3