
Abstract
Background
The 2012 consensus guideline on intraductal papillary mucinous neoplasm of the pancreas (IPMN) described a three-stage criteria involving main pancreatic duct (MPD) size with definitions of malignancy relevant for treatment decisions. Re-evaluation and simplification of this classification for clinicians are warranted.
Methods
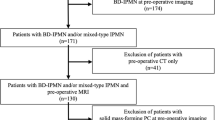
Data from the Seoul National University Hospital of 375 consecutive patients with pathology-confirmed IPMN after surgery were analyzed. The association between clinicopathologic characteristics of IPMN and MPD size was assessed. The cut-off value of MPD size for a current definition of malignancy prediction was calculated.
Results
Diagnostic accuracy for malignancy was highest when the cut-off value of MPD size was 7 mm (area under the curve = 0.7126). Dichotomizing IPMN into MPD ≤7 mm versus MPD >7 mm, patient age (p = 0.039), sex (p = 0.001), presence of mural nodule (p < 0.001), and invasiveness risk (13.2 vs. 39.8 %, p < 0.001) resulted in significantly different results. Mural nodule-negative patients with MPD >7 mm had a significantly lower 5-year survival rate than those with MPD ≤7 mm (78.4 vs. 91.4 %, p = 0.006). Among patients with MPD size ≤7 mm, elevated serum CA 19-9 and mural nodule were independent risk factors of malignancy. Patients with MPD size ≤7 mm without these risk factors had malignancy risk of 2.6 %.
Conclusion
Using the definition of malignancy provided in the 2012 guideline, the MPD size >7 mm criterion was statistically driven. The current morphologic classification of IPMN can be simplified as branch-duct-predominant IPMN (MPD ≤7 mm)’ and main-duct-predominant IPMN (MPD >7 mm). Patients who are determined to have main-duct-predominant IPMN and branch-duct-predominant IPMN with elevated serum CA 19-9 or mural nodule are recommended to undergo surgical treatment.


Similar content being viewed by others

References
Tanaka M, Chari S, Adsay V et al (2006) International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology 6:17–32
Tanaka M, Fernandez-Del Castillo C, Adsay V et al (2012) International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 12:183–197
Salvia R, Fernández-del Castillo C, Bassi C et al (2004) Main-duct intraductal papillary mucinous neoplasms of the pancreas. Ann Surg 239:678–687
Shimizu Y, Yamaue H, Maguchi H et al (2013) Predictors of malignancy in intraductal papillary mucinous neoplasm of the pancreas: analysis of 310 pancreatic resection patients at multiple high-volume centers. Pancreas 42:883–888
Anand N, Sampath K, Wu BU (2013) Cyst features and risk of malignancy in intraductal papillary mucinous neoplasms of the pancreas: a meta-analysis. Clin Gastroenterol Hepatol 11:913–921
Kawamoto S, Lawler LP, Horton KM et al (2006) MDCT of intraductal papillary mucinous neoplasm of the pancreas: evaluation of features predictive of invasive carcinoma. AJR Am J Roentgenol 186:687–695
Bournet B, Kirzin S, Carrere N et al (2009) Clinical fate of branch duct and mixed forms of intraductal papillary mucinous neoplasia of the pancreas. J Gastroenterol Hepatol 24:1211–1217
Sahani DV, Kadavigere R, Blake M et al (2006) Intraductal papillary mucinous neoplasm of pancreas: multi-detector row CT with 2D curved reformations—correlation with MRCP. Radiology 238:560–569
Akita H, Takeda Y, Hoshino H et al (2011) Mural nodule in branch duct-type intraductal papillary mucinous neoplasms of the pancreas is a marker of malignant transformation and indication for surgery. Am J Surg 202:214–219
Schmidt CM, White PB, Waters JA et al (2007) Intraductal papillary mucinous neoplasms: predictors of malignant and invasive pathology. Ann Surg 246:644–651; discussion 651–644
Waters JA, Schmidt CM, Pinchot JW et al (2008) CT vs MRCP: optimal classification of IPMN type and extent. J Gastrointest Surg 12:101–109
Kang MJ, Jang JY, Kim SJ et al (2011) Cyst growth rate predicts malignancy in patients with branch duct intraductal papillary mucinous neoplasms. Clin Gastroenterol Hepatol 9:87–93
Hwang DW, Jang JY, Lee SE et al (2012) Clinicopathologic analysis of surgically proven intraductal papillary mucinous neoplasms of the pancreas in SNUH: a 15-year experience at a single academic institution. Langenbecks Arch Surg 397:93–102
Sadakari Y, Ienaga J, Kobayashi K et al (2010) Cyst size indicates malignant transformation in branch duct intraductal papillary mucinous neoplasm of the pancreas without mural nodules. Pancreas 39:232–236
Lee CJ, Scheiman J, Anderson MA et al (2008) Risk of malignancy in resected cystic tumors of the pancreas ≤3 cm in size: is it safe to observe asymptomatic patients? A multi-institutional report. J Gastrointest Surg 12:234–242
Irie H, Honda H, Aibe H et al (2000) MR cholangiopancreatographic differentiation of benign and malignant intraductal mucin-producing tumors of the pancreas. AJR Am J Roentgenol 174:1403–1408
Nakagohri T, Kinoshita T, Konishi M et al (2007) Surgical outcome of intraductal papillary mucinous neoplasms of the pancreas. Ann Surg Oncol 14:3174–3180
Mimura T, Masuda A, Matsumoto I et al (2010) Predictors of malignant intraductal papillary mucinous neoplasm of the pancreas. J Clin Gastroenterol 44:e224–e229
Sugiyama M, Izumisato Y, Abe N et al (2003) Predictive factors for malignancy in intraductal papillary-mucinous tumours of the pancreas. Br J Surg 90:1244–1249
Nara S, Onaya H, Hiraoka N et al (2009) Preoperative evaluation of invasive and noninvasive intraductal papillary-mucinous neoplasms of the pancreas: clinical, radiological, and pathological analysis of 123 cases. Pancreas 38:8–16
Nagai K, Doi R, Doi R, Ito T et al (2009) Single-institution validation of the international consensus guidelines for treatment of branch duct intraductal papillary mucinous neoplasms of the pancreas. J Hepatobiliary Pancreat Surg 16:353–358
Kim SC, Park KT, Lee YJ et al (2008) Intraductal papillary mucinous neoplasm of the pancreas: clinical characteristics and treatment outcomes of 118 consecutive patients from a single center. J Hepatobiliary Pancreat Surg 15:183–188
Adsay NV, Kloppel G, Fukushima N et al (2010) Intraductal neoplasms of the pancreas. In: Bosman FT, Carneiro F, Hruban RH (eds) WHO classification of tumours of the digestive system. IARC Press, Lyon
Ohno E, Hirooka Y, Itoh A et al (2009) Intraductal papillary mucinous neoplasms of the pancreas: differentiation of malignant and benign tumors by endoscopic ultrasonography findings of mural nodules. Ann Surg 249:628–634
Einstein DM, Singer AA, Chilcote WA et al (1991) Abdominal lymphadenopathy: spectrum of CT findings. Radiographics 11:457–472
Arikawa S, Uchida M, Uozumi J et al (2011) Utility of multidetector row CT in diagnosing branch duct IPMNs of the pancreas compared with MR cholangiopancreatography and endoscopic ultrasonography. Kurume Med J 57:91–100
Serikawa M, Sasaki T, Fujimoto Y et al (2006) Management of intraductal papillary-mucinous neoplasm of the pancreas: treatment strategy based on morphologic classification. J Clin Gastroenterol 40:856–862
Levy P, Jouannaud V, O’Toole D et al (2006) Natural history of intraductal papillary mucinous tumors of the pancreas: actuarial risk of malignancy. Clin Gastroenterol Hepatol 4:460–468
Crippa S, Fernandez-Del Castillo C, Salvia R et al (2010) Mucin-producing neoplasms of the pancreas: an analysis of distinguishing clinical and epidemiologic characteristics. Clin Gastroenterol Hepatol 8:213–219
Takano S, Fukasawa M, Maekawa S et al (2014) Deep sequencing of cancer-related genes revealed GNAS mutations to be associated with intraductal papillary mucinous neoplasms and its main pancreatic duct dilation. PLoS ONE 9:e98718
Dal Molin M, Matthaei H, Wu J et al (2013) Clinicopathological correlates of activating GNAS mutations in intraductal papillary mucinous neoplasm (IPMN) of the pancreas. Ann Surg Oncol 20:3802–3808
He J, Cameron JL, Ahuja N et al (2013) Is it necessary to follow patients after resection of a benign pancreatic intraductal papillary mucinous neoplasm? J Am Coll Surg 216:657–665; discussion 665–657
Kang MJ, Jang JY, Lee KB et al (2013) Long-term prospective cohort study of patients undergoing pancreatectomy for intraductal papillary mucinous neoplasm of the pancreas: implications for postoperative surveillance. Ann Surg 260:356–363
Acknowledgments
This study was supported by a grant of the Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (No. HI14C2640).
Conflicts of interest
The authors disclose no conflicts.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplement Figure 1
Maximum balanced accuracy obtained when the cut-off value of 0.24 is used as the prediction probability for malignancy (TIFF 71 kb)
Supplement Figure 2
Sensitivity, specificity and balanced accuracy of malignancy prediction at the main duct diameter of 7 mm were 53.8, 80.7 and 67.2 %, respectively (TIFF 63 kb)
Rights and permissions
About this article

Cite this article
Kang, M.J., Jang, JY., Lee, S. et al. Clinicopathological Meaning of Size of Main-Duct Dilatation in Intraductal Papillary Mucinous Neoplasm of Pancreas: Proposal of a Simplified Morphological Classification Based on the Investigation on the Size of Main Pancreatic Duct. World J Surg 39, 2006–2013 (2015). https://doi.org/10.1007/s00268-015-3062-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-015-3062-0