
Abstract
Background
Transarterial chemoembolization (TACE) is recommended as the standard care for unresectable hepatocellular carcinoma (HCC) at Barcelona Clinic Liver Cancer (BCLC) stage A–B. However, the efficacy of TACE on large (≥ 10 cm) stage A–B HCC is far from satisfactory, and it is proposed that hepatic artery infusion chemotherapy (HAIC) might be a better first-line treatment of this disease. Hence, we compared the safety and efficacy of HAIC with the modified FOLFOX (mFOLFOX) regimen and those of TACE in patients with massive unresectable HCC.
Methods
A prospective, non-randomized, phase II study was conducted on patients with massive unresectable HCC. The protocol involved HAIC with the mFOLFOX regimen (oxaliplatin, 85 mg/m2 intra-arterial infusion; leucovorin, 400 mg/m2 intra-arterial infusion; and fluorouracil, 400 mg/m2 bolus infusion and 2400 mg/m2 continuous infusion) every 3 weeks and TACE with 50 mg of epirubicin, 50 mg of lobaplatin, 6 mg of mitomycin, and lipiodol and polyvinyl alcohol particles. The tumor responses, time-to-progression (TTP), and safety were assessed.
Results
A total of 79 patients were recruited for this study: 38 in the HAIC group and 41 in the TACE group. The HAIC group exhibited higher partial response and disease control rates than did the TACE group (52.6% vs. 9.8%, P < 0.001; 83.8% vs. 52.5%, P = 0.004). The median TTPs for the HAIC and TACE groups were 5.87 and 3.6 months (hazard radio [HR] = 2.35, 95% confidence interval [CI] = 1.16–4.76, P = 0.015). More patients in the HAIC group than in the TACE group underwent resection (10 vs. 3, P = 0.033). The proportions of grade 3–4 adverse events (AE) and serious adverse events (SAE) were lower in the HAIC group than in the TACE group (grade 3–4 AEs: 13 vs. 27, P = 0.007; SAEs: 6 vs. 15, P = 0.044). More patients in the TACE group than in the HAIC group had the study treatment terminated early due to intolerable treatment-related adverse events or the withdrawal of consent (10 vs. 2, P = 0.026).
Conclusions
HAIC with mFOLFOX yielded significantly better treatment responses and less serious toxicity than did TACE. HAIC might represent a feasible and promising first-line treatment for patients with massive unresectable HCC.
Similar content being viewed by others

Introduction
Hepatocellular carcinoma (HCC) is the third common cancer worldwide and the second leading cause of cancer death in China [1]. Currently, most guidelines recommend transarterial chemoembolization (TACE), a technique combining intra-arterial chemotherapy and selected embolization, as the standard of care for unresectable HCC at Barcelona Clinic Liver Cancer (BCLC) stage A–B [2,3,4]. However, the efficacy of TACE on large (≥ 10 cm) stage A–B HCC is far from satisfactory [5,6,7]. The disease control rate (DCR) was less than 50%, and the median overall survival was only 6.5–9.1 months [8,9,10]. One reason is that complete embolization of all tumor-feeding arteries is especially difficult for massive HCCs because these HCCs usually have multiple intrahepatic and/or extrahepatic collateral arterial supplies and arteriovenous fistulas. Moreover, after embolization for large tumors, patients are at a high risk of serious embolization-related adverse events (AEs), such as serious post-embolization syndrome, liver/renal dysfunction, and ectopic embolism. TACE-related death rates of 6.5–20% have been reported [9, 10].
Some researchers have proposed that continuous hepatic artery infusion chemotherapy (HAIC) might be a better first-line treatment than TACE for patients with massive HCCs [11, 12]. Recent researches suggest that chemotherapy plays an important role in TACE, and adding embolization might be more detrimental than beneficial for these patients [13,14,15,16]. Compared with TACE, HAIC provides more stable and sustained local delivery of chemotherapy agents [17]. Several cisplatin (DDP)-based HAIC regimens have been reported to provide an encouraging therapeutic efficacy on HCC [18,19,20,21]. Nevertheless, the DDP dose was limited by renal, neurological, and gastrointestinal toxicities [22]. In contrast, oxaliplatin (OXA) has been reported to be a better DNA synthesis inhibitor than cisplatin and have better synergism with 5-fluorouracil (5-FU) with a different toxicity profile [23,24,25]. Furthermore, two recent large multicenter studies evaluating OXA-based regimens as first-line systemic chemotherapy for advanced HCC demonstrated manageable toxicities and promising tumor responses [26, 27].
Hence, it is important to investigate whether OXA-based HAIC is a better first-line treatment than TACE for patients with massive unresectable HCC. However, to date, only a few preliminary studies have evaluated the efficacy and safety of OXA-based HAIC regimens compared with conventional TACE. One phase I study showed that OXA-based HAIC was well tolerable in HCC patients [28]. Additionally, another retrospective single-cohort study reported by Li et al. [29] showed that the combination use of OXA-based HAIC and conventional TACE is a safe and promising treatment for patients with HCCs larger than 10 cm in diameter. Here, we present results from a prospective, non-randomized, controlled study that assessed the efficacy and safety of HAIC with OXA, 5-FU, and leucovorin (LV) in patients with massive unresectable HCC. The modified FOLFOX6 (mFOLFOX6) regimen was used because the safety of HAIC with the mFOLFOX6 regimen has been documented in several phase I/II trials in patients with hepatic metastases from colorectal cancer [30, 31]. Our primary objective was to compare the responses of massive unresectable HCC to HAIC with FOLFOX with those to TACE. The secondary objective was to assess the time-to-radiological progression (TTP) and toxicity.
Patients and methods
Patients and study design
This prospective, non-randomized study was approved by the institutional review board of Sun Yat-sen University Cancer Center and was performed in accordance with the Declaration of Helsinki of 1975 as revised in 1983. The study was registered at http://ClinicalTrials.gov (No. NCT03048123). Between October 1, 2015 and October 1, 2016, consecutive patients with unresectable HCC treated at our institution were enrolled. Patients had to provide signed informed consent before enrollment in the study.
HCC was diagnosed based on the criteria used by the European Association for the Study of the Liver (EASL). All patients met the following criteria: (a) the sum of diameters of all lesions longer than 10 cm with the maximum lesion longer than 7 cm; (b) age between 18 and 75 years; (c) the tumor was not amenable to surgical resection or any other curative treatment; (d) platelet count ≥ 75,000/μL, hemoglobin ≥ 8.5 g/dL, total bilirubin ≤ 30 mmol/L, and serum albumin ≥ 32 g/L; and (e) the absence of cirrhosis or a cirrhotic status of Child–Pugh class A only. Patients were excluded from the study if they met any of the following criteria: (a) a previous history of treatment for HCC; (b) vascular invasion or distant metastasis; (c) severe underlying cardiac or renal diseases; or (d) a second primary malignancy. Each patient was informed of the details of the TACE and HAIC procedures, especially concerning the uncertain benefits and complication risks associated with HAIC, as well as other possible treatment options, such as systemic chemotherapy. The treatment choice of either HAIC or TACE was made at the patients’ request after a full discussion with our multidisciplinary treatment team, which included radiologists, surgeons, hepatologists, and oncologists.
Treatment
TACE was performed according to our previously reported protocol [16]. Chemolipiodolization was performed using 50 mg of epirubicin (pharmorubicin; Pfizer, Wuxi, Jiangsu, China), 50 mg of lobaplatin (Hainan Changan International Pharmaceutical Co. Ltd., Haikou, Hainan, China), and 6 mg of mitomycin C (Zhejiang Hisun Pharmaceutical Co. Ltd., Taizhou, Zhejiang, China) mixed with 10 mL of lipiodol (Lipiodol Ultra-Fluide; Guerbet Laboratories, Aulnay Sous Bois, Paris, France). If necessary, up to 20 mL of additional pure lipiodol was injected. The injection was stopped when stasis of blood flow in the target artery was observed. Subsequently, embolization was performed with the injection of polyvinyl alcohol particles that were 300–500 μm in diameter through the catheter to reach stasis in the tumor-feeding artery. Repeated TACE was performed at intervals of 6 weeks.
In the HAIC group, patients were treated using a 3-week cycle regimen. A catheter was advanced into the hepatic artery according to our previously reported protocol [16]. A microcatheter was selectively placed into the feeding arteries of the tumor. The gastroduodenal artery was occluded by a coil when necessary. Then, the microcatheter was connected to the artery infusion pump to administer the following treatment: OXA, 85 mg/m2 intra-arterial infusion on day 1; LV, 400 mg/m2 intra-arterial infusion on day 1; and 5-FU, 400 mg/m2 bolus infusion on day 1 and 2400 mg/m2 continuous infusion over 46 h. After HAIC was completed, the indwelling catheter and the sheath were removed, and manual compression was performed to achieve hemostasis.
HAIC and TACE were discontinued when disease progression (including vascular invasion or the development of extrahepatic spread) or intolerable AEs occurred or when the patient was eligible for another treatment (surgical resection) or withdrew consent. Additionally, the study treatment was suspended when the following conditions occurred: technical difficulty in repeating the treatment (stenosis or occlusion of the tumor-feeding artery or an artery only supplied by the extrahepatic collateral arteries) or unsuitable characteristics (neutrophil count < 1200/μL, platelet count < 60,000/μL, total bilirubin > 30 mmol/L, or albumin < 3.0 mg/dL). The study treatment was stopped if no recovery occurred after a 30-day delay.
If the study treatment was discontinued, the following treatment was defined as subsequent treatment. The subsequent treatment decisions of both groups would be made according to the same protocol by the same multidisciplinary team, based on the tumor burden, liver function, and the patient’s request. Basically, hepatic resections were performed on patients whose tumor shrank to be resectable. For patients with tumor progression without contraindications to TACE, repeating TACE was recommended. For patients whose residual tumors could not be embolized due to technical problems, radiofrequency ablations were used to destroy residual tumors when it was feasible. Conservative treatments were given to patients with terminal HCC, Child–Pugh C liver function, or Eastern Cooperative Oncology Group (ECOG) score > 2 [32].
Efficacy and safety
According to the Response Evaluation Criteria in Solid Tumors (RECIST) [33], tumor responses were evaluated by radiologists who were blinded to the treatment. All objective responses were confirmed at least 4 weeks after the first observation. DCR is defined as the rate of complete response (CR) plus partial response (PR) plus stable disease (SD). Objective response rate (ORR) is defined as the rate of CR plus PR. TTP was calculated from the time of the first transcatheter therapy to the time of disease progression.
AEs and serious adverse events (SAEs) were monitored and recorded by professional nurses who were blinded to the treatment. Until study treatment was discontinued, AEs were assessed during and after each treatment procedure and at all follow-up visits and were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE) version 3.0 [34]. SAEs included treatment-related hospitalization or prolonged hospitalization, dysfunction or disability, life-threatening consequences, and death. Treatment-related death was defined as death caused by a complication within 30 days after the procedure.
Follow-up
The follow-up ended on January 24, 2017. Contrast-enhanced computed tomography (CT) was performed every 6 weeks. Blood tests, including liver function test and the serum alpha-fetoprotein (AFP) level test, were performed during each treatment period. For patients with tumors that shrank to a resectable size, the choice of the next treatment was determined according to the patient’s request and the results of discussions by our multidisciplinary team.
Sample size
The sample size was computed using the DCR as the main end point. A 5% significance level for the two-sided Fisher’s exact test for equality should have 80% power to detect differences between an 80% DCR with HAIC and a 50% DCR with TACE. The minimal sample size needed to detect a significant difference was calculated to be 38 patients per group.
Statistical analyses
For comparisons of baseline variables, Student’s t test was used for continuous variables, and the Chi square test was used for categorical variables. TTP was estimated using the Kaplan–Meier method and compared using the log-rank test. The patients without tumor progression were censored. A P value < 0.05 was considered significant. All statistical processing was performed using the Statistical Package for Social Sciences version 13.0 (SPSS Inc., Chicago, IL, USA).
Results
Patient characteristics
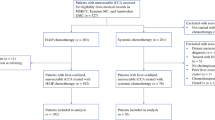
Between October 1, 2015 and October 1, 2016, 114 consecutive patients with HCC were treated using either HAIC or TACE. Seventy-nine patients met the criteria for inclusion in this analysis: 38 underwent HAIC, and 41 underwent TACE (Fig. 1). The baseline characteristics of all patients are described in Table 1. The only difference between groups was that the HAIC group had more patients with a prolonged prothrombin time (P = 0.003).

Flow diagram of patients with unresectable hepatocellular carcinoma who underwent either HAIC or TACE. HAIC hepatic artery infusion chemotherapy; TACE transarterial chemoembolization; AEs adverse events
Treatment
The 79 patients underwent a total of 215 study treatment sessions. Patients in the HAIC group received more sessions than did patients in the TACE group (146 vs. 69, P = 0.003). Patients in the HAIC group received an average of 3.8 ± 1.5 HAIC sessions (range 1–6 sessions; median: 4 sessions), whereas patients in the TACE group received an average of 1.7 ± 0.8 TACE sessions (range 1–3 sessions; median: 1 session) (P < 0.001). More patients in the HAIC group than in the TACE group underwent surgical resection (10 vs. 3, P = 0.033). There was no significant difference in the number of patients receiving other subsequent treatments between the HAIC and TACE groups (Table 2).
Safety
AEs are summarized in Table 3. There was no significant difference in the overall number of patients who had AEs between the HAIC and TACE groups (35 vs. 41, P = 0.107). However, the number of patients reporting AEs of grade ≥ 3 or SAEs was significantly smaller in the HAIC group than in the TACE group (AEs of grade ≥ 3: 13 vs. 27, P = 0.007; SAEs: 6 vs. 15, P = 0.044). Two patients in the TACE group died of an SAE, whereas no treatment-related death occurred in the HAIC group (P = 0.494). The occurrence rates of fever, hyperbilirubinemia, and alanine transaminase (ALT) elevation were higher in the TACE group, whereas those of sensory neuropathy, diarrhea, and hypoproteinemia were higher in the HAIC group (all P < 0.05). Furthermore, particular abdominal pain was observed in 10 patients of HAIC group when injecting OXA, and the pain disappeared when the injection was stopped.
The tolerability of HAIC and TACE was analyzed. In the TACE group, 10 (24.4%) patients had treatment terminated early (6 weeks after beginning therapy) due to intolerable chemoembolization-related AEs or withdrawal of consent by the patient. However, in the HAIC group, only 2 (5.3%) patients had treatment terminated early. This difference was significant (P = 0.026).
Efficacy
The tumor responses among patients are shown in Table 4. No complete responses were achieved in either group. The DCR and ORR was significantly higher in the HAIC group than in the TACE group (DCR: 83.8% vs. 52.5%, P = 0.004; ORR: 54.1% vs. 9.8%, P < 0.001).
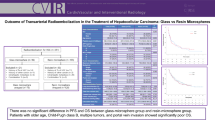
In the univariate analysis, the median TTP was 5.9 months (95% confidence interval [CI] = 3.9–7.8 months) in the HAIC group and 3.6 months (95% CI = 1.8–5.4 months) in the TACE group. The TTP was significantly longer in the HAIC group than in the TACE group (P = 0.015), and the hazard radio was 2.35 (95% CI = 1.16–4.76). Progression-free survival was shown in Fig. 2.

Kaplan-Meier estimated progression-free survival curves of patients with unresectable hepatocellular carcinoma. Of the 79 patients, 38 underwent HAIC, and 41 underwent TACE. HAIC hepatic artery infusion chemotherapy; TACE transarterial chemoembolization
Discussion
In this prospective, non-randomized, phase II study, we compared the safety and efficacy of HAIC with mFOLFOX6 versus TACE in patients with massive unresectable HCC. This study demonstrated encouraging results for both safety and efficacy of HAIC with mFOLFOX6. HAIC-related AEs in our study were consistent with previous report investigating systemic chemotherapy with mFOLFOX6 [26] with the exception of one particular AE (abdominal pain) associated with OXA injection. The occurrence rate of cytotoxic agent-specific AEs was significantly higher in the HAIC group than in the TACE group, including sensory neuropathy (OXA-specific) and diarrhea (5-FU-specific). In contrast, the occurrence rate of embolization-specific AEs, such as fever and hyperbilirubinemia, was significantly higher in the TACE group than in the HAIC group. There were no significant differences in the overall rate of AEs between the two groups. However, the numbers of patients reporting AEs of grade ≥ 3 and SAEs were both significantly smaller in the HAIC group than in the TACE group. The tolerability of HAIC was also better than that of TACE. Compared with the HAIC group, more patients in the TACE group had their study treatment terminated early due to intolerable treatment-related AEs or the withdrawal of consent by the patient (10 vs. 2). These findings suggested a significant superiority in the safety of HAIC with mFOLFOX over TACE.
Some previous studies recommended using the modified RECIST (mRECIST) criteria to assess tumor response in clinical trials of locoregional treatment of HCC, because devascularization rather than tumor shrinkage may be a hallmark of response in HCC [35]. Nevertheless, in contrast to HAIC, the CT response assessment following TACE may be confounded by the presence of lipiodol. Therefore, RECIST is a better guideline than mRECIST for comparing tumor responses to HAIC and TACE, and we used RECIST to evaluate tumor responses in the present study. Patients in the HAIC group achieved a significantly higher partial response rate than did patients in the TACE group (52.6% vs. 9.8%). There was also a significant difference between the two groups in the median TTP (5.9 vs. 3.6 months). The number of patients who underwent resection was significantly larger in the HAIC group than in the TACE group (10 vs. 3). These findings suggested a significant superiority of HAIC with mFOLFOX over TACE in terms of efficacy on massive HCCs. Because more than half of the recruited patients remained alive when this study was terminated, an overall survival analysis could not be conducted. The above results strongly support the launch of a large prospective, randomized, controlled study as soon as possible.
The first limitation of the present study was its non-randomized nature because the treatment choices depended on the patients’ requests. However, no significant differences were found in the baseline characteristics between the two groups. Moreover, the patients in both groups were treated strictly according to the study protocol. The difference in the numbers of study treatment sessions can also be explained by the different treatment intervals and the superiority of HAIC with mFOLFOX over TACE in terms of both efficacy and safety. The second limitation was that subsequent treatments may be a confounding factor. However, subsequent treatments of both groups were performed according to the same multidisciplinary treatment protocol by the same team. Furthermore, we used tumor response to evaluate efficacy of study treatment, and we recorded study treatment-related AEs. Tumor responses and study treatment-related AEs were not likely be influenced by subsequent treatment.
In conclusion, the present study demonstrated that patients in the HAIC group had significantly better tumor responses and less SAEs than patients in the TACE group. More patients in the HAIC group than in the TACE group received potential curative treatments after tumor down-staging. Thus, HAIC might be a better choice for patients with massive unresectable HCC.
References
Chen W, Zheng R, Zeng H, Zhang S. The incidence and mortality of major cancers in China, 2012. Chin J Cancer. 2016;35(1):73. doi:10.1186/s40880-016-0137-8.
Bruix J, Sherman M, American Association for the Study of Liver D. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53(3):1020–2. doi:10.1002/hep.24199.
European Association For The Study Of The L, European Organisation For R, Treatment Of C. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2012;56(4):908–43. doi:10.1016/j.jhep.2011.12.001.
Verslype C, Rosmorduc O, Rougier P, Group EGW. Hepatocellular carcinoma: ESMO-ESDO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2012;23(Suppl 7):vii41–8. doi:10.1093/annonc/mds225.
Ryder SD, Rizzi PM, Metivier E, Karani J, Williams R. Chemoembolisation with lipiodol and doxorubicin: applicability in British patients with hepatocellular carcinoma. Gut. 1996;38(1):125–8.
Ebied OM, Federle MP, Carr BI, Pealer KM, Li W, Amesur N, et al. Evaluation of responses to chemoembolization in patients with unresectable hepatocellular carcinoma. Cancer. 2003;97(4):1042–50.
Li S, Zhang L, Huang ZM, Wu PH. Transcatheter arterial chemoembolization combined with CT-guided percutaneous thermal ablation versus hepatectomy in the treatment of hepatocellular carcinoma. Chin J Cancer. 2015;34(6):254–63. doi:10.1186/s40880-015-0023-9.
Xue T, Le F, Chen R, Xie X, Zhang L, Ge N, et al. Transarterial chemoembolization for huge hepatocellular carcinoma with diameter over ten centimeters: a large cohort study. Med Oncol. 2015;32(3):64. doi:10.1007/s12032-015-0504-3.
Huang YH, Wu JC, Chen SC, Chen CH, Chiang JH, Huo TI, et al. Survival benefit of transcatheter arterial chemoembolization in patients with hepatocellular carcinoma larger than 10 cm in diameter. Aliment Pharmacol Ther. 2006;23(1):129–35. doi:10.1111/j.1365-2036.2006.02704.x.
Poon RT, Ngan H, Lo CM, Liu CL, Fan ST, Wong J. Transarterial chemoembolization for inoperable hepatocellular carcinoma and postresection intrahepatic recurrence. J Surg Oncol. 2000;73(2):109–14.
Sumie S, Yamashita F, Ando E, Tanaka M, Yano Y, Fukumori K, et al. Interventional radiology for advanced hepatocellular carcinoma: comparison of hepatic artery infusion chemotherapy and transcatheter arterial lipiodol chemoembolization. AJR Am J Roentgenol. 2003;181(5):1327–34. doi:10.2214/ajr.181.5.1811327.
Kim HY, Kim JD, Bae SH, Park JY, Han KH, Woo HY, et al. A comparative study of high-dose hepatic arterial infusion chemotherapy and transarterial chemoembolization using doxorubicin for intractable, advanced hepatocellular carcinoma. Korean J Hepatol. 2010;16(4):355–61. doi:10.3350/kjhep.2010.16.4.355.
Kirchhoff TD, Rudolph KL, Layer G, Chavan A, Greten TF, Rosenthal H, et al. Chemoocclusion vs chemoperfusion for treatment of advanced hepatocellular carcinoma: a randomised trial. European J Surg Oncol. 2006;32(2):201–7. doi:10.1016/j.ejso.2005.11.003.
Okusaka T, Kasugai H, Shioyama Y, Tanaka K, Kudo M, Saisho H, et al. Transarterial chemotherapy alone versus transarterial chemoembolization for hepatocellular carcinoma: a randomized phase III trial. J Hepatol. 2009;51(6):1030–6. doi:10.1016/j.jhep.2009.09.004.
Yamasaki T, Hamabe S, Saeki I, Harima Y, Yamaguchi Y, Uchida K, et al. A novel transcatheter arterial infusion chemotherapy using iodized oil and degradable starch microspheres for hepatocellular carcinoma: a prospective randomized trial. J Gastroenterol. 2011;46(3):359–66. doi:10.1007/s00535-010-0306-5.
Shi M, Lu LG, Fang WQ, Guo RP, Chen MS, Li Y, et al. Roles played by chemolipiodolization and embolization in chemoembolization for hepatocellular carcinoma: single-blind, randomized trial. J Natl Cancer Inst. 2013;105(1):59–68. doi:10.1093/jnci/djs464.
Ensminger WD. Intrahepatic arterial infusion of chemotherapy: pharmacologic principles. Semin Oncol. 2002;29(2):119–25.
Song DS, Song MJ, Bae SH, Chung WJ, Jang JY, Kim YS, et al. A comparative study between sorafenib and hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma with portal vein tumor thrombosis. J Gastroenterol. 2015;50(4):445–54. doi:10.1007/s00535-014-0978-3.
Lin CC, Hung CF, Chen WT, Lin SM. Hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma with portal vein thrombosis: impact of early response to 4 weeks of treatment. Liver Cancer. 2015;4(4):228–40. doi:10.1159/000367737.
Nouso K, Miyahara K, Uchida D, Kuwaki K, Izumi N, Omata M, et al. Effect of hepatic arterial infusion chemotherapy of 5-fluorouracil and cisplatin for advanced hepatocellular carcinoma in the Nationwide Survey of Primary Liver Cancer in Japan. Br J Cancer. 2013;109(7):1904–7. doi:10.1038/bjc.2013.542.
Tsai WL, Lai KH, Liang HL, Hsu PI, Chan HH, Chen WC, et al. Hepatic arterial infusion chemotherapy for patients with huge unresectable hepatocellular carcinoma. PLoS ONE. 2014;9(5):e92784. doi:10.1371/journal.pone.0092784.
Osaki A, Suda T, Kamimura K, Tsuchiya A, Tamura Y, Takamura M, et al. A safe and effective dose of cisplatin in hepatic arterial infusion chemotherapy for hepatocellular carcinoma. Cancer Med. 2013;2(1):86–98. doi:10.1002/cam4.55.
Cassidy J. Review of oxaliplatin: an active platinum agent in colorectal cancer. Int J Clin Pract. 2000;54(6):399–402.
Soulie P, Bensmaine A, Garrino C, Chollet P, Brain E, Fereres M, et al. Oxaliplatin/cisplatin (L-OHP/CDDP) combination in heavily pretreated ovarian cancer. Eur J Cancer. 1997;33(9):1400–6.
Maurel J, Cervantes A, Conill C, Salazar R, Martin-Richard M, Pera M, et al. Phase I trial of oxaliplatin in combination with cisplatin, protacted-infusion fluorouracil, and radiotherapy in advanced esophageal and gastroesophageal carcinoma. Int J Radiat Oncol Biol Phys. 2005;62(1):91–6. doi:10.1016/j.ijrobp.2004.09.009.
Qin S, Bai Y, Lim HY, Thongprasert S, Chao Y, Fan J, et al. Randomized, multicenter, open-label study of oxaliplatin plus fluorouracil/leucovorin versus doxorubicin as palliative chemotherapy in patients with advanced hepatocellular carcinoma from Asia. J Clin Oncol. 2013;31(28):3501–8. doi:10.1200/JCO.2012.44.5643.
Zaanan A, Williet N, Hebbar M, Dabakuyo TS, Fartoux L, Mansourbakht T, et al. Gemcitabine plus oxaliplatin in advanced hepatocellular carcinoma: a large multicenter AGEO study. J Hepatol. 2013;58(1):81–8. doi:10.1016/j.jhep.2012.09.006.
Rathore R, Safran H, Soares G, Dubel G, McNulty B, Ahn S, et al. Phase I study of hepatic arterial infusion of oxaliplatin in advanced hepatocellular cancer: a brown university oncology group study. Am J Clin Oncol. 2010;33(1):43–6. doi:10.1097/COC.0b013e31819d8668.
Li JH, Xie XY, Zhang L, Le F, Ge NL, Li LX, et al. Oxaliplatin and 5-fluorouracil hepatic infusion with lipiodolized chemoembolization in large hepatocellular carcinoma. World J Gastroenterol. 2015;21(13):3970–7. doi:10.3748/wjg.v21.i13.3970.
Kern W, Beckert B, Lang N, Stemmler J, Beykirch M, Stein J, et al. Phase I and pharmacokinetic study of hepatic arterial infusion with oxaliplatin in combination with folinic acid and 5-fluorouracil in patients with hepatic metastases from colorectal cancer. Ann Oncol. 2001;12(5):599–603.
Kemeny NE, Niedzwiecki D, Hollis DR, Lenz HJ, Warren RS, Naughton MJ, et al. Hepatic arterial infusion versus systemic therapy for hepatic metastases from colorectal cancer: a randomized trial of efficacy, quality of life, and molecular markers (CALGB 9481). J Clin Oncol. 2006;24(9):1395–403. doi:10.1200/JCO.2005.03.8166.
Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649–55.
Tsuchida Y, Therasse P. Response evaluation criteria in solid tumors (RECIST): new guidelines. Med Pediatr Oncol. 2001;37(1):1–3. doi:10.1002/mpo.1154.
The National Cancer Institute. Common terminology criteria for adverse events v3.0 (CTCAE). http://www.eortc.be/services/doc/ctc/ctcaev3.pdf. Accessed 25 Apr 2012.
Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60. doi:10.1055/s-0030-1247132.
Authors’ contributions
MS designed the study. MKH, YL, and MS drafted the manuscript and participated in patient selection and implementation of the study. WW, SHL, and RPG assisted in patient selection and helped collect the data. MKH, LQJ, and ZSY performed the statistical analysis. All authors read and approved the final manuscript.
Acknowledgements
This work was supported by the National Natural Science Foundation of China (No. 81625017 and No. 81572385) and the Fundamental Research Funds for the Central Universities of China (No. 16ykjc36).
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
The key raw data have been deposited into the Research Data Deposit (http://www.researchdata.org.cn), with the Approval Number of RDDA2017000166.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
He, MK., Le, Y., Li, QJ. et al. Hepatic artery infusion chemotherapy using mFOLFOX versus transarterial chemoembolization for massive unresectable hepatocellular carcinoma: a prospective non-randomized study. Chin J Cancer 36, 83 (2017). https://doi.org/10.1186/s40880-017-0251-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40880-017-0251-2