
Abstract
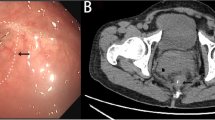
We present a case of successful minimally invasive treatment of a completely obstructed rectal anastomosis by using a transanal plasmakinetic resectoscope, along with a review of the relevant literature. A 75-year-old man underwent low anterior resection for rectal cancer. Complete obstruction of the rectal anastomosis was visualized at 6.0 cm from the anal verge, 5 months later. We carefully cut at the center of the circular staple line to find the orifice of anastomosis with a plasmakinetic resectoscope. Then, a sufficient amount of fibrotic tissue at the stenosis was resected to maintain the continuity of the bowel. At 4 months follow-up, the patient had complete resolution of symptoms. Transanal plasmakinetic resection is a possible choice for treatment of a completely obstructed colorectal anastomosis. However, these techniques have risks and should be implemented with great caution in selected patients by skilled endoscopists or surgeons.




Similar content being viewed by others


References
Luchtefeld MA, Milsom JW, Senagore A, Surrell JA, Mazier WP (1989) Colorectal anastomotic stenosis. Results of a survey of the ASCRS membership. Dis Colon Rectum 32:733–736
Lefevre JH, Bretagnol F, Maggioni L et al (2011) Redo surgery for failed colorectal or coloanal anastomosis: a valuable surgical challenge. Surgery 149:65–71
Bong JW, Lim SB (2019) Transanal minimally invasive surgery as a treatment option for a completely occluded anastomosis after low anterior resection: a new approach to severe anastomotic stenosis. Asian J Endosc Surg 12:175–177
Curcio G, Spada M, di Francesco F, Tarantino I, Barresi L, Burgio G, Traina M (2010) Completely obstructed colorectal anastomosis: a new nonelectrosurgical endoscopic approach before balloon dilatation. World J Gastroenterol 16:4751–4754
Yazawa K, Morioka D, Matsumoto C et al (2014) Blunt penetration technique for treatment of a completely obstructed anastomosis after rectal resection: a case report. J Med Case Rep 8:236
Yuan X, Liu W, Ye L, Wu M, Hu B (2019) Combination of endoscopic incision and balloon dilation for treatment of a completely obstructed anastomotic stenosis following colorectal resection: a case report. Medicine (Baltimore) 98:e16292
Kaushik N, Rubin J, McGrath K (2006) Treatment of benign complete colonic anastomotic obstruction by using an endoscopic rendezvous technique. Gastrointest Endosc 63:727–730
Albertsmeier M, Rittler P, Hoffmann RT, Spelsberg F (2011) Treatment of a completely obstructed colonic anastomotic stricture using a CT-guided endoscopic rendezvous technique. Endoscopy 43(Suppl 2 UCTN):E5–E6
Poincloux L, Pezet D, Rouquette O (2016) Successful recanalization of complete anastomotic stricture using colorectal endoscopic ultrasound-guided rendezvous thus allowing stoma reversal: two cases. Endoscopy 48(S 01):E353–E354
Sanaei O, Ngamruengphong S, Chen YI, Bukhari M, Brewer Gutierrez O, Kumbhari V, Khashab MA (2017) Endoscopic ultrasonography-guided freestyle rendezvous recanalization of a complete postoperative rectosigmoid anastomotic obstruction with a lumen-apposing metal stent. Endoscopy 49:E206–E207
Gornals JB, Albines G, Trenti L, Mast R, Frago R (2015) EUS-guided recanalization of a complete rectal anastomotic stenosis by use of a lumen-apposing metal stent. Gastrointest Endosc 82(4):752
De Lusong MA, Shah JN, Soetikno R et al (2008) Treatment of a completely obstructed colonic anastomotic stricture by using a prototype forward-array echoendoscope and facilitated by SpyGlass. Gastrointest Endosc 68:988–992
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Kawada K, Sakai Y (2016) Preoperative, intraoperative and postoperative risk factors for anastomotic leakage after laparoscopic low anterior resection with double stapling technique anastomosis. World J Gastroenterol 22:5718–5727
Oz MC, Forde KA (1990) Endoscopic alternatives in the management of colonic strictures. Surgery 108:513–519
Ravo B (1988) Colorectal anastomotic healing and intracolonic bypass procedure. Surg Clin North Am 68:1267–1294
Kwon YH, Jeon SW, Lee YK (2013) Endoscopic management of refractory benign colorectal strictures. Clin Endosc 46:472–475
Hagiwara A, Sakakura C, Shirasu M, Torii T, Hirata Y, Yamagishi H (1999) Sigmoidofiberscopic incision plus balloon dilatation for anastomotic cicatricial stricture after anterior resection of the rectum. World J Surg 23:717–720
McGrath K, Brazer S (2002) Combined antegrade and retrograde dilation: a new endoscopic technique in the management of complex esophageal stricture [comment]. Gastrointest Endosc 56:163
Baumgart DC, Veltzke-Schlieker W, Wiedenmann B, Hintze RE (2005) Successful recanalization of a completely obliterated esophageal stricture by using an endoscopic rendezvous maneuver. Gastrointest Endosc 61:473–475
Lee BC, Oh S, Lim SB, Yu CS, Kim JC (2017) Transanal minimally-invasive surgery for treating patients with regressed rectal cancer after preoperative chemoradiotherapy. Ann Coloproctol 33:52–56
Nepal P, Mori S, Kita Y, Tanabe K, Baba K, Uchikado Y, Kurahara H, Arigami T, Sakoda M, Maemura K, Natsugoe S (2019) Radial incision and cutting method using a transanal approach for treatment of anastomotic strictures following rectal cancer surgery: a case report. World J Surg Oncol 17:48
Nepal P, Mori S, Kita Y, Tanabe K, Baba K, Sasaki F, Nasu Y, Ido A, Uchikado Y, Kurahara H, Arigami T, Sakoda M, Maemura K, Natsugoe S (2019) Combined endoscopic submucosal dissection and transanal minimally invasive surgery for the management of lower rectal adenoma extending above the dentate line: a case report. Medicine (Baltimore) 98:e15289
Caycedo-Marulanda A, Jiang HY, Kohtakangas EL (2017) Transanal minimally invasive surgery for benign large rectal polyps and early malignant rectal cancers: experience and outcomes from the first Canadian centre to adopt the technique. Can J Surg 60:416–423
Atallah S, Albert M, Debeche-Adams T, Larach S (2013) Transanal minimally invasive surgery (TAMIS): applications beyond local excision. Tech Coloproctol 17:239–243
Funding
This study was supported by the First Hospital of Jilin University.
Author information
Authors and Affiliations
Contributions
Jinguo Wang was the lead investigator, drafted the article, and performed the surgery and revised the manuscript; Na Wang drafted the article, reviewed the literature, and revised the manuscript; Daguang Wang reviewed the literature, drafted the article, and made critical revisions to the manuscript; Weihua Tong was the assistant surgeon, drafted the article, collected the patient’s information, and gave the final approval of the manuscript.
Corresponding author
Ethics declarations
We have obtained Institutional Ethics approval and written informed consent to participate this study and to publish this paper from the patient.
Conflict of Interest
The authors declare that they have no conflict of interest.
There is no part of this article presented in conference proceedings. I hereby certify that this paper consists of original, unpublished work which is not under consideration for publication elsewhere.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(MP4 34463 kb).
Rights and permissions
About this article

Cite this article
Wang, N., Wang, D., Tong, W. et al. Minimally Invasive Treatment of a Completely Obstructed Rectal Anastomosis by Using a Transanal Plasmakinetic Resectoscope: a Case Report and Review of Literature. Indian J Surg 83, 1127–1133 (2021). https://doi.org/10.1007/s12262-020-02674-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12262-020-02674-1