
Abstract
Background
Low fraction of inspired oxygen (FIO2) reduces the atelectasis area during anesthesia induction. However, atelectasis may occur during laryngoscopy and endotracheal intubation because lungs can collapse within a fraction of a second. We assessed the effects of ventilation with 100 and 40 % oxygen on functional residual capacity (FRC) in patients undergoing general anesthesia.
Methods
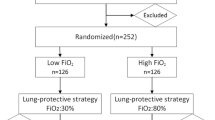
Twenty patients scheduled for elective open abdominal surgery were randomized into 40 % oxygen (GI, n = 10) and 100 % oxygen (GII, n = 10) groups and FRC was measured. Preoxygenation and mask ventilation with 40 and 100 % oxygen were used in GI and GII, respectively. In both groups, 40 % oxygen was used for anesthesia maintenance after intubation. Bilateral lung ventilation was performed with volume guarantee and low tidal volume (7 ml/kg predicted body weight) using bilevel airway pressure. We measured FRC and blood gas in all patients during preoxygenation, after intubation, and during surgery.
Results
FRC decreased from during preoxygenation (GI 2380 ml, GII 2313 ml) to after intubation (GI 1569 ml, GII 1586 ml) and significantly decreased during surgery (GI 1338 ml, GII 1417 ml) (P < 0.05). PaO2/FIO2 decreased from during preoxygenation (GI 419 mmHg, GII 427 mmHg) to after intubation (GI 381 mmHg, GII 351 mmHg) and significantly decreased during surgery (GI 333 mmHg, GII 291 mmHg) (P < 0.05). No significant differences were found between the groups in both parameters.
Conclusions
FRC significantly decreased from the awake state to surgery in both groups. FRC was not influenced by FIO2 elevation at anesthesia induction.



Similar content being viewed by others


References
Rothen HU, Sporre B, Engberg G, Wegenius G, Reber A, Hedenstierna G. Prevention of atelectasis during general anaesthesia. Lancet. 1995;345:1387–91.
Edmark L, Kostova-Aherdan K, Enlund M, Hedenstierna G. Optimal oxygen concentration during induction of general anesthesia. Anesthesiology. 2003;98:28–33.
Tanoubi I, Drolet P, Donati F. Optimizing preoxygenation in adults. Can J Anaesth. 2009;56:449–66.
Wahba RW. Perioperative functional residual capacity. Can J Anaesth. 1991;38:384–400.
Hedenstierna G, Löfström B, Lundh R. Thoracic gas volume and chest-abdomen dimensions during anesthesia and muscle paralysis. Anesthesiology. 1981;55:499–506.
Olegård C, Söndergaard S, Houltz E, Lundin S, Stenqvist O. Estimation of functional residual capacity at the bedside using standard monitoring equipment: a modified nitrogen washout/washin technique requiring a small change of the inspired oxygen fraction. Anesth Analg. 2005;101:206–12.
Choncholas G, Sondergaard S, Heinonen E. Validation and clinical application of a first order step response equation for nitrogen clearance during FRC measurement. J Clin Monit Comput. 2008;22:1–9.
Dixon BJ, Dixon JB, Carden JR, Burn AJ, Schachter LM, Playfair JM, Laurie CP, O’Brien PE. Preoxygenation is more effective in the 25 degrees head-up position than in the supine position in severely obese patients: a randomized controlled study. Anesthesiology. 2005;102:1110–5.
Don HF, Wahba M, Cuadrado L, Kelkar K. The effects of anesthesia and 100 percent oxygen on the functional residual capacity of the lungs. Anesthesiology. 1970;32:521–9.
Hewlett AM, Hulands GH, Nunn JF, Milledge JS. Functional residual capacity during anaesthesia III: artificial ventilation. Br J Anaesth. 1974;46:495–503.
Satoh D, Kurosawa S, Kirino W, Wagatsuma T, Ejima Y, Yoshida A, Toyama H, Nagaya K. Impact of changes of positive end-expiratory pressure on functional residual capacity at low tidal volume ventilation during general anesthesia. J Anesth. 2012;26:664–9.
Rusca M, Proietti S, Schnyder P, Fraccarolo P, Hendenstierna G, Spahn DR, Magnusson L. Prevention of atelectasis formation during induction of general anesthesia. Anesth Analg. 2003;97:1835–9.
Tusman G, Böhm SH. Prevention and reversal of lung collapse during the intra-operative period. Best Pract Res Clin Anaesthesiol. 2010;24:183–97.
Martínez G, Cruz P. Atelectasis in general anesthesia and alveolar recruitment strategies. Rev Esp Anestesiol Reanim. 2008;55:493–503.
Futier E, Constantin JM, Pelosi P, Chanques G, Kwiatkoskwi F, Jaber S, Bazin JE. Intraoperative recruitment maneuver reverses detrimental pneumoperitoneum-induced respiratory effects in healthy weight and obese patients undergoing laparoscopy. Anesthesiology. 2010;113:1310–9.
Hedenstierna G, Edmark L. Mechanisms of atelectasis in the perioperative period. Best Pract Res Clin Anaesthesiol. 2010;24:157–69.
Bikker IG, Scohy TV, Bogers JC, Bakker J, Gommers D, et al. Measurement of end-expiratory lung volume in intubated children without interruption of mechanical ventilation. Intensive Care Med. 2009;35:1749–53.
Acknowledgments
Support was provided solely from institutional and/or departmental sources.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Kanaya, A., Satoh, D. & Kurosawa, S. Higher fraction of inspired oxygen in anesthesia induction does not affect functional residual capacity reduction after intubation: a comparative study of higher and lower oxygen concentration. J Anesth 27, 385–389 (2013). https://doi.org/10.1007/s00540-012-1547-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-012-1547-7