
Abstract
Background and Aims
Difficult cannulation is a well known risk for post-ERCP pancreatitis. This study evaluated the outcomes of needle-knife fistulotomy (NKF) used prior to being faced with difficult biliary cannulation.
Methods
Patients who underwent endoscopic retrograde cholangiopancreatography (ERCP) for the purpose of biliary endotherapy between January 2007 and December 2008 were eligible for this study; 218 patients were recruited. Biliary cannulation was performed only by a standard catheter or a pull type papillotome, without wire-guided assistance in all patients. If selective cannulation was not achieved within five cannulation attempts, NKF was performed, and the results were compared with the easy cannulation group that succeeded biliary cannulation within five attempts.
Results
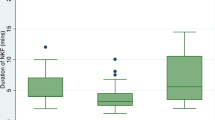
Needle-knife fistulotomy (NKF) was performed in 72 (33.0%) of the 218 patients. The total success rate of the ERCP was 98.2% (214/218), and for the NKF group the success rate was 94.4% (68/72). The rate of complications in patients with NKF did not increase compared to patients in the easy cannulation group (P > 0.05): 4.2% (3/72) versus 3.4% (5/146) for acute pancreatitis, 6.9% (5/72) versus 6.8% (10/146) for bleeding, and 1.4% (1/72) versus 0% (0/146) for perforation, respectively.
Conclusions
Our results suggest that the use of NKF for biliary cannulation might be safe and effective. Therefore, in experienced hands, early use of NKF might be recommended.

Similar content being viewed by others


References
Bailey AA, Bourke MJ, Kaffes AJ, et al. Needle-knife sphincterotomy: factors predicting its use and the relationship with post-ERCP pancreatitis (with video). Gastrointest Endosc. 2010;71:266–271.
Fukatsu H, Kawamoto H, Harada R, et al. Quantitative assessment of technical proficiency in performing needle-knife precut papillotomy. Surg Endosc. 2009;23:2066–2072.
Khatibian M, Sotoudehmanesh R, Ali-Asgari A, et al. Needle-knife fistulotomy versus standard method for cannulation of common bile duct: a randomized controlled trial. Arch Iran Med. 2008;11:16–20.
Weber A, Roesch T, Pointner S, et al. Transpancreatic precut sphincterotomy for cannulation of inaccessible common bile duct: a safe and successful technique. Pancreas. 2008;36:187–191.
Parlak E, Cicek B, Disibeyaz S, et al. Early decision for precut sphincterotomy: is it a risky preference? Dig Dis Sci. 2007;52:845–851.
Laohavichitra K, Akaraviputh T, Methasate A, et al. Comparison of early pre-cutting versus standard technique for biliary cannulation in endoscopic retrograde cholangiopancreatography: a personal experience. World J Gastroenterol. 2007;13:3734–3737.
Zhou PH, Yao LQ, Xu MD, et al. Application of needle-knife in difficult biliary cannulation for ERCP. Hepatobiliary Pancreat Dis Int. 2006;5:590–594.
Kaffes AJ, Sriram PV, Rao GV, et al. Early institution of pre-cutting for difficult biliary cannulation: a prospective study comparing conventional versus a modified technique. Gastrointest Endosc. 2005;62:669–674.
Tang SJ, Haber GB, Kortan P, et al. Precut papillotomy versus persistence in difficult biliary cannulation: a prospective randomized trial. Endoscopy. 2005;37:58–65.
Abu-Hamda EM, Baron TH, Simmons DT, et al. A retrospective comparison of outcomes using three different precut needle knife techniques for biliary cannulation. J Clin Gastroenterol. 2005;39:717–721.
Catalano MF, Linder JD, Geenen JE. Endoscopic transpancreatic papillary septotomy for inaccessible obstructed bile ducts: comparison with standard pre-cut papillotomy. Gastrointest Endosc. 2004;60:557–561.
Mavrogiannis C, Liatsos C, Romanos A, et al. Needle-knife fistulotomy versus needle-knife precut papillotomy for the treatment of common bile duct stones. Gastrointest Endosc. 1999;50:334–339.
Kasmin FE, Cohen D, Batra S, et al. Needle-knife sphincterotomy in a tertiary referral center: efficacy and complications. Gastrointest Endosc. 1996;44:48–53.
Freeman ML, Nelson DB, Sherman S, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 1996;335:909–918.
Sherman S, Ruffolo T, Hawes RH, et al. Complications of endoscopic sphincterotomy. Gastroenterology. 1991;101:1068–1075.
Cotton PB. Needle-knife precut sphincterotomy: the devil is in the indications. Endoscopy. 1997;29:888.
Dhir V, Mohandas KM. Is precut papillotomy guilty as accused? Gastrointest Endosc. 1999;50:143.
Cotton PB. Precut sphincterotomy: a risky technique for the experts only. Gastrointest Endosc. 1989;35:578–579.
Kim DI, Kim MH, Lee SK, et al. Risk factors for recurrence of primary bile duct stones after endoscopic biliary sphincterotomy. Gastrointest Endosc. 2001;54:42–48.
Tytgat GN. The Sydney system: endoscopic division. Endoscopic appearances in gastritis/duodenitis. J Gastroenterol Hepatol. 1991;6:223–234.
Cotton PB, Lehman G, Vennes JA, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc. 1991;37:383–393.
Rollhauser C, Johnson M, Al-Kawas FH. Needle-knife papillotomy: a helpful and safe adjunct to endoscopic retrograde cholangiopancreatography in a selected population. Endoscopy. 1998;30:691–696.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lim, J.U., Joo, K.R., Cha, J.M. et al. Early Use of Needle-Knife Fistulotomy Is Safe in Situations Where Difficult Biliary Cannulation Is Expected. Dig Dis Sci 57, 1384–1390 (2012). https://doi.org/10.1007/s10620-012-2030-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-012-2030-x