
Abstract
Background
Positron emission tomography (PET) is poised to become a useful imaging modality in staging and evaluating therapeutic responses in patients with metastatic pancreatic cancer (mPC). This analysis from a phase 1/2 study examined the utility of early PET imaging in patients with mPC treated with nab-paclitaxel plus gemcitabine.
Methods
Tumors were measured by [18F]2-fluoro-2-deoxyglucose PET/computed tomography (CT) in patients who received nab-paclitaxel 100 (n = 13), 125 (n = 38), or 150 (n = 1) mg/m2 plus gemcitabine 1000 mg/m2 on days 1, 8, and 15 of a 28-day cycle. Lesion metabolic activity was evaluated at baseline and 6 and 12 weeks postbaseline.
Results
Fifty-two patients had baseline and ≥1 follow-up PET scan. The median maximum standardized uptake values per pancreatic lesion in the nab-paclitaxel 100 mg/m2 and 125 mg/m2 cohorts were 5.1 and 6.5, respectively. Among patients who had a metabolic response by PET, those who received nab-paclitaxel 125 mg/m2 had a 4-month survival advantage over those who received 100 mg/m2. All patients in the nab-paclitaxel 125 mg/m2 cohort experienced an early complete metabolic response (CMR; 34%) or partial metabolic response (PMR; 66%). In the nab-paclitaxel 125 mg/m2 cohort, investigator-assessed objective response rates were 77% and 44% among patients with a CMR and PMR, respectively, with no correlation between PET and CT response (Spearman r s = 0.22; P = 0.193). Patients in the nab-paclitaxel 125 mg/m2 cohort with a CMR experienced a significantly longer overall survival vs those with a PMR (median, 23.0 vs 11.2 months; P = 0.011), and a significant correlation was found between best percentage change in tumor burden by PET and survival: for each 1% decrease in PET score, the risk of death decreased by 2%.
Conclusions
The majority of primary pancreatic tumors and their metastases were PET avid, and PET effectively measured changes in tumor metabolic activity at 6 and 12 weeks. These results support the antitumor activity of nab-paclitaxel 125 mg/m2 plus gemcitabine 1000 mg/m2 for treating mPC and the utility of PET for measuring treatment response. Treatment response by PET analysis may be considered when evaluating investigational agents in mPC.
Trial registration
NCT00398086.
Similar content being viewed by others

Background
The use of positron emission tomography (PET) with [18F]2-fluoro-2-deoxyglucose as a tracer combined with computed tomography (18F-FDG/CT) to evaluate tumors has increased in recent years because of its high sensitivity and specificity. Currently, 18F-FDG/CT is used for diagnosing, initial staging, detecting recurrent disease, and evaluating response in various malignant tumors, including breast cancer, non-small cell lung cancer, colorectal cancer, esophageal cancer, head and neck cancer, cervical cancer, diffuse large B-cell lymphoma, and melanoma [1,2,3,4,5,6,7,8,9,10]. Primary pancreatic adenocarcinoma has also been shown to be FDG avid by PET/CT [11], and an association between metabolic response and survival has been demonstrated in patients with metastatic pancreatic cancer (mPC) [12], providing support for the feasibility of PET/CT for pancreatic tumors. Continued research may validate PET as a useful tool for measuring treatment response in this disease state.
The treatment of mPC is among the most challenging in clinical oncology, with a 5-year survival rate of only ≈ 3% [13, 14]. Since 1997, gemcitabine monotherapy has been a standard of care for treating mPC until recently, when the PRODIGE and MPACT trials demonstrated significant survival benefits with FOLFIRINOX (folinic acid, 5-fluorouracil, irinotecan, and oxaliplatin) and nab-paclitaxel plus gemcitabine, respectively, compared with gemcitabine monotherapy [15,16,17]. Based on the positive findings of the phase 3 MPACT trial, nab-paclitaxel plus gemcitabine was approved for the first-line treatment of mPC [17, 18]. Although these findings are encouraging, effective PC treatment remains a major challenge, and there is a need to identify those patients who are most likely to benefit from specific therapies.
At week 8 in the MPACT trial, ≈ 5 times more patients experienced a metabolic response by PET per criteria from the European Organisation for Research and Treatment of Cancer (EORTC) [19] than an objective response by CT per Response Evaluation Criteria In Solid Tumors (RECIST) [20, 21], and patients with a tumor response identified by either modality had a median overall survival (OS) of >10 months [12]. The initial findings on the utility of PET/CT to assess response with nab-paclitaxel plus gemcitabine in a phase 1/2 study of patients with mPC were previously reported [22]. The preliminary data demonstrated that a complete loss of FDG metabolic activity was associated with an improved OS with nab-paclitaxel plus gemcitabine [22]. Furthermore, assessment of treatment response by PET was more sensitive than by CT; for all patients, the median decrease in metabolic activity at 12 weeks was 79% (n = 55; by 18F-FDG PET scan using EORTC criteria), whereas the overall response rate was 46% (n = 67; by CT scan using RECIST v1.0) [22]. Here we report the final analysis of the PET/CT data from the phase 1/2 trial and a more detailed analysis of the 18F-FDG PET/CT data in measuring efficacy outcomes in patients with mPC who received nab-paclitaxel 125 or 100 mg/m2 plus gemcitabine.
Methods
This open-label study, consisting of a phase 1 dose-finding portion and an expanded phase 2 portion at the maximum tolerated dose, was conducted at 4 centers in the United States in accordance with the Declaration of Helsinki and Good Clinical Practice Guidelines of the International Conference on Harmonization. Written informed consent was obtained from all patients before they entered the study. Details of the patients and methods in this study were reported previously [22]. Briefly, patients aged ≥18 years who had histologically or cytologically confirmed mPC with measurable disease by CT scan, as defined by the RECIST v1.0 guidelines, and no previous treatment for metastatic disease received nab-paclitaxel (100, 125, or 150 mg/m2) followed by gemcitabine (1000 mg/m2)—both administered intravenously on days 1, 8, and 15 every 28 days. Sixty-seven patients were enrolled in the trial: 20, 44, and 3 patients received 100, 125, and 150 mg/m2 nab-paclitaxel, respectively. The maximum tolerated dose was established as 125 mg/m2 of nab-paclitaxel plus 1000 mg/m2 of gemcitabine once a week for 3 weeks every 28 days, which was the dose and schedule used in the phase 3 MPACT trial [17, 22]. This regimen is also the US Food and Drug Administration–approved dose and schedule for the treatment of mPC according to the prescribing information [18].
18F-FDG PET/CT acquisition and scan lesion evaluation
18F-FDG PET/CT scans of target and nontarget lesions were taken at baseline and at 6 and/or 12 weeks postbaseline. Patients underwent at least a 4-h fast prior to each scan. Patients were injected with a mean 5.5 × 1011 mBq 18F-FDG (range, 3.3 × 1011–10.4 × 1011 mBq) based upon body mass 0.44 × 1010 to 1.5 × 1010 mBq/kg. All patients’ fasting glucose values were within an acceptable range (< 200 mg/dL). The average uptake period was 66 min (range, 50 to 110 min; 88% of all scans were conducted at an uptake period of 50 to 85 min). Each patient also underwent a low-dose CT scan for attenuation correction followed by a whole-body (orbitomeatal line to mid thighs) PET emission scan. The PET images were acquired in 2D and 3D modes per site standards (2–5 min per bed position) and then iteratively reconstructed with z-axis postprocessing filtering and corrected for attenuation using the low-dose CT scan series.
Baseline
Target lesions were chosen based on size and location. No more than 5 lesions in any 1 organ system and no more than 10 lesions in total were chosen for analysis of standardized uptake values (SUVs). The maximum SUV (SUVmax) of all target lesions within a patient was then summed and served as a measure of tumor burden at the baseline time point, referred to as SUVmax Total. Note that SUVmax has been commonly used, particularly at the time this study was conducted, to evaluate tumor burden and change in tumor burden by PET [3,4,5,6,7, 12, 23]. Nontarget lesions were noted, and the anatomical location of both target and nontarget lesions was recorded.
Follow-up
Scans of target and nontarget lesions were performed at weeks 6 and 12 postbaseline. The SUVmax of all target lesions was then summed, and the total served as a measure of tumor burden for that particular scan (SUVmax Total). The images were then evaluated for the presence of new lesions on the 18F-FDG PET/CT fused images as appropriate.
In addition to the confirmatory CT scans following the PET imaging at 6 and 12 weeks, contrast-enhanced diagnostic-quality spiral CT scans were performed separately at baseline and every 4 weeks to evaluate tumor response to therapy per RECIST. The diagnostic CT scans required the evaluation of the chest, abdomen, and pelvis using the kVp, mAs, and slice thickness ≤ 5 mm to perform lesion assessments according to RECIST guidelines. Comparisons of PET/CT and diagnostic-quality spiral CT scans as markers of efficacy at specific time points were not feasible because of the difference in timing of the scans.
Image analysis
De-identified images were interpreted by a single reader (RLK). Images were inspected for quality, body coverage, and dose infiltration at the injection site and for other factors that could have altered quantitative analysis. The images were interpreted to determine treatment response using the PET/CT and image-fusion 18F-FDG PET/CT data sets. The locations of the metastatic lesions were noted, and SUVs were determined when appropriate. The SUV activity in normal tissue of the liver and mediastinum was recorded. 18F-FDG activity was considered to indicate malignancy when the 18F-FDG activity was focal, was greater than the background 18F-FDG metabolism, and had a corresponding abnormality on CT. Target lesions were selected on baseline PET/CT scans without guidance from follow-up scans. Up to 5 lesions were selected for target lesion SUVmax analysis from visual inspection of the lesions with the greatest FDG uptake. Both primary pancreatic and metastatic lesions were included. All other hypermetabolic tumor lesions were considered nontarget lesions. Subsequently, SUVmax measurements of the target lesions were assessed on follow-up PET/CT scans. In the case of resolved hypermetabolic activity, the target lesions were given an SUVmax value of 0. Nontarget lesions were followed qualitatively for 1) complete resolution of FDG activity, 2) significant increase of FDG uptake compared to baseline scans, or 3) neither resolution nor significant increase (ie, metabolically stable) of FDG activity. Finally, any FDG focus that was consistent with malignant uptake that was not present previously was declared a new lesion if, in the opinion of the reader, it was consistent with malignant uptake. In order to assign time-point response, the sum of the SUVmax for target lesions was used to assess interval change from baseline along with a determination of new lesion development and change in nontarget lesion FDG behavior for final response assignment (Table 1).
SUVs
Standardized uptake values were determined using an SUV function integrated into a GE Advantage Window Workstation. In order to obtain the SUV measurement, a 1.5-cm region of interest (ROI) was deposited on the image slice that had the most intense 18F-FDG activity determined by visual inspection. By definition, an SUV is a reflection of the amount of 18F-FDG activity in an ROI per the following formula:
Calculation of % tumor response on 18F-FDG PET/CT
The percentage of change in SUV activity was calculated using the following formula:
The metabolic response category on the follow-up scans was then determined based on the EORTC criteria for PET response (Table 1) [19].
Statistical analysis
The characteristics of the target lesions were analyzed using standard descriptive statistics. Statistical analyses were carried out using SPSS 19 software. The best 18F-FDG PET/CT response rate for each patient, measured as the percentage of change in SUVmax Total at follow-up compared with baseline, was calculated and classified per EORTC criteria (Table 1); note that the more stringent threshold of a ≥ 25% decrease was always used to define partial response because even the first postbaseline scan was at week 6, which was considered to be >1 cycle of treatment (see Table).
The relationship between the best PET response and OS was tested, using a log-rank test, in the group with a complete metabolic response (CMR, defined in Table 1) vs the non-CMR group (all had a partial metabolic response [PMR]) in the nab-paclitaxel 125 mg/m2 dose cohort. A Cox proportional hazards model was used to determine whether the best percentage of change in PET was associated with OS. A nonparametric rank-correlation test was used to determine whether a correlation existed between the best percentage of PET and radiographic (using CT) changes; the data were summarized by Spearman rank-correlation coefficient. The relationship of CT and PET response was also evaluated by comparing rates of objective response in patients who had a CMR vs a PMR (CT and PET responses evaluated as categorical variables). A P value ≤ 0.05 was considered statistically significant.
Results
Of the 67 enrolled patients, 61 had a baseline 18F-FDG PET/CT scan, and 52 patients had both a baseline 18F-FDG PET/CT scan and at least 1 follow-up 18F-FDG PET/CT scan at 6 weeks, 12 weeks, or both. Of the 20 treated patients in the nab-paclitaxel 100 mg/m2 cohort, 13 had a baseline and at least 1 follow-up 18F-FDG PET/CT scan at 6 weeks, 12 weeks, or both. Of the 44 treated patients in the nab-paclitaxel 125 mg/m2 cohort, 38 had a baseline and at least 1 follow-up 18F-FDG PET/CT scan at 6 weeks, 12 weeks, or both. Lack of follow-up scans was primarily due to disease progression, patient choice, or logistical/monetary reasons. Of 13 patients in the nab-paclitaxel 100 mg/m2 cohort who had at least 1 follow-up 18F-FDG PET/CT scan, 12 had an 18F-FDG PET/CT scan at 6 weeks, and 12 had an 18F-FDG PET/CT scan at 12 weeks. Of 38 patients in the nab-paclitaxel 125 mg/m2 cohort who had at least 1 follow-up 18F-FDG PET/CT scan, 37 had an 18F-FDG PET/CT scan at 6 weeks, and 34 had an 18F-FDG PET/CT scan at 12 weeks. The median age of all patients was 61 years and of those in the nab-paclitaxel 100 and 125 mg/m2 cohorts was 57 and 61 years, respectively (Table 2).
Distribution of lesions on 18F-FDG PET/CT
The distribution and baseline SUVmax of lesions from patients enrolled in this study are summarized in Table 3. Among all patients, primary pancreatic (n = 43) lesions were the most common target lesions examined. The mean SUVmax of pancreatic lesions was 6.9 (median, 6.4; range, 1.5–17.5). The most common sites of metastases were liver (n = 37), with an average SUVmax of 7.6 (median, 6.6; range, 2.2–15.7); peritoneum (n = 28), with an average SUVmax of 5.9 (median, 5.3; range, 0.6–20.7); and mediastinal lymph nodes (n = 18), with an average SUVmax of 4.5 (median, 4.0; range, 1.5–11.3). These findings were generally consistent between the 2 dose cohorts, with liver and peritoneum being the most common sites of metastases. Metastatic lesions were identified by PET/CT in most anatomical sites, with the exception of the brain and kidney. This distribution of involved sites is consistent with the known spread of PC metastasis by both lymphatic and hematogeneous routes.
Individual lesion analysis
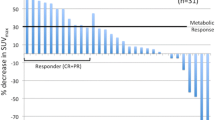
A total of 42 and 154 lesions were evaluated on the 18F-FDG PET/CT scans for patients in the nab-paclitaxel 100 and 125 mg/m2 cohorts, respectively. The median numbers of target lesions per patient to be scanned by 18F-FDG PET/CT at baseline were 3.0 and 4.0 in patients in the nab-paclitaxel 100 and 125 mg/m2 cohorts, respectively. The best PET responses from baseline in patients in the nab-paclitaxel 100 and 125 mg/m2 cohorts are shown in Fig. 1. Among patients in the nab-paclitaxel 100 mg/m2 cohort, the median SUVmax per lesion was 5.1 (quartiles 1–3 range, 3.4–11.2). Among patients in the nab-paclitaxel 125 mg/m2 cohort, the median SUVmax per lesion was 6.5 (quartiles 1–3 range, 3.9–9.5).

Waterfall plot of best responses by 18F-FDG PET/CT. CMR, complete metabolic response; CT, computed tomography; nab-P, nab-paclitaxel; PET, positron emission tomography; PMR, partial metabolic response; SMD, stable metabolic disease. a The blue circle represents 0% best response from a single patient in the nab-P 100 mg/m2 cohort
18F-FDG PET/CT metabolic response
A summary of the 18F-FDG response by dose cohort is presented in Table 4. Of the 52 evaluable patients, 17 (33%) had an EORTC-defined CMR, 32 (62%) had a PMR, and 3 (6%) had stable metabolic disease. No patients had progressive disease based on PET during this testing interval up to 12 weeks. Patients in the nab-paclitaxel 100 mg/m2 cohort (n = 13) experienced an EORTC-defined CMR (3 [23%]), a PMR (7 [54%]), or stable metabolic disease (3 [23%]). Patients in the nab-paclitaxel 125 mg/m2 cohort (n = 38) had either an EORTC-defined CMR (13 [34%]) or a PMR (25 [66%]).
Among patients in the nab-paclitaxel 100 mg/m2 cohort with a follow-up 18F-FDG PET/CT scan at 6 and 12 weeks (n = 11), 6 (55%) had a decrease, 4 (36%) had an increase, and 1 (9%) had no change (either no change or change <1%) in SUVmax from week 6 to week 12. Among patients in the nab-paclitaxel 125 mg/m2 cohort with a follow-up 18F-FDG PET/CT scan at 6 and 12 weeks (n = 33), 19 (58%) had a decrease, 7 (21%) had an increase, and 7 (21%) had no change (either no change or change <1%) in SUVmax from week 6 to week 12.
18F-FDG PET/CT response and median overall survival
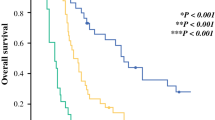
Among patients who achieved a CMR or PMR by PET, a survival difference of ≈ 4 months was observed in favor of the nab-paclitaxel 125 mg/m2 cohort vs the 100 mg/m2 cohort (median, 15.6 vs 11.4 months, respectively; Table 5). In the nab-paclitaxel 125 mg/m2 cohort, the OS in patients with a CMR was significantly longer than that of patients with a PMR (median, 23.0 vs 11.2 months; P = 0.011; Fig. 2). Within this cohort, a significant correlation was observed between best percentage of change in tumor burden by PET, evaluated as a continuous variable, and OS; namely, for each 1% decrease in PET SUV, the risk of death decreased by 2% (hazard ratio 0.98; 95% CI, 0.965–0.995; P = 0.010).

Overall survival by PET metabolic response among patients in the nab-paclitaxel 125 mg/m2 cohort. CMR, complete metabolic response; OS, overall survival; PET, positron emission tomography; PMR, partial metabolic response
Radiographic response by CT scan and relationship with PET
Among patients in the nab-paclitaxel 125 mg/m2 cohort, the investigator-assessed objective CT response rates by diagnostic (spiral) CT per RECIST v1.0 were 77% in patients with a CMR vs 44% in patients with a PMR (both evaluated as categorical variables; P = 0.053); 21 of 38 patients had a partial response, and 8 of 38 patients had stable disease for ≥16 weeks by CT scan. The every-4-week response rates (per CT) over 28 weeks are reported in Table 6. The median time to best response by CT, as determined by the investigator, was 2.7 months collectively in patients in both the nab-paclitaxel 125 and 100 mg/m2 cohorts (Fig. 3). No significant correlation was observed between best percentage of change in tumor burden by 18F-FDG PET/CT and radiographic measurement by CT scan (Spearman analysis; r s = 0.22; P = 0.193).

Time to best response by CT in the 125 and 100 mg/m2 nab-paclitaxel cohorts. CT, computed tomography
Discussion
The current study from a phase 1/2 trial provides evidence that pancreatic tumors and their associated metastases are hypermetabolic. 18F-FDG PET/CT is a useful tool for monitoring treatment response, changes in tumor metabolic activity, and predicting survival in this disease setting.
The results described here support the previously reported survival benefit and antitumor activity of the nab-paclitaxel 125 mg/m2 plus gemcitabine 1000 mg/m2 regimen for treating mPC [17, 22]. The CMR and PMR rates were numerically higher in patients in the nab-paclitaxel 125 mg/m2 cohort than in those in the nab-paclitaxel 100 mg/m2 cohort (34% vs 23% and 66% vs 54%, respectively). Furthermore, a survival difference favoring the 125 vs the 100 mg/m2 nab-paclitaxel group was observed in both the PET-evaluable population (> 4-month survival benefit for 125 vs 100 mg/m2 [median, 15.6 vs 10.9 months, respectively]) and the all-evaluable population (≈ 3-month survival benefit [median, 12.2 vs 9.3 months, respectively) [22]. The longer survival in patients treated with nab-paclitaxel 125 mg/m2, despite a similar or even higher baseline SUVmax, suggests a greater clinical benefit with the 125 mg/m2 dose than with the 100 mg/m2 dose. Additionally, the high metabolic response rates observed in the PET-evaluable cohorts (100% and 77% in the 125 and 100 mg/m2 nab-paclitaxel dose cohorts, respectively) may reflect the previously published relatively high radiological response rates observed in this study (48% and 45% in the 125 and 100 mg/m2 nab-paclitaxel dose cohorts, respectively [22]).
In this study, 18F-FDG PET/CT responses at 6 or 12 weeks predicted survival among patients in the nab-paclitaxel 125 mg/m2 cohort. The OS in patients in this cohort who had a CMR was significantly longer than that of patients who had a PMR (median, 23.0 vs 11.2 months, respectively; P = 0.011)—an observation that is consistent with our previous report for all patients with a CMR vs those without a CMR (median, 20.1 vs 10.3 months, respectively; P = 0.01) [22]. In addition, a significant correlation was found between the best percentage of change in PET score—evaluated as a continuous variable—and survival. These findings agree with the findings of a phase 1 study of patients with advanced PC that reported a significant correlation between improved OS and a decreased metabolic activity via PET in hepatic metastases [24]. That study, by Beatty and colleagues, underscores the utility of PET in analyses involving immunotherapies, in which radiological methods by CT could be complicated by inflammation. The validation of correlating a change in metabolic activity with survival strongly supports the clinical utility of PET analysis.
The analysis of change in SUVmax from week 6 to week 12 is informative of the dynamics of tumor metabolic response to therapy. This analysis suggests that when patients experience a metabolic response following treatment with nab-paclitaxel 125 mg/m2 plus gemcitabine 1000 mg/m2, that response is unlikely to be reversed over a 6-week period. Determining the clinical activity of a particular treatment regimen at an early time point could inform the physician about whether to continue the current therapy or to switch to a different therapeutic option. Early assessment of clinical activity is particularly important given the recent interest in developing treatment plans for patients with mPC. In a study of neoadjuvant human epidermal growth factor receptor 2–positive breast cancer, metabolic responses determined by 18FDG PET/CT were evident at 2 weeks posttreatment, and a significant correlation (R 2 = 0.81) was observed between the change in SUVmax at weeks 2 and 6 [5]. At weeks 2 and 6, the metabolic response rates (CMR plus PMR) of the primary tumor were 72% and 60%, respectively. Reductions in tumor metabolic activity reflected treatment outcome—the reduction in SUVmax at both 2 and 6 weeks was significantly greater in those with a pathological complete response (pCR) vs those without a pCR (P = 0.02 at both time points). Similarly, in a study of patients with previously treated non-small cell lung cancer, patients with a PMR 14 days after erlotinib treatment (26% of PET-evaluable patients) had a longer OS compared with patients without a metabolic response (P = .03) [23].
Previously, a controversy existed among oncologists regarding the usefulness of 18F-FDG PET/CT for measuring tumor response in the mPC setting because of the perceived lack of sufficient FDG uptake in pancreatic lesions and the increased expense associated with the procedure. The current analysis confirms that primary pancreatic tumors and their metastases are PET avid and that 18F-FDG-PET/CT is useful for monitoring their metabolic activity in this setting. Although the combined/hybrid device is more expensive than CT alone, it has the advantage of providing both functions as stand-alone examinations. This allows for improved staging and monitoring of disease progression and, thus, for potentially improved treatment plans. Furthermore, our data suggest that 18F-FDG PET/CT is a valuable adjunct for assessing treatment response and can predict clinical outcomes in patients treated with nab-paclitaxel plus gemcitabine, particularly in patients who received the indicated dose and schedule.
Although the use of 18F-FDG PET/CT in the mPC setting is promising, our study had some limitations. First, the number of patients evaluated by 18F-FDG PET/CT was relatively small, and not all trial participants underwent PET/CT imaging because of either patient or physician discretion. Another limitation of the analysis was that 15 patients (6 in the nab-paclitaxel 125 mg/m2 cohort) had PET scans only at baseline. Although this limitation could have had some effect on the overall correlation of PET responses with survival, it is unlikely that all of the patients would have had a CMR if a follow-up PET scan had been performed. Such a result would not negate the important observation of the long survival durations in patients who experienced a CMR.
The PET results of the phase 1/2 study presented here agree with those of the phase 3 MPACT trial in that PET appeared to be a more sensitive modality than spiral CT for measuring treatment response [12]. Both data sets support the notion that a metabolic response by PET is associated with longer survival. It is important to point out that these were distinct studies that differed in design and conduct, as reflected by the different median baseline SUVmax values (6.5 in this study and 4.6 in the phase 3 trial; both among patients in the nab-paclitaxel 125 mg/m2 plus gemcitabine cohorts); thus, a direct comparison cannot be made.
Conclusions
The results of this study support the idea that metastatic and primary pancreatic lesions are FDG avid and that 18F-FDG PET/CT in mPC is a useful tool for monitoring treatment response in patients treated with nab-paclitaxel plus gemcitabine, particularly at the indicated dose and schedule. The metabolic response rates observed in this study using PET/CT support the activity of the nab-paclitaxel 125 mg/m2 plus gemcitabine 1000 mg/m2 combination regimen for treating mPC. The significant correlation between the decrease in metabolic activity, as evident by FDG uptake, and decreased risk of death highlights the clinical utility of PET and suggests that this modality may be useful in predicting the success of experimental regimens. The median OS of 23.0 months in the CMR group deserves further evaluation in subsequent studies.
Abbreviations
- 18F-FDG:
-
[18F]2-fluoro-2-deoxyglucose
- CA 19–9:
-
Carbohydrate antigen 19–9
- CMR:
-
Complete metabolic response
- CT:
-
Computed tomography
- ECOG PS:
-
Eastern Cooperative Oncology Group performance status
- EORTC:
-
European Organisation for Research and Treatment of Cancer
- FOLFIRINOX:
-
Folinic acid, 5-fluorouracil, irinotecan, and oxaliplatin
- mPC:
-
Metastatic pancreatic cancer
- nab-P:
-
nab-paclitaxel
- OS:
-
Overall survival
- pCR:
-
Pathological complete response
- PET:
-
Positron emission tomography
- PMD:
-
Progressive metabolic disease
- PMR:
-
Partial metabolic response
- RECIST:
-
Response Evaluation Criteria In Solid Tumors
- ROI:
-
Region of interest
- SMD:
-
Stable metabolic disease
- SUV:
-
Standardized uptake values
- SUVmax :
-
Maximum standardized uptake values
- SUVmax Total:
-
Standardized uptake values of all target lesions
References
Koers K, Francken AB, Haanen JB, Woerdeman LA, van der Hage JA. Vemurafenib as neoadjuvant treatment for unresectable regional metastatic melanoma. J Clin Oncol. 2013;31:e251–3.
Li J, Xiao Y. Application of FDG-PET/CT in radiation oncology. Front Oncol. 2013;3:80.
McArthur GA, Puzanov I, Amaravadi R, Ribas A, Chapman P, Kim KB, et al. Marked, homogeneous, and early [18F]fluorodeoxyglucose-positron emission tomography responses to vemurafenib in BRAF-mutant advanced melanoma. J Clin Oncol. 2012;30:1628–34.
Qiao W, Zhao J, Xing Y, Wang C, Wang T. Predictive value of [18F]fluoro-2-deoxy-d-glucose positron emission tomography for clinical outcome in patients with relapsed/refractory diffuse large B-cell lymphoma prior to and after autologous stem cell transplant. Leuk Lymphoma. 2014;55:276–82.
Gebhart G, Gamez C, Holmes E, Robles J, Garcia C, Cortes M, et al. 18F-FDG PET/CT for early prediction of response to neoadjuvant lapatinib, trastuzumab, and their combination in HER2-positive breast cancer: results from neo-ALTTO. J Nucl Med. 2013;54:1862–8.
van Gool MH, Aukema TS, Schaake EE, Rijna H, Codrington HE, Valdés Olmos RA, et al. 18F-fluorodeoxyglucose positron emission tomography versus computed tomography in predicting histopathological response to epidermal growth factor receptor-tyrosine kinase inhibitor treatment in resectable non-small cell lung cancer. Ann Surg Oncol. 2014;21:2831–7.
Engelmann BE, Loft A, Kjaer A, Nielsen HJ, Gerds TA, Benzon EV, et al. Positron emission tomography/computed tomography and biomarkers for early treatment response evaluation in metastatic colon cancer. Oncologist. 2014;19:164–72.
Teyton P, Metges JP, Atmani A, Jestin-Le Tallec V, Volant A, Visvikis D, et al. Use of positron emission tomography in surgery follow-up of esophageal cancer. J Gastrointest Surg. 2009;13:451–8.
Prestwich RJ, Subesinghe M, Gilbert A, Chowdhury FU, Sen M, Scarsbrook AF. Delayed response assessment with FDG-PET-CT following (chemo) radiotherapy for locally advanced head and neck squamous cell carcinoma. Clin Radiol. 2012;67:966–75.
Yu L, Jia C, Wang X, Lu P, Tian M, Wang W, et al. Evaluation of 18F-FDG PET/CT in early-stage cervical carcinoma. Am J Med Sci. 2011;341:96–100.
Reske SN, Grillenberger KG, Glatting G, Port M, Hildebrandt M, Gansauge F, et al. Overexpression of glucose transporter 1 and increased FDG uptake in pancreatic carcinoma. J Nucl Med. 1997;38:1344–8.
Ramanathan RK, Goldstein D, Korn RL, Arena F, Moore M, Siena S, et al. Positron emission tomography response evaluation from a randomized phase III trial of weekly nab-paclitaxel plus gemcitabine versus gemcitabine alone for patients with metastatic adenocarcinoma of the pancreas. Ann Oncol. 2016;27:648–53.
Cancer Facts and Figures 2017. American Cancer Society. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2016/cancer-facts-and-figures-2016.pdf. 2017. Accessed 10 Feb 2017.
SEER Stat Fact Sheets: Pancreas Cancer. Surveillance, Epidemiology, and End Results Program. http://seer.cancer.gov/statfacts/html/pancreas.html 2017. Accessed 10 Feb 2017.
Conroy T, Desseigne F, Ychou M, Bouche O, Guimbaud R, Becouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364:1817–25.
Goldstein D, El-Maraghi RH, Hammel P, Heinemann V, Kunzmann V, Sastre J, et al. nab-Paclitaxel plus gemcitabine for metastatic pancreatic cancer: long-term survival from a phase III trial. J Natl Cancer Inst. 2015. doi 10.1093/jnci/dju413.
Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013;369:1691–703.
Celgene Corporation. Abraxane for injectable suspension (paclitaxel protein-bound particles for injectable suspension) (albumin-bound): Summit, NJ: Celgene Corporation; 2015.
Young H, Baum R, Cremerius U, Herholz K, Hoekstra O, Lammertsma AA, et al. Measurement of clinical and subclinical tumour response using [18F]-fluorodeoxyglucose and positron emission tomography: review and 1999 EORTC recommendations. European Organization for Research and Treatment of Cancer (EORTC) PET Study Group. Eur J Cancer. 1999;35:1773–82.
Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92:205–16.
Therasse P, European Organisation for Research and Treatment of Cancer Data Center. Evaluation of response: new and standard criteria. Ann Oncol. 2002;13(Suppl 4):127–9.
Von Hoff DD, Ramanathan RK, Borad MJ, Laheru DA, Smith LS, Wood TE, et al. Gemcitabine plus nab-paclitaxel is an active regimen in patients with advanced pancreatic cancer: a phase I/II trial. J Clin Oncol. 2011;29:4548–54.
Mileshkin L, Hicks RJ, Hughes BG, Mitchell PL, Charu V, Gitlitz BJ, et al. Changes in 18F-fluorodeoxyglucose and 18F-fluorodeoxythymidine positron emission tomography imaging in patients with non-small cell lung cancer treated with erlotinib. Clin Cancer Res. 2011;17:3304–15.
Beatty GL, Torigian DA, Chiorean EG, Saboury B, Brothers A, Alavi A, et al. A phase I study of an agonist CD40 monoclonal antibody (CP-870,893) in combination with gemcitabine in patients with advanced pancreatic ductal adenocarcinoma. Clin Cancer Res. 2013;19:6286–95.
Acknowledgements
Medical writing assistance was provided by Aaron Runkle, PhD, MediTech Media, Ltd. Biostatistical support was provided by Helen Liu and Xiaobin Yuan, Celgene Corporation. The authors are fully responsible for all content and editorial decisions related to this manuscript.
Funding
A research grant from the Stand Up To Cancer (SU2C) Dream Team to Dr. Daniel D. Von Hoff provided support for the translational studies. This study was supported by Celgene Corporation, Summit, NJ.
Availability of data and materials
The data sets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice, Guidelines of the International Conference on Harmonization. Written informed consent was obtained from all patients before entering the study.
Consent for publication
Not applicable.
Competing interests
RLK: research funding: Celgene; DDVH: consultant or advisory role, honoraria, and research funding: Celgene; MJB: nothing to disclose; RCB: consultant: Celgene; DM: employment: Celgene; MFR: employment: Celgene; RKR: consultant or advisory role, honoraria, and research funding: Celgene.
The manuscript has not been submitted for publication nor is it under consideration for publication elsewhere.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Korn, R.L., Von Hoff, D.D., Borad, M.J. et al. 18F-FDG PET/CT response in a phase 1/2 trial of nab-paclitaxel plus gemcitabine for advanced pancreatic cancer. Cancer Imaging 17, 23 (2017). https://doi.org/10.1186/s40644-017-0125-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40644-017-0125-5