
Abstract
Recent international consensus guidelines propose that cystic pancreatic tumors less than 3 cm in size in asymptomatic patients with no radiographic features concerning for malignancy are safe to observe; however, there is little published data to support this recommendation. The purpose of this study was to determine the prevalence of malignancy in this group of patients using pancreatic resection databases from five high-volume pancreatic centers to assess the appropriateness of these guidelines. All pancreatic resections performed for cystic neoplasms ≤3 cm in size were evaluated over the time period of 1998–2006. One hundred sixty-six cases were identified, and the clinical, radiographic, and pathological data were reviewed. The correlation with age, gender, and symptoms (abdominal pain, nausea and vomiting, jaundice, presence of pancreatitis, unexplained weight loss, and anorexia), radiographic features suggestive of malignancy by either computed tomography, magnetic resonance imaging, or endoscopic ultrasound (presence of solid component, lymphadenopathy, or dilated main pancreatic duct or common bile duct), and the presence of malignancy was assessed using univariate and multivariate analysis. Among the 166 pancreatic resections for cystic pancreatic tumors ≤3 cm, 135 cases were benign [38 serous cystadenomas, 35 mucinous cystic neoplasms, 60 intraductal papillary mucinous neoplasms (IPMN), 1 cystic papillary tumor, and 1 cystic islet cell tumor], whereas 31 cases were malignant (14 mucinous cystic adenocarcinomas and 13 invasive carcinomas and 4 in situ carcinomas arising in the setting of IPMN). A greater incidence of cystic neoplasms was seen in female patients (99/166, 60%). Gender was a predictor of malignant pathology, with male patients having a higher incidence of malignancy (19/67, 28%) compared to female patients (12/99, 12%; p < 0.02). Older age was associated with malignancy (mean age 67 years in patients with malignant disease vs 62 years in patients with benign lesions (p < 0.05). A majority of the patients with malignancy were symptomatic (28/31, 90%). Symptoms that correlated with malignancy included jaundice (p < 0.001), weight loss (p < 0.003), and anorexia (p < 0.05). Radiographic features that correlated with malignancy were presence of a solid component (p < 0.0001), main pancreatic duct dilation (p = 0.002), common bile duct dilation (p < 0.001), and lymphadenopathy (p < 0.002). Twenty-seven of 31(87%) patients with malignant lesions had at least one radiographic feature concerning for malignancy. Forty-five patients (27%) were identified as having asymptomatic cystic neoplasms. All but three (6.6%) of the patients in this group had benign disease. Of the patients that had no symptoms and no radiographic features, 1 out of 30 (3.3%) had malignancy (carcinoma in situ arising in a side branch IPMN). Malignancy in cystic neoplasms ≤3 cm in size was associated with older age, male gender, presence of symptoms (jaundice, weight loss, and anorexia), and presence of concerning radiographic features (solid component, main pancreatic duct dilation, common bile duct dilation, and lymphadenopathy). Among asymptomatic patients that displayed no discernable radiographic features suggestive of malignancy who underwent resection, the incidence of occult malignancy was 3.3%. This study suggests that a group of patients with small cystic pancreatic neoplasms who have low risk of malignancy can be identified, and selective resection of these lesions may be appropriate.
Similar content being viewed by others


References
Brugge WR, Lauwers GY, Shani D, Fernandez-del Castillo C, Warshaw AL. Cystic neoplams of the pancreas. N Engl J Med. 2004;351:1218–1226.
Tanaka M, Chari S, Adsay V, Fernandez-del Castillo C, et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology. 2006;6:17–32.
Fernandez-del Castillo C, Targarona J, Thayer SP, Rattner dW, Brugge WR, Warshaw AL. Incidental pancreatic cysts; clinicopathologic characteristics and comparison with symptomatic patients. Arch Surg. 2003;138:427–434.
Warshaw AL, Compton CC, Lewandowski K, et al. Cystic tumors of the pancreas: new clinical, radiologic, and pathologic observations in 67 patients. Ann Surg. 1990;212:432–443.
Meyer W, Kohler J, Gebhardt C. Cystic neoplasms of the pancreas: Cystadenomas and cystadenocarcinomas. Langenbeck’s Arch Surg. 1999;384:44–49.
Sarr MG, Carpenter HA, Prabhakar LP, et al. Clinical and pathologic correlation of 84 mucinous cystic neoplasms of the pancreas. Ann Surg. 2003;138:427–434.
Sohn TA, Yeo CJ, Cameron JL, et al. Intraductal papillary mucinous neoplasms of the pancreas: An increasingly recognized clinicopathalogic entity. Ann Surg. 2001;234:313–322.
Spinelli KS, Fromwiller E, Daniel RA, et al. Cystic pancreatic neoplasms—Observe or operate? Ann Surg. 2004;239:651–657.
Allen PJ, D’Angelica M, Gonen M, Jaques DP, Coit DG, et al. A selective approach to the resection of cystic lesions of the pancreas: Results from 539 consecutive patients. Ann Surg. 2006;244:572–582.
Winter JM, Cameron JL, Lillemoe KD, et al. Periampullary and pancreatic incidentaloma: A single institution’s experience with an increasingly common diagnosis. Ann Surg. 2006;243:673–680.
Talamini MA, Pitt HA, Hruban RH, et al. Spectrum of cystic tumors of the pancreas. Am J Surg. 1992;163:117–124.
Curry CA, Eng J, Horton KM. CT of primary cystic pancreatic neoplasms: Can CT be used for patient triage and treatment? Am J Roentgenol. 200;175:99–103.
Brugge WB, Lewandroski K, Lee-Lewandroski E, et al. Diagnosis of pancreatic cystic neoplasms: a report of the Cooperative Pancreatic Cyst Study. Gastroenterology. 2004;126:1330–1336.
Khalid A, McGrath KM, Zahid M, et al. The role of pancreatic cyst fluid molecular analysis in predicting cyst pathology. Clin Gastroenterl Hepatol. 2005;3:967–973.
Horvath KD, Chabot JA. An aggressive resectional approach to cystic neoplasms of the pancreas. Am J Surg. 1999;178:269–274.
Hardacre JM, McGee MF, Sellato TA, Schulak JA. An aggressive surgical approach is warranted in the management of cystic pancreatic neoplasms. Am J Surg. 2007;193:374–379.
Birkmeyer JD, Warshaw AL, Finlayson SR, et al. Relationship between hospital volume and late survival after pancreaticoduodenectomy. Surgery. 1999;126:178–183.
Walsh RM, Vogt DP, Henderson JM, et al. Natural history of indeterminate pancreatic cysts. Surgery.. 2005;138:665–670.
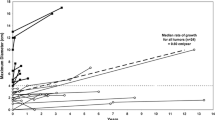
Tseng JF, Warshaw AL, Shani DV, et al. Serous cystadenoma of the pancreas: Tumor growth rates and recommendations for treatment. Ann Surg. 2005;242:413–419.
Moesinger RC, Talamini MA, Hruban RH, et al. Large cystic pancreatic neoplasm: Pathology, resectability, and outcome. Ann Surg Oncol. 1999;6:682–691.
Wiseneauer CA, Schmidt CM, Cummings OW, Yiannoutsos CT, et al. Preoperative predictors of malignancy in pancreatic intraductal papillary mucinous neoplasms. Arch Surg. 2003;138:610–618.
Sahani DV, Saokar A, Hahn PF, Brugge WR, et al. Pancreatic cysts 3 cm or smaller: How aggressive should treatment be? Radiology. 2006;238:912–919.
Sarr MG, Murr M, Smyrk TC, et al. Primary cystic neoplasms of the pancreas: neoplastic disorders of emerging importance—Current state-of-the art and unanswered questions. J Gastrointes Surg. 2003;7:417–28.
Chari ST, Yadav D, Smyrk TC, et al. Study of recurrence after surgical resection of intraductal papillary mucinous neoplasm of the pancreas. Gastroenterology. 2002;123:1500–1507.
Allen PJ, Jaques DP, D’Angelica M, et al. Cystic lesions of the pancreas: Selection criteria for operative and nonoperative management in 209 patients. J Gastrointes Surg. 2003;7:970–977.
Procacci C, Carbognin G, Accordini S, et al. CT features of malignant mucinous cystic tumors of the pancreas. Eur Radiol. 2001;11:1626–1630.
Author information
Authors and Affiliations
Corresponding author
Additional information
Discussion
Jennifer F. Tseng, M.D. (Worcester, MA): I want to congratulate Dr. Lee, Dr. Simeone, and colleagues from five institutions for their work putting together a multi-institution series on cystic tumors. Dr. Lee, thank you for an excellent presentation and for allowing me to review the manuscript. I have two questions and a comment.
First, in contrast to the existing literature, you found in your series that side-branch IPMNs did not have a decreased risk of malignancy compared with main duct variants. Why do you think this is, and do you think it reflects the heterogeneous nature of your series?
Second, it is interesting that more men than women have malignancy at OR, Dr. Fernandez and I found in our series on serous cystadenomas that men had larger lesions and also presented at a later age, suggesting a delay in diagnosis. Do you think this is at play in your series; were men older?
The final question is your manuscript refers to the role of EUS. How did you define the sensitivity and specificity and accuracy of the cytology? Was it the pathologist calling it malignant? Were biopsies that had no epithelium present and thus were not diagnostic of malignancy termed benign or indeterminant, and how was the presence of mucin considered in the determination for operation? Do size and symptoms now trump mucin in your view in terms of a determination of whether this patient needs to go to the OR?
And finally my comment is there is an unspoken elephant in the room every time one of us presents one of these surgical series. We present patients that have already had the gold standard of operation and operative pathology and try to extrapolate backwards to the patients that we are truly interested in, and the results of these tests we are trying to evaluate, such as radiology and EUS and biopsy and fluid characteristics, in part determine who actually gets an operation. Therefore, our evaluation of these tests is biased by the fact that we do not have surgical pathology on everyone who gets the tests. The population we are truly interested in is, however, patients who have cystic tumors in the general population. These two populations may be very different. On the one hand, surgical populations may be enriched for patients with malignant outcomes. On the other hand, as we have no knowledge of patients that never came to the operating room, we do not know what their outcomes were. And the only way, in my opinion, to answer these questions, which plague all of our surgical series, is to have prospective studies of cystic lesions and other lesions of the pancreas with broad-based inclusion criteria that predate considerably the decision for operation.
Thank you very much.
Cheong Lee, M.D. (Ann Arbor, MI): I agree with you wholeheartedly about the critical need for a prospective analysis to determine the best treatment for these lesions. To answer your first question in terms of our findings between side branch and main branch IPMN and why the relative risks of malignancy were almost equivocal, whereas the literature reports that main duct malignant lesions are more likely, this is likely due to the limited sample size in our study. However, we currently do not know the natural history of these lesions. We do not fully understand their biologic behavior due to the lack of a prospective series, as Dr. Tseng has mentioned. However, I do think that size does matter in these lesions, and regardless of tumor type, there is probably an overall lower incidence of malignancy when a lesion is smaller than 3 cm.
To answer your second question as to why there is a greater proportion of cancer in men, that is a very interesting point. We were surprised to find this in our study as well. I think indeed it could reflect a later diagnosis in men, but there could also be some unknown biological reason that these neoplasms behave differently in men. That calls for other studies to study that fact.
The third question you had was about the definition of what was called malignancy by cytopathologists. I agree, this is one of the limitations in our study in that there were variable criteria for the diagnosis of malignancy by cytopathologists between institutions. Some cytopathologists were conservative in their call for malignant atypia found in the cytologist’s specimen. However, we noted the key words in the readings, such as high grade, atypical glandular cells, concern for adenocarcinoma, mucinous epithelium, and concern for malignancy. All these key words we noted as being positive for malignancy. Now, the cytology was considered benign when there was no mention of atypia and the lesions were considered low grade.
Lygia Stewart, M.D. (San Francisco, CA): How many of the patients that had mucin positivity and an elevated CEA greater than 192 had malignancy or did not have malignancy, and did you check for mucin? You did not mention it in your talk.
Dr. Lee: We did not specifically look for mucin, but in terms of the CEA level and cytology, we found there were a total of 15 patients who had a positive cytology and CEA levels for both the mucin-producing tumor and malignancy.
Mark P. Callery, M.D. (Boston, MA): What should you do with a 48-year-old woman with a 2.8-cm asymptomatic, except for anxiety, cyst in her uncinate process whose father passed away from pancreatic cancer at age 60?
Dr. Lee: Thank you. That is the key question.
Keith D. Lillemoe, M.D. (Indianapolis, IN): You gave 3.3% for your total percentage of asymptomatic tumors less than 3 cm. Can you give an actual percentage for those that you were able to prove that were mucin-producing tumors? The one cancer was in a mucin tumor. So what was your percentage for asymptomatic mucin-producing tumors?
Dr. Lee: There were three. All the premalignant types, there were three in the asymptomatic patients. So 6.6% of those patients had malignancy.
Dr. Lillemoe: No, no, you did not answer my question. How many asymptomatic less than 3-cm mucin-producing tumors did you have?
Dr. Lee: There was a higher percentage of mucin-producing tumors overall. Actually 79% of the tumors that we found that were less than 3 cm were mucin-producing tumors.
Dr. Lillemoe: Again, my question is, what is the incidence of cancer in asymptomatic mucinous-producing tumors than 3 cm in size?
Dr. Lee: It is 19%.
Dr. Lillemoe: Which is a lot higher than the mortality of a pancreaticoduodenectomy.
Dr. Lee: Correct.
Rights and permissions
About this article
Cite this article
Lee, C.J., Scheiman, J., Anderson, M.A. et al. Risk of Malignancy in Resected Cystic Tumors of the Pancreas ≤3 cm in Size: Is it Safe to Observe Asymptomatic Patients? A Multi-institutional Report. J Gastrointest Surg 12, 234–242 (2008). https://doi.org/10.1007/s11605-007-0381-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-007-0381-y