
Abstract
Background
To investigate the retinal capillary density (RCD) of the macula using optical coherence tomography angiography (OCT-A) in type 2 diabetic patients and to further determine the association with risk factors.
Methods
A total of 212 eyes from 212 subjects were recruited; subjects included diabetics with no retinopathy (NDR, n = 90 eyes), diabetics with mild retinopathy DR (MDR, n = 36 eyes), and healthy participants (Control, n = 86 eyes). All participants underwent OCT-A scanning. RCD was quantified by superficial and deep retinal capillary layers (SRCL and DRCL) from OCT-A images.
Results
RCD in SRCL and DRCL was lower in NDR (P < 0.001) as well as in MDR (P < 0.001) when compared with control eyes. Diabetic patients were subdivided according to individual risk factors, complications related to diabetes, and hyperglycemia. Diabetic patients showed lower RCD in both the SRCL and DRCL when compared with healthy controls. Diabetics with age > 55y, HbA1c > 7% had significantly reduced DRCL (P < 0.05) when compared with the other group of diabetics (age < 55y, HbA1c < 7%). Diabetics with a blood urea nitrogen (BUN) > 8.2 mmol/L had significantly reduced SRCL and DRCL when compared to the other group of diabetics.
Conclusions
Risk factors including older age, higher level of HbA1c, LDL-C and BUN, were associated with lower RCDs found in type 2 diabetic patients with and without mild DR by OCT-A. The impairment of retinal capillary by OCT-A may play a key role in the early monitoring of management in diabetes.
Similar content being viewed by others


Background
Diabetes mellitus (DM) is characterized by chronic hyperglycemia [1] and the development of diabetes-specific macrovascular and microvascular alterations [2, 3]. Diabetic retinopathy (DR), one of the common microvascular complications relating to diabetes, is a leading cause of vision impairment and vision loss among adults [1, 4]. Although the causes of vascular damage as well as visual function abnormality are not fully understood, evidence from histopathologic studies has shown that the changes in the retinal capillaries precede the first clinical visible retinal signs, such as microaneurysms [5,6,7,8,9]. Therefore, early surrogate clinical biomarkers that can detect and quantify the preclinical lesions of retinal capillaries in diabetic patients are needed to predict the development of DR from the earliest stages and allow for early intervention to eventually retard or prevent retinopathy.
Fluorescein angiography (FA) [10, 11], or color fundus photographs [3, 12,13,14], have been widely used to establish the categorical grading of non-perfusion in DR. However, grading with FA is seldom done in the routine clinical practice due to its invasive nature. In addition, these two modalities do not evaluate the retinal capillary network reliably and cannot detect subtle changes due to their low resolution [15,16,17]. Optical coherence tomography angiography (OCT-A) is a novel imaging modality that can noninvasively and quickly demonstrate the intra-retinal microvasculature with quantitative and objective assessments [18,19,20,21]. Various parameters such as macular vascular density [22,23,24], macular vascular fractal dimension [22,23,24] and the area of foveal avascular zone (FAZ) [22,23,24], have been used to quantify retinal perfusion in diabetic patients with or without clinical DR by using OCT-A. In fact, type 2 DM is a disease of middle-aged and elderly individuals who have a higher prevalence of hypertension and are at higher risk of cardiovascular disease and mortality. Therefore, apart from the conventional DR risk factors (e.g., duration of DM or glycated hemoglobin A1C [HbA1c]) [25], it is also important to examine the effects of other systemic risk factors (e.g., age, sex, body mass index [BMI], blood pressure as well as relevant venous blood test parameters) on the retinal microvasculature in patients with type 2 DM, which are still unclear currently. The purpose of this study is to quantify the retinal capillary density (RCD) of the macula using OCT-A in type 2 diabetic patients with or without mild retinopathy, and to further evaluate the associations with risk factors.
Methods
Study population
Healthy volunteers and type 2 DM participants were recruited from the endocrine department of the Second Affiliated Hospital & Yuying Children’s Hospital and the Fundus Clinic of the Eye Hospital, Wenzhou Medical University, Wenzhou, China, from November 2015 to October 2017. Participants with high myopia, nondiabetic macular pathology, media opacity, or other significant eye diseases were excluded. Informed consent was obtained, and the study was approved by the ethics committee of the Eye Hospital of Wenzhou Medical University and complied with the tenets of the Declaration of Helsinki. All diabetic patients were initially graded into two subgroups according to the International Clinical Diabetic Retinopathy Severity Scale [26]: DM without retinopathy (NDR), and mild non-proliferative DR (MDR).
Demographic information collected from the patients included age, sex, duration of DM, smoke and alcohol history as well as their treatment history for DM. In addition, BMI, systolic blood pressure (SBP), diastolic blood pressure (DBP), venous blood tests, and ophthalmologic examinations were performed on each patient. BMI was calculated as weight in kilograms divided by the square of height in meters. Venous blood was obtained for measurement of HbA1C, serum triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), total cholesterol (TC), blood urea nitrogen (BUN), and serum creatinine. Ophthalmologic examinations included assessment of best-corrected visual acuity (BCVA) using a logarithm of the mild angle of resolution (LogMAR), intraocular pressure (IOP) measurement, slit-lamp biomicroscopy, axial length (AL) measurement and three ophthalmoscopy methods, including slit-lamp biomicroscopy with a fundus pre-set lens, color fundus photographs (KOWA nonmyd α-DIII, 8300, Japan) and panoramic wide-angle laser fundus camera (ophthalmoscope-Daytona, P200T, Optos, UK). One masked specialist (LY) used the three ophthalmoscopy methods to confirm the subgroups (NDR or MDR). Healthy controls were recruited during the same study period from subjects who received annual eye examinations or from the family members of the patients.
OCT-A measurements and segmentation
All the enrolled subjects were imaged by an OCT-A system (Optovue, RTVueXR Avanti; Optovue, Inc., Fremont, CA, USA). The Optovue takes 304 × 304 volumetric A-scans at 70,000 A-scans per second, which uses the proprietary split-spectrum amplitude-decorrelation angiography (SSADA) algorithm to produce detailed images and to minimize scan acquisition time. Dense horizontal and vertical raster cubes are acquired and combined by a proprietary algorithm to reduce motion artifacts. All subjects used Motion Correction Technology to reduce motion artifact for ultra-high resolution images for the 3 × 3 mm image acquisition area centered on the fovea. The OCT instrument automatically detected and separated the retina vascular layer into the superficial and deep retinal capillary plexuses (SRCL, DRCL, respectively). The superficial retinal capillary layer extended from 3 μm below the internal limiting membrane to 15 μm below the inner plexiform layer (IPL). The deep retinal capillary layer extended from 15 to 70 μm below the IPL, which included both the intermediate and deep capillary plexus. If there was an obvious deviation for the segmentation obtained by the OCT-A system, the segmentation lines were then adjusted manually.
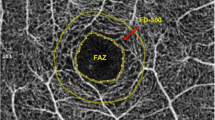
RCD (%) was defined as the proportion of the measured area occupied by perfused vessels, which was defined as pixels having signal acquired by the SSADA algorithm. It was used to characterize the vascular structural information and was calculated on the imported raw OCT-A images in PNG format by our custom automated algorithm, as described in our previous study [27]. The grayscale of each two-dimensional OCT-A image was first extended by bicubic interpolation to 1024 × 1024 pixels to enhance image details. Next, a two-way combined method consisting of a canny edge detector algorithm and a level set algorithm was used to detect the boundary of FAZ. The area within the FAZ, having a circle of fixed radius (diameter = 0.6 mm), was then determined to establish the baseline signal to-noise ratio for global thresholding. This image was then separately processed to generate two binary images by global thresholding and adaptive thresholding: the first image contained only the large blood vessels. The other binary image contained large and small vessels. The two resulting binary vessel maps were subtracted to obtain a binary image containing only the small vessels. RCD was then calculated for the 2.5 mm diameter zone after excluding the FAZ (diameter = 0.6 mm). All the above methods were performed using MATLAB v.2015a (Mathworks Inc., Natick, MA, USA).
Statistical analysis
All data were expressed as the mean ± standard deviation. One-way analysis of variance (ANOVA) was used to test for differences among groups. Chi-squared test was used to test for differences in sex, eye laterality, smoking history, alcohol and insulin therapy. The diabetic group, including NDR and MDR, were divided into two new-subgroups, according to each individual characteristic, hyperglycemia, and complications related to diabetes, respectively. The relationships between the RCD and systemic factors were evaluated by the differences between each newly divided subgroup. All data were analyzed with SPSS software (version 23.0; SPSS Inc., Chicago, Illinois, USA). P values < 0.05 were considered statistically significant.
Results
A total of 212 eyes from 212 subjects were recruited, including type 2 DM (126 eyes) and 86 healthy participants (86 eyes). Segmentation lines were adjusted manually for 20 images from 10 eyes due to their obvious deviation errors. From the diabetic eyes, 90 eyes had NDR and 36 had MDR, respectively. There were no statistically significant differences in the demographic characteristics among the three groups, except for the BCVA (P < 0.001) and SBP (P = 0.031) (Table 1).
Raw OCT-A and their corresponding postprocessed binary images of the superficial and deep retinal capillary layers in the control eyes, and in the eyes of diabetic patients with NDR and MDR were acquired (Fig. 1).

Representative optical coherence tomography angiography (OCT-A) and postprocessed images for a control, diabetes without retinopathy (NDR) and diabetes with mild retinopathy (MDR) eyes illustrating the automated analysis algorithm. Original OCT-A images of the superficial retinal capillary layers of control (a), NDR (e) and MDR (i) eyes and binary images of the capillary plexus after removing background noise and larger vessels of control (b), NDR (f) and MDR (j) eyes. Original OCT-A images of the deep retinal capillary layers of control (c), NDR (g) and MDR (k) eyes and Binary images of the capillary plexus after removing background noise of control (d), NDR (h) and MDR (l) eyes. Control, control eyes; NDR, diabetic patients with no DR; MDR, diabetic patients with mild DR; SRCL, superficial retinal capillary layer; DRCL, deep retinal capillary layer; BI: binary images
Retinal capillary density in three groups
As shown in Table 2 and Fig. 2, there were significant differences of the RCDs both in SRCL and DRCL among the three groups. In SRCL, the mean RCD was significantly lower in diabetic patients with MDR (41.0 ± 2.7%) compared with the NDR (42.4 ± 3.0%, P = 0.004, Table 2, Fig. 2) and healthy groups (43.9 ± 1.8%, P < 0.001, Table 2, Fig. 2). Moreover, there was also a statistically significant decrease of RCD in the NDR group compared with healthy participants (P < 0.001, Table 2, Fig. 2). In DRCL, the mean RCD in patients with MDR (46.6 ± 6.1%) was also significantly deceased compared with the NDR (49.9 ± 5.8%, P = 0.001) and healthy groups (52.6 ± 3.0%, P < 0.001 Table 2, Fig. 2). There was also a statistically significant decrease in RCD in the NDR group compared with the healthy groups (P < 0.001, Table 2, Fig. 2).

Comparisons of the retinal capillary density (RCD) in diabetic patients with controls on OCT-A images in the superficial and deep retinal capillary layers (SRCL and DRCL). The RCDs in the SRCL (a) and DRCL (b) of both the no DR (NDR) group and the mild DR (MDR) group were lower than those of the control group. In addition, the RCDs in the MDR group were also decreased compared to those of the NDR group. *P < 0.05, **P < 0.01, ***P < 0.001
Influence of individual characteristics
The diabetic group, including NDR and MDR, was divided into two new-subgroups, according to each individual characteristic, such as age (<55y or > 55y), sex (male or female), BMI (< 25 kg/m2 or > 25 kg/m2), history of smoking and alcohol consumption (yes or no, respectively). In SRCL, when comparing the two newly formed diabetic subgroups with healthy controls, the RCDs of each diabetic subgroup were significantly deceased (all P < 0.01). However, the RCD in SRCL was not significantly decreased between the two diabetic subgroups (P > 0.05). In DRCL, the RCDs of each diabetic subgroup were also significantly decreased compared to those in the control group (all P < 0.05). In addition, when comparing each diabetic subgroup, the RCDs were significantly decreased in those with age > 55y compared with those with age < 55y in the DRCL (P < 0.001, Table 3, Fig. 3). No significant difference was seen between the diabetic subgroups when other individual characteristics were evaluated (P > 0.05).

Comparisons of the retinal capillary density (RCD) in diabetic subgroups grouped by major risk factors with controls on OCT-A images in the superficial and deep retinal capillary layers (SRCL and DRCL). The RCDs in SRCL and the DRCL of diabetic subgroups grouped by major risk factors were lower than those of the control group. In addition, the RCDs in the diabetic groups with age > 55y (a), HbA1c > 7% (b), LDL-C > 3.1 mmol/L (c), or BUN > 8.2 mmol/L (d) were also decreased compared to those of the other groups. *P < 0.05, **P < 0.01, ***P < 0.001
Influence of hyperglycemia
The diabetic group, including NDR and MDR, was further divided according to hyperglycemia, which included the duration of diabetes (< 5y or > 5y), insulin treatment (yes or no) and HbA1c level (< 7% or > 7%). In SRCL, when comparing two new diabetic subgroups with controls, there was a significantly reduced RCD in two new diabetic subgroups in all sectors of SRCL (all P < 0.05). There was no significant difference (P > 0.05) when both subgroups of the diabetics were compared. In DRCL, the two new diabetic subgroups had lower RCD in DRCL compared with the controls (P < 0.05). Moreover, when the two diabetic groups were compared, the RCDs in DRCL in the diabetic subgroup with HbA1c > 7% were lower than those with HbA1c < 7% (P < 0.05, Table 3, Fig. 3).
Influence of complications related to diabetes
In addition, the diabetic group was also divided according to various characteristics of complications related to diabetes, which included hypertension (SBP < 140 mmHg or > 140 mmHg, and DBP < 90 mmHg or > 90 mmHg), hyperlipidemia (TG < 1.7 mmol/L or > 1.7 mmol/L, TC < 5.2 mmol/L or > 5.2 mmol/L, HDL-C < 1.96 mmol/L or > 1.96 mmol/L, and LDL-C < 3.1 mmol/L or > 3.1 mmol/L) and renal dysfunction (BUN < 8.2 mmol/L or > 8.2 mmol/L, and Creatinine < 70 μmol/L or > 70 μmol/L). The SRCL showed significantly reduced (P < 0.05) RCD in each diabetic subgroup when compared to the controls with SBP, DBP, TG, TC, LDL-C, BUN and creatinine used as the parameters. When compared between each diabetic subgroup, the RCDs in SRCL in the diabetic subgroup with LDL-C > 3.1 mmol/L and BUN > 8.2 mmol/L were lower than those with LDL-C < 3.1 mmol/L and BUN < 8.2 mmol/L, respectively (P < 0.05, Table 3, Fig. 3). In DRCL, the RCDs of each diabetic subgroup were significantly reduced (P < 0.05) when compared to the healthy controls with SBP, DBP, TG, TC, LDL-C, BUN and creatinine evaluated as parameters. Furthermore, when compared between each diabetic subgroup according to various characteristics of complications related to diabetes, the RCDs in DRCL in the subgroup with BUN > 8.2 mmol/L were also lower than the other subgroup (P < 0.05, Table 3, Fig. 3).
We also determined whether diabetic retinopathy was correlated with RCD when adjusted for other factors. For all diabetes subjects (included NDR and MDR), multiple linear regressions showed that RCD in SRCL (P = 0.027) and DRCL (P < 0.001) was independently and negatively correlated with age after adjustment for other risk factors.
Discussion
In this cross-sectional study, we demonstrated retinal capillary loss in type 2 diabetic patients with and without mild retinopathy by quantifying RCD using OCT-A. Additionally, we found that type 2 diabetic patients who were older, had higher HAb1c, LDL-C and BUN, had more severe capillary abnormalities. The ability of the indicator to quantify the impairment of retinal capillary network in diabetic patients especially in patients without clinical DR, has important implications for the early detection and prevention of retinopathy, and the understanding of the pathophysiological mechanisms underlying DR development [5, 6, 28]. The present study demonstrated that the RCD in diabetic patients without clinical DR was decreased compared with non-diabetic eyes, which was consistent with our previous study using the FD value [27]. However, Nesper et al. [29] reported that there was no significant difference in retinal vessel densities between the NDR patients and controls. One possible reason for such discrepancy might be whether the large vessels in the OCT-A images were removed in the analysis of retinal vessel density. In our study, the custom automated algorithm helped in the extraction of large vessels and the density of the capillaries were measured, which were also used in the previous study [30]. To the best of our knowledge, this is the first study to investigate the relationships between this early indicator and various diabetic risk factors, where we found that decreased RCD had a negative correlation with increasing age, and those with higher HAb1c, LDL-C and BUN.
Although studies have reported that intense glycemic control can prevent and delay the initiation of diabetic retinopathy [31, 32], the close association between diabetes and the prevalence of microvascular complications was also demonstrated [25, 31, 33, 34]. Some other studies found a substantial incidence of retinopathy, even among patients with good glycemic control [35]. Previous studies have shown that both increased FAZ and decreased vessel density were associated with worsening DR severity, including NDR/mild/moderate/severe non-proliferative DR and proliferative DR, using OCT-A [22,23,24, 29, 36]. Our study also showed decreased RCD in diabetic patients with mild DR compared with patients without retinopathy and controls. The decreased RCD in the early stages, reflecting ischemia of the macula, might be associated with the initiation of impaired retinal microvasculature in diabetic patients. Therefore, our results support the hypothesis that the RCD of the macula quantified by OCT-A may be a sensitive indicator of early retinal microvascular damage in diabetes even before the clinical signs of diabetic retinopathy occur.
Type 2 diabetic patients have a significant risk of blindness from diabetic retinopathy and are at higher risk of developing cardiovascular disease and mortality related to systematic microvascular complications [1, 2, 37, 38]. The current study investigated the associations between the early impairment of the retinal microvasculature and the risk factors of patients with type 2 DM, which might have a potential value for guiding clinicians. We found that only age, HbA1c, LDL-C and BUN levels have an obvious and reliable influence on the decreased RCD, especially in the DRCL, after we divided the diabetic patients into two subgroups by various risk factors. Wei et al. [39] investigated the age-related alterations in retinal microvascular network in healthy subjects using OCT-A and found that the retinal vessel density decreased during aging. The results were similar with those obtained in our study, even though the subjects of the current study were diabetic patients and the other risk factors of which might have some extra effect on the impairment of retinal microvasculature. Therefore, a huge database of age-matched healthy subjects as a reference is important in the clinical diagnosis of the microvascular damage of diabetic patients. As shown in our study which enrolled age-matched control subjects, the decreased RCD found in diabetic patients with and without MDR may represent a novel and specific biomarker for evaluating the early presence of microvascular damage related to type 2 DM. Dieren et al. [32] indicated that effective glycemic control was related to decreasing HbA1c levels. Cheung et al. [1] reported that a 1% decrease in glycated HbA1c might be roughly equal to a 40% decrease risk of retinopathy. In the present study, we also found that the HbA1c level of more than 7%, reflecting poor long-term blood sugar control, also had a major influence on the impairment of retinal microvessels in diabetic patients. In addition, we found that increasing LDL-C was another significant risk factor for decreasing the RCD and might aggravate the damage of retinal microvasculature in type 2 diabetic patients, which is consistent with previous studies. Papavasileiou et al. [40] reported that higher total and LDL cholesterol were associated with the presence of hard exudates, and a greater hard exudate area was measured in the fundus photographs in African Americans with type 2 DM. Ting et al. [24] found that hyperlipidemia was also associated with a reduced capillary density index using a swept-light source OCT-A device. Ivers et al. [41] demonstrated that diabetics with longer duration, and insulin treatment had a significantly increased risk for DR, however, this was not detected in the early stage of diabetic patients of our study. Therefore, diabetic patients with different severities of retinopathy in the two studies might be one of the main reasons for the discrepancy.
In our study, the more significant decreases of RCD in diabetic subgroups were found to occur in the DRCL compared to those in the SRCL. This may be attributed to the different characteristics of anatomical structures in the two layers. In fact, the DRCL has more abundant smaller vessels than the SRCL [42, 43]. In our previous study, we found that fractal dimensions had larger areas under the ROC curve in the DRCL than the SRCL, which indicated a higher diagnostic value [27]. Perhaps capillary vasoconstriction in the deep retinal capillary layer occurs earlier or more frequently to compensate for the reduced blood flow and the resulting hypoxia and ischemia in early DM, which has been reported in previous studies [27, 43, 44]. Moreover, in the present study, we found that the diabetic patients who were older, or with higher HbA1c, TG, LDL-C and BUN level had decreased RCD in the retina, especially in the DRCL. These might demonstrate that protection and treatment of the microvasculature in the DRCL in the early stage of DM are of a particular value.
Our study, however, has some limitations. First, the cross-sectional and non-interventional natures of the study limits our ability to determine the role of OCT-A in the prediction of incidence and progression of DR. A longitudinal study with a larger sample size is needed to further investigate the clinical utility of retinal capillary measurements based on OCT-A images as a potential tool to evaluate the early impairment of diabetic microvasculature in the future. Secondly, a venous blood test was not performed in the control subjects. Therefore, it cannot be excluded that some of the controls had undetected Type 2 DM or other systematic diseases. However, this may not impact our results because the non-diagnosed controls would most likely have led to an underestimate of the difference in RCD between the diabetic patients and the controls rather than an overestimate. In addition, although the OCT-A provided improved visualization of the superficial and deep capillary networks compared to FA, the current technology of OCT-A is limited by a small field of view (3 × 3 mm2). This may limit our understanding of the vascular changes in the peripheral retina in the early stages of DR. Finally, the present study showed that RCD in SRCL (P = 0.027) and DRCL (P < 0.001) was independently and negatively correlated with age after adjusting for other risk factors by multiple linear regression. The result showed it was indispensable that the interaction of age with other risk factors should to be considered in the future study. The lack of correlations among the other risk factors and RCD may be due to the small sample sizes, and thus further studies with larger populations are warranted.
Conclusions
In summary, this study demonstrated, using OCT-A, that lower RCD (equating to more impaired vessels) were found in diabetic patients with and without mild DR. Aging, higher HbA1c, LDL-C and BUN level were found to be the major risk factors in the retinal microvascular impairment of type 2 diabetic patients, and OCT-A is considered to be a promising approach to detect early microvasculature impairment in diabetic patients by noninvasively evaluating capillary perfusion.
Availability of data and materials
All relevant data are within the paper and its supporting information files.
References
Cheung N, Mitchell P, Wong TY. Diabetic retinopathy. Lancet. 2010;376(9735):124–36.
Fong DS, Aiello L, Gardner TW, King GL, Blankenship G, Cavallerano JD, et al. Diabetic retinopathy. Diabetes Care. 2003;26(Suppl 1):S99–S102.
Grauslund J, Green A, Kawasaki R, Hodgson L, Sjølie AK, Wong TY. Retinal vascular fractals and microvascular and macrovascular complications in type 1 diabetes. Ophthalmology. 2010;117(7):1400–5.
Klein BE. Overview of epidemiologic studies of diabetic retinopathy. Ophthalmic Epidemiol. 2007;14(4):179–83.
Tiedeman JS, Kirk SE, Srinivas S, Beach JM. Retinal oxygen consumption during hyperglycemia in patients with diabetes without retinopathy. Ophthalmology. 1998;105(1):31–6.
Lorenzi M. The polyol pathway as a mechanism for diabetic retinopathy: attractive, elusive, and resilient. Exp Diabetes Res. 2007;2007:61038.
Blaslov K, Bulum T, Duvnjak L. The role of endothelial dysfunction driven by adipocitokines in the development and progression of microvascular complications in patients with type 1 and type 2 diabetes. Med Hypotheses. 2015;84(6):593–5.
Bursell SE, Clermont AC, Oren B, King GL. The in vivo effect of endothelins on retinal circulation in nondiabetic and diabetic rats. Invest Ophthalmol Vis Sci. 1995;36:596–607.
Klein R, Klein BE, Moss SE, Wong TY, Hubbard L, Cruickshanks KJ, et al. The relation of retinal vessel caliber to the incidence and progression of diabetic retinopathy: XIX: the Wisconsin Epidemiologic Study of Diabetic Retinopathy. Arch Ophthalmol. 2004;122(1):76–83.
Avakian A, Kalina RE, Sage EH, Rambhia AH, Elliott KE, Chuang EL, et al. Fractal analysis of region-based vascular change in the normal and non-proliferative diabetic retina. Curr Eye Res. 2002;24(4):274–80.
Kwiterovich KA, Maguire MG, Murphy RP, Schachat AP, Bressler NM, Bressler SB, et al. Frequency of adverse systemic reactions after fluorescein angiography. Results of a prospective study. Ophthalmology. 1991;98(7):1139–42.
Cheung CY, Lamoureux E, Ikram MK, Sasongko MB, Ding J, Zheng Y, et al. Retinal vascular geometry in Asian persons with diabetes and retinopathy. J Diabetes Sci Technol. 2012;6:595–605.
Lim SW, Cheung N, Wang JJ, Donaghue KC, Liew G, Islam FM, et al. Retinal vascular fractal dimension and risk of early diabetic retinopathy: a prospective study of children and adolescents with type 1 diabetes. Diabetes Care. 2009;32(11):2081–3.
Yau JW, Kawasaki R, Islam FM, Shaw J, Zimmet P, Wang JJ, et al. Retinal fractal dimension is increased in persons with diabetes but not impaired glucose metabolism: the Australian Diabetes, Obesity and Lifestyle (AusDiab) study. Diabetologia. 2010;53:2042–5.
Mendis KR, Balaratnasingam C, Yu P, Barry CJ, McAllister IL, Cringle SJ, et al. Correlation of histologic and clinical images to determine the diagnostic value of fluorescein angiography for studying retinal capillary detail. Invest Ophthalmol Vis Sci. 2010;51(11):5864–9.
Kashani AH, Chen CL, Gahm JK, Zheng F, Richter GM, Rosenfeld PJ, et al. Optical coherence tomography angiography: a comprehensive review of current methods and clinical applications. Prog Retin Eye Res. 2017;60:66–100.
de Carlo TE, Romano A, Waheed NK, Duker JS. A review of optical coherence tomography angiography (OCTA). Int J Retina Vitreous. 2015;1:5.
Jia Y, Bailey ST, Wilson DJ, Tan O, Klein ML, Flaxel CJ, et al. Quantitative optical coherence tomography angiography of choroidal neovascularization in age-related macular degeneration. Ophthalmology. 2014;121(7):1435–44.
Gadde SG, Anegondi N, Bhanushali D, Chidambara L, Yadav NK, Khurana A, et al. Quantification of vessel density in retinal optical coherence tomography angiography images using local fractal dimension. Invest Ophthalmol Vis Sci. 2016;57(1):246–52.
Samara WA, Shahlaee A, Adam MK, Khan MA, Chiang A, Maguire JI, et al. Quantification of diabetic macular ischemia using optical coherence tomography angiography and its relationship with visual acuity. Ophthalmology. 2017;124(2):235–44.
Jia Y, Bailey ST, Hwang TS, McClintic SM, Gao SS, Pennesi ME, et al. Quantitative optical coherence tomography angiography of vascular abnormalities in the living human eye. Proc Natl Acad Sci U S A. 2015;112(18):E2395–402.
Kim AY, Chu Z, Shahidzadeh A, Wang RK, Puliafito CA, Kashani AH. Quantifying microvascular density and morphology in diabetic retinopathy using spectral-domain optical coherence tomography angiography. Invest Ophthalmol Vis Sci. 2016;57(9):OCT362–70.
Durbin MK, An L, Shemonski ND, Soares M, Santos T, Lopes M, et al. Quantification of retinal microvascular density in optical coherence tomographic angiography images in diabetic retinopathy. JAMA Ophthalmol. 2017;135(4):370–6.
Ting DSW, Tan GSW, Agrawal R, Yanagi Y, Sie NM, Wong CW, et al. Optical coherence tomographic angiography in type 2 diabetes and diabetic retinopathy. JAMA Ophthalmol. 2017;135(4):306–12.
Yau JW, Rogers SL, Kawasaki R, Lamoureux EL, Kowalski JW, Bek T, et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35:556–64.
Wilkinson CP, Ferris FL 3rd, Klein RE, Lee PP, Agardh CD, Davis M, et al. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology. 2003;110(9):1677–82.
Chen Q, Ma Q, Wu C, Tan F, Chen F, Wu Q, et al. Macular vascular fractal dimension in the deep capillary layer as an early indicator of microvascular loss for retinopathy in type 2 diabetic patients. Invest Ophthalmol Vis Sci. 2017;58(9):3785–94.
Carnevali A, Sacconi R, Corbelli E, Tomasso L, Querques L, Zerbini G, et al. Optical coherence tomography angiography analysis of retinal vascular plexuses and choriocapillaris in patients with type 1 diabetes without diabetic retinopathy. Acta Diabetol. 2017;54(7):695–702.
Nesper PL, Roberts PK, Onishi AC, Chai H, Liu L, Jampol LM, et al. Quantifying microvascular abnormalities with increasing severity of diabetic retinopathy using optical coherence tomography angiography. Invest Ophthalmol Vis Sci. 2017;58(6):BIO307–15.
Yang Y, Wang J, Jiang H, Yang X, Feng L, Hu L, et al. Retinal microvasculature alteration in high myopia. Invest Ophthalmol Vis Sci. 2016;57(14):6020–30.
Ohkubo Y, Kishikawa H, Araki E, Miyata T, Isami S, Motoyoshi S, et al. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: a randomized prospective 6-year study. Diabetes Res Clin Pract. 1995;28(2):103–17.
van Dieren S, Kengne AP, Chalmers J, Beulens JW, Davis TM, Fulcher G, et al. Intensification of medication and glycaemic control among patients with type 2 diabetes - the ADVANCE trial. Diabetes Obes Metab. 2014;16:426–32.
Sacks FM, Hermans MP, Fioretto P, Valensi P, Davis T, Horton E, et al. Association between plasma triglycerides and high-density lipoprotein cholesterol and microvascular kidney disease and retinopathy in type 2 diabetes mellitus: a global case-control study in 13 countries. Circulation. 2014;129:999–1008.
Ting DS, Cheung GC, Wong TY. Diabetic retinopathy: global prevalence, major risk factors, screening practices and public health challenges: a review. Clin Exp Ophthalmol. 2016;44:260–77.
Rodríguez-Gutiérrez R, Montori VM. Glycemic control for patients with type 2 diabetes mellitus: our evolving faith in the face of evidence. Circ Cardiovasc Qual Outcomes. 2016;9(5):504–12.
Takase N, Nozaki M, Kato A, Ozeki H, Yoshida M, Ogura Y. Enlargement of foveal avascular zone in diabetic eyes evaluated by en face optical coherence tomography angiography. Retina. 2015;35(11):2377–83.
Sivaprasad S, Gupta B, Crosby-Nwaobi R, Evans J. Prevalence of diabetic retinopathy in various ethnic groups: a worldwide perspective. Surv Ophthalmol. 2012;57:347–70.
Kyari F, Tafida A, Sivasubramaniam S, Murthy GV, Peto T, Gilbert CE, et al. Prevalence and risk factors for diabetes and diabetic retinopathy: results from the Nigeria national blindness and visual impairment survey. BMC Public Health. 2014;14:1299.
Wei Y, Jiang H, Shi Y, Qu D, Gregori G, Zheng F, et al. Age-related alterations in the retinal microvasculature, microcirculation, and microstructure. Invest Ophthalmol Vis Sci. 2017;58:3804–17.
Papavasileiou E, Davoudi S, Roohipoor R, Cho H, Kudrimoti S, Hancock H, et al. Association of serum lipid levels with retinal hard exudate area in African Americans with type 2 diabetes. Graefes Arch Clin Exp Ophthalmol. 2017;255(3):509–17.
Ivers RQ, Cumming RG, Mitchell P, Peduto AJ. Blue Mountains Eye Study. Diabetes and risk of fracture: the Blue Mountains Eye Study. Diabetes Care. 2001;24(7):1198–203.
Savastano MC, Lumbroso B, Rispoli M. In vivo characterization of retinal vascularization morphology using optical coherence tomography angiography. Retina. 2015;35(11):2196–203.
McLenachan S, Magno AL, Ramos D, Catita J, McMenamin PG, Chen FK, et al. Angiography reveals novel features of the retinal vasculature in healthy and diabetic mice. Exp Eye Res. 2015;138:6–21.
Scarinci F, Nesper PL, Fawzi AA. Deep retinal capillary nonperfusion is associated with photoreceptor disruption in diabetic macular ischemia. Am J Ophthalmol. 2016;168:129–38.
Acknowledgements
We thank William Robert Kwapong, PhD, Wenzhou Medical University for providing editing services for this manuscript and thank Jingwei Zheng, MD, Wenzhou Medical University for statistical consultation for data analysis.
Funding
This study was supported by research grants from the National Key Research and Development Program of China (2016YFC0102500, 2016YFE0107000), the Key R&D Program Projects in Zhejiang Province (2019C03045), Zhejiang Provincial Natural Science Foundation of China (LY19H120003), the National Nature Science Foundation of China (Grant No. 81570880) and Public Service Program of Wenzhou Science and Technology Bureau (Y20160151).
Author information
Authors and Affiliations
Contributions
Design of the study (MS, QC, FT, FL); Conduct of the study, data collection, analysis and interpretation (FT, QC, XZ, CW, YQ, YL, YW); Manuscript preparation and review (MS, QC, FT, FL). All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study had been approved by the ethics committee of the Eye Hospital of Wenzhou Medical University, and followed the tenets of the Declaration of Helsinki (KYK 2017 [41]).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Tan, F., Chen, Q., Zhuang, X. et al. Associated risk factors in the early stage of diabetic retinopathy. Eye and Vis 6, 23 (2019). https://doi.org/10.1186/s40662-019-0148-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40662-019-0148-z