
Abstract
Background
For subsolid non-small cell lung cancers (NSCLCs), solid size (SS), which is the maximal diameter of the solid component, correlates more accurately with tumor prognosis than the total size, which is the maximal diameter of the entire tumor, including ground-glass opacity. We reviewed the propriety of the TNM staging based on the SS for early-stage NSCLCs.
Methods
We retrospectively reviewed the preoperative radiological reports, clinical records, and pathological reports of NSCLC cases in our hospital between 2010 and 2013, and clinical stage (c-Stage) 0 and I tumors were selected. Disease-free survival (DFS), based on survival analysis, was used to assess the tumor characteristics that predicted the prognosis.
Results
A total of 247 NSCLC diagnoses in 231 patients (88 women and 143 men; age, 67 ± 7 years) were included in our cohort. They were classified into solid (n = 131) and subsolid (n = 116) nodules. The DFS curves indicated that prognosis was significantly worse in the following order: c-Stage 0, c-Stage IA, and c-Stage IB tumors (p = 0.016). Patients with solid nodules showed a significantly worse prognosis than patients with subsolid nodules (p < 0.001). A multivariate Cox proportional hazards model showed that the significant predictive factors for DFS were c-Stage (hazard ratio, 1.600; p = 0.020) and solid nodules (hazard ratio, 3.077; p = 0.031).
Conclusions
For early-stage NSCLCs, the c-Stage based on the SS in subsolid nodules was useful for predicting postoperative DFS. In addition, whether nodules were solid or subsolid was another independent prognostic factor.
Similar content being viewed by others


Background
It is well known that the prognosis of non-small cell lung cancer (NSCLC) with masses equal to or less than 3 cm in diameter is favorable [1, 2]. Therefore, localized tumors that meet this criteria on computed tomography (CT) images without nodes or distant metastases are considered early-stage cancers (clinical T1aN0M0; stage IA), according to the tumor–node–metastasis (TNM) classification of the Union for International Cancer Control (UICC) [3].
NSCLCs are classified clinically into solid nodules, including only solid components, and subsolid nodules, including ground-glass opacity (GGO) components, based on thin-section CT findings. Some previous studies have focused on the solid component that reflects the intra-tumoral collapse of the airspace or fibrosis within the subsolid nodules and have demonstrated that the solid size (SS), which is the maximal diameter of the solid component, correlates with tumor invasiveness and patient prognosis [4,5,6,7]. Therefore, SS measurements have been adopted as the clinical T factor and clinical staging (c-Stage) in the latest UICC (8th version) of the TNM classification [8]. For solid nodules, the total size (TS) measurement, which is equal to the SS, has been adopted as before. On the other hand, a recent study by Hattori et al. indicated that the presence of a GGO component in the tumor was an index of favorable prognosis [9, 10].
In the present study, we retrospectively evaluated whether the clinical staging based on the 8th version of the UICC could reflect the postoperative prognosis of patients with small NSCLC. In addition, differences in prognoses between patients with solid- and subsolid-type lung cancers were verified.
Methods
This retrospective study was approved by our Institutional Review Board, and written informed consent was waived (approval no. 2017–0437).
Patient selection
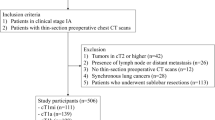
Using the retrieval function of picture archiving and communication systems, we searched our institutional database for CT, positron emission tomography/CT, and pathological reports on patients with pathologically confirmed, surgically resected primary lung cancer between August 2010 and December 2013. During this period, 596 surgeries for lung cancer were performed in our institution. Based on the preoperative CT reports, radiologic information obtained from thin-section CTs included clinical TS, ratio of consolidation to tumor (C/T ratio), location of tumor, and c-Stage based on the TNM classification in the 7th version of UICC. Solid nodules were defined as those with a C/T ratio of 100%, whereas subsolid nodules were defined as those with a C/T ratio < 100%. Based on the TS and C/T ratios, the SSs of subsolid nodules were calculated, and the c-Stage was transferred from the 7th to 8th version definitions. Moreover, we selected NSCLCs measuring ≤3.0 cm in SS. Tumors that did not have information about the c-Stage were excluded from our cohort.
The clinical records of all selected cases were reviewed to obtain data on the patients’ age, sex, date of surgery, operative procedure performed, and postoperative course. Lobectomy was regarded as standard surgery, and wide wedge resection and segmentectomy were regarded as limited surgeries. The patients were scheduled for follow-ups every 1 to 3 months for 2 years after the surgery and every 6 months thereafter. In patients with a high risk of recurrence, a CT of the chest and abdomen was performed every 6 to 12 months, according to the physician’s recommendation. When recurrence was suspected, additional imaging surveys were performed.
Statistical analysis
Disease-free survival (DFS) was assessed using the Kaplan–Meier method, and the survival curves for each group were compared using the log-rank test. DFS was defined as the interval between the surgery and the first disease recurrence, including local recurrence and distant metastasis, or death from any cause. In patients with multiple synchronous lung cancers, the tumor with the highest c-Stage was deemed to have relapsed. On univariate and multivariate analyses of DFS, the Cox proportional hazards model was used to assess the effects of tumor characteristics as potential prognostic factors.
Statistical analysis was performed using the commercial software SPSS version 23 (IBM Corp., Armonk, NY, USA). A p-value < 0.05 was considered statistically significant.
Results
A total of 247 NSCLC cases in 231 patients (88 women and 143 men; average ± standard deviation of age, 67 ± 7 years) were included in this study. Sixteen patients had synchronous tumors. Thin-section CT findings included solid (n = 131) and subsolid (n = 116) nodules. Table 1 shows the correlation between the 7th and 8th version definitions of the c-Stage. The postoperative histopathologic diagnoses were adenocarcinoma (n = 203), squamous cell carcinoma (n = 28), adenosquamous carcinoma (n = 9), large-cell carcinoma (n = 5), mucoepidermoid carcinoma (n = 1), and adenoid cystic carcinoma (n = 1). Postoperative recurrence was observed in 30 patients. Tumor-related or unexplained deaths were observed in 18 patients. The other patient and tumor characteristics are shown in Table 2.
Kaplan–Meier curves for DFS of all patients with NSCLC showed a significant difference among those with c-Stage 0, IA, and IB tumors (p = 0.016, Fig. 1), and patients with c-Stage 0 tumors showed a better prognosis than those with c-Stage IA and IB tumors. According to the subgroup of c-Stage IA tumors, there were significant differences among c-Stage IA1, IA2, and IA3 (p = 0.011, Fig. 2); patients with c-Stage IA1 tumors showed a better prognosis than those with c-Stage IA2 and IA3 tumors. In addition, patients with subsolid tumors showed a significantly better prognosis than those with solid tumors (p < 0.001, Fig. 3a). Patients with subsolid tumors showed a significantly better prognosis than patients with solid tumors among the c-Stage IA tumors (p = 0.026, Fig. 3b), and patients with subsolid tumors showed a better prognosis than patients with solid tumors among the c-Stage IB tumors, although significant differences were not observed (p = 0.102, Fig. 3c). Univariate and multivariate Cox proportional hazards models indicated that the patients’ age, c-Stage, and presence of solid nodules were significant factors that correlated with the postoperative prognosis, although the patients’ sex and operative procedures performed were not significant (Table 3). In the subgroup of adenocarcinomas, univariate and multivariate Cox proportional hazards models indicated that the c-Stage and presence of solid nodules were significant factors correlated with postoperative prognosis (Table 4).

The graph shows Kaplan-Meier curves for disease-free survival according to clinical stage 0-IB. There is a significant difference among c-Stage 0, IA, and IB tumors (p = 0.016)

The graph shows Kaplan-Meier curves for disease-free survival according to the subgroup of clinical stage IA tumors. There is a significant difference among c-Stage IA1, IA2, and IA3 tumors (p = 0.011)

The graph shows Kaplan-Meier curves for disease-free survival according to the subgroup of solid tumors and subsolid tumors. For all tumors (a) and clinical stage IA tumors (b), patients with subsolid tumors show a significantly better prognosis than those with solid tumors (p < 0.001 and p = 0.026, respectively). For clinical stage IB (c), patients with subsolid tumors show a better prognosis than patients with solid tumors among the clinical stage IB tumors, although significant differences were not observed (p = 0.102)
Discussion
The present study showed that the 8th version of the UICC of the TNM classification based on SS measurements in subsolid lung cancers on a multidetector CT accurately correlated with postoperative recurrence in patients with c-Stage 0, IA, and IB NSCLCs. In patients with c-Stage IA, the TNM classification based on SS measurements accurately correlated with postoperative recurrence. The prognosis of patients with c-Stage IA1 tumors with SS ≤1.0 cm was as excellent as that of patients with c-Stage 0 tumors that were regarded as noninvasive tumors. The multivariate Cox proportional hazards model indicated that the c-Stage could independently predict the postoperative prognosis.
Our study also showed whether solid or subsolid nodules also correlated significantly with patient prognosis. In patients with c-Stage IA tumors with SS ≤3.0 cm, patients with subsolid nodules showed significantly better prognosis than that of patients with solid nodules. Our results are consistent with the results of a previous study by Hattori et al. that showed that the presence of a GGO component within a tumor indicates favorable prognosis in patients with c-Stage IA NSCLC [9, 10]. In c-Stage IB tumors with pleural invasion and/or SS > 3 cm, patients with subsolid nodules showed tendencies of a better prognosis than those of patients with solid nodules on the Kaplan–Meier curves, although significant differences were not observed. Multivariate analysis demonstrated that the presence of solid/ subsolid nodules was a significant independent factor for DFS, as with age and c-Stage. Subsolid nodules are mainly composed of adenocarcinomas, in which GGO reflects the replacement of the alveolar epithelium by well-differentiated tumor cells. On the other hand, solid nodules include squamous cell carcinomas and large cell carcinomas, besides adenocarcinomas. Since squamous cell carcinomas, adenosquamous carcinomas, and large cell carcinomas are more invasive and malignant than adenocarcinomas, these histopathological types might lead to a worse prognosis in patients with solid nodules [1, 11,12,13,14]. Therefore, we surveyed only adenocarcinomas and found that the c-Stage and presence of solid/subsolid nodules were significant factors for DFS, even within the subgroup. The presence or absence of a GGO component could have a strong influence on the prognosis, even in patients with adenocarcinoma.
A recent study proved that the concordance rate between the c-Stage and pathological stage (p-Stage) of the 7th version of the UICC for small lung cancers had moderate reproducibility, and p-Stage but not c-Stage was a significant prognostic indicator of DFS upon multivariate analysis [15]. For c-Stage I NSCLCs, stereotactic radiotherapy (SRT) has been recently shown to confer outcomes comparable with those of surgery [16, 17]. However, in this setting, p-Stage is not confirmed. From our results, to predict the prognosis of patients with unoperated NSCLC, both the c-Stage and the presence of either solid/ subsolid nodules should be considered.
This study had several limitations. It was a retrospective and a single-center study, the TSs were measured manually, and the SSs were calculated on the basis of the TSs and C/T ratios described in the preoperative radiological reports. Hence, solid nodules were differentiated visually from subsolid nodules by radiologists. This might have led to some measurement errors. If computer-aided diagnosis software could automatically discriminate solid from subsolid nodules and measure the maximal diameter of the solid components in tumors, then the measurement accuracy could be improved. In addition, the volume of the solid component of subsolid NSCLCs shows better correlation with postoperative recurrence [4, 18]. Moreover, the pathological invasive size was not measured and compared with SS in this study because our cohort included old cases, and the pathologists at the time did not measure this.
Conclusions
In conclusion, for early-stage NSCLCs, the c-Stage of the 8th version of the UICC based on the SS in a subsolid tumor was useful for predicting the postoperative DFS. On the other hand, whether solid or subsolid nodules were present was another independent prognostic factor. Therefore, to evaluate the prognosis of patients with unoperated NSCLC more accurately, both the c-Stage and the presence of either solid/ subsolid nodules should be considered.
Availability of data and materials
The dataset supporting the conclusions of this article is included within the article. The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- C/T ratio:
-
Ratio of consolidation to tumor
- c-Stage:
-
Clinical stage
- CT:
-
Computed tomography
- DFS:
-
Disease-free survival
- GGO:
-
Ground-glass opacity
- NSCLC:
-
Non-small cell lung cancer
- p-Stage:
-
Pathological stage
- SS:
-
Solid Size
- TS:
-
Total Size
- UICC:
-
Union for International Cancer Control
References
Rena O, Oliaro A, Cavallo A, et al. Stage I non-small cell lung carcinoma: really an early stage? Eur J Cardiothorac Surg. 2002;21(3):514–9.
Roviaro G, Varoli F, Vergani C, Nucca O, Maciocco M, Grignani F. Long-term survival after videothoracoscopic lobectomy for stage I lung cancer. Chest. 2004;126(3):725–32.
Rami-Porta R, Bolejack V, Crowley J, et al. The IASLC lung cancer staging project: proposals for the revisions of the T descriptors in the forthcoming eighth edition of the TNM classification for lung cancer. J Thorac Oncol. 2015;10(7):990–1003.
Kamiya S, Iwano S, Umakoshi H, et al. Computer-aided volumetry of part-solid lung cancers by using CT: solid component size predicts prognosis. Radiology. 2018;287(3):1030–40.
Yanagawa M, Kusumoto M, Johkoh T, et al. Radiologic-pathologic correlation of solid portions on thin-section CT images in lung adenocarcinoma: a multicenter study. Clin Lung Cancer. 2018;19(3):e303–12.
Aokage K, Miyoshi T, Ishii G, et al. Clinical and pathological staging validation in the eighth edition of the TNM classification for lung cancer: correlation between solid size on thin-section computed tomography and invasive size in pathological findings in the new T classification. J Thorac Oncol. 2017;12(9):1403–12.
Nakamura S, Fukui T, Taniguchi T, et al. Prognostic impact of tumor size eliminating the ground glass opacity component: modified clinical T descriptors of the tumor, node, metastasis classification of lung cancer. J Thorac Oncol. 2013;8(12):1551–7.
Travis WD, Asamura H, Bankier AA, et al. The IASLC lung cancer staging project: proposals for coding T categories for subsolid nodules and assessment of tumor size in part-solid tumors in the forthcoming eighth edition of the TNM classification of lung cancer. J Thorac Oncol. 2016;11(8):1204–23.
Hattori A, Matsunaga T, Takamochi K, Oh S, Suzuki K. Importance of ground glass opacity component in clinical stage IA radiologic invasive lung cancer. Ann Thorac Surg. 2017;104(1):313–20.
Hattori A, Matsunaga T, Takamochi K, Oh S, Suzuki K. Neither maximum tumor size nor solid component size is prognostic in part-solid lung cancer: impact of tumor size should be applied exclusively to solid lung cancer. Ann Thorac Surg. 2016;102(2):407–15.
Nakamura H, Sakai H, Kimura H, Miyazawa T, Marushima H, Saji H. Difference in postsurgical prognostic factors between lung adenocarcinoma and squamous cell carcinoma. Ann Thorac Cardiovasc Surg. 2017;23(6):291–7.
Ito R, Iwano S, Kishimoto M, Ito S, Kato K, Naganawa S. Correlation between FDG-PET/CT findings and solid type non-small cell cancer prognostic factors: are there differences between adenocarcinoma and squamous cell carcinoma? Ann Nucl Med. 2015;29(10):897–905.
Takei H, Asamura H, Maeshima A, et al. Large cell neuroendocrine carcinoma of the lung: a clinicopathologic study of eighty-seven cases. J Thorac Cardiovasc Surg. 2002;124(2):285–92.
Okumura M, Goto M, Ideguchi K, et al. Factors associated with outcome of segmentectomy for non-small cell lung cancer: long-term follow-up study at a single institution in Japan. Lung Cancer. 2007;58(2):231–7.
Umakoshi H, Iwano S, Yokoi K, et al. FDG PET/CT overcomes discordance between clinical and pathologic TNM classification of small-size primary lung cancer: influence on postoperative prognosis. Clin Lung Cancer. 2018;19(1):e37–45.
Nagata Y, Hiraoka M, Shibata T, et al. Prospective trial of stereotactic body radiation therapy for both operable and inoperable T1N0M0 non-small cell lung cancer: Japan Clinical Oncology Group Study JCOG0403. Int J Radiat Oncol Biol Phys. 2015;93(5):989–96.
De Ruysscher D, Nakagawa K, Asamura H. Surgical and nonsurgical approaches to small-size nonsmall cell lung cancer. Eur Respir J. 2014;44(2):483–94.
Furumoto H, Shimada Y, Imai K, et al. Prognostic impact of the integration of volumetric quantification of the solid part of the tumor on 3DCT and FDG-PET imaging in clinical stage IA adenocarcinoma of the lung. Lung Cancer. 2018;121:91–6.
Acknowledgements
We thank an experienced medical editor at Editage by Cactus Communications for an English language check and revision.
Funding
This work was supported by KAKENHI (15 K09919) from the Japanese Ministry of Education, Culture, Sports, Science and Technology (MEXT).
Author information
Authors and Affiliations
Contributions
Each author contributed to the preparation of the manuscript as follows: SI conceived and planned the study, analyzed the data, and drafted the manuscript. HU and SK contributed to the data collection and helped to draft the manuscript. KY, KK, and TF collected the patients’ data and revised the draft. SN supervised the study and performed a critical revision of the manuscript. All of the authors have read the manuscript and have approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This retrospective study was approved by our Institutional Review Board, and written informed consent was waived (approval no. 2017–0437).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Iwano, S., Umakoshi, H., Kamiya, S. et al. Postoperative recurrence of clinical early-stage non-small cell lung cancers: a comparison between solid and subsolid nodules. Cancer Imaging 19, 33 (2019). https://doi.org/10.1186/s40644-019-0219-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40644-019-0219-3