
Abstract
Background
Needle knife papillotomy (NKP) and fistulotomy (NKF) are the two most commonly used rescue techniques for patients with difficult biliary cannulation (DBC). Anatomy of the major duodenal papillae (MDP) influences the optimal precut technique for biliary access. However, comparative studies of the success and safety of NKP and NKF based on the anatomy of MDP have been scarce.
Methods
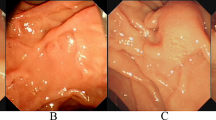
Patients with intact MDPs for therapeutic endoscopic retrograde cholangio-pancreatography (ERCP) in our center were enrolled. Early needle knife precuts were uniformly applied to patients with DBC. Difficult MDPs were classified into one of five types based on their endoscopic anatomy. Each type of MDP was allocated to NKP or NKF treatment. Patients with types 1 and 2 papillae always received NKF, 3 and 4 received NKP, and 5 could receive either. The safety and efficacy were analyzed between NKP and NKF, and among different types of MDPs.
Results
A total of 188 out of 1674 patients undergoing ERCP satisfied the criteria for early precutting: 75 patients were assigned to the NKP group and 113 to the NKF group. The total initial success rate of biliary cannulation (ISRBC) of the precut techniques (both NKP and NKF) for patients with DBC was 91.5%. The ISRBC of patients of the NKP group was similar to that of the NKF group (90.7% vs 92.0%, P > 0.05). The ISRBC of the patients in the swollen MDP subgroup (96.1%) was higher than that of patients in the distorted MDP subgroup (81.8%, P = 0.030). The total and specific complications of the patients of the NKP group were similar to those of the NKF group (P > 0.05).
Conclusions
NKP and NKF, as selected on the basis of MDP anatomy, are equally safe and highly efficient for patients with DBC to allow biliary cannulation. Patients with swollen MDPs had a higher ISRBC than patients with distorted MDPs. Selecting a precut method based on MDP anatomy is an effective and safe strategy for patients with DBC.


Similar content being viewed by others


References
Lopes L, Dinis-Ribeiro M, Rolanda C. Early precut fistulotomy for biliary access: time to change the paradigm of “the later, the better”? Gastrointest Endosc 2014;80:634–641. https://doi.org/10.1016/j.gie.2014.03.014.
Mariani A, Di Leo M, Giardullo N et al. Early precut sphincterotomy for difficult biliary access to reduce post-ERCP pancreatitis: a randomized trial. Endoscopy 2016;48:530–535. https://doi.org/10.1055/s-0042-102250.
Davee T, Garcia JA, Baron TH. Precut sphincterotomy for selective biliary duct cannulation during endoscopic retrograde cholangiopancreatography. Ann Gastroenterol 2012;25:291–302.
Chen J, Wan JH, Wu DY et al. Assessing quality of precut sphincterotomy in patients with difficult biliary access: an updated meta-analysis of randomized controlled trials. J Clin Gastroenterol 2018;52:573–578. https://doi.org/10.1097/MCG.0000000000001077.
Mammen A. Difficult biliary access: advanced cannulation and sphincterotomy technique. Gastrointest Endosc Clin N Am. 2015;25:619–630. https://doi.org/10.1016/j.giec.2015.06.007.
Gong B, Hao L, Bie L et al. Does precut technique improve selective bile duct cannulation or increase post-ERCP pancreatitis rate? A meta-analysis of randomized controlled trials. Surg Endosc. 2010;24:2670–2680. https://doi.org/10.1007/s00464-010-1033-y.
Lopes L, Dinis-Ribeiro M, Rolanda C. Safety and efficacy of precut needle-knife fistulotomy. Scand J Gastroenterol. 2014;49:759–765. https://doi.org/10.3109/00365521.2014.898085.
Testoni PA, Mariani A, Aabakken L et al. Papillary cannulation and sphincterotomy techniques at ERCP: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2016;48:657–683. https://doi.org/10.1055/s-0042-108641.
Katsinelos P, Lazaraki G, Chatzimavroudis G et al. The endoscopic morphology of major papillae influences the selected precut technique for biliary access. Gastrointest Endosc. 2015;81:1056. https://doi.org/10.1016/j.gie.2014.11.018.
Linder S, Söderlund C. Factors influencing the use of precut technique at endoscopic sphincterotomy. Hepatogastroenterology 2007;54:2192–2197.
Kawakami H, Kubota Y, Kawahata S et al. Transpapillary selective bile duct cannulation technique: review of Japanese randomized controlled trials since 2010 and an overview of clinical results in precut sphincterotomy since 2004. Dig Endosc 2016;28:77–95. https://doi.org/10.1111/den.12621.
Swan MP, Alexander S, Moss A et al. Needle knife sphincterotomy does not increase the risk of pancreatitis in patients with difficult biliary cannulation. Clin Gastroenterol Hepatol. 2013;11:e1. https://doi.org/10.1016/j.cgh.2012.12.017.
Cennamo V, Fuccio L, Repici A et al. Timing of precut procedure does not influence success rate and complications of ERCP procedure: a prospective randomized comparative study. Gastrointest Endosc. 2009;69:473–479. https://doi.org/10.1016/j.gie.2008.09.037.
Elmunzer BJ, Scheiman JM, Lehman GA et al. A randomized trial of rectal indomethacin to prevent post-ERCP pancreatitis. N Engl J Med. 2012;366:1414–1422. https://doi.org/10.1056/NEJMoa1111103.
Hong S, Qiwen B, Ying J et al. Body mass index and the risk and prognosis of acute pancreatitis: a meta-analysis. Eur J Gastroenterol Hepatol. 2011;23:1136–1143. https://doi.org/10.1097/MEG.0b013e32834b0e0e.
Cotton PB, Eisen GM, Aabakken L et al. A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc 2010;71:446–454. https://doi.org/10.1016/j.gie.2009.10.027.
Cotton PB, Lehman G, Vennes J et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc 1991;37:383–393. https://doi.org/10.1016/s0016-5107(91)70740-2.
Zhang QS, Han B, Xu JH et al. Needle-knife papillotomy and fistulotomy improved the treatment outcome of patients with difficult biliary cannulation. Surg Endosc. 2016;30:5506–5512. https://doi.org/10.1007/s00464-016-4914-x.
Mavrogiannis C, Liatsos C, Romanos A et al. Needle-knife fistulotomy versus needle-knife precut papillotomy for the treatment of common bile duct stones. Gastrointest Endosc. 1999;50:334–339.
Katsinelos P, Gkagkalis S, Chatzimavroudis G et al. Comparison of three types of precut technique to achieve common bile duct cannulation: a retrospective analysis of 274 cases. Dig Dis Sci. 2012;57:3286–3292. https://doi.org/10.1007/s10620-012-2271-8.
Horiuchi A, Nakayama Y, Kajiyama M et al. Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla. Clin Gastroenterol Hepatol. 2007;5:1113–1118.
Lee TH, Bang BW, Park SH et al. Precut fistulotomy for difficult biliary cannulation: is it a risky preference in relation to the experience of an endoscopist? Dig Dis Sci. 2011;56:1896–1903. https://doi.org/10.1007/s10620-010-1483-z.
Zheng M, Liu X, Li N, Li WZ. Emergency endoscopic needle-knife precut papillotomy in acute severe cholangitis resulting from impacted common bile duct stones at duodenal papilla. Dig Liver Dis 2017;50:267–270. https://doi.org/10.1016/j.dld.2017.11.015.
Maharshi S, Sharma SS. Early precut versus primary precut sphincterotomy to reduce post-ERCP pancreatitis: randomized controlled trial (with videos). Concise and informative title—primary precut to prevent post ERCP pancreatitis. Gastrointest Endosc 2021;93:586–593. https://doi.org/10.1016/j.gie.2020.06.064.
Fiocca F, Fanello G, Cereatti F et al. Early “shallow” needle-knife papillotomy and guidewire cannulation: an effective and safe approach to difficult papilla. Therap Adv Gastroenterol 2015;8:114–120. https://doi.org/10.1177/1756283X15576466.
Kylänpää L, Grönroos J, Grönroos J et al. Macroscopic appearance of the major duodenal papilla influences bile duct cannulation: a prospective multicenter study by the Scandinavian Association for Digestive Endoscopy Study Group for ERCP. Gastrointest Endosc 2019;90:957–963. https://doi.org/10.1016/j.gie.2019.07.014.
Lim JU, Joo KR, Cha JM et al. Early use of needle-knife fistulotomy is safe in situations where difficult biliary cannulation is expected. Dig Dis Sci 2012;57:1384–1390. https://doi.org/10.1007/s10620-012-2030-x.
Liao WC, Angsuwatcharakon P, Isayama H et al. International consensus recommendations for difficult biliary access. Gastrointest Endosc 2017;85:295–304. https://doi.org/10.1016/j.gie.2016.09.037.
ASGE Standards of Practice Committee, Anderson MA, Fisher L, Jain R et al. Complications of ERCP. Gastrointest Endosc 2012;75:467–473. https://doi.org/10.1016/j.gie.2011.07.010.
Tang Z, Yang Y, Yang Z et al. Early precut sphincterotomy does not increase the risk of adverse events for patients with difficult biliary access: a systematic review of randomized clinical trials with meta-analysis and trial sequential analysis. Medicine (Baltimore) 2018;97:e12213. https://doi.org/10.1097/MD.0000000000012213.
Navaneethan U, Konjeti R, Lourdusamy V et al. Precut sphincterotomy: efficacy for ductal access and the risk of adverse events. Gastrointest Endosc 2015;81:924–931. https://doi.org/10.1016/j.gie.2014.09.015.
Lee TH, Park SH, Yang JK et al. Is the isolated-tip needle-knife precut as effective as conventional precut fistulotomy in difficult biliary cannulation? Gut Liver. 2018;12:597–605. https://doi.org/10.5009/gnl17572.
Furuya CK, Sakai P, Marinho FRT et al. Papillary fistulotomy vs conventional cannulation for endoscopic biliary access: a prospective randomized trial. World J Gastroenterol. 2018;24:1803–1811. https://doi.org/10.3748/wjg.v24.i16.1803.
Acknowledgments
We thank LetPub (www.letpub.com) for its linguistic assistance during the preparation of this manuscript.
Funding
Funding was provided by Hongkou District Health Bureau (Grant No. ZK15-06).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zhang, Qs., Xu, Jh., Dong, Zq. et al. Success and Safety of Needle Knife Papillotomy and Fistulotomy Based on Papillary Anatomy: A Prospective Controlled Trial. Dig Dis Sci 67, 1901–1909 (2022). https://doi.org/10.1007/s10620-021-06983-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-021-06983-7