
Abstract
Biological therapies have revolutionized the treatment of disease across a number of therapeutic areas including retinal diseases. However, on occasion, such treatments may be relatively more expensive compared to small molecule therapies. This can restrict patient access and treatment length leading to suboptimal clinical outcomes. Several biosimilar candidates of ranibizumab and aflibercept are currently in development and the first biosimilar of ranibizumab received EMA approval in August and FDA approval in September 2021. Biosimilars are biological medicines that are highly similar to an already-approved biological medicine (reference product). The physicochemical and clinical similarity of a biosimilar is determined by a rigorous analytical and clinical program, including extensive pharmacokinetic and pharmacodynamic analysis with phase III equivalence studies where appropriate. These phase III studies are carried out in a patient population that is representative of all of the potential approved therapeutic indications of the originator product and the most sensitive for detecting potential differences between the biosimilar and the reference product. Biosimilars have been used successfully across a wide range of therapeutic areas for the past 15 years where they have achieved substantial cost savings that can be reinvested into healthcare systems without affecting the quality of patient care. The current review provides an introduction to biosimilars with the aim of preparing retinal specialists for discussing these products with their patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Anti-VEGFs are highly effective within retinal diseases but cost can potentially limit the intensity or length of therapy and thereby provide suboptimal clinical outcomes. |
Biosimilar candidates of ranibizumab and aflibercept are currently in development for the treatment of retinal diseases and some have received regulatory approval. |
The physicochemical and clinical similarity of a biosimilar to its reference is determined by a rigorous analytical and clinical program including phase III equivalence studies where appropriate. |
Biosimilars may optimize clinical outcomes while providing substantial cost savings that can be reinvested into healthcare systems. |
The current review provides an introduction to biosimilars with the aim of preparing retinal specialists for discussing these products with their patients. |
Introduction
The introduction of recombinant biological therapies has transformed treatment across a wide range of therapeutic areas including oncology, endocrinology, immune-mediated inflammatory disorders, kidney disease, and supportive care [1,2,3,4,5,6]. Biological therapies have also significantly improved outcomes in the treatment of neovascular retinal disorders [7], where recombinant proteins targeting vascular endothelial growth factors (VEGFs) are now considered first-line treatment options [8].
While undoubtedly effective, biologics are associated with high costs driven by the expense of their development [9, 10]. These high costs can lead to clinical unmet needs such as delayed treatment access or worsening disease activity in patients with rheumatoid arthritis (RA) [11, 12], restriction of treatment to those patients with RA who have severe disease [13, 14], and potentially premature cessation of therapy in patients with psoriasis or psoriatic arthritis [15].
Biosimilars are biological medicines that are highly similar to, and have no clinically meaningful differences from, an already-approved biological medicine (reference product) that may provide patient access at a reduced cost [16]. They have become established treatment options for diseases such as RA, psoriasis, cancer, and inflammatory bowel disease [17,18,19], and there are 82 biosimilars currently approved in the EU and 29 in the USA (Fig. 1; [20, 21]). Biosimilars have been shown to provide cost savings across therapeutic areas and at all levels of the healthcare system and such cost savings can be used to treat more patients and or invested in clinical services to improve patient care [22].

Key biosimilar legislation and guidance development and biosimilar cumulative approvals in the EU and USA
Biosimilars have recently entered the ophthalmology field for the treatment of neovascular retinal diseases and are expected to lead to reductions in expenditures on anti-VEGF treatments [23, 24]. While some retinal specialists may have gained experience in using biosimilars when treating non-infectious uveitis with biosimilar adalimumab, not all clinicians may be familiar with these products [25,26,27,28].
This review aims to provide an introduction to biosimilars for retinal specialists: how they are developed; their regulatory approval pathway; and how they can best be leveraged to optimize the management of neovascular retinal diseases in clinical practice. Experience from other therapeutic areas has shown that comprehensive, relatable, and timely education on biosimilars, in addition to clinical experience, is critical to their widespread and well-informed adoption [29]. The article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
What Role May Biosimilars Play in the Ophthalmology Space?
Of an estimated global drug budget of US $1 trillion in 2018, innovative biologics accounted for 29% (US $296 billion [30]). In ophthalmology alone, the annual Medicare drug costs for ranibizumab averaged $1.3 billion between 2011 and 2015, and the costs of aflibercept averaged $1.4 billion between 2013 and 2015. Combined, ranibizumab and aflibercept accounted for 12% of the Medicare Part B budget annually [31]. In attempts to reduce the cost of, and increase access to, anti-VEGFs within neovascular retinal diseases, physicians have turned to using off-label bevacizumab (it is currently indicated for solid tumors only [32]). Bevacizumab appears generally non-inferior to ranibizumab and aflibercept in neovascular age-related macular degeneration (nAMD) and diabetic macular edema (DME), although a recent trial in retinal vein occlusion (RVO) could not conclude that bevacizumab was non-inferior to aflibercept [33,34,35,36]. Also, ziv-aflibercept, an anti-VEGF drug approved for treating colorectal cancer, has been investigated as a treatment for nAMD [37], despite the fact that in the EU intravitreal use of ziv-aflibercept is contraindicated because of its hyperosmotic properties [38]. In addition to their off-label-driven limitations, both products require additional compounding prior to use in retinal diseases, which may increase the risk of intraocular infections [39,40,41,42].
High acquisition costs and consequent access restriction can lead to potential vision complications or vision loss in vulnerable ophthalmology patient groups [43] and across all socioeconomic situations. In the LUMINOUS study, a global real-world study on treatment practices for ranibizumab in nAMD, 72.9% of patients received six or fewer injections in the first year and 35.5% of patients received three or fewer. The same study demonstrated that treatment outcomes correlated to the number of injections given, such that the greater the number of injections given, on average, the better the visual outcome [44]. The authors suggested that undertreatment may be linked to several factors including reimbursement of treatment, limited medical insurance coverage, and limited access to treatment and high treatment cost. In the USA the presence of a co-pay decreased the odds of patients with DME receiving anti-VEGF therapy (by 40%) and also decreased the odds of the patient following up (by 37%) [45]. In another study from Australia, lower out-of-pocket costs were associated with higher adherence and compliance rates for anti-VEGF therapy in patients with AMD or DME [46]. Treatment costs may have an even greater impact in low- and middle-income countries. A single-center, retrospective review of 648 patients with retinal diseases from India showed that over half of patients were lost to follow-up. The most common reason given was unaffordability (41%) with the proportion of patients stating this increasing with the number of treatment injections given [47]. Undoubtedly, there is a need to provide more affordable and cost-effective anti-VEGF treatments for neovascular retinal diseases globally.
The introduction of biosimilars has been shown to reduce costs across a range of therapeutic areas. Table 1 provides an overview of some modelling and real-life studies showing the cost savings possible through the use of biosimilars within rheumatology, gastroenterology, dermatology, oncology, and supportive care. These savings increased when biosimilars were used for longer and over a larger number of patients. The majority of studies also calculated that these cost savings could result in tens of thousands of additional patients being treated with biologics, which could increase substantially should the benefits of biosimilars be available more widely. There is no reason to believe that biosimilars could not have a similar effect with ophthalmology.
Regulation, Development, and Approval of Biosimilars
The evolution of biosimilars within the EU began in 2004 when Directive 2004/27/EC provided legal basis for the definition of what biosimilars are, followed by the development of guidelines covering overarching principles, quality attributes, non-clinical/clinical requirements, and product-class specific items (Fig. 2). Biosimilars are different from generics in that generic versions of simple, chemically synthesized compounds are created by predictable chemical processes whereas biosimilars are manufactured using complex processes using living cell lines and require a comprehensive approval process [16]. For biosimilars, the development time is significantly longer, the development costs are significantly higher, and the manufacturing process requires a higher level of expertise compared with that needed for generic compounds [48]. A typical small molecule generic drug will take 3–5 years to develop and costs $1–5 million, while a biosimilar may take around 8 years and costs $100–200 million to develop. In comparison, a novel originator biologic takes 12 years or more to develop with costs in excess of £1 billion [49, 50].
In order to gain regulatory approval, biosimilars are required to demonstrate a high degree of similarity to the originator molecule in terms of quality characteristics, biological activity, safety and efficacy, based on a comprehensive comparability exercise [51,52,53,54]. The foundation of the biosimilarity exercise is a thorough side-by-side analysis of the quality attributes of the biosimilar and its reference product [55]. The techniques used to analyze quality characteristics have improved continually over the past decade in terms of accuracy and sensitivity which allows biosimilar manufacturers detect and characterize differences between two products with high degrees of certainty [56, 57]. Several complementary methods are used to determine the quality “fingerprint” of a biosimilar with an emphasis of so-called critical product quality attributes (CQAs), which are the chemical, physical, biological, and microbiological characteristics that can be defined, measured, and continually monitored to ensure that the final product outputs remain within acceptable limits of quality (Fig. 2) [58, 59]. Minor structural differences between the biosimilar and the reference biologic may be present as long as these have no clinically relevant impact. Such differences occur commonly for originator biologics and are inherent to manufacturing in biological expression systems, and may also be affected by changes to their manufacturing process, such as cell line/cell culture media, or equipment changes [60]. Regulators have a great deal of experience in dealing with such manufacturing changes, which are considered acceptable as long as it can be supported that the changes do not impact the efficacy or safety of the product. The definition of biosimilars applied here excludes molecules that are available in certain regulatory regions outside the EU and USA but were not approved following a stringent regulatory approval process—so-called intended copies or nonregulated biologics [61] (Table 1, Supplementary Material).

Methods used to determine the quality attribute “fingerprint” of the biosimilar
Totality of Evidence
For biosimilars the focus for approval is on the totality of evidence generated through a comprehensive and complex comparability exercise using a stepwise approach. The aim is not to re-establish a product’s efficacy/safety profile but to demonstrate similarity to the originator product for which a benefit–risk profile has already been established. The first step is to establish similarity in terms of quality (physicochemical and biological), the second is a pharmacological comparison (non-clinical comparability), and the final step is clinical comparability (clinical trials [58]). As shown in Fig. 3 [62], most of the regulatory emphasis with biosimilars is placed on the first (analytical) step or proving that the biosimilar is chemically, structurally, and biologically highly similar to the originator molecule. Only if these conditions are met will the biosimilar be taken to the next level of scrutiny in studies involving humans. In most cases, this starts with a determination of the pharmacokinetic (PK) profile. Of note, biosimilar candidate products for the treatment of retinal vascular diseases have not undergone phase I studies because of the limited relevance of systemic pharmacokinetics/pharmacodynamics resulting from intravitreal administration. For products where accepted pharmacodynamic markers exist, biosimilars may be approved on the basis of combined pharmacokinetic/pharmacodynamic studies, e.g., blood glucose concentrations in clamp studies for insulins, absolute neutrophil counts for granulocyte-colony stimulating factor, or serum calcium levels for teriparatide. However, for many products, including most monoclonal antibodies, such pharmacodynamic markers do not exist and well-designed, adequately powered phase III studies are required to confirm similarity to the reference product in terms of clinical efficacy and safety, usually involving several hundreds of patients [62, 63]. These trials are designed to exclude clinically meaningful differences in efficacy, safety, and immunogenicity and are performed in a patient population that is representative of approved therapeutic indications of the reference product and that will be sensitive for detecting potential differences between the biosimilar and the reference [64]. Typically, an equivalence design with symmetric inferiority and superiority margins is used [53].

Comparison of the development pathways for reference biologics and biosimilars
(Reproduced from Future Oncol. (2021) 17(19), 2529–2544 with permission of Future Medicine Ltd.) [65]
As for all biological products, manufacturers of biosimilars are required to provide regulatory authorities with robust post-approval risk management plans and pharmacovigilance programs to identify, characterize, and minimize a medicine’s important risks when used in wider patient populations [66].
Immunogenicity
A key consideration when developing any biological drug, including biosimilars, is their potential to elicit the formation of anti-drug antibodies (ADAs), i.e., their immunogenicity. Recent published evidence of rare, but severe, cases of intraocular inflammation after intravitreal injection of brolucizumab have sensitized the ophthalmology community to this topic [67, 68]. Whether a biological elicits ADAs depends on a number of product, patient, and clinical factors [69, 70]. The impact of ADAs can range from having no clinical effect to reducing a drug’s effect by interfering with its ability to bind its target, or increase the clearance of the drug from circulation, or in some cases eliciting hypersensitivity reactions [71, 72]. Animal models are not predictive for immunogenic responses in humans; therefore potential differences in immunogenicity between a biosimilar and its reference product can only be determined by performing clinical studies. An assessment of comparative immunogenicity is a regulatory expectation in all clinical studies involving biosimilars. Table 2 presents data from various studies comparing biosimilars to their reference products across different therapeutic areas. It should be noted that the sensitivity of ADA assays has greatly increased in the past decade, which means that levels of ADAs reported in more recent studies, including those comparing biosimilars, are often higher than earlier studies involving the same comparators [73]. As different assays use different methodologies and apply different cutoff limits for positivity, care should be taken when comparing ADA results from different studies. For currently authorized products in the EU and USA across several therapeutic areas, the rate of immunogenicity was found to be similar between biosimilars and their reference products [74].
Extrapolation
Extrapolation refers to the regulatory process of granting a clinical indication that is approved for the reference biologic to a biosimilar without providing clinical efficacy and safety data from within that indication [75, 76]. Usually, a biosimilar will be tested in a phase III clinical trial involving a study population that is representative of all of the potential approved therapeutic indications of the originator product, but also sensitive for detecting subtle differences (e.g., immunogenicity) that may impact on clinical practice [64]. For example, SB5, a biosimilar version of adalimumab, was approved on the basis of a clinical trial involving patients with RA, as this was the patient population deemed the most sensitive. SB5 was also approved for the other indications approved for the reference product including juvenile idiopathic arthritis, axial spondyloarthritis, psoriatic arthritis, psoriasis, pediatric plaque psoriasis, Crohn’s disease (including pediatric), ulcerative colitis, uveitis (including pediatric), and hidradenitis suppurativa [77]. The scientific rationale for extrapolation is based on a demonstration that the reference and biosimilar products have the same mechanism of action [78]. Both the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) state that if the totality of evidence in the biosimilar application supports a demonstration of biosimilarity for at least one of the reference product’s indications, it is possible for the biosimilar manufacturer to use these data and information to scientifically justify approval for other indications that were not directly studied by the biosimilar manufacturer (FDA, Biosimilar product regulatory review and approval [76]). Scientific justification can be based on existing literature, or by additional in vitro data supporting similarity across indications. Extrapolation is also applied following major changes in the manufacturing process of reference biologicals. The manufacturer follows regulatory guidance to conduct a comprehensive comparability program to establish that any pre- and post-manufacturing changes are sufficiently similar to allow continued authorization [76]. Therefore, currently marketed biologic molecules are, in a way, biosimilars of themselves at the time of their first approval.
Interchangeability
A source of confusion when discussing biosimilars remains around the theme of “interchangeability”, which is complicated by different meanings in different jurisdictions. Interchangeability refers to the exchanging of one medicine with another one that is expected to have the same clinical effects owing to high levels of similarity. Switching refers to interchanging an originator or biosimilar for a different biosimilar with the agreement of the prescriber, whereas (automatic) substitution occurs at the level of the pharmacist without consulting the prescriber [79]. In the EU, interchangeability is mostly a scientific term. The EMA does not address interchangeability directly and leaves these decisions to individual member states and automatic substitution of biosimilars is not practised in most EU countries. In the USA “interchangeable” is a legal designation allowing pharmacists to substitute biosimilars (if so permitted by state laws [80]) and it requires additional clinical evidence. In July 2021 the FDA approved the first interchangeable biosimilar product, insulin glargine-yfgn, a biosimilar of insulin glargine [81, 82]. Both biosimilars and interchangeable products have to adhere to the same standards of similarity. The view that biosimilars and originator products will not differ in their clinical effects is supported by published clinical studies and post-marketing surveillance data [79]. Indeed, systematic literature reviews conclude that the current body of evidence suggests no clinically relevant impact of initiating or switching to biosimilars across a number of therapeutic areas [74, 83, 84]. However, interchangeability may impede pharmacovigilance and traceability as not all jurisdictions require innovators and biosimilars to have distinct biological names [85].
The Biosimilars Pipeline in Ophthalmology
Several biosimilar candidates of ranibizumab and aflibercept are currently in development and the first biosimilar ranibizumab was recently approved by the FDA and the EMA (Table 3).
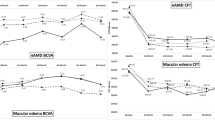
The initial results from the randomized, double-blind, phase III trial of SB11 (Samsung Bioepis, South Korea) in nAMD were recently published [100]. A total of 705 patients with nAMD were randomized 1:1 to receive SB11 or reference ranibizumab (both 0.5 mg Q4W) until week 48 with the last assessment at 52 weeks. Two primary endpoints were defined to satisfy different regulatory agencies: central subfield thickness (CST) at week 4 (EMA endpoint) and best corrected visual acuity (BCVA) at week 8 (FDA/Korean MFDS endpoint). The difference in CST at week 4 was − 8.4 (95% CI − 19.4 to 2.7) with changes in CST of − 108 and − 100 μm for SB11 and reference ranibizumab, respectively. The difference in BCVA at week 8 was − 0.8 (90% CI − 1.8 to 0.2) with changes in BCVA of + 6.2 and + 7.0 letters for SB11 and reference ranibizumab, respectively. SB11 was concluded to be non-inferior to reference ranibizumab for the prespecified primary endpoints. The secondary endpoints of safety, immunogenicity, and pharmacokinetics were similar between SB11 and reference ranibizumab. At week 52 the differences in BCVA (− 0.6, 90% CI − 2.1 to 0.9) and CST (− 14.9, 95% CI − 25.3 to − 4.5) were maintained, as were other secondary endpoints and safety criteria [101]. On the basis of these data, SB11 was approved by the EMA in August and the FDA in September 2021. Extrapolation of SB11 from nAMD to other indications may not be as contentious as for biosimilars in other therapeutic areas given that its mechanism of action is determined by binding of VEGFA across all authorized indications, it has generally low immunogenicity [100], is similar to reference ranibizumab with respect to structural, physicochemical, and biological properties [100], and has a non-glycosylated antibody fragment [102]. The European Public Assessment Report (EPAR) from the EMA states that “extrapolation to all approved indications of Lucentis applied for is supported” [103] and so in Europe SB11 is licensed for nAMD, proliferative diabetic retinopathy (DR), DME, macular edema associated with RVO, and choroidal neovascularization. The formulation of SB11 contains the same excipients in the same quantities as the reference product [103]. The FDA approved all indications with the labeled recommended dose of 0.5 mg (0.05 mL) including AMD, RVO and choroidal neovascularization. DR and DME were excluded [88] as the 0.3 mg (0.05 mL) presentation used for DR and DME was not available at the time of approval.
In its phase III trial within the nAMD population (COLUMBUS-AMD, N = 477) FYB201 (0.5 mg Q4W) (Formycon AG/Bioeq, Germany) was found to be equivalent to reference ranibizumab (0.5 mg Q4W) with respect to BCVA following 8 weeks of treatment, the primary endpoint. In the US-relevant population (baseline BCVA between 20/32 and 20/100 Snellen equivalent) investigators observed a mean change from baseline BCVA of + 5.1 vs + 5.6 letters on the Early Treatment Diabetic Retinopathy Study (ETDRS) test (difference − 0.4, 90% CI − 1.6 to 0.9) for patients treated with FYB201 or reference ranibizumab, respectively, meaning that the two treatments were equivalent. The difference in CST at week 48 was 3.68 μm (90% CI − 13.28 to 20.63 μm) from baseline CST of 182.9 μm and 190.8 μm for FYB201 and reference ranibizumab, respectively. There were no safety or immunogenicity concerns and outcomes did not differ between treatments [104].
Practical Guide for the Use of Biosimilars
Achieving the full cost-saving benefits of biosimilars requires patients currently receiving the reference product to switch to a biosimilar. The key question for patients and prescribers alike is will switching have any untoward effects such as loss of disease control, increased rates of adverse events, or more pronounced immunogenicity? A large number of studies have provided reassurance that switching from reference biologics to biosimilars is effective and safe [26, 74, 105,106,107,108,109,110,111].
In those therapeutic areas where biosimilars have been available for a number of years, it is apparent that the quality of physician–patient communication can have a large impact on the success of a biosimilar switch, and particularly on a phenomenon known as the nocebo effect. The nocebo effect is the opposite to the placebo effect, being defined as “a negative effect of a pharmacological or non-pharmacological medical treatment that is induced by patients’ expectations, and that is unrelated to the physiological action of the treatment” [112]. The nocebo effect may come into play when patients are switched from a reference biological to a biosimilar, and may be triggered by perceptions of biosimilars as “cheap copies” of branded medicines. It can have a number of potential consequences including increased symptom burden, psychological distress, and the number of adverse events experienced by patients; non-adherence, reduced quality of life, and wasted medication; increased healthcare costs; more complicated treatment regimens; and the cost savings from biosimilars not being realized [113,114,115,116,117]. The effects of the nocebo effect can be mitigated through physicians having a better understanding of biosimilars including how they are approved and passing this increased confidence onto their patients. In addition, better physician and patient education and communication, finding a balance between communicating important clinical information and counselling on safety profile expectations, and using educational strategies such as leaflets and patient video clips to recount treatment experiences could help to prevent the nocebo response [118,119,120,121,122,123,124]. However, a large systematic review of double-blind versus open-label studies of switching from an originator product to a biosimilar across several therapeutic areas noted that current evidence is insufficient to confirm a biosimilar nocebo effect, although there was some evidence to support the theory [125]. Even though open-label studies did show a decrease in persistence versus clinical trials, this was not associated with a decrease in efficacy [74].
Some physicians may query why they should use biosimilars when payers will reimburse reference products, or when bevacizumab or ziv-aflibercept is available to them. The fact that the use of both bevacizumab and ziv-aflibercept in ophthalmology is off-label, together with concerns regarding inflammation and infection following intravitreal administration of both products, may create a sense of uncertainty with prescribers [39,40,41,42, 126]. Furthermore, the use of bevacizumab is not available in all countries, or even uniformly within countries, reflecting diverging opinions of governments and clinical societies on its use [127]. With ziv-aflibercept there are also concerns over potential retinal damage caused by its hyperosmotic solution [38, 126], with its ophthalmic use in the EU being contraindicated for that reason. Finally, while the questioning of the use of biosimilars might be reasonable on an individual level, the reinvestment of savings provided by biosimilars on institutional, regional, and national levels (Table 1) can be used to improve patient care by treating more patients without increasing cost. Other potential benefits of the savings resulting from the use of biosimilars include taking on more staff to increase capacity, or investing in training and education for staff and patients around the subject of biosimilars [22, 51].
Conclusions
High-quality biosimilars may soon reach the field of ophthalmology and hold the promise of reducing drug expenditures and improving access to high-quality biologics. A growing amount of evidence from clinical trials and real-world studies from multiple therapeutic areas has failed to find clinically relevant differences between biosimilars and their originator products in terms of efficacy, safety, and immunogenicity. Furthermore, the benefits of biosimilars go beyond that of mere cost savings for healthcare systems. The acceptance and use of biosimilars can increase patients’ access to biological therapies, increase the number of healthcare providers available to treat patients via redeployment of savings, shift the recommendation of biological therapy earlier in treatment algorithms and guidelines, and fuel innovation in the development of new treatments. All of these will undoubtedly improve outcomes for patients and healthcare systems alike.
References
Brogden RN, Heel RC. Human insulin. A review of its biological activity, pharmacokinetics and therapeutic use. Drugs. 1987;34(3):350–71.
Cote-Daigneault J, Bouin M, Lahaie R, Colombel JF, Poitras P. Biologics in inflammatory bowel disease: what are the data? United Eur Gastroenterol J. 2015;3(5):419–28.
Faulds D, Sorkin EM. Epoetin (recombinant human erythropoietin). A review of its pharmacodynamic and pharmacokinetic properties and therapeutic potential in anaemia and the stimulation of erythropoiesis. Drugs. 1989;38(6):863–99.
Mao EJ, Hazlewood GS, Kaplan GG, Peyrin-Biroulet L, Ananthakrishnan AN. Systematic review with meta-analysis: comparative efficacy of immunosuppressants and biologics for reducing hospitalisation and surgery in Crohn’s disease and ulcerative colitis. Aliment Pharmacol Ther. 2017;45(1):3–13.
Maximiano S, Magalhaes P, Guerreiro MP, Morgado M. Trastuzumab in the treatment of breast cancer. BioDrugs. 2016;30(2):75–86.
Renwick W, Pettengell R, Green M. Use of filgrastim and pegfilgrastim to support delivery of chemotherapy: twenty years of clinical experience. BioDrugs. 2009;23(3):175–86.
Blick SK, Keating GM, Wagstaff AJ. Ranibizumab. Drugs. 2007;67(8):1199–206 (discussion 207–9).
Flaxel CJ, Adelman RA, Bailey ST, et al. Age-related macular degeneration Preferred Practice Pattern®. Ophthalmology. 2020;127(1):P1–65.
Pillai N, Dusheiko M, Burnand B, Pittet V. A systematic review of cost-effectiveness studies comparing conventional, biological and surgical interventions for inflammatory bowel disease. PLoS ONE. 2017;12(10): e0185500.
van der Velde G, Pham B, Machado M, et al. Cost-effectiveness of biologic response modifiers compared to disease-modifying antirheumatic drugs for rheumatoid arthritis: a systematic review. Arthritis Care Res (Hoboken). 2011;63(1):65–78.
Bergstra SA, Branco JC, Vega-Morales D, et al. Inequity in access to bDMARD care and how it influences disease outcomes across countries worldwide: results from the METEOR-registry. Ann Rheum Dis. 2018;77(10):1413–20.
Pappas DA, Gerber RA, Litman HJ, et al. Delayed treatment acceleration in patients with rheumatoid arthritis who have inadequate response to initial tumor necrosis factor inhibitors: data from the corrona registry. Am Health Drug Benefits. 2018;11(3):148–58.
National Institute for Health and Care Excellence. Adalimumab, etanercept, infliximab, certolizumab pegol, golimumab, tocilizumab and abatacept for rheumatoid arthritis not previously treated with DMARDs or after conventional DMARDs only have failed. Technology Appraisal Guidance. NICE. 2016. www.nice.org.uk/guidance/ta375. Accessed 25 Feb 2021.
National Institute for Health and Care Excellence. Review of TA375; Adalimumab, etanercept, infliximab, certolizumab pegol, golimumab, tocilizumab and abatacept for rheumatoid arthritis not previously treated with DMARDs or after conventional DMARDs only have failed. Technology Appraisal Review Proposal Paper. NICE. 2019. https://www.nice.org.uk/guidance/ta375/evidence/consultation-paper-january-2019-pdf-6779359118. Accessed 25 Feb 2021.
van de Kerkhof PC, Reich K, Kavanaugh A, et al. Physician perspectives in the management of psoriasis and psoriatic arthritis: results from the population-based Multinational Assessment of Psoriasis and Psoriatic Arthritis survey. J Eur Acad Dermatol Venereol. 2015;29(10):2002–10.
Vulto AG, Jaquez OA. The process defines the product: what really matters in biosimilar design and production? Rheumatology (Oxford). 2017;56(suppl4):iv14–29.
Carrascosa JM, Jacobs I, Petersel D, Strohal R. Biosimilar drugs for psoriasis: principles, present, and near future. Dermatol Ther (Heidelb). 2018;8(2):173–94.
Gecse KB, Cumming F, D’Haens G. Biosimilars for inflammatory bowel disease: how can healthcare professionals help address patients’ concerns? Expert Rev Gastroenterol Hepatol. 2019;13(2):143–55.
Zhao S, Chadwick L, Mysler E, Moots RJ. Review of biosimilar trials and data on adalimumab in rheumatoid arthritis. Curr Rheumatol Rep. 2018;20(10):57.
European Medicines Agency. Medicines; biosimilars. 2021. https://www.ema.europa.eu/en/medicines/search_api_aggregation_ema_medicine_types/field_ema_med_biosimilar. Accessed 20 May 2021.
Food and Drug Administration. Biosimilar Product Information. 2021. https://www.fda.gov/drugs/biosimilars/biosimilar-product-information. Accessed 20 May 2021.
Razanskaite V, Bettey M, Downey L, et al. Biosimilar infliximab in inflammatory bowel disease: outcomes of a managed switching programme. J Crohns Colitis. 2017;11(6):690–6.
Narayanan R, Hariprasad SM, Sheth J. Biosimilars for the treatment of retinal diseases. Ophthalmic Surg Lasers Imaging Retina. 2021;52(5):242–6.
Sharma A, Kumar N, Parachuri N, Bandello F, Kuppermann BD, Loewenstein A. Biosimilars for retinal diseases: an update. Am J Ophthalmol. 2021;224:36–42.
Fabiani C, Vitale A, Emmi G, et al. The role of biosimilars in uveitis: long-term real-world outcomes of the switch from original to biosimilar TNF-alpha inhibitors. Front Pharmacol. 2019;10:1468.
Kumar N, Follestad T, Sen HN, Austeng D. A systematic switch from originator infliximab to biosimilar infliximab in patients with non-infectious uveitis. Am J Ophthalmol. 2021;225:178–84.
Sota J, Gentileschi S, Vitale A, et al. Effectiveness of SB5, an adalimumab biosimilar, in patients with noninfectious uveitis: a real-life monocentric experience. Asia Pac J Ophthalmol (Phila). 2021. https://doi.org/10.1097/APO.0000000000000380.
Thomas AS. Biologics for the treatment of noninfectious uveitis: current concepts and emerging therapeutics. Curr Opin Ophthalmol. 2019;30(3):138–50.
Cazap E, Jacobs I, McBride A, Popovian R, Sikora K. Global acceptance of biosimilars: importance of regulatory consistency, education, and trust. Oncologist. 2018;23(10):1188–98.
IQVIA. Global, European and Belgian pharmaceutical market trends. 2019. https://www.cib-pharma.be/uploads/global-european-andbelgian-pharmaceutical-market-trends-2019-final1552840137.pdf. Accessed 16 Dec 2019.
Patel S. Medicare spending on anti-vascular endothelial growth factor medications. Ophthalmol Retina. 2018;2(8):785–91.
Avastin Prescribing Information. 2021. https://www.gene.com/download/pdf/avastin_prescribing.pdf. Accessed 25 Feb 2021.
Catt Research Group, Martin DF, Maguire MG, et al. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. N Engl J Med. 2011;364(20):1897–908.
Diabetic Retinopathy Clinical Research Network, Wells JA, Glassman AR, et al. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N Engl J Med. 2015;372(13):1193–203.
Hykin P, Prevost AT, Sivaprasad S, et al. Intravitreal ranibizumab versus aflibercept versus bevacizumab for macular oedema due to central retinal vein occlusion: the LEAVO non-inferiority three-arm RCT. Health Technol Assess. 2021;25(38):1–196.
Low A, Faridi A, Bhavsar KV, et al. Comparative effectiveness and harms of intravitreal antivascular endothelial growth factor agents for three retinal conditions: a systematic review and meta-analysis. Br J Ophthalmol. 2019;103(4):442–51.
D’Souza HS, Kapoor KG, Wagner AL. Ziv-aflibercept for better regulating neovascular age-related macular degeneration (ZEBRA): a prospective randomized trial. Semin Ophthalmol. 2021;36(1–2):28–34.
Zaltrap Summary of Product Characteristics. 2017. Accessed 04 Feb 2022.
Daien V, Nguyen V, Essex RW, et al. Incidence and outcomes of infectious and noninfectious endophthalmitis after intravitreal injections for age-related macular degeneration. Ophthalmology. 2018;125(1):66–74.
Goldberg RA, Flynn HW Jr, Isom RF, Miller D, Gonzalez S. An outbreak of streptococcus endophthalmitis after intravitreal injection of bevacizumab. Am J Ophthalmol. 2012;153(2):204–8.
Ricci F, Calabrese A, De Felici C, Missiroli F, Pileri M, Regine F. A cluster of presumed, noninfectious endophthalmitis after intravitreal injection of bevacizumab: long-term follow-up. Digit J Ophthalmol. 2016;22(2):41–5.
VanderBeek BL, Bonaffini SG, Ma L. Association of compounded bevacizumab with postinjection endophthalmitis. JAMA Ophthalmol. 2015;133(10):1159–64.
Robinson PC, Conrad D. Biologic therapy for uveitis: addressing access issues is paramount. Intern Med J. 2020;50(4):508–9.
Holz FG, Figueroa MS, Bandello F, et al. Ranibizumab treatment in treatment-naive neovascular age-related macular degeneration: results from LUMINOUS, a global real-world study. Retina. 2020;40(9):1673–85.
VanderBeek BL, Scavelli K, Yu Y. Determinants in initial treatment choice for diabetic macular edema. Ophthalmol Retina. 2020;4(1):41–8.
Jackson S, Stokes JP. Impact of out-of-pocket costs on patient initiation, adherence and persistence rates for patients treated with anti-vascular endothelial growth factor medicines. Clin Exp Ophthalmol. 2020;48(4):477–85.
Kelkar A, Webers C, Shetty R, et al. Factors affecting compliance to intravitreal anti-vascular endothelial growth factor therapy in Indian patients with retinal vein occlusion, age-related macular degeneration, and diabetic macular edema. Indian J Ophthalmol. 2020;68(10):2143–7.
Zangeneh F, Dolinar R. Biosimilar drugs are not generics. Endocr Pract. 2016;22(1):6–7.
Pharmaceutical Technology. Biosimilar development: the incentives and challenges. 2017. https://www.pharmaceutical-technology.com/comment/commentwhat-are-the-incentives-and-challenges-to-biosimilar-development-5751024/. Accessed 05 May 2021.
Federal Trade Commission. Emerging health care issues: follow-on biologic drug competition. 2009. https://www.ftc.gov/sites/default/files/documents/reports/emerging-health-care-issues-follow-biologic-drug-competition-federal-trade-commission-report/p083901biologicsreport.pdf. Accessed 27 Oct 2021.
Dutta B, Huys I, Vulto AG, Simoens S. Identifying key benefits in European off-patent biologics and biosimilar markets: it is not only about price! BioDrugs. 2020;34(2):159–70.
European Medicines Agency. Biosimilars in the EU. Guide for healthcare professionals. 2014. https://www.ema.europa.eu/en/documents/leaflet/biosimilars-eu-information-guide-healthcare-professionals_en.pdf. Accessed 25 Feb 2021.
Food and Drug Administration. Scientific Considerations in Demonstrating Biosimilarity to a Reference Product Guidance for Industry, 2015. https://www.fda.gov/media/82647/download. Accessed 25 Feb 2021.
World Health Organization. Guidelines on evaluation of similar biotherapeutics products (SBPs), 2013. https://www.who.int/biologicals/publications/trs/areas/biological_therapeutics/TRS_977_Annex_2.pdf?ua=1. Accessed 25 Feb 2021.
Food and Drug Administration. Guidance for Industry. Development of therapeutic protein biosimilars: comparative analytical assessment and other quality-related considerations. 2021. https://www.fda.gov/media/125484/download. Accessed 20 May 2021.
Duivelshof BL, Jiskoot W, Beck A, Veuthey JL, Guillarme D, D’Atri V. Glycosylation of biosimilars: recent advances in analytical characterization and clinical implications. Anal Chim Acta. 2019;16(1089):1–18.
Hada V, Bagdi A, Bihari Z, Timari SB, Fizil A, Szantay C Jr. Recent advancements, challenges, and practical considerations in the mass spectrometry-based analytics of protein biotherapeutics: a viewpoint from the biosimilar industry. J Pharm Biomed Anal. 2018;30(161):214–38.
Declerck P, Farouk RM. The road from development to approval: evaluating the body of evidence to confirm biosimilarity. Rheumatology (Oxford). 2017;56(suppl_4):iv4–13.
Food and Drug Administration. Guidance for industry. Q8(R2) Pharmaceutical development. 2021. https://www.fda.gov/media/71535/download. Accessed 12 May 2021.
Vezer B, Buzas Z, Sebeszta M, Zrubka Z. Authorized manufacturing changes for therapeutic monoclonal antibodies (mAbs) in European Public Assessment Report (EPAR) documents. Curr Med Res Opin. 2016;32(5):829–34.
Dorner T, Kay J. Biosimilars in rheumatology: current perspectives and lessons learnt. Nat Rev Rheumatol. 2015;11(12):713–24.
Kiss S, Fine HF, Krawitz J. Coming of age: biosimilars. Ophthalmic Surg Lasers Imaging Retina. 2018;49(3):162–5.
Wolff-Holz E, Garcia Burgos J, Giuliani R, et al. Preparing for the incoming wave of biosimilars in oncology. ESMO Open. 2018;3(6): e000420.
European Medicines Agency. Guideline on similar biological medicinal products containing biotechnology-derived proteins as active substance: non-clinical and clinical issues, 2014. https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-similar-biological-medicinal-products-containing-biotechnology-derived-proteins-active_en-2.pdf. Accessed 04 May 2021.
Diaz LP, Millan S, Chaban N, Campo AD, Spitzer E. Current state and comparison of the clinical development of bevacizumab, rituximab and trastuzumab biosimilars. Future Oncol. 2021;17(19):2529–44.
Zuniga L, Calvo B. Biosimilars: pharmacovigilance and risk management. Pharmacoepidemiol Drug Saf. 2010;19(7):661–9.
Mones J, Srivastava SK, Jaffe GJ, et al. Risk of inflammation, retinal vasculitis, and retinal occlusion-related events with brolucizumab: post hoc review of HAWK and HARRIER. Ophthalmology. 2021;128(7):1050–9.
Singer M, Albini TA, Seres A, et al. Clinical characteristics and outcomes of eyes with intraocular inflammation after brolucizumab: post hoc analysis of HAWK and HARRIER. Ophthalmol Retina. 2021. https://doi.org/10.1016/j.oret.2021.05.003.
Schellekens H. Bioequivalence and the immunogenicity of biopharmaceuticals. Nat Rev Drug Discov. 2002;1(6):457–62.
Schreitmuller T, Barton B, Zharkov A, Bakalos G. Comparative immunogenicity assessment of biosimilars. Future Oncol. 2019;15(3):319–29.
Krieckaert C, Rispens T, Wolbink G. Immunogenicity of biological therapeutics: from assay to patient. Curr Opin Rheumatol. 2012;24(3):306–11.
Smith A, Manoli H, Jaw S, et al. Unraveling the effect of immunogenicity on the PK/PD, efficacy, and safety of therapeutic proteins. J Immunol Res. 2016;2016:2342187.
Bloem K, Hernandez-Breijo B, Martinez-Feito A, Rispens T. Immunogenicity of therapeutic antibodies: monitoring antidrug antibodies in a clinical context. Ther Drug Monit. 2017;39(4):327–32.
Barbier L, Ebbers HC, Declerck P, Simoens S, Vulto AG, Huys I. The efficacy, safety, and immunogenicity of switching between reference biopharmaceuticals and biosimilars: a systematic review. Clin Pharmacol Ther. 2020;108(4):734–55.
Tesser JR, Furst DE, Jacobs I. Biosimilars and the extrapolation of indications for inflammatory conditions. Biologics. 2017;11:5–11.
Weise M, Kurki P, Wolff-Holz E, Bielsky MC, Schneider CK. Biosimilars: the science of extrapolation. Blood. 2014;124(22):3191–6.
European Medicines Agency. Imraldi SmPC. 2020. https://www.ema.europa.eu/en/documents/product-information/imraldi-epar-product-information_en.pdf. Accessed 25 Feb 2020.
Feagan BG, Choquette D, Ghosh S, et al. The challenge of indication extrapolation for infliximab biosimilars. Biologicals. 2014;42(4):177–83.
Kurki P, van Aerts L, Wolff-Holz E, Giezen T, Skibeli V, Weise M. Interchangeability of biosimilars: a European perspective. BioDrugs. 2017;31(2):83–91.
Koyfman H. Biosimilarity and Interchangeability in the biologics price competition and innovation act of 2009 and FDA’s 2012 draft guidance for industry. Biotechnol Law Rep. 2013;32(4):238–51.
Food and Drug Administration. FDA approves first interchangeable biosimilar insulin product for treatment of diabetes. Silver Spring: FDA; 2021.
Food and Drug Administration. Biosimilar and interchangeable biologics: more treatment choices. 2021. https://www.fda.gov/consumers/consumer-updates/biosimilar-and-interchangeable-biologics-more-treatment-choices. Accessed 20 Sep 2021.
Cohen HP, Blauvelt A, Rifkin RM, Danese S, Gokhale SB, Woollett G. Switching reference medicines to biosimilars: a systematic literature review of clinical outcomes. Drugs. 2018;78(4):463–78.
Inotai A, Prins CPJ, Csanadi M, Vitezic D, Codreanu C, Kalo Z. Is there a reason for concern or is it just hype? A systematic literature review of the clinical consequences of switching from originator biologics to biosimilars. Expert Opin Biol Ther. 2017;17(8):915–26.
Afzali A, Furtner D, Melsheimer R, Molloy PJ. The automatic substitution of biosimilars: definitions of interchangeability are not interchangeable. Adv Ther. 2021;38(5):2077–93.
ClinicalTrials.gov. A study to evaluate CKD-701 and Lucentis® in patients with neovascular(wet) age related macular degeneration. 2021. https://www.clinicaltrials.gov/ct2/show/NCT04857177. Accessed 20 Sep 2021.
ClinicalTrials.gov. Efficacy and safety of the biosimilar ranibizumab FYB201 in comparison to lucentis in patients with neovascular age-related macular degeneration (COLUMBUS-AMD). 2019. https://www.clinicaltrials.gov/ct2/show/NCT02611778. Accessed 20 Sep 2021.
Food and Drug Administration. FDA approves first biosimilar to treat macular degeneration disease and other eye conditions. 2021.https://www.fda.gov/news-events/press-announcements/fda-approves-first-biosimilar-treat-macular-degeneration-disease-and-other-eye-conditions. Accessed 05 Oct 2021.
European Medicines Agency. Byooviz EPAR. 2021. https://www.ema.europa.eu/en/medicines/human/EPAR/byooviz. Accessed 05 Oct 2021.
ClinicalTrials.gov. Comparing the efficacy and safety of biosimilar candidate xlucane versus lucentis® in patients with nAMD (XPLORE). 2021. https://clinicaltrials.gov/ct2/show/NCT03805100. Accessed 20 Sep 2021.
ClinicalTrials.gov. Efficacy, safety, pharmacokinetics, immunogenicity of GNR-067 and Lucentis® (NAP). 2020. https://clinicaltrials.gov/ct2/show/NCT04667039. Accessed 20 Sep 2021.
ClinicalTrials.gov. Study to compare efficacy and safety of LUBT010 and Lucentis® in patients with neovascular AMD. 2021. https://clinicaltrials.gov/ct2/show/NCT04690556. Accessed 20 Sep 2021.
ClinicalTrials.gov. A study to understand effectiveness and safety of ABP 938 compared to aflibercept (Eylea®) in patients suffering with neovascular age-related macular degeneration [Neovascular (Wet) AMD]. 2021. https://clinicaltrials.gov/ct2/show/NCT04270747. Accessed 20 Sep 2021.
ClinicalTrials.gov. Efficacy and safety of the aflibercept FYB203 biosimilar in comparison to Eylea® in patients with neovascular age-related macular degeneration (MAGELLAN-AMD). 2021. https://clinicaltrials.gov/ct2/show/NCT04522167. Accessed 20 Sep 2021.
ClinicalTrials.gov. Comparative study to evaluate the efficacy and safety of MYL-1701P and Eylea® in subjects with diabetic macular edema. 2021. https://clinicaltrials.gov/ct2/show/NCT03610646. Accessed 20 Sep 2021.
ClinicalTrials.gov. A study to compare SB15 (proposed aflibercept biosimilar) to Eylea in subjects with neovascular age-related macular degeneration (AMD). 2021. https://clinicaltrials.gov/ct2/show/NCT04450329. Accessed 20 Sep 2021.
ClinicalTrials.gov. A study to compare SCD411 and Eylea® in subjects with wet age-related macular degeneration (AMD). 2020. https://clinicaltrials.gov/ct2/show/NCT04480463. Accessed 20 Sep 2021.
ClinicalTrials.gov. A clinical effectiveness study examining the efficacy and safety of ONS-5010 in subjects with neovascular age-related macular degeneration (AMD). 2021. https://clinicaltrials.gov/ct2/show/NCT03834753. Accessed 20 Sep 2021.
ClinicalTrials.gov. A phase 3 two-part study of the efficacy and safety of HLX04-O in subjects with wet age-related macular degeneration. 2021. https://clinicaltrials.gov/ct2/show/NCT04740671. Accessed 20 Sep 2021.
Woo SJ, Veith M, Hamouz J, et al. Efficacy and safety of proposed ranibizumab biosimilar (SB11) versus reference ranibizumab (RBZ) in subjects with neovascular age-related macular degeneration: randomized clinical trial. JAMA Ophthalmology. 2021;139:68–76.
Bressler NM, Veith M, Hamouz J, et al. Biosimilar SB11 versus reference ranibizumab in neovascular age-related macular degeneration: 1-year phase III randomised clinical trial outcomes. Br J Ophthalmol. 2021. https://doi.org/10.1136/bjophthalmol-2021-319637.
Kessler M, Goldsmith D, Schellekens H. Immunogenicity of biopharmaceuticals. Nephrol Dial Transpl. 2006;21(Suppl 5):v9-12.
European Medicines Agency. Byooviz-Assessment Report. 2021. https://www.ema.europa.eu/en/documents/assessment-report/byooviz-epar-public-assessment-report_en.pdf. Acessed 05 Oct 2021.
Holz FG, Oleksy P, Ricci F, et al. Efficacy and safety of biosimilar FYB201 compared with ranibizumab in neovascular age-related macular degeneration. Ophthalmology. 2021. https://doi.org/10.1016/j.ophtha.2021.04.031.
Czepielewski MA, Garret Q, Vencio SAC, et al. Switching from originator recombinant growth hormone (Genotropin) to biosimilar (CRISCY): results from a 6-month, multicentric, non-inferiority, extension trial. Growth Horm IGF Res. 2021;56:101372.
Ebbers HC, Pieper B, Issa A, Addison J, Freudensprung U, Rezk MF. Real-world evidence on etanercept biosimilar SB4 in etanercept-naive or switching patients: a systematic review. Rheumatol Ther. 2019;6(3):317–38.
Gerdes S, Thaci D, Griffiths CEM, et al. Multiple switches between GP2015, an etanercept biosimilar, with originator product do not impact efficacy, safety and immunogenicity in patients with chronic plaque-type psoriasis: 30-week results from the phase 3, confirmatory EGALITY study. J Eur Acad Dermatol Venereol. 2018;32(3):420–7.
Glintborg B, Loft AG, Omerovic E, et al. To switch or not to switch: results of a nationwide guideline of mandatory switching from originator to biosimilar etanercept. One-year treatment outcomes in 2061 patients with inflammatory arthritis from the DANBIO registry. Ann Rheum Dis. 2019;78(2):192–200.
Jorgensen KK, Olsen IC, Goll GL, et al. Switching from originator infliximab to biosimilar CT-P13 compared with maintained treatment with originator infliximab (NOR-SWITCH): a 52-week, randomised, double-blind, non-inferiority trial. Lancet. 2017;389(10086):2304–16.
Pugliese D, Guidi L, Privitera G, et al. Switching from IFX originator to biosimilar CT-P13 does not impact effectiveness, safety and immunogenicity in a large cohort of IBD patients. Expert Opin Biol Ther. 2021;21(1):97–104.
Wiland P, Jeka S, Dokoupilova E, et al. Switching to biosimilar SDZ-ADL in patients with moderate-to-severe active rheumatoid arthritis: 48-week efficacy, safety and immunogenicity results from the phase III, randomized, double-blind ADMYRA study. BioDrugs. 2020;34(6):809–23.
Pouillon L, Danese S, Hart A, et al. Consensus report: clinical recommendations for the prevention and management of the nocebo effect in biosimilar-treated IBD patients. Aliment Pharmacol Ther. 2019;49(9):1181–7.
Barsky AJ, Saintfort R, Rogers MP, Borus JF. Nonspecific medication side effects and the nocebo phenomenon. JAMA. 2002;287(5):622–7.
Colloca L, Miller FG. The nocebo effect and its relevance for clinical practice. Psychosom Med. 2011;73(7):598–603.
Rezk MF, Pieper B. Treatment outcomes with biosimilars: be aware of the nocebo effect. Rheumatol Ther. 2017;4(2):209–18.
Sarnola K, Merikoski M, Jyrkka J, Hameen-Anttila K. Physicians’ perceptions of the uptake of biosimilars: a systematic review. BMJ Open. 2020;10(5): e034183.
Tweehuysen L, Huiskes VJB, van den Bemt BJF, et al. Open-label, non-mandatory transitioning from originator etanercept to biosimilar SB4: six-month results from a controlled cohort study. Arthritis Rheumatol. 2018;70(9):1408–18.
Colloca L, Barsky AJ. Placebo and nocebo effects. N Engl J Med. 2020;382(6):554–61.
Colloca L, Finniss D. Nocebo effects, patient-clinician communication, and therapeutic outcomes. JAMA. 2012;307(6):567–8.
Colloca L, Panaccione R, Murphy TK. The clinical implications of nocebo effects for biosimilar therapy. Front Pharmacol. 2019;10:1372.
Daniali H, Flaten MA. A qualitative systematic review of effects of provider characteristics and nonverbal behavior on pain, and placebo and nocebo effects. Front Psychiatry. 2019;10:242.
Enck P, Bingel U, Schedlowski M, Rief W. The placebo response in medicine: minimize, maximize or personalize? Nat Rev Drug Discov. 2013;12(3):191–204.
Kristensen LE, Alten R, Puig L, et al. Non-pharmacological effects in switching medication: the nocebo effect in switching from originator to biosimilar agent. BioDrugs. 2018;32(5):397–404.
Planes S, Villier C, Mallaret M. The nocebo effect of drugs. Pharmacol Res Perspect. 2016;4(2): e00208.
Odinet JS, Day CE, Cruz JL, Heindel GA. The biosimilar nocebo effect? A systematic review of double-blinded versus open-label studies. J Manag Care Spec Pharm. 2018;24(10):952–9.
Mansour AM, Stewart MW, Farah ME, Mansour HA, Chhablani J. Ziv-aflibercept: a cost-effective, off-label, highly potent antagonist of vascular endothelial growth factor. Acta Ophthalmol. 2019. https://doi.org/10.1111/aos.14328.
Bro T, Derebecka M, Jorstad OK, Grzybowski A. Off-label use of bevacizumab for wet age-related macular degeneration in Europe. Graefes Arch Clin Exp Ophthalmol. 2020;258(3):503–11.
Aladul MI, Fitzpatrick RW, Chapman SR. The effect of new biosimilars in rheumatology and gastroenterology specialities on UK healthcare budgets: results of a budget impact analysis. Res Social Adm Pharm. 2019;15(3):310–7. https://doi.org/10.1016/j.sapharm.2018.05.009.
Jha A, Upton A, Dunlop WC, Akehurst R. The budget impact of biosimilar infliximab (Remsima®) for the treatment of autoimmune diseases in five European countries. Adv Ther. 2015;32(8):742–56. https://doi.org/10.1007/s12325-015-0233-1.
Brodszky V, Rencz F, Pentek M, Baji P, Lakatos PL, Gulacsi L. A budget impact model for biosimilar infliximab in Crohn’s disease in Bulgaria, the Czech Republic, Hungary, Poland, Romania, and Slovakia. Expert Rev Pharmacoecon Outcomes Res. 2016;16(1):119–25. https://doi.org/10.1586/14737167.2015.1067142.
Lee SM, Jung JH, Suh D, et al. Budget impact of switching to biosimilar trastuzumab (CT-P6) for the treatment of breast cancer and gastric cancer in 28 European countries. BioDrugs. 2019;33(4):423–36. https://doi.org/10.1007/s40259-019-00359-0.
Gulacsi L, Brodszky V, Baji P, Rencz F, Pentek M. The rituximab biosimilar CT-P10 in rheumatology and cancer: a budget impact analysis in 28 European countries. Adv Ther. 2017;34(5):1128–44. https://doi.org/10.1007/s12325-017-0522-y.
MacDonald K, McBride A, Alrawashdh N, Abraham I. Cost-efficiency and expanded access of prophylaxis for chemotherapy-induced (febrile) neutropenia: economic simulation analysis for the US of conversion from reference pegfilgrastim to biosimilar pegfilgrastim-cbqv. J Med Econ. 2020;23(12):1466–76. https://doi.org/10.1080/13696998.2020.1833339.
Yang J, Liu R, Ektare V, Stephens J, Shelbaya A. Does biosimilar bevacizumab offer affordable treatment options for cancer patients in the USA? A budget impact analysis from US commercial and Medicare payer perspectives. Appl Health Econ Health Policy. 2021;19(4):605–18. https://doi.org/10.1007/s40258-021-00637-5.
Yang J, Liu R, Granghaud A, Zaidi O, Stephens J. Biosimilar pegfilgrastim may offer affordable treatment options for patients in France: a budget impact analysis on the basis of clinical trial and real-world data. J Med Econ. 2021;24(1):665–74. https://doi.org/10.1080/13696998.2021.1922252.
Jang M, Simoens S, Kwon T. Budget impact analysis of the introduction of rituximab and trastuzumab intravenous biosimilars to EU-5 markets. BioDrugs. 2021;35(1):89–101. https://doi.org/10.1007/s40259-020-00461-8.
Alten R, Batko B, Hala T, et al. Randomised, double-blind, phase III study comparing the infliximab biosimilar, PF-06438179/GP1111, with reference infliximab: efficacy, safety and immunogenicity from week 30 to week 54. RMD Open. 2019;5(1):e000876. https://doi.org/10.1136/rmdopen-2018-000876.
Smolen JS, Choe JY, Prodanovic N, et al. Comparing biosimilar SB2 with reference infliximab after 54 weeks of a double-blind trial: clinical, structural and safety results. Rheumatology (Oxford). 2017;56(10):1771–9. https://doi.org/10.1093/rheumatology/kex254.
Choe JY, Prodanovic N, Niebrzydowski J, et al. A randomised, double-blind, phase III study comparing SB2, an infliximab biosimilar, to the infliximab reference product Remicade in patients with moderate to severe rheumatoid arthritis despite methotrexate therapy. Ann Rheum Dis. 2017;76(1):58–64. https://doi.org/10.1136/annrheumdis-2015-207764.
Fleischmann RM, Alten R, Pileckyte M, et al. A comparative clinical study of PF-06410293, a candidate adalimumab biosimilar, and adalimumab reference product (Humira®) in the treatment of active rheumatoid arthritis. Arthritis Res Ther. 2018;20(1):178. https://doi.org/10.1186/s13075-018-1676-y.
Cohen SB, Alonso-Ruiz A, Klimiuk PA, et al. Similar efficacy, safety and immunogenicity of adalimumab biosimilar BI 695501 and Humira reference product in patients with moderately to severely active rheumatoid arthritis: results from the phase III randomised VOLTAIRE-RA equivalence study. Ann Rheum Dis. 2018;77(6):914–21. https://doi.org/10.1136/annrheumdis-2017-212245.
Weinblatt ME, Baranauskaite A, Niebrzydowski J, et al. Phase III randomized study of SB5, an adalimumab biosimilar, versus reference adalimumab in patients with moderate-to-severe rheumatoid arthritis. Arthritis Rheumatol. 2018;70(1):40–8. https://doi.org/10.1002/art.40336.
Emery P, Vencovsky J, Sylwestrzak A, et al. 52-week results of the phase 3 randomized study comparing SB4 with reference etanercept in patients with active rheumatoid arthritis. Rheumatology. 2017;56(12):2093–101. https://doi.org/10.1093/rheumatology/kex269.
Suh CH, Yoo DH, Kasay AB, et al. Long-term efficacy and safety of biosimilar CT-P10 versus innovator rituximab in rheumatoid arthritis: 48-week results from a randomized phase III trial. BioDrugs. 2019;33(1):79–91. https://doi.org/10.1007/s40259-018-00331-4.
Griffiths CEM, Thaçi D, Gerdes S, et al. The EGALITY study: a confirmatory, randomized, double-blind study comparing the efficacy, safety and immunogenicity of GP2015, a proposed etanercept biosimilar, vs. the originator product in patients with moderate-to-severe chronic plaque-type psoriasis. Br J Dermatol. 2017;176(4):928–38. https://doi.org/10.1111/bjd.15152.
Papp K, Bachelez H, Costanzo A, et al. Clinical similarity of the biosimilar ABP 501 compared with adalimumab after single transition: long-term results from a randomized controlled, double-blind, 52-week, phase III trial in patients with moderate-to-severe plaque psoriasis. Br J Dermatol. 2017;177(6):1562–74. https://doi.org/10.1111/bjd.15857.
Hercogova J, Papp KA, Chyrok V, Ullmann M, Vlachos P, Edwards CJ. AURIEL-PsO: a randomized, doubleblind phase III equivalence trial to demonstrate the clinical similarity of the proposed biosimilar MSB11022 to reference adalimumab in patients with moderate-to-severe chronic plaque-type psoriasis. Br J Dermatol. 2020;182(2):316–26. https://doi.org/10.1111/bjd.18220.
Rezvani H, Mortazavizadeh SM, Allahyri A, et al. Efficacy and safety of proposed bevacizumab biosimilar BE1040V in patients with metastatic colorectal cancer: a phase III, randomized, double-blind, noninferiority clinical trial. Clin Ther. 2020;42(5):848–59. https://doi.org/10.1016/j.clinthera.2020.03.009.
Reinmuth N, Bryl M, Bondarenko I, et al. PF-06439535 (a bevacizumab biosimilar) compared with reference bevacizumab (Avastin®), both plus paclitaxel and carboplatin, as first-line treatment for advanced nonsquamous non-small-cell lung cancer: a randomized, double-blind study. BioDrugs. 2019;33(5):555–70. https://doi.org/10.1007/s40259-019-00363-4.
Waller CF, Ranganna GM, Pennella EJ, et al. Randomized phase 3 efficacy and safety trial of proposed pegfilgrastim biosimilar MYL-1401H in the prophylactic treatment of chemotherapy-induced neutropenia. Ann Hematol. 2019;98(5):1217–24. https://doi.org/10.1007/s00277-019-03639-5.
Blackwell K, Donskih R, Jones CM, et al. A comparison of proposed biosimilar LA-EP2006 and reference pegfilgrastim for the prevention of neutropenia in patients with early-stage breast cancer receiving myelosuppressive adjuvant or neoadjuvant chemotherapy: Pegfilgrastim Randomized Oncology (Supportive Care) Trial to Evaluate Comparative Treatment (PROTECT-2), a phase III, randomized, double-blind trial. Oncologist. 2016;21(7):789–94. https://doi.org/10.1634/theoncologist.2016-0011.
Pegram MD, Bondarenko I, Zorzetto MMC, et al. PF-05280014 (a trastuzumab biosimilar) plus paclitaxel compared with reference trastuzumab plus paclitaxel for HER2-positive metastatic breast cancer: a randomised, double-blind study. Br J Cancer. 2019;120(2):172–82. https://doi.org/10.1038/s41416-018-0340-2.
Pivot X, Bondarenko I, Nowecki Z, et al. A phase III study comparing SB3 (a proposed trastuzumab biosimilar) and trastuzumab reference product in HER2-positive early breast cancer treated with neoadjuvant-adjuvant treatment: Final safety, immunogenicity and survival results. Eur J Cancer 2018;93:19–27. https://doi.org/10.1016/j.ejca.2018.01.072.
Shi Y, Song Y, Qin Y, et al. A phase 3 study of rituximab biosimilar HLX01 in patients with diffuse large B-cell lymphoma. J Hematol Oncol. 2020;13(1):38. https://doi.org/10.1186/s13045-020-00871-9.
Sharman JP, Liberati AM, Ishizawa K, et al. A randomized, double-blind, efficacy and safety study of PF-05280586 (a rituximab biosimilar) compared with rituximab reference product (MabThera®) in subjects withpreviously untreated CD20-positive, low-tumor-burden follicular lymphoma (LTB-FL). BioDrugs. 2020;34(2):171–81. https://doi.org/10.1007/s40259-019-00398-7.
Nishi S, Yamada M, Tsuruya K, Masakane I, Nakamoto H. JR-131. A biosimilar of darbepoetin alfa, for the treatment of hemodialysis patients with renal anemia: a randomized, double-blinded, parallel-group phase 3 study. Ther Apher Dial 2020;24(2):126–35. https://doi.org/10.1111/1744-9987.13422.
Garg SK, Wernicke-Panten K, Wardecki M, et al. Efficacy and safety of insulin aspart biosimilar SAR341402 versus originator insulin aspart in people with diabetes treated for 26 weeks with multiple daily injections in combination with insulin glargine: a randomized open-label trial (GEMELLI 1). Diabetes Technol Ther. 2020;22(2):85–95. https://doi.org/10.1089/dia.2019.0382.
Peterkova V, Arslanoglu I, Bolshova-Zubkovskaya E, et al. A randomized, double-blind study to assess the efficacy and safety of valtropin, a biosimilar growth hormone, in children with growth hormone deficiency. Horm Res. 2007;68(6):288–93. https://doi.org/10.1159/000105494.
Czepielewski MA, Garret Q, Vencio SAC, et al. Efficacy and safety of a biosimilar recombinant human growth hormone (r-hGH Cristalia) compared with reference r-hGH in children with growth hormone deficiency (CERES study): A randomized, multicentric, investigator-blind, phase 3 trial. Growth Horm IGF Res. 2019;48–49:29–35. https://doi.org/10.1016/j.ghir.2019.07.003.
Hagino H, Narita R, Yokoyama Y, Watanabe M, Tomomitsu M. A multicenter, randomized, rater-blinded, parallel-group, phase 3 study to compare the efficacy, safety, and immunogenicity of biosimilar RGB-10 and reference once-daily teriparatide in patients with osteoporosis. Osteoporos Int. 2019;30(10):2027–37. https://doi.org/10.1007/s00198-019-05038-y.
Acknowledgements
Editorial assistance in the preparation of this manuscript was provided by Iain Bartlett of Springer Healthcare Ltd. Funding for this assistance was provided by Biogen International GmbH, Baar, Switzerland.
Funding
Biogen International GmbH provided financial support for the preparation of this review article and for the journal’s Rapid Service Fee. The content of the article and decision to publish was at the authors’ discretion.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
Seenu M. Hariprasad, Richard P. Gale, Christina Y. Weng, Hans C. Ebbers, Mourad F. Rezk, and Ramin Tadayoni contributed to the conception, drafting, and finalization of the article including approval to submit.
Disclosures
Christina Y. Weng has acted as a consultant for Allergan/AbbVie, Alcon, Novartis, DORC, Regeneron, REGENXBIO, Genentech, and Alimera Sciences. Ramin Tadayoni has acted as a consultant for Novartis, Bayer, Allergan, Roche, Genentech, Thea, Oculis, Alcon, Zeiss. Mourad F. Rezk and Hans C. Ebbers are employees of Biogen International GmbH and may hold stock in Biogen. Seenu M. Hariprasad is a consultant or on the speaker’s bureau for Allergan, EyePoint Pharmaceuticals, Bausch & Lomb, Alimera Sciences, Novartis, Spark, Biogen and Regeneron. Richard P. Gale has acted as a consultant, or is on the speaker’s bureau, for Novartis, Bayer, Allergan/ Abbvie, Roche, Almeria, Heidelberg.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Hariprasad, S.M., Gale, R.P., Weng, C.Y. et al. An Introduction to Biosimilars for the Treatment of Retinal Diseases: A Narrative Review. Ophthalmol Ther 11, 959–982 (2022). https://doi.org/10.1007/s40123-022-00488-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40123-022-00488-w