
Abstract
Background
Cancer development is associated with deregulated microRNA (miRNA) in body fluids including serum, plasma, and bronchoalveolar lavage (BAL). Early diagnosis and early treatment of lung cancer improve survival and response to treatment. So, finding an easy detectable biomarker is crucially important to improve the disease outcome. So, we analyzed the differential expression of miRNA using microarray both in serum and BAL of 37 non-small cell lung cancer (NSCLC) patients and 30 healthy control subjects (15 non-smokers and 15 smokers).
Results
A total of 32 miRNAs were significantly differentially expressed in serum of NSCLC patients versus controls (13 up-regulated and 19 down-regulated), whereas 14 miRNAs were significantly differentially expressed in BAL of NSCLC patients relative to control (12 upregulated and 2 downregulated). The accuracy of MiRNAs to detect lung cancer patients versus control was 94.3% with a specificity of 97.8% and a sensitivity of 92.3%.
Conclusions
Expression of miRNAs is specific in both serum and BAL of NSCLC patients, indicating that they might be considered easy diagnostic biomarkers for early lung cancer detection.
Similar content being viewed by others


Background
Lung cancer occurs when the body loses control over the continuously proliferating cells of the lung [1]. Lung cancer is responsible for more deaths in males than any other cancers; while its contribution to female cancer mortality is limited to the more developed countries [2]. The type of lung cancer and the stage at presentation are the two most important factors determining the 5-year survival [3]. Unfortunately, a great proportion of lung cancer patients present only with late metastases [4]. Dysregulated microRNAs (miRNA) have been detected in patients with cancer [5].
MiRNAs are a group of tiny, single-stranded, non-coding RNA molecules. They contribute mainly by downregulation of gene expression after completing transcription and organization of many processes on cellular levels. These processes include growth, differentiation, metabolism, and apoptosis [6, 7]. The source of circulating miRNAs is leakage from body cells including malignant cells [8]. They are resistant to digestion by RNase and other extreme conditions including boiling, prolonged storage, and freezing making them one of the most important biological markers [9].
Our study aimed to study the differential miRNA expression profiles in NSCLC Egyptian patients. We investigated whether their expression in serum and BAL could be used as easy detectable biomarkers for NSCLC.
Methods
Study design
This observational prospective study was carried out on 67 subjects at the Chest Department, Tanta University Hospital and Genomic Signature Cancer Centre of Tanta University International Educational Hospital, Egypt, from June 2015 to June 2018 after the approval of the ethics committee of Faculty of Medicine, Tanta University. Recruitment, sample collection, and measurement were done during the first year and then follow up only for survival for 2 years. Study was registered in ClinicalTrials.gov (Identifier NCT02445924) on 15 May 2015 URL: https://clinicaltrials.gov/ct2/show/NCT02445924.
Subjects
MiRNAs were extracted from serum and BAL of 37 NSCLC patients and 30 healthy volunteers (15 non-smokers and 15 smokers). Informed written consents were obtained from all participants. Recently, diagnosed NSCLC patients who did not receive chemotherapy, surgery, or radiation therapy were included in the study. Lung cancer was confirmed by histopathological examination of BAL, brush, and/or biopsy. While patients with concomitant asthma, COPD, broncheiactasis, upper/lower respiratory tract infection in the preceding 4 weeks, active pulmonary tuberculosis, associated cancer beside lung cancer, and patients who received chemotherapy, surgery or radiation therapy previous to the sample collection was excluded from the study. The same exclusion criteria were applied for the controls.
RNA extraction
Venous blood (5 ml) was collected, and serum obtained and stored at − 20 °C or − 80 °C until required. BAL (20 ml) was centrifuged at 1800g and 4 °C for 10 min. Cell pellet from BAL was frozen as a dry pellet at – 80 °C for later RNA isolation. Total RNA, including miRNAs from serum and BAL, was isolated by TRIzol (Invitrogen) (Qiagen USA Maryland Germantown) in combination with RNeasy Mini Kit from Qiagen. Five milliliters of serum was added to 5 volumes QIAzol Lysis Reagent and mixed by pipetting up and down. The mix was stored at − 80° until all samples available for simultaneous processing
Analysis of RNA and miRNA concentration with nano drop
The concentration and purity of the large RNA (mRNA) fractions (> 200 nucleotides) and small RNA (miRNA) fractions (< 200 nucleotides) were assessed using the Nano Drop spectrophotometer (Nano Drop Technologies). The sample arm was used to compress the sample resulting in the formation of a sample column, held in place by surface tension. Spectral measurements were made with a tightly controlled path length of 0.1 cm.
Analysis of RNA and miRNA integrity with Agilent 2100 bio analyzer
Quantification and data analysis by the Agilent 2100 Expert software (Version B.02.03). Integrity of the total and large RNA fraction was assessed using the RNA 6000 Nano Lab Chip Series II Assay, and the small RNA enriched fractions were also analyzed using the small RNA assay—RNA samples loaded onto the Agilent chip that were separated by capillary electrophoresis according to their molecular weight.
Flash Tag™ Biotin HSR RNA Labeling Procedure
The Flash Tag™ Biotin HSR Labeling Kit was used. The starting RNA input was 60 to 100 ng/L of total RNA. This protocol describes labeling total RNA or low molecular weight (LMW) RNA for analysis by Affymetrix® Gene Chip® (USA Qiagen Company) miRNA Arrays (TaqMan Array Human MicroRNA Card containing a total of 384 TaqMan MicroRNA assays per card) and includes an in-process ELOSA QC Assay. The labeling process was completed in less than one hour. Expression Console™ 1.4.1.46 software was used
Analysis of microRNAS using quantitative RT-PCR
Some miRNAs that were differently expressed using microarray were verified using quantitative real-time polymerase chain reaction (qRT-PCR) using TaqMan miRNA assay. These include analysis of fold change of miR-15b-5p, miR-193b, miR-301, miR-19b-1, miR-106a, miR-106b, miR-16-5b, miR-146a, let-7 g, miR-98, mir20b, miR-1, and miR-30a of 18 patients and 14 controls in both serum and BAL samples. Total RNA was isolated from samples using QIAzol Lysis Reagent (Qiagen USA) (1 to 10 ng of total RNA per 15-μL RT reaction). RT reaction was performed in an Applied Biosystem’s 7900 instrument.
RT reactions were carried out at 16 °C for 30 min, 42 °C for 30 min, and 85 °C for 5 min, and then maintained at 4 °C. There were significant correlations between microarray and qRT-PCR analysis.
Statistical analysis
Statistical analyses were performed by using the SPSS software (Version 17.0, SPSS Inc., Chicago, IL, USA). Statistically significant differences were considered when P < 0.05. Parametric t test (unpaired, two tailed) for each miRNA was done following verification of the normal distribution of the measured data. Receiver operating characteristic (ROC) was analyzed to find the relative sensitivity and specificity of serum and BAL miRNA for diagnosis of lung cancer.
We verified whether the miRNA (both serum and BAL) was differentially expressed or not by checking the fold change (FC), which is the ratio of y/x, where y = miRNA expression in the test sample (control or patient), x = standard miRNA expression level, and fold change = x/y.
If FC = 1, then the miRNA is not differentially expressed, if FC is more than 1, then the miRNA is upregulated while FC is much smaller than 1.0, then the miRNA is downregulated, and miRNA that is either downregulated or upregulated is said to be differentially expressed. Values were presented in log fold change.
The concentrations of miRNAs were normalized to reference miRNA level, and relative levels were evaluated using the comparative quantification cycle (Cq). Relative amount of each miRNA to ref rRNA was described using the equation 2 – ΔCT, where ΔCT = CTmiRNA–CTref mirna and CT (concentration).
Results
Demographic data of patients and controls are shown in Table 1.
Two lung cancer patients were hypertensive while another two were diabetics, and they did not show significant miRNA expression pattern.
In this study, a total of 32miRNAs were differentially expressed in NSCLC patients versus control. Thirteen miRNAs were significantly upregulated, while 19 were significantly downregulated in the NSCLC serum relative to control (Tables 2 and 3).
To evaluate the effect of smoking on miRNA expression, we compared serum miRNA expression between control smokers and non-smokers. We found that miR-143, miR-181, and miR-199a were the most consistently upregulated while miR-1246, miR-146a, miR218, miR-133, and let7-a were the most consistently downregulated in control smokers versus control non-smokers (Table 4).
We found that in NSCLC smokers, serum miR-143, miR-181, and miR-199a were significantly upregulated, and serum miR-146a and let 7a were significantly downregulated versus control smokers (Table 5).
In our study, a total of 14 miRNAs were differentially expressed in BAL of NSCLC patients versus control. Out of them, 12 miRNAs were significantly consistently upregulated (miR-19b-1, miR-1285, miR-1289, miR-1303, miR-217, miR-29a-5p, miR-548-3p, miR-650, miR-106a, miR-106-b, miR-143, miR-10-b), while two miRNAs (miR-1 and miR-30a) exhibited significant downregulation (Table 6).
In order to evaluate the accuracy of the measured miRNAs in reaching a statistical significance, 100 repetitions of 10-fold changes were done. Using a subset of 29 miRNAs, the best results were obtained with an accuracy of 94.3% [93.9–94.8%], a specificity of 97.8% [97.1–98.4%], and a sensitivity of 92.3% [91.5–92.3%].
After 2 years follow-up, eight patients of NSCLC group died. We found high expression of seven miRNAs (miR21-5, miR143-p, miR155, miR17-3p, miR106a, miR-221, and miR93) and low expression of 10 miRNAs (miR30d-5p, miR137, miR372, miR182, let-7 family, miR-182, miR145, miR499a-5p, miR-1, miR451a, and miR 486-5P) in their sera in comparison to survivors. Upregulated and downregulated miRNAs in sera of NSCLC patients who died are presented in Table 7.
Receiver operating characteristic (ROC) was analyzed, and we found sensitivity of 91.9% and 94.6% for serum and BAL miRNA, respectively, for diagnosis of lung cancer with specificity of 93.3% and 96.6%, respectively (Table 8).
Discussion
The identification of specific miRNA profile in lung cancer may aid in early diagnosis with the least invasive maneuver [10]. In this study, a total of 32 miRNAs were differentially expressed in NSCLC sera versus controls while 14 miRNAs were differentially expressed in BAL of NSCLC compared to control.
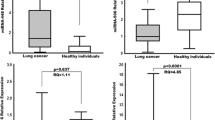
The upregulation of miR-15b-5b in sera of NSCLC patients in our study was in accordance with the results of Fan et al. [11]. They also found other five serum miRNAs (miR-16-5p, miR-17b-5p, miR-19-3p, miR-20a-5p, and miR-92-3p) to be significantly downregulated in NSCLC which was similar to our results except for miR-92-3p which was not significantly deregulated in sera of our patients. This difference might be explained by the difference in sample size and ethnicity of patients.
On the other hand, Patnaik et al. [12] reported that let-7 family and miR 126 had no differential expression between lung cancer patients and control which was opposite to our results. The difference might be because they examined only 75% of known human mature miRNAs, while we examined the whole panel of miRNA in our study. In addition, they used whole blood instead of serum. Another factor is that all their patients were heavy smokers and over sixty of age.
The findings of differentially expressed serum miRNAs in NSCLC versus control in our study are consistent with findings of some other studies [13,14,15,16,17,18,19]. Similar to our results, two independent studies found significant upregulation of serum miR-141, miR-200b, miR-193b, and miR-301 in NSCLC patients [20, 21]. The upregulation of miR-340 and miR-203 is also in agreement with the work of some other researchers [22]. In accordance with our results, downregulation of miR-146a was reported by Park et al [23] who used microarray and qRT-PCR (reverse transcriptase PCR) to investigate the miRNA expression profiles.
In accordance of our results, Rehbein et al. [24] reported that a panel of eight microRNAs (miR 19b-1, 1285, 1289, 1303, 217, 29a-5p, 548-3p, 650) were differentially upregulated in BAL of lung cancer patients versus non-cancerous patients using microarray.
In addition, Molina-Pinelo et al. [25] demonstrated upregulation of four miRNA clusters (the mir-17-92 cluster and its paralogues, mir-106a-363 and mir-106b-25; and the miR-192-194 cluster) in BAL of patients with lung adenocarcinoma. Upregulated mir-106a and mir-106b were exactly as in our results; however, the other two miRNAs were not deregulated in BAL of our patients. This difference might be because they included only adenocarcinoma patients, so squamous cell and large cell carcinoma patients were not included.
In another study, Molina-Pinelo et al. [26] documented downregulation of miR-17, miR19b, miR195, and miR20b in BAL and serum of lung cancer patients, while in our patients, we found these microRNAs to be downregulated in serum only and not in BAL. One of the reasons for this discordance is that pre-analytic sample preparation methods are different, and that there is no standard so far. Also, Molina-Pinelo et al. [26] included only ten patients in their study, with only six lung adenocarcinoma stage III or IV while two of them were healthy and two had interstitial lung disease.
In 2015, Kim et al. declared similar expression of miR-21 and miR-143 in BAL fluid as detected in our patients [27]. Like in our results, Sheervalilou et al. [28] described upregulation of miR-10b and downregulation of miR-1 and miR30 in BAL of NSCLC patients compared to control, but they used RT-PCR.
In a trial to study the effect of smoking on miRNA profile, we found three miRNAs to be significantly upregulated (miR-143, miR-181, and miR-199a) while other five were significantly downregulated (miR-133, miR-1246, miR-146a, miR218, and let7-a) in control smokers versus control non-smokers. These findings matched the results of Wang et al. [29] who found that miR-143 and miR-199a were upregulated by smoking. However, they described upregulation of miR-240 in smokers which was not detected in our study. Moreover, downregulation of let-7a in smokers was reported in another study [30] but in contrast to our results, they documented upregulation of miR-124 in smokers.
Another study [31] showed a different expression profile of miRNA in smokers as let7d, miR-150, miR-192, miR-197, and miR320 were upregulated in current smokers, while ex-smokers had higher serum expression of miR-1, miR-150, miR-195, and miR-320. Unlike our results, they found an overexpression of miR-146 in smokers. The difference from our results may be because they used qRT-PCR while we used microarray, difference in race, and sample size.
After 2 years follow-up, we detected high expression of seven miRNAs (miR21-5, miR143-p, 155, miR17-3p, miR106a, and miR93) and low expression of ten miRNAs (miR30d-5p, miR137, miR372, miR182, let-7 family, miR145, miR21-5, miR21-5, miR21-5, miR21-5, miR21-5, miR21-5, miR499a-5p , miR-1 ,miR451a, and miR 486) in non-survivors indicating that they might have a prognostic value in lung cancer. In 2017, Li et al. [32] concluded that three miRNAs could predict the clinical outcome of NSCLC patients including high expression of miR-21-5p and the low expression of miR-30d-5p which is consistent with our results. In addition, Fortunato et al. [33] clarified downregulation of miR-499a-5p and considered it a predictor of poor prognosis in NSCLC patients.
Different studies stated that members of the let-7 family exhibit downregulation in lung cancer and has a strong association with metastasis, advanced stages, and poor survival considering it a prognostic marker [20, 34,35,36,37].
Receiver operating characteristic (ROC) was analyzed, and we found sensitivity of 91.9% and 94.6% for serum and BAL miRNA, respectively, for diagnosis of lung cancer with specificity of 93.3% and 96.6%, respectively. These data were in accordance with yang et al. [38].
Limitations
This study was limited by the relatively small number of patients; the high cost of technique can explain this limitation. Although using microarray to detect miRNA expression is more expensive compared to cheaper methods as qRT-PCR, microarray can profile thousands of microRNAs concomitantly in a very short time permitting easy standardization of the technique.
Conclusions
NSCLC leads to a deregulation of miRNA expression compared to healthy individuals using microarray. Serum and BAL miRNAs may be used as novel biomarkers in early diagnosis of lung cancer. Verification of the results using next generation sequencing will help a better understanding of the specific panel of miRNAs in lung cancer. To our knowledge, this is the first study done in Middle East on NSCLC patients using microarray for studying the whole panel of miRNA.
Availability of data and materials
All the data of the current study are available from the corresponding author upon reasonable request.
Abbreviations
- NSCLC:
-
Non-small cell lung cancer
- MiRNA:
-
MicroRNA
- RT-PCR:
-
Reverse transcriptase polymerase chain reaction
- BAL:
-
Broncho-alveolar lavage
References
Cooper WA, Lam DC, O’Toole SA, Minna JD (2013) Molecular biology of lung cancer. J Thorac Dis 5(S5):S479–S490. https://doi.org/10.3978/j.issn.2072-1439.2013.08.03
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A (2015) Global cancer statistics, 2012. CA Cancer J Clin 65:87–108
Carnio S, Novello S, Papotti M, Loiacono M, Scagliotti GV (2013) Prognostic and predictive biomarkers in early stage non small-cell lung cancer: tumor based approaches including gene signatures. Transl Lung Cancer Res 2(5):372–381. https://doi.org/10.3978/j.issn.2218-6751.2013.10.05
Midthun DE (2016) Early detection of lung cancer. Fl000Res 5:739
Vescovo VD, Grasso M, Barbareschi M, Denti MA (2014) MicroRNAs as Lung Cancer Biomarkers. World J Clin Oncol 5(4):604–620
Perron MP, Provost P (2008) Protein interactions and complexes in human microRNA biogenesis and function. Front Biosci 13:2537–2547
Rajewsky N (2006) L(ou)sy miRNA targets? Nat Struct Mol Biol 13:754–755
Zhang B, Pan X, Cobb G, Anderson TA (2007) microRNAs as oncogenes and tumor suppressors. Dev Biol 302:1–12
Ma PC, Maulik G, Christensen J, Salgia R (2003) c-Met: structure, functions and potential for therapeutic inhibition. Cancer Metastasis Rev 22:309–325
Wang Y, Chen J, Lin Z, Cao J, Huang H, Jiang Y, He H, Yang L, Ren NY, Liu G (2016) Role of deregulated microRNAs in non-small cell lung cancer progression using fresh-frozen and formalin-fixed, paraffin-embedded samples. Oncol Lett 11:801–808
Fan L, Qi H, Teng J, Su B, Chen H, Wang C, Xia Q (2016) Identification of serum miRNAs by nano-quantum dots microarray as diagnostic biomarkers for early detection of non-small cell lung cancer. Tumor Biol 37(6):7777–7784
Patnaik SK, Kannisto ED, Mallick R, Vachani A, Yendamuri S (2017) Whole blood microRNA expression may not be useful for screening non-small cell lung cancer. PLoS One 12(7):e0181926 (1-19)
Keller A, Leidinger P, Borries A, Wendschlag A, Wucherpfennig F, Scheffler M, Huwer H, Lenhof HP, Meese E (2009) miRNAs in lung cancer-studying complex fingerprints in patient’s blood cells by microarray experiments. BMC Cancer 9:353
Keller A, Backes C, Leidinger P, Kefer N, Boisguerin V, Barbacioru C, Vogel B, Matzas M, Huwer H, Katus HA, Stahler C, Meder B, Meese E (2011) Next-generation sequencing identifies novel microRNAs in peripheral blood of lung cancer patients. Mol BioSyst 7(12):3187–3199
Leidinger P, Keller A, Borries A, Huwer H, Rohling M, Huebers J, Lenhof HP, Meese E (2011) Specific peripheral miRNA profiles for distinguishing lung cancer from COPD. Lung Cancer 74(1):41–47
Leidinger P, Backes C, Dahmke IN, Galata V, Huwer H, Stehle I, Bals R, Keller A, Meese E (2014) What makes a blood cell based miRNA expression pattern disease specific?—a miRNome analysis of blood cell subsets in lung cancer patients and healthy controls. Oncotarget 5(19):9484–9497
Patnaik SK, Yendamuri S, Kannisto E, Kucharczuk JC, Singhal S, Vachani A (2012) MicroRNA expression profiles of whole blood in lung adenocarcinoma. PLoS One 7(9):e46045
Jeong HC, Kim EK, Lee JH, Lee JM, Yoo HN, Kim JK (2011) Aberrant expression of let-7a miRNA in the blood of non-small cell lung cancer patients. Mol Med Rep 4(2):383–387
Ulivi P, Foschi G, Mengozzi M, Scarpi E, Silvestrini R, Amadori D, Zoli W (2013) Peripheral blood miR-328 expression as a potential biomarker for the early diagnosis of NSCLC. Int J Mol Sci 14(5):10332–10342
Inamura K, Ishikawa Y (2016) MicroRNA In lung cancer: novel biomarkers and potential tools for treatment. J Clin Med 5(3):36
Nadal E, Truini A, Nakata A, Lin J, Reddy RM, Chang AC, Ramanath N, Gotoh N, Beer DG, Chen G (2015) A novel serum 4-microRNA signature for lung cancer detection. Sci Rep 5:12464. https://doi.org/10.1038/srep12464
Wozniak MB, Scelo G, Muller DC, Mukeria A, Zaridze D, Brennan P (2015) Circulating microRNAs as non-invasive biomarkers for early detection of non-small- cell lung cancer. PLoS One 10(5):e0125026
Park DH, Jeon HS, Lee SY, Choi YY, Lee HW, Yoon S, Lee JC, Yoon YS, Kim DS, Na MJ, Kwon SJ, Kim DS, Kang J, Park JY, Son JW (2015) MicroRNA-146a inhibits epithelial mesenchymal transition in non-small cell lung cancer by targeting insulin receptor substrate 2. Int J Oncol 47:1545–1553
Rehbein G, Schmidt B, Fleischhacke M (2015) Extracellular microRNAs in bronchoalveolar lavage samples from patients with lung diseases as predictors for lung cancer. Clin Chim Acta 450:78–82
Molina-Pinelo S, Pastor MD, Suarez R, Romero-Romero B, Gonzalez De la Pena M, Salinas A, Garcia-Carbonero R, De Miguel MJ, Rodriguez-Panadero F, Carnero A, Paz-Ares L (2014) MicroRNA clusters: dysregulation in lung adenocarcinoma and COPD. Eur Respir J 43:1740–1749
Molina-Pinelo S, Suarez R, Pastor MD, Nogal A, Marguez-Martin E, Martin-Juan J, Carnero A, Paz-Ares L (2012) Association between the miRNA signatures in plasma and bronchoalveolar fluid in respiratory pathologies. Dis Markers 32:221–230
Kim JO, Gazala S, Razzak R, Guo L, Ghosh S, Roa WH, Bedard EL (2015) Non-small cell lung cancer detection using microRNA expression profiling of bronchoalveolar lavage fluid and sputum. Anticancer Res 35(4):1873–1880
Sheervalilou R, Khamaneh AM, Sharifi A, Nazemiyeh M, Taghizadieh A, Ansarin K, Zarghami N (2017) Using miR-10b, miR-1 and miR-30a expression profiles of bronchoalveolar lavage and sputum for early detection of non-small cell lung cancer. Biomed Pharmacother 88:1173–1182
Wang G, Wang R, Strulovici-Barel Y, Salit J, Staudt MR, Ahmed J, Tilley AE, Yee-Levin J, Holimann C et al (2015) Persistence of smoking-induced dysregulation of MiRNA expression in the small airway epithelium despite smoking cessation. Pcr PLoS One 10(4):e0120824
Banerjee A, Waters D, Camacho O, Minet E (2015) Quantification of plasma microRNAs in a group of healthy smokers, ex-smokers and non-smokers and correlation to biomarkers of tobacco exposure. Biomarkers 20(2):123–131
Suzuki K, Yamada H, Nagura A, Ohashi K, Ishikawa H, Yamazaki M, Ando Y, Ichino N et al (2016) Association of cigarette smoking with serum microRNA expression among middle-aged Japanese adults. Fujita Med J 2:1–5
Li C, Yin Y, Liu X, Xi X, Xue W, Qu Y (2017) Non-small cell lung cancer associated microRNA expression signature: integrated bioinformatics analysis, validation and clinical significance. Oncotarget 8(15):24564–24578
Fortunato O, Verri C, Pastorino U, Sozzi G, Boeri M (2016) MicroRNA profile of lung tumor tissues is associated with a high risk plasma miRNA signature. Microarrays (Basel) 5(3):18
Sun CC, Li SJ, Zhang F, Pan JY, Wang L, Yang CL, Xi YY, de Li J (2016) Hsa-miR-329 exerts tumor suppressor function through down-regulation of MET in non-small cell lung cancer. Oncotarget 7(16):21510–21527
Li M, Zhang S, Wu N, Wu L, Wang C, Lin Y (2016) Overexpression of miR-499–5p inhibits non-small cell lung cancer proliferation and metastasis by targeting VAV3. Sci Rep 6:23100
Avgeris M, Mavridis K, Tokas T, Stravodimos K, Fragoulis EG, Scorilas A (2015) Uncovering the clinical utility of miR-143, miR-145 and miR-224 for predicting the survival of bladder cancer patients following treatment. Carcinogenesis 36:528–537
Wang R, Wang ZX, Yang JS, Pan X, De W, Chen LB (2011) MicroRNA-451 functions as a tumor suppressor in human non-small cell lung cancer by targeting ras-related protein 14 (RAB14). Oncogene 30:2644–2658
Yang X, Zhang Q, Zhang M, Su W, Wang Z, Li Y, Zhang J, Beer DG, Yang S, Chen G (2019) Serum microRNA signature is capable of early diagnosis for non-small cell lung cancer. Int J Biol Sci 15:1712–1722
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
All the authors shared in the concept, design, definition of intellectual content, literature search, clinical studies, data acquisition, data analysis, statistical analysis, manuscript preparation, manuscript editing, and manuscript review. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Study protocol was approved by the ethics committee of Faculty of Medicine, Tanta University, Egypt (Approval code 2858/11/14). Informed written consents were obtained from all participants.
Consent for publication
Not applicable.
Competing interests
Authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mansour, S.A., Farhat, A.A., Abd El-Zaher, A.H. et al. MicroRNA genetic signature in non-small cell lung cancer (NSCLC) Egyptian patients. Egypt J Bronchol 14, 20 (2020). https://doi.org/10.1186/s43168-020-00021-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43168-020-00021-2