
Abstract
Background
Today, the attention of researchers has been drawn to the use of medicinal plant for the treatment of kidney stones. The aim of this study was to investigate the effect of five plants used in traditional medicine on the dissolution of calcium oxalate and calcium phosphate stones. Then, the ability of more effective plants to dissolve stones collected from patients after Percutaneous Nephrolithotripsy was investigated.
Methods
The aerial part of plants were extracted by maceration method. The synthesized stones in laboratory were incubated with different concentrations of the extract. Next, the concentrations of calcium oxalate and calcium phosphate were measured by a calcium kit and BT 3000. The effect of the extract with the best activity on the stones collected from the patients was also studied. The composition of clinical stones was determined by colorimetric method. The total phenolic content (TPC) of the extracts was determined.
Results
The highest dissolution of calcium oxalate stones was observed by the G. struthium extract and the highest dissolution of calcium phosphate stones by the A. euchroma and A. officinalis root extracts. The dissolution percentage of clinical stones by the A. euchroma extract was significantly higher than other extract (P < 0.05). The highest TPC was observed in A. euchroma extract (P < 0.05).
Conclusion
The A. euchroma extract exhibited the greatest dissolution activity on laboratory calcium oxalate and calcium phosphate stones as well as clinical stones made of high amounts of calcium oxalate. Therefore, the extract can be effective in preventing and treating kidney stones.
Similar content being viewed by others


Background
Worldwide, the spread of kidney stone disease is rising with a few numbers of effective drugs. This urological disorder affects about 12% of the world’s population [1]. About 80% of all kidney stones are composed of oxalate calcium, and around 20% of kidney stones made of calcium phosphate which, like oxalate calcium stones, are formed as a result of increased calcium [2, 3]. Due to the stupendous costs and side effects of instrument embedding and urinary tract surgery, special attention has now been drawn to the use of herbal products [4,5,6]. Medicinal plants have long been used as an important source by humans and even animals [7]. Nowadays, many researchers have based their research on medicinal plants and a variety of old methods such as those conducted by Ibn Sina. Given the richness of the Iranian traditional medicine, the medicinal plants that, according to the various traditional textbooks, are widely used to treat kidney stones include Alcea officinalis, Petroselinum crispum, Arnebia euchroma, Ferula persica, and Gypsophila struthium [8]. As a well known plant in Iranian traditional medicine, A. euchroma is a perennial plant belonging to the Boraginaceae family. The plant is also known in Iran as Havachoubeh or Giahsorkh [9]. A. euchroma is rich in naphthoquinone, shikonin, alkanin, and sohexenylnaphthazarin derivatives that have various medicinal properties including anti-inflammatory, antimicrobial and anticancer properties [10, 11]. F. persica is from the Umbelliferae family and is called Sakbinage in Arabic language. In traditional medicine, the gum and resin of this plant are used as expectorant, antispasmodic, carminative, and laxative, as well as to treat dyspepsia, neurological diseases, such as epilepsy, and various pains, especially joint pain [12]. The parsley, scientifically called P. crispum, belongs to the Umbelliferae family, whose leaves are used in traditional medicine for the treatment of constipation, abdominal bloating, jaundice, colitis, edema, rheumatism, prostate problems, and liver disease [13]. The plant compounds contain volatile oils and flavonoids, making this vegetable play an unparalleled role in human health [14]. Various parts of these plants, including leaves, flowers and roots, have been proposed in traditional medicine for the treatment of inflammation, severe cough, bronchitis, swelling, stomach ache, kidney stones and bladder diseases. Studies have shown that root and flower of different species of Alcea contain varied amounts of flavonoids, polyphenols, polysaccharides, mucilage, fibers, unsaturated fatty acids, minerals and albumin [14].
Another medicinal plant used in traditional medicine is Kondosh scientifically called G. struthium belonging to the Caryophyllaceae family. The plant’s root contains toxic alkaloids such as veratrin, which causes vasodilatation and is hypotensive. This plant is used to calm neuropathic pain and acts as an anti-rheumatic herbal drug. Its root is tonic and laxative. It is also used to treat some skin diseases [15].
Given the richness of the Iranian traditional medicine and medicinal plants frequently cited in traditional medicine, this study was conducted to investigate five plants used in traditional medicine on the dissolution of calcium oxalate and calcium phosphate stones in vitro.
Material and methods
Plant
First, the studied plants (A. officinalis, P. crispum, A. euchroma, F. persica and G. struthium) were prepared from the local market, and after scientific and systematic identification by a botanist, a voucher herbarium specimen was deposited for each of them at the Herbarium of the Medicinal Plants Research Center of Shahrekord University of Medical Sciences (SKUMS) Table 1.
Extraction
Extraction was done by maceration method. To this end, the plant powder was mixed with ethanol 70% (1: 5) and kept at room temperature for 48 h. Then, the mixture was filtered using a filter paper and the Büchner flask, the resulting solution was concentrated in vacuum by a rotary evaporator, and the extracts were dried by freeze-drying [16].
Preparation of purified laboratory calcium oxalate and calcium phosphate stones
To prepare the stones of interest, an equimolar calcium chloride dihydrate solution, along with a solution of sodium oxalate solution and 10 cc 2 N sulphuric acid, was poured into a beaker to form a calcium oxalate sediment. Further, an equimolar calcium chloride dihydrate solution, along with 10 cc 2 normal sulfuric acid and disodium hydrogen phosphate, was poured into a beaker to form a calcium phosphate sediment. Both sediments were neutralized by ammonia solution and washed with distilled water at 60 °C for 4 h. In addition, the synthesized crystalline stones were identified by the infrared spectroscopy (FT-IR) method described in our previous study [17].
Estimation of dissolution rate of calcium oxalate and calcium phosphate stones
First, cellulose dialysis membrane activation (SIGMA D9652) was performed according to the manufacturer’s instructions described in our previous study [17]. One mg of calcium oxalate and calcium phosphate were weighed and immersed along with the extracts under study at different (3, 10 and 30 mg/dL) concentrations inside the semi-permeable membrane in 0.1 M Tris buffer. Further, groups containing extracts alone or 1 mg of calcium oxalate or calcium phosphate were also considered. After incubation at 37 °C for 7 h, the content of semi-permeable membranes in each group was transferred to the test tubes, and 2 ml of 1 N sulfuric acid was added and the concentration of calcium oxalate and calcium phosphate was measured after each treatment using a calcium kit (Pars Azmoon Co.) and the BT-3000. The dissolution percentage of stones was also calculated by the formula below.
Dissolution percentage (%) = [calcium content of stone - (calcium content of stone in the presence of extract - calcium content of extract)/stone calcium content (× 100)]. All experiments were performed in triplicate [17].
Effect of the most effective extract on PCNL stones
After analyzing the data and selecting the best extract, all the steps mentioned were performed on 5 stones collected after the PCNL procedure. It should be noted that the collected stones are combined. Specific kits for the analysis of urinary tract stones (Darman-Kav Co.) and the colorimetric method manual were used to investigate the composition of clinical stones [18].
Measuring total phenolic content (TPC)
Total phenolic content (TPC) was measured using the Folin-Ciocalteu colorimetric method in gallic acid equivalent (GAE) in grams of dried extract. Initially, different concentrations of gallic acid and extracts were prepared in 60% methanol solution. Then, 0.1 ml of each concentration was transferred to the test tube. Next, 0.5 ml of 10% Folin-Ciocalteu solution was added to each test tube, and after 3–8 min, 0.4 ml of 7.5% sodium carbonate solution was added. After 30 min, optical absorbance was read by a spectrophotometer at 765 nm. Finally, the TPC of the extract was calculated and expressed in mg GAE/g dried extract [19].
Data analysis
The data were summarized as means ± standard deviation for normally distributed variables, or medians with interquartile range (Median (IQR)) for non-normally distributed variables. Normality distribution was assessed with the Kolmogorov test. Because percentages were non-normally distributed, they were analyzed using Kruskal-Wallis test. Total phenolic content was normally distributed, so it was analyzed using ANOVA with LSD multiple comparison test. Statistical significance was defined as P < 0.05 in all tests and analysis was performed by SPSS version 24.
Results
Dissolution percentages of calcium oxalate and calcium phosphate stones
According to the results of Kruskal-Wallis test, the dissolution percentages of oxalate calcium and calcium phosphate were significantly different depending on the type of extract (P = 0.001). The highest dissolution rate of oxalate calcium stones was obtained for the G. struthium extract 62.9 (61.6–66.1), and the highest dissolution rate of calcium phosphate for the A. euchroma extract 64.7 (56.2–72.1) and the A. officinalis root extract 74.2 (68.5–83.1) (Figs. 1 and 2). The dissolution rates of oxalate calcium and calcium phosphate stones were significantly different in terms of extract concentration (P = 0.006 and P = 0.041, respectively). The dissolution percentages of oxalate calcium stones by the extract at 3.3 and 10 mg/dL were not significantly different (P = 1) but the dissolution percentages of this stone by the extract at 3.3 and 30 mg/dL were significantly different (P = 0.009). The dissolution percentages of oxalate calcium stones by the extract at 10 and 30 mg/dL were significantly different (P = 0.041) (Fig. 3 and 4).

Percent dissolution of oxalate calcium (CaOx) by different extracts. Petroselinum crispum (P.C), Gypsophila struthium (G.S), Alcea officinalis (Root) (A.O.R), Arnebia euchroma (A.E), Ferula persica (F.P) and Alcea officinalis (Flower) (A.O.F).

Percent dissolution of phosphat calcium (CaP) by different extracts. Petroselinum crispum (P.C), Gypsophila struthium (G.S), Alcea officinalis (Root) (A.O.R), Arnebia euchroma (A.E), Ferula persica (F.P) and Alcea officinalis (Flower) (A.O.F).

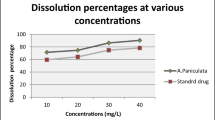
Percent dissolution of oxalate calcium (CaOx) based on extract concentration

Percent dissolution of phosphat calcium (CaP) based on extract concentration
The compositions of clinical stones
According to the diagnostic results, in the five clinical stones studied (S1, S2, S3, S4, S5), calcium oxalate accounts for the highest content and magnesium-ammonium phosphate and ammonium urate the least content Table 2.
The effects of the A. euchroma, G. struthium and A. officinalis extracts on the dissolution of clinical stones
After analyzing the results at the screening stage, the effects of the A. euchroma, G. struthium and A. officinalis extracts on the dissolution of clinical stones were investigated. The results regarding the dissolution percentages of different clinical stones by the A. euchroma, G. struthium and A. officinalis extracts were not significantly different (P = 850) (Fig. 5). According to the results of Kruskal-Wallis test, the dissolution percentages of clinical stones by different extracts were significantly different (P < 0.001). The dissolution percentages of clinical stones by the G. struthium and A. officinarum root extracts were not significantly different (P = 1.000). The dissolution percentages of clinical stones by the A. euchroma extract was significantly different from those by the G. struthium and A. officinalis root extracts (P < 0.001); in other words, the highest dissolution activity was exhibited by the A. euchroma extract and the lowest dissolution activity by the A. officinalis root extract (Fig. 6).

Dissolution percentage of clinical stone (S1, S2, S3, S4, S5) by Arnebia euchroma, Gypsophila struthium and Alcea officinalis (Root) according to stone type

Percent dissolution of clinical stone (S1, S2, S3, S4, S5) by Arnebia euchroma, Gypsophila struthium and Alcea officinalis (Root) according to extract type
The analysis of variance in total phenolic content (TPC)
The results of analysis of variance showed that the TPC of the A. euchroma, A. officinalis root, G. struthium, P. crispum, A. officinalis flower, and F. persica extract were significantly different (P < 0.05) (Table 3). The results of the comparison of the mean TPCs of extracts showed that the A. euchroma extract contains the highest TPC (58.11 mg GAE/g dried powder) with a significant difference compared to other extracts (P < 0.05). The lowest amount of TPC was obtained in the A. officinalis root extract (28.08 mg GAE/g dried powder) with a significant difference compared to other extracts (P < 0.05) except for the F. persica extract Table 3.
Discussion
Many people around the world suffer from problems related to urinary tract stones. Calcium stones are the most common and account for about 75% of the total stones. These stones can be composed of calcium oxalate (50%), calcium phosphate (5%) or both (45%). Many factors contribute to the formation of urinary tract stones. Hypercalciuria is the most common cause of formation of urinary tract stones [20]. Urinary tract stones are mainly composed of crystalline components. Multiple stages of crystal formation include nucleation, growth, and accumulation of crystals [21].
The treatments for kidney stones include Extracorporeal Shock Wave Lithotripsy (ESWL) and drug therapy. ESWL may cause acute kidney injury, decrease renal function and increase the likely that are among the serious problems due to the treatments for urinary stones [22]. In vitro and in vivo data and clinical trials indicate that the medicinal plants and their active ingredients can be useful as alternative or complementary therapies in the management of the urinary system. The medicinal plants and their active ingredients can be useful because they improve restorative mechanisms naturally and do not cause side effects [21]. In this regard a number of medicinal plants such as Dolichos biflorus, Tribulus terrestris and Bergenia ligulata have been found to exhibit therapeutic properties against urinary tract stones in in vitro and in vivo and clinical trials [20, 23].
In the present study, the dissolution percentages of oxalate calcium and calcium phosphate stones were significantly different for different types and concentrations of the extracts. The G. striuthum extract exhibited the highest dissolution percentage of calcium oxalate stones and the A. euchroma and A. officinalis root extracts exhibited the highest dissolution percentage of calcium phosphate stones. Then, the dissolution percentages of clinical stones with high calcium oxalate content by the A. euchroma, A. officinalis root and F. persica extracts were determined. It was observed that the dissolution percentage of clinical stones by the A. euchroma extract was significantly higher than those by the G. struthium and A. officinalis root extracts. In the present study the A. euchroma extract exhibited the highest dissolution of kidney stones in vitro.
Joshi et al. (2005) evaluated the effectiveness of Tribulus terrestris and Bergenia ligulata in vitro. To this end, aqueous Tribulus terrestris and Bergenia ligulata extracts along with supernatant solutions were added, and the formation of crystals was comparatively measured with and without the aqueous extracts. It was observed that both extracts inhibited the formation of calcium oxalate crystals, with the higher efficacy of Bergenia ligulata. The main components of Tribulus terrestris include steroidal saponins and secondary components include alkaloids and common phytosterols, especially B-cytosterol. In the extracts of Bergenia ligulata, the presence of bergenin, b-sitosterol and gallic acid have been identified. Therefore, these biomacromolecules are likely to play an important role in inhibiting calcium oxalate crystals [20]. In the study of Byahatti et al. (2010), the effects of alcoholic, butanolic, and ethyl acetate extracts of Bergenia ciliata leaf and their phenolic fractions were evaluated for dissolution of calcium oxalate and calcium phosphate stones in an in vitro model. The results showed that phenolic fraction isolated from the ethyl acetate extract, the highest solubility was shown on both stones [24]. Hua-Fang Cai et al. (2012) investigated the effectiveness of total phenols and flavonoids isolated from the ethanolic extract of Orthosiphon stamineus and polysaccharides isolated from the aqueous extract of this plant in the dissolution of calcium oxalate crystals in an in vivo model. The results showed that phenols and flavonoids isolated from the ethanolic extract and also polysaccharides from the aqueous extract were effective in dissolving calcium oxalate crystals and polysaccharides significantly inhibited the nucleation and accumulation of calcium oxalate crystals [25]. In the study of Patel et al. (2010), the activity of Piper nigrum extract in the dissolution of calcium phosphate and calcium oxalate stones was evaluated. The results of that study showed that the aqueous and alcoholic extracts have a greater effect than ethyl acetate and petroleum extracts in preventing the formation, crystallization and accumulation of calcium phosphate and oxalate calcium stones. The researchers stated that this effect may be due to the presence of alkaloids in the ethanolic and aqueous extracts [26]. In the present study, the A. euchroma extract was found to have the highest phenolic content and showed the highest efficacy in dissolving stones. This can be due to active ingredients especially phenolic compounds in the extract. Studies have shown that the A. euchroma extract contains polyphenolic compounds, flavonoids, saponins, alkaloids and other phytochemical compounds [27]. The anti-crystallization properties of saponins have been well known for preventing the accumulation of macroproteins that act as stimulants of crystallization [28]. It has been observed that saponin-rich Terminalia arjuna extract inhibits the accumulation and formation of calcium phosphate crystals [29]. In addition, saponin-rich Herniaria hirsuta fraction is a strong inhibitor of oxalate calcium in vitro [30]. The therapeutic effects of saponin-rich fraction of plant extracts in animal models of kidney stones have been reported. In one study, in renal stone mice with, crystalluria, hypercalciuria, polyuria, nephrocalcinosis, renal dysfunction and oxidative stress were manifested as increased lipid peroxidation, reduced glutathione reduction, and decreased activity of the catalase enzyme in the kidney. All these improved after treatment with saponin-rich Solanum xanthocarpum fraction [31].
The renal epithelial cells exposed to excess amounts of oxalic acid produce reactive oxygen species relative to the amount of the intracellular antioxidants. Subsequently, oxidative stress in the kidney results in damage to the cell DNA and the onset of crystallization. Clinical studies have also provided evidence for the development of oxidative stress in the stone-forming kidneys of the patients. The relationship between the formation of stones and the development of a common disorder is due to specific pathological characteristics. Oxidative stress is a common feature of cardiovascular disease, such as high blood pressure, diabetes, atherosclerosis and myocardial infarction [32]. In a study by Ceban et al. (2016), the effects of oxidative and antioxidant status in patients with renal stone before and after surgery were investigated. The results show that the complicated surgical treatments for kidney stones leads to reduction of oxidative stress [33]. In the study of Davalos et al. (2010), the cytotoxic effects of calcium oxalate monohydrate (COM) on biochemical and vital parameters of the cell and the protective effects of antioxidants against COM were investigated. The results showed that COM exerts toxic effects on the LLC-PK1 renal tubular epithelial cells by inducing oxidative stress, resulting in a decrease in cell survival, adverse impacts on biochemical parameters and eventually apoptosis. N-acetylcysteine (NAC) can prevent the severe effects of cytotoxicity, protects against COM attack, and prevents kidney injury and consequently the formation of stone [34]. Natural phenolic compounds act as antioxidants and inhibit free radicals. Therefore, the preventive and therapeutic effects of the extracts on kidney stones can be partly due to the anti-inflammatory and antioxidant effects of the compounds present in them. By interfering with the process of cell destruction by crystals, these compounds may prevent the release or action of inflammation-progressing factors that are effective on the heterogeneous nucleation of crystals [35]. The dissolution of calcium phosphate and calcium oxalate stones has also been attributed to phenolic compounds. In a study, the dissolution activity of calcium phosphate and oxalate calcium stones by the fraction rich in phenolic compounds was observed to be higher than that by the extract alone [24]. Phenolic acids are another group of non-flavonoid phenolic compounds that are widely found in plants and have various biological activities such as anti-inflammatory, antibacterial, antiviral, antitumor and antioxidant properties [36]. In this study, the highest TPC was observed in the A. euchroma (58.11 mg GAE/g dried powder) with a significant difference to the TPC of other extracts (P < 0.05). It seems that the higher efficacy of the A. euchroma than other extracts is due to the types and amounts of its active ingredients. In this regard, it is suggested that the content of the saponin, alkaloid and tannic compounds of these extracts be determined by experimental methods and their relationship with the dissolution of stones in vitro, in order to determine which compounds are more closely related to the dissolution activity. It can therefore be effective in the prevention and treatment of kidney stones in people susceptible to developing oxalate and calcium phosphate stones, and it is recommended for further studies in the animal and clinical phases. In the present study, the activity of various extracts in dissolving calcium phosphate stones was higher than that in dissolving calcium oxalate stones. In the study of Byahatti et al. (2010), consistent with the results of our study, the activity of plant extracts in the dissolution of calcium phosphate stones (67.74%) was higher than that in the dissolution of calcium oxalate stones (36.95%) [24].
Conclusion
Based on the results of the present study, the dissolution percentages of oxalate calcium and calcium phosphate stones were significantly different depending on the type and concentration of extract. The highest dissolution of calcium oxalate stones was obtained for the G. struthium extract and the highest dissolution rate of calcium phosphate stones by the A. euchroma and A. officinalis root extracts. The dissolution percentage of clinical stones by the A. euchroma extract was significantly higher than those by the G. struthium extract and A. officinalis root extract. The A. euchroma extract exhibited the greatest dissolution activity on calcium oxalate and calcium phosphate stones as well as clinical stones. Both animal studies and clinical trials are recommended to further investigate this argument.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- PCNL:
-
Percutaneous nephrolithotripsy
- TPC:
-
Total phenolic content
- GAE:
-
Gallic acid equivalent
- ESWL:
-
Extracorporeal shock wave lithotripsy
- COM:
-
Calcium oxalate monohydrate
- NAC:
-
N-Acetylcysteine
References
Alelign T, Petros B. Kidney stone disease: an update on current concepts. Adv Urol. 2018;2018:1–12.
Kumar V, Abbas AK, Fausto N, Aster JC. Robbins and Cotran pathologic basis of disease. Philadelphia: Elsevier Saunders; 2005.
Moe OW. Kidney stones: pathophysiology and medical management. Lancet. 2006;367(9507):333–44.
Ronco C, Bellomo R, Kellum JA, Ricci Z. Critical Care Nephrology E-Book. Philadelphia: Elsevier Health Sciences; 2017.
Rosa M, Usai P, Miano R, Kim FJ, Agrò EF, Bove P, Micali S. Recent finding and new technologies in nephrolithiasis: a review of the recent literature. BMC Urol. 2013;13(1):1–11.
Touhami M, Laroubi A, Elhabazi K, Loubna F, Zrara I, Eljahiri Y, et al. Lemon juice has protective activity in a rat urolithiasis model. BMC Urol. 2007;7(1):1–10.
Ali A. Ibn Sina (Avicenna): the prince of physicians. Ann Saudi Med. 2007;27(2):134–5.
Faridi P, Roozbeh J, Mohagheghzadeh A. Ibn-Sina's life and contributions to medicinal therapies of kidney calculi. Iranian J Kidney Dis. 2012;6(5):339–45.
Tavakolifar B, Rezazadeh S, Badi H, Akhondzadeh S, Heidari M, Aghamohamadi E. The study of arnebia (Arnebia euchroma (Royle) IM Johnst) solution effectiveness on the treatment of Acne vulgaris. J Med Plants. 2010;9(34):150–5.
Shen CC, Syu WJ, Li SY, Lin CH, Lee GH, Sun CM. Antimicrobial activities of naphthazarins from arnebia euchroma. J Nat Prod. 2002;65(12):1857–62.
Kim SH, Kang IC, Yoon TJ, Park YM, Kang KS, Song GY, et al. Antitumor activities of a newly synthesized shikonin derivative, 2-hyim-DMNQ-S-33. Cancer Lett. 2001;172(2):171–5.
Dehpour AA, Ebrahimzadeh MA, Fazel NS, Mohammad NS. Antioxidant activity of the methanol extract of Ferula assafoetida and its essential oil composition. Grasas Aceites. 2009;60(4):405–12.
Jassim AM. Protective effect of Petroselinum crispum (parsley) extract on histopathological changes in liver, kidney and pancreas induced by sodium valproate-in male rats. Kufa J Vet Med Sci. 2013;4(1):20–7.
Kumar SS, Sudhakar S, Kapil S, Snigdha T. Ethno-pharmacological review on Althaea officinalis. WJPPS. 2016;5(7):425–32.
Martínez-Nieto MI, Segarra-Moragues JG, Merlo E, Martínez-Hernández F, Mota JF. Genetic diversity, genetic structure and phylogeography of the Iberian endemic Gypsophila struthium (Caryophyllaceae) as revealed by AFLP and plastid DNA sequences: connecting habitat fragmentation and diversification. Bot J Linn Soc. 2013;173(4):654–75.
Tona L, Cimanga R, Mesia K, Musuamba C, De Bruyne T, Apers S, et al. In vitro antiplasmodial activity of extracts and fractions from seven medicinal plants used in the Democratic Republic of Congo. J Ethnopharmacol. 2004;93(1):27–32.
Torki A, Hosseinabadi T, Fasihzadeh S, Sadeghimanesh A, Wibowo J, Lorigooini Z. Solubility of calcium oxalate and calcium phosphate crystallization in the presence of crude extract and fractions from Kelussia odoratissima Mozaff. Pharm Res. 2018;10(4):379–84.
Barzegarnejad A, Azadbakht M, Emadian O, Ahmadi M. Effect of some fractions of the extract of Juniperus communis fruit on solving kidney stones in vitro. J Mazandaran Univ Med Sci. 2014;23(110):146–52.
Bahmani M, Rafieian-Kopaei M, Parsaei P, Mohsenzadegan A. The anti-leech effect of Peganum harmala L. extract and some anti-parasite drugs on Limnatis nilotica. Afr J Microbiol Res. 2012;6(10):2586–90.
Joshi V, Parekh B, Joshi M, Vaidya A. Herbal extracts of Tribulus terrestris and Bergenia ligulata inhibit growth of calcium oxalate monohydrate crystals in vitro. J Cryst Growth. 2005;275(1–2):e1403–8.
Bahmani M, Baharvand-Ahmadi B, Tajeddini P, Rafieian-Kopaei M, Naghdi N. Identification of medicinal plants for the treatment of kidney and urinary stones. J Renal Inj Prev. 2016;5(3):129–33.
Coe FL, Evan A, Worcester E. Kidney stone disease. J Clin Invest. 2005;115(10):2598–608.
Garimella T, Jolly C, Narayanan S. In vitro studies on antilithiatic activity of seeds of Dolichos biflorus Linn. And rhizomes of Bergenia ligulata wall. Phytother Res. 2001;15(4):351–5.
Byahatti VV, Pai KV, D’Souza MG. Effect of phenolic compounds from Bergenia ciliata (haw.) Sternb. Leaves on experimental kidney stones. Anc Sci Life. 2010;30(1):14–7.
Zhong YS, Yu CH, Ying HZ, Wang ZY, Cai HF. Prophylactic effects of Orthosiphon stamineus Benth. Extracts on experimental induction of calcium oxalate nephrolithiasis in rats. J Ethnopharmacol. 2012;144(3):761–7.
Patel MA, Patel PK, Seth AK. Inhibition of calcium oxalate crystallization by the fruit extracts of Piper nigrum L. Pharm Online. 2011;2:1169–77.
Damianakos H, Kretschmer N, Sykłowska-Baranek K, Pietrosiuk A, Bauer R, Chinou I. Antimicrobial and cytotoxic isohexenylnaphthazarins from Arnebia euchroma (Royle) Jonst.(Boraginaceae) callus and cell suspension culture. Molecules. 2012;17(12):14310–22.
Saha S, Verma RJ. Inhibition of calcium oxalate crystallisation in vitro by an extract of Bergenia ciliata. Arab J Urol. 2013;11(2):187–92.
Chaudhary A, Singla S, Tandon C. In vitro evaluation of Terminalia arjuna on calcium phosphate and calcium oxalate crystallization. Indian J Pharm Sci. 2010;72(3):340–5.
Fouada A, Yamina S, Nait MA, Mohammed B, Abdlekrim R. In vitro and in vivo antilithiasic effect of saponin rich fraction isolated from herniaria hirsuta. J Bras Nefrol. 2006;28(4):199–203.
Patel PK, Patel MA, Vyas BA, Shah DR, Gandhi TR. Antiurolithiatic activity of saponin rich fraction from the fruits of Solanum xanthocarpum Schrad. & Wendl.(Solanaceae) against ethylene glycol induced urolithiasis in rats. J Ethnopharmacol. 2012;144(1):160–70.
Khan SR. Is oxidative stress, a link between nephrolithiasis and obesity, hypertension, diabetes, chronic kidney disease, metabolic syndrome? Urol Res. 2012;40(2):95–112.
Ceban E, Banov P, Galescu A, Botnari V. Oxidative stress and antioxidant status in patients with complicated urolithiasis. J Med Life. 2016;9(3):259–62.
Davalos M, Konno S, Eshghi M, Choudhury M. First prize (tie): oxidative renal cell injury induced by calcium oxalate crystal and renoprotection with antioxidants: a possible role of oxidative stress in nephrolithiasis. J Endourol. 2010;24(3):339–45.
El-Dakhakhny M, Madi N, Lembert N, Ammon H. Nigella sativa oil, nigellone and derived thymoquinone inhibit synthesis of 5-lipoxygenase products in polymorphonuclear leukocytes from rats. J Ethnopharmacol. 2002;81(2):161–4.
Saxena M, Saxena J, Pradhan A. Flavonoids and phenolic acids as antioxidants in plants and human health. Int J Pharm Sci Rev Res. 2012;16(2):130–4.
Acknowledgements
The authors gratefully thank the Research and Technology Deputy of Shahrekord University of Medical Sciences and Medical Plants Research Center of Shahrekord University of Medical Sciences for all supports provided.
Funding
This study was funded by Research and Technology Deputy of Shahrekord University of Medical Sciences (Grant no: 2388). The funders have no role in the design of the study, data collection, analysis, interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
ZL was responsible for the conception of the study and participated in the in vitro design and worked on the draft of manuscript. MSh, ZL and SKh designed, conducted and interpreted the research outcome of the in vitro study, performed the statistical analysis and worked on the draft of manuscript. DA and SM performed the assay and made contribution to the revision of the draft manuscript. EB worked on the standardization of the herbal extract and performed all the experiments of this study. All authors read and approved the final manuscript. SM, ZL and MSh prepared the manuscript. Before submission all the authors have checked and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All stages of experimentation were carried out in accordance with the regulations of the ethical commitee of Shahrekord University of Medical sciences (Ethics code: IR.SKUMS.REC.1396.17).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shirani, M., Arjaki, D., Kheiri, S. et al. An in vitro screening potential traditional medicinal plants for nephrolithiasis. Clin Phytosci 6, 66 (2020). https://doi.org/10.1186/s40816-020-00209-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40816-020-00209-5