
Abstract
Background
Ulaanbaatar, Mongolia, is one of the world’s worst air-polluted cities, but effects of this air pollution on the population health status have not yet been evaluated. Therefore, we developed a Mongolian version of the SF-36v2 questionnaire to investigate the health status of Mongolian population.
Methods
Health checkups were conducted in Ulaanbaatar and the health status was measured using a Mongolian translated version of the SF-36v2 questionnaire. The reliability and validity of the Mongolian SF-36v2 questionnaire, and the relationship between health status and respiratory condition were examined.
Results
Factor analysis of the Mongolian SF-36v2 questionnaire showed that the “Role-physical” and “Role-emotional” were classified into a single subscale. The “Mental health” and “Vitality” were each divided into two subscales. Cronbach’s alpha and intraclass correlation coefficient (ICC) for reproducibility were >0.7, except for “General health perceptions” (Cronbach’s alpha and ICC < 0.7), “Social functioning” (Cronbach’s alpha < 0.7), and “Vitality” (ICC < 0.7). The SF-36v2 subscales and the corresponding items of the COOP/WONCA charts were correlated, and subjects with respiratory symptoms showed lower SF-36v2 scores compared to normal subjects, suggesting external validity. Subjects with respiratory symptoms showed significantly lower scores for the majority of the SF-36v2 subscales than those with normal lung function. In subjects with combined ventilatory impairment, “Physical functioning”, “Role-physical”, “Bodily pain”, and “Vitality” scores were significantly lower than those with normal lung function.
Conclusions
The Mongolian version of the SF-36v2 questionnaire provides substantial reliability and validity, and is useful for evaluating the health status of Mongolian adults with ventilatory impairment. Health status measured by SF-36v2 was significantly aggravated by combined ventilatory impairment when compared with normal lung function.
Similar content being viewed by others

Background
Ulaanbaatar, the capital of Mongolia, is one of the world’s worst air-polluted cities and there have been growing concerns about air pollution from anthropogenic sources (WHO 2014). A remarkable increase in coal and biomass fuel consumption during the winter months is the major cause of air pollution in Ulaanbaatar, in addition to its topographic characteristics as a basin (Amarsaikhan et al. 2014). Increased coal consumption during winter is primarily due to an increased household use of coal-fired stoves or boilers. This increase in household coal consumption is contributed by a population influx from rural areas to Ulaanbaatar, leading to the development of ger districts, which are characterized by ger clusters comprising traditional Mongolian nomadic tents with poor infrastructure. During winter, coal or biomass-fired stoves used in each ger is a major cause of frequent smog in Ulaanbaatar. Four coal-fired electric power stations in Ulaanbaatar are also a significant source of air pollution. However, the health effects of this air pollution on the Ulaanbaatar populace have not yet been fully evaluated. The lack of appropriate questionnaires and medical supplies such as spirometers are contributing factors to this dearth of research in Mongolia. Although Enkhjargal et al. reported that the air pollution was associated with respiratory diseases especially among children, there has been no report on the effect of air pollution on the respiratory health of adult or elderly subjects (Enkhjargal et al. 2010). Sonomjamts et al. and Viinanen et al. have independently reported on the prevalence of asthma and allergic rhinitis among Mongolian subjects (Sonomjamts et al. 2014; Viinanen et al. 2005). However, there has been no report on the association between respiratory diseases and the health status of Mongolian adults.
Short-Form 36 Health Survey (SF-36v2) is a suitable tool for assessing health-related quality of life and has been used in many physical health conditions and healthcare settings (Aaronson et al. 1998; Garratt et al. 1993). It measures health status as the extent to which physical health impacts on functional ability and perceived well-being in mental, social and physical aspects of life. The SF-36v2 utilizes a scoring system based on eight functional health and well-being categories: physical functioning (PF), role limitations due to physical health problems (RP), bodily pain (BP), general health perceptions (GH), Vitality (VT), social functioning (SF), role limitations due to emotional problems (RE) and mental health (MH). The SF-36v2 has been translated into many languages and is widely used as a multilingual questionnaire in consideration of participant cultural background, such as language and customs (Li et al. 2003; Hoopman et al. 2006; Guermazi et al. 2012; Mbada et al. 2015). However, there is currently no Mongolian version of the SF-36v2.
In this study, we translated the original English version of the SF-36v2, which is widely used globally for health status measurement, into a Mongolian version. We then conducted a study to evaluate the usefulness of this Mongolian SF-36v2 questionnaire for health status assessment of Mongolian adults living in Ulaanbaatar.
Methods
Translation of the English SF-36v2 and COOP/WONCA charts into Mongolian
Translation of the English SF-36v2 (Table 1) into Mongolian was carried out with permission of QualityMetric Inc. (New York, NY, USA), the copyright holder of the SF-36v2, in accordance with the written directives (McHorney et al. 1993). Briefly, the English SF-36v2 was translated into Mongolian and after back translation, the expressions and lexicon were assessed by native Mongolian and English speakers. The translation was revised several times to ensure both conceptual equivalence with the original English version and ease of understanding by the target language population. The Mongolian SF-36v2 was then pilot tested through cognitive debriefing interviews of regular Mongolian citizens, after which QualityMetric staff, in collaboration with the translation team, reviewed the contents thoroughly and obtained final approval of the Mongolian version after minor adjustments. The English version of the COOP/WONCA charts was translated into Mongolian with permission of van Weel, the author of the original version (van Weel 1993). The translation process was similar to that of the SF-36v2. Permission to use the Japanese version of SF-36v2 was also obtained from Quality Metric. For the Japanese version of the COOP/WONCA charts, permission was obtained from the Japan Primary Care Association.
Self-completed questionnaire and health survey
A self-completed questionnaire package was administered containing questions regarding age, sex, occupation, and respiratory symptoms, and the translated SF-36v2 and COOP/WONCA charts. At the time of questionnaire administration, height, body weight, blood pressure, and peripheral capillary oxygen saturation (SpO2) were measured, and a medical interview and auscultation by a physician were also conducted. A pulmonary function test was performed with the HI-105 spirometer (CHEST M.I., Inc., Tokyo, Japan) where the forced vital capacity (FVC) and forced expiratory volume in one second (FEV1) were measured and the FEV1/FVC ratio was calculated. Subjects were classified into four groups according to the guidelines of The Japanese Respiratory Society; normal, obstructive (FEV1/FVC ratio <70 %), restrictive (FVC < 80 % of predicted value), and combined ventilatory impairment (FEV1/FVC ratio <70 % and FVC < 80 % of predicted value) (Sasaki et al. 2001).
Subjects
Health surveys were carried out at eight community clinics located all over Ulaanbaatar from 2012 to 2013. Participants were recruited by announcements advertising the health survey for male and female subjects aged 40–79 years. Administration of the self-completed questionnaire, body measurements, and medical examination including the pulmonary function test were performed in male and female community volunteers aged 40–79 years (Table 2).
Seven hundred and thirty-seven self-reported questionnaires were collected, and 32 subjects were excluded from analysis due to an incomplete SF-36v2 or COOP/WONCA charts. A total of 705 (95.7 %) collected questionnaires were eligible for analysis.
Twenty-nine healthy volunteers were recruited for reproducibility assessment of the Mongolian SF-36v2. Those involved in this reproducibility assessment were tested using the Mongolian SF-36v2, and re-tested after 1 week using the same questionnaire.
Japanese subjects recruited in the Kumamoto prefecture were also investigated. Subjects who visited the healthcare center were recruited into our study. Administration of the self-completed questionnaire, body measurements, and medical examination were also performed in male and female participants aged 40–79 years, and 855 subjects were eligible for analysis. Demographic characteristics of Japanese participants are shown in Additional file 1: Table S1. Significant gender differences were found in the smoking status and occupation category for both countries.
Data handling and statistical analyses
All data were handled by questionnaire ID, and managed as electronic data for the analysis. SF-36v2 scores were converted to subscale scores according to the Manual of the Japanese version of the SF-36v2 (Fukuhara and Suzukamo 2004). Each subscales was based on questions in the original version of the SF-36v2 as follows; PF, Q3 (a–j); RP, Q4 (a–d); BP, Q7 and Q8; GH, Q1 and Q11 (a–d); VT, Q9 (a, e, g, i); SF, Q6 and Q10; RE, Q5 (a–c); MH, Q9 (b, c, d, f, h). Statistical analyses including Welch’s t test for parametric analyses of continuous variables of two groups, Steel–Dwass test following Kruskal–Wallis test for non-parametric analysis of continuous variables, χ2-test for analyses of categorical data, factor analysis using varimax rotation, and calculations for Spearman’s correlation coefficient and intraclass correlation were carried out on the statistical software packages JMP version 11 (SAS Institute Inc., Cary, NC, USA) or SPSS ver. 21.0 (IBM Corp., Armonk, NY, USA). P values less than 0.05 were considered to be statistically significant.
Ethical considerations
The present study was approved by the Clinical Ethical Review Board of Kurume University School of Medicine. Before investigation, participants were provided with explanations in person as to the purpose and method of the study, as well as information regarding the handling of the results. The study was carried out upon receipt of written consent.
Results
Construct validity, reliability and reproducibility
The English version of the SF-36v2 consists of eight subscales PF, RP, BP, GH, VT, SF, RE and MH. Factor analysis was carried out using the Mongolian version of the SF-36v2 to test the construct validity (Table 3). For the PF, BP, and GH subscales, the Mongolian SF-36v2 consisted of the same items as the English SF-36v2. The RP and RE subscales were consolidated into a single factor that is different from the English SF-36v2. The MH subscale was divided into two subscales, with one as the same factor as SF, and the other as the same factor as VT. Two of the questions comprising the VT subscale were classified as another independent factor. In the Japanese SF-36v2, the RP, GH, BP, and RE subscales consisted of the same items as the English version. Although the VT and MH factors were composed of two factors, the questions making up these subscales were not identical to the English SF-36v2. One of the factors of the VT/MH subscales included questions in the SF subscale. Two of the questions that constituted the PF subscale were classified as another independent factor (Additional file 2: Table S2). Internal consistency reliability was assessed by calculating Cronbach’s α (Table 4). Cronbach’s α calculated for eight subscales exceeded 0.7 (range 0.711–0.892) in six subscales except for VT (α = 0.544) and SF (α = 0.599). The reproducibility of the questionnaire was examined using the test–retest method, and the retest was carried out on the same subject after an interval of 1 week (Table 4). The eight subscales showed significantly high correlation (Spearman’s correlation coefficients 0.624–0.948) between the test and retest. Intraclass correlation coefficients (ICC) exceeded 0.7 (range 0800–0.943) in six subscales except for GH [0.600, 95 % confidence interval (CI) 0.303–0.792] and VT (0.692, 95 % CI 0.440–0.844).
External validity
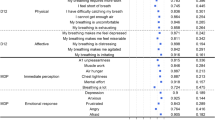
Individual scores of the eight subscales of the SF-36v2 and the corresponding items of the COOP/WONCA charts were highly correlated (Table 5): the PF subscales of the SF-36v2 showed the highest correlation coefficient with “Pain”, the RP, VT, SF, and RE subscales corresponded to “Daily activities”, and the BP, GH, SF, and MH subscales corresponded to the “Pain”, “Overall health”, “Social activities”, and “Feelings” scales of the COOP/WONCA charts, respectively.
The relationships between the SF-36v2 subscale score and the respiratory symptoms were analyzed (Table 6). Subjects who answered positive on question 1 (Q1), “Does the weather affect your cough?” showed significantly lower scores on six out of eight subscales except for RE and VT, compared to those who answered “No cough”. When compared with subjects without sputum production in the absence of a cold, subjects who answered positive on Q2, “Do you ever cough up sputum from your chest when you don’t have a cold?” showed significantly lower scores on all subscales. For Q3, “Do you usually cough up sputum from your chest first thing in the morning?”, subjects who answered in the affirmative showed significantly lower scores than subjects who answered in the negative in seven subscales except for MH. Subjects with frequent wheezing showed significantly lower scores in five subscales except for RP, RE, and VT compared to those who did not wheeze frequently. Subjects who answered positive on Q5, “Do you have or had any allergy?” showed significantly lower scores on seven subscales except for PF compared to subjects without any allergy.
Effects of ventilatory impairment and physiological parameters on SF-36v2 subscale scores
Pulmonary function tests in all subjects were performed by trained staff. The subjects were classified into four groups according to the results of the pulmonary function test: normal lung function, obstructive, restrictive, or combined ventilatory impairment. Figure 1 shows the effect of ventilatory impairment on the SF-36v2 subscale scores. When compared with the scores of subjects with normal lung function, the scores in the combined ventilatory impairment group were significantly lower for PF, RP, BP, and VT. Subjects with combined ventilatory impairment also showed significantly lower scores for PF, PR, and BP when compared with subjects with obstructive ventilatory impairment. There were no other significant differences in scores, although the scores tended to be lower in restrictive and combined ventilatory impairment.

Effects of lung function on SF-36v2 subscales scores in Mongolian subjects. SF36v2 subscales; PF physical functioning, RP role limitations due to physical health problems, BP bodily pain, GH general health perceptions, VT vitality, SF social functioning, RE role limitations due to emotional problems; and MH mental health. Data are presented as mean percentage of the mean score of subjects with normal lung function ± standard error of the mean. Nonparametric multiple comparisons were carried out by Steel–Dwass test on each pair following Kruskal–Wallis test. *P < 0.05; **P < 0.01; ***P < 0.005 between each group
Effects of physiological parameters such as body mass index (BMI), SpO2, FVC, FEV1, FEV1/FVC ratio, systolic and diastolic blood pressure on SF-36v2 subscale scores were assessed by gender (Table 7). Subjects were divided in two groups according to the median of each parameter. In males, PF score was lower in subjects with lower SpO2, FVC, and FEV1. Lower RP and MH scores correlated with lower FVC scores, and MH score was further lowered by lower BMI. Scores in RE, BP, GH, VT and SF subscales were not significantly affected by any physiological parameters. In females, PF scores were lower in those with higher BMI and blood pressure, and lower FVC and FEV1. Lower FVC and FEV1 also lowered BP scores, and MH scores were higher in those with lower SpO2. Lower RP and RP scores correlated with higher systolic blood pressure. GH, VT and SF subscales were not significantly affected by any physiological parameters.
Discussion
The present study was carried out to clarify the factors affecting the health status of Mongolian subjects, particularly those with ventilatory impairment, due to growing concerns about air pollution from anthropogenic sources. As a tool for evaluating the health status of Mongolian subjects, the Mongolian version of the SF-36v2 showed generally satisfactory construct validity although the Mongolian subjects aged 40–79 years in this study did not distinguish between the RP and RE subscales. Additionally, the MH subscales were divided into the SF and VT subscales. Internal consistency reliability was confirmed by Cronbach’s α, and the reliability examined by the test–retest method showed significantly high correlations with ICCs that were of substantially high value to confirm the reproducibility. In addition, the external validity of the Mongolian SF-36v2 was confirmed through correlation with COOP/WONCA charts and questions regarding respiratory symptoms. These results suggest that this questionnaire is useful for evaluating differences in health status between Mongolian subjects with normal lung function and those with ventilatory impairment.
The SF-36v2 has been translated into many languages and is widely used as a multilingual questionnaire for the measurement of health status differences between normal subjects and patients with various diseases such as multiple sclerosis (Fernandez et al. 2011), rheumatoid arthritis (Matcham et al. 2014), schizophrenia (Papaioannou et al. 2011), chronic obstructive pulmonary disease (Prieto et al. 1997), cardiovascular disease (Jenkinson et al. 1997; Dempster and Donnelly 2001), and cancer (Mosconi et al. 2002). However, no Mongolian SF-36v2 has been developed to date. Therefore, we developed the Mongolian version of the SF-36v2 questionnaire in collaboration with seven language professionals with permission from QualityMetric over the course of more than 2 years. We investigated 737 Mongolian subjects, which equaled approximately 0.1 % of the Mongolian population aged 40 years or more, from autumn of 2012 to winter of 2013. Mongolians aged 40 years or more account for 26.6 % of the total Mongolian population (United Nations 2014, 2015).
The construct validity of the Mongolian version of the SF-36v2 was assessed by factor analysis. The result showed that the subscales regarding mental components, which consist of the VT, SF, RE and MH subscales, were not clearly divided as with the English version, in contrast to the subscales regarding physical components, which consist of the PF, RP, BP and GH, although the RP and RE subscales were consolidated in the Mongolian subjects. Nevertheless, the subscales of the physical component were independent of each other. Both the RP and RE subscales of the SF-36v2 were highly correlated with the “Daily activity” subscale of the COOP/WONCA charts. This result suggests that Mongolians recognized that limitations in daily activities were mainly due to physical health problems rather than emotional or mental problems. In their study assessing the construct validity of the SF36v2 covering patients with mental illness and healthy volunteers, McHorney et al. demonstrated that RP correlated with medical severity and psychometrics, and RE correlated with psychiatric disorder and psychiatric severity (McHorney et al. 1993). However, Ware et al. performed a principal component analysis of the SF36v2 in a study of ten countries in Europe and the USA, and demonstrated that RP and RE were race-independent for the physical component score and the mental component score, respectively (Ware et al. 1998). We previously reported that factor analysis of the SF-36v2 collected from 783 citizens of the general populace in Japan and China aged 50–79 years showed that the RP and RE subscales were clearly divided (Yamaguchi et al. 2013). These results suggest that recognition of physical and psychological roles in daily activities is independent of age, sex and race. With respect to occupation, approximately 40 % of Mongolian male and 51 % of female subjects were not in employment or retired in this study. Relatively high unemployment rates were also shown in our previous study where 32.6 % of Japanese male, 45.8 % of Japanese female, 20.2 % of Chinese male, and 39.1 % of Chinese female subjects were not in employment or retired (Yamaguchi et al. 2013). Therefore, the effect of occupational status on the recognition of the role in daily activity was suggested to be small. Japanese and Chinese have quite different lifestyles and worldviews when compared with Mongolians, probably because Japanese and Chinese are essentially settled agricultural people compared to Mongolians who comprise nomadic, hunter-gatherer tribes. This difference may be a reason why Mongolians consider physical and mental aspects of daily activities as a unified concept. Further investigation is required to clarify the Mongolian-specific concept of the physical-mental interface.
SF-36v2 was validated as a tool for evaluating health-related quality of life in patients with symptomatic chronic obstructive pulmonary disease (COPD), characterized by persistent airway obstruction caused by a mixture of small airway disease and parenchymal destruction (Mahler and Mackowiak 1995). We therefore analyzed the effects of each physiological parameter on SF-36v2 subscales in participants with ventilatory impairment. SF-36v2 subscale scores were analyzed by sex because these parameters differ between sexes (Table 7). Physiological parameters such as FVC, FEV1 and SpO2 mainly affected physical aspects of the health status such as PF and RP subscales in male subjects, and BMI, FVC, FEV1 and blood pressure mainly affected PF, RP and BP subscales in female subjects with the exception of several mental aspects such as RE and MH. GH, VT and SF subscales were not significantly affected by any physiological parameters measured in the present study. The most susceptible subscale of SF-36v2 was PF in both sexes although the effect varied according to sex. It has been reported that there is sex-difference of SF-36v2 scores (Hajian-Tilaki et al. 2016; Kitaoka et al. 2016; Prata et al. 2016). Nevertheless, the subscales which differed by sex were entirely different between these reports and the present study because of differences in subjects’ age, clinical background and ethnic group. Therefore, further investigation of the effect of the respiratory symptoms on the health status measured by SF-36v2 is required.
Based on recent data, approximately two-thirds of the Mongolian population live in cities such as Ulaanbaatar, and the population density in urban areas has been increasing dramatically. Smog covering Ulaanbaatar occurs frequently in winter due to coal or biomass burning, leading to concerns about the health effects of air pollution, especially for children and elderly people who belong to the high-risk group. Recently, Jadambaa et al. listed the environmental risk factors for Mongolia in their systematic review of 59 reports including indoor or outdoor air pollution, metals, environmental tobacco smoke, and other toxic chemicals (Jadambaa et al. 2015). These risk factors are associated with cardiovascular and respiratory diseases in adults and neurodevelopmental disorder in children. However, the health effects of air pollution on respiratory health in Mongolian adults have not yet been fully investigated. Additionally, air quality monitoring and a longitudinal study would be necessary to clarify the association between health status and air pollution in Mongolia.
In addition to air pollution, cigarette smoking including second-hand smoke has been reported to be a cause of lung function decline (Xu et al. 1992; Anthoniesen et al. 2002; James et al. 2005). In the present study, there were no significant differences in health status measured by SF-36v2 between never-smokers and ever-smokers (ex- and current-smokers) in any of the ventilatory impairment groups (Additional file 3: Table S3). Therefore, in the present study, smoking was not suggested as a cause of health status decline but as a cause of lung function decline.
A major limitation in this study is the sampling of participants. The male-to-female ratio was approximately 1:2 because this study was carried out during working hours on weekdays. The sex imbalance may have been contributed by recruitment of passers-by and the sex-difference inherent in the Mongolian lifestyle and culture. Additionally, there were few established local communities in Ulaanbaatar due to the strong tradition of individualism in Mongolians, leading to a lukewarm response to the call for the survey. The female population of the Mongolian population aged 40–79 years was similar (52.7 %) to the male population during 2012–2013 (United Nations 2014), suggesting a potential for selection bias in this study sampling. However, the focus of this study was for validation of the Mongolian SF-36v2. In general, the national norm of the SF-36v2 scores are calculated based on scores obtained from the healthy population aged 20–70 years (Fukuhara and Suzukamo 2004). The survey carried out in this study was intended for people aged 40–79 years, and participants included patients with respiratory impairment who were susceptible to environmental factors such as air pollution. Here, we have demonstrated that the Mongolian SF-36v2 was valid and reliable for both healthy people and in those with respiratory impairment. Further studies in an unbiased population of healthy people representing the Mongolian population is needed to determine the national norm of SF-36v2 scores and the COOP/WONCA charts.
Conclusions
The results of our present study demonstrated the substantial reliability and validity of the Mongolian SF-36v2, and suggest that the Mongolian SF-36v2 was useful to evaluate the health status of Mongolian adults with normal or abnormal lung function. Health status measured by SF-36v2 was significantly aggravated by combined ventilatory impairment when compared with normal lung function.
Abbreviations
- SF-36v2:
-
Short-form 36 Health Survey version 2
- PF:
-
physical functioning
- RP:
-
role limitations due to physical problems
- BP:
-
bodily pain
- GH:
-
general health perceptions
- VT:
-
vitality
- SF:
-
social functioning
- RE:
-
role limitation due to emotional problems
- MH:
-
mental health
- SpO2 :
-
peripheral capillary oxygen saturation
- FVC:
-
forced vital capacity
- FEV1 :
-
forced expiratory volume in one second
- BMI:
-
body mass index
- ICC:
-
intraclass correlation coefficient
- CI:
-
confidence interval
References
Aaronson NK, Muller M, Cohen PDA, Essink-Bot ML, Fekkes M, Sanderman R et al (1998) Translation, validation, and norming of the Dutch language version of the SF-36 health survey in community and chronic disease populations. J Clin Epidemiol 51(11):1055–1068
Amarsaikhan D, Battsengel V, Nergui M, Ganzorig M, Bolor G (2014) A study on air pollution in Ulaanbaatar city, Mongolia. J Geosci Environ Prot 2:123–128
Anthoniesen NR, Connet JE, Murray RP, for the Lung Health Study Research Group (2002) Smoking and lung function of Lung Health Study participants after 11 years. Am J Respir Crit Care Med 166:675–679
Dempster M, Donnelly M (2001) A comparative analysis if the SF-12 and the SF-36 among ischemic heart disease patients. J Health Psychol 6(6):707–711
Enkhjargal A, Suvd B, Burmaa B, Enkhtsetseg S (2010) Health impact assessment of ambient air pm 2.5 and pm 10 in Ulaanbaatar city. J Mong Med Sci 4(154). http://mongolmed.mn/article/2113
Fernandez O, Baumstarck-Barrau K, Simeoni MC, Auguier P, MusiQoL Study Group (2011) Patient characteristics and determinants of quality of life in an international population with multiple sclerosis: assessment using the MusiQoL and SF-36 questionnaires. Mult Scler 17(10):1238–1249
Fukuhara S, Suzukamo Y (2004) Manual of SF-36v2 Japanese version. Kyoto Institute for Health Outcomes and Process Evaluation Research, Tokyo
Garratt AM, Ruta DA, Abdalla MI, Buckingham JK, Russell T (1993) The SF36 health survey questionnaire: an outcome measure suitable for routine use within the NHS? BMJ 306(6890):1440–1444
Guermazi M, Allouch C, Yahia M, Huissa TB, Ghorbel S, Damak J et al (2012) Translation in Arabic, adaptation and validation of the SF-36 Health Survey for use in Tunisia. Ann Phys Rehabil Med 55(6):388–403
Hajian-Tilaki K, Heidari B, Hajian-Tilaki A (2016) Solitary and combined negative influences of diabetes, obesity and hypertension on health-related quality of life of elderly individuals: A population-based cross-sectional study. Diabetes Metab Syndr (Epub ahead of print). doi:10.1016/j.dsx.2016.01.018
Hoopman R, Terwee CB, Muller MJ, Aaronson NK (2006) Translation and validation of the SF-36 Health Survey for use among Turkish and Moroccan ethnic minority cancer patients in The Netherlands. Eur J Cancer 42(17):2982–2990
Jadambaa A, Spickett J, Badrakh B, Norman RE (2015) The impact of the environment on health in Mongolia: a systematic review. Asia Pac J Public Health 27(1):45–75
James AL, Palmer LJ, Kicic E, Maxwell PS, Lagan SE, Ryan GF et al (2005) Decline in lung function in the Buusselton Health Study. The effects of asthma and cigarette smoking. Am J Respir Crit Care Med 171:109–114
Jenkinson C, Jenkinson D, Shepperd S, Petersen S (1997) Evaluation of treatment for congestive heart failure in patients aged 60 years and older using generic measures of health status (SF-36 and COOP charts). Age Ageing 26(1):7–13
Kitaoka M, Mitoma J, Asakura H, Anyenda OE, Ngyuyen TTT, Hamagishi T et al (2016) The relationship between hypertension and health-related quality of life: adjusted by chronic pain, chronic diseases, and life habits in the general middle-aged population in Japan. Environ Health Prev Med (Epub ahead of print). doi:10.1007/s12199-016-0514-6
Li L, Wang HM, Shen Y (2003) Chinese SF-36 Health Survey: translation, cultural adaptation, validation, and normalization. J Epidemiol Community Health 57(4):259–263
Mahler DA, Mackowiak JI (1995) Evaluation of the Short-Form 36-Item Questionnaire to measure health-related quality of life in patients with COPD. Chest 107:1585–1589
Matcham F, Scott IC, Rayner L, Hotopf M, Kingsley GH, Norton S et al (2014) The impact of rheumatoid arthritis on quality-of-life assessed using the SF-36: a systematic review and meta-analysis. Semin Arthritis Rheum 44(2):123–130
Mbada CE, Adeogun GA, Ogunlana MO, Adedoyin RA, Akinsulore A, Awotidebe TO et al (2015) Translation, cross-cultural adaptation and psychometric evaluation of Yoruba version of the short-form 36 health survey. Health Qual Life Outcomes 13:141
McHorney CA, Ware JE, Raczek AE (1993) The MOS 36-item short-from health survey (SF-36): II Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med Care 3:247–263
Mosconi P, Apolone G, Barni S, Secondino S, Sbanotto A, Filiberti A (2002) Quality of life in breast and colon cancer long-term survivors: an assessment with the EORTC QLD-C30 and SF-36 questionnaires. Tumori 88(2):110–116
Papaioannou D, Brazier J, Parry G (2011) How valid and responsive are generic health status measures, such as EQ-5D and SF-36, in schizophrenia? A systematic review. Value Health 14(6):907–920
Prata J, Martins AQ, Ramos S, Rocha-Gonçalves Coelho R (2016) Gender differences in quality of life perception and cardiovascular risk in a community sample. Rev Port Cardiol 35(3):153–160
Prieto L, Alonso J, Ferrer M, Anto JM, Quality of Life in COPD Study Group (1997) Are results of the SF-36 health survey and the Nottingham Health Profile similar? A comparison in COPD patients. J Clin Epidemiol 50(4):463–473
Sasaki H, Nakamura M, Kida A, Kambe M, Takahashi K, Fujimura M et al (2001) Reference values of spirogram and arterial blood gas levels in Japanese. Ann Jpn Respir Soc 39:1–17
Sonomjamts M, Dashdemberel S, Logii N, Nakae K, Chigusa Y, Ohhira S et al (2014) Prevalence of asthma and allergic rhinitis among adult population in Ulaanbaatar, Mongolia. Asia Pac Allergy 4:25–31
United nations Economic and Social Commission for Asia and the Pacific, ESCAP Statistical Database (2014) Statistical yearbook for Asia and the Pacific 2014. http://www.unescap.org/sites/default/files/ESCAP-SYB2014_0.pdf. Accessed 11 Oct 2015
United nations Economic and Social Commission for Asia and the Pacific, ESCAP Statistical Database (2015) http://www.unescap.org/stat/data/statdb/DataExplorer.aspx. Accessed 11 Oct 2015
van Weel C (1993) Functional status in primary care: COOP/WONCA charts. Disabil Rehabil 15:96–101
Viinanen A, Munkhbayarlah S, Zevgee T, Narantsetseg L, Ts Naidansuren, Koskenvuo M et al (2005) Prevalence of asthma, allergic rhino conjunctivitis and allergic sensitization in Mongolia. Allergy 60:1370–1377
Ware JE Jr, Kosinski M, Gandek B, Aaronson NK, Apolone G, Bech P et al (1998) The factor structure of the SF36 health survey in 10 countries: results from the IQOLA project. J Clin Epidemiol 51(11):1159–1165
World Health Organization (WHO) (2014) Ambient (outdoor) air pollution database 2014, by country and city. http://www.who.int/entity/quantifying_ehimpacts/national/countryprofile/aap_pm_database_may2014.xls?ua=1. Accessed 11 Oct 2015
Xu X, Dockery DW, Ware JH, Speizer FE, Ferris BG Jr (1992) Effects of cigarette smoking on rate of loss of pulmonary function in adults: a longitudinal assessment. Am Rev Respir Dis 146:1345–1348
Yamaguchi M, Nakao M, Obata H, Ikeda H, Kanda T, Wang Q et al (2013) Application of the COOP/WONCA charts to aged patients with chronic obstructive pulmonary disease: a comparison between Japanese and Chinese populations. BMC Public Health 13:754–764
Authors’ contributions
MN was an assistant Professor at Kurume University and was involved in the literature search, data collection, data editing, analysis, interpretation, and preparation of the manuscript. He took the lead in developing this manuscript. KY was an advisor and was involved in the literature search and data collection, and helped with drafting of the manuscript. YI supervised MN and was involved in the literature search; data collection, editing, analysis, and interpretation; provided discussion and advice; helped with manuscript preparation; and participated in the development of the study proposal. She also supervised all aspects of this study. RB was an advisor and was actively involved in translation of the SF-36v2, and helped with drafting of the manuscript. BS and DI were advisors and were actively involved in data collection in Ulaanbaatar, Mongolia, and helped with drafting of the manuscript. All authors read and approved the final manuscript.
Acknowledgements
The authors would like to express their deep gratitude to Dr. Go Hasegawa, Ms. Tomoe Terasaki, Ms. Midori Yamaguchi, and Dr. Fumiko Ono of Kurume University, and Prof. Hisamitsu Omori of Kumamoto University. We also extend our appreciation to all the doctors who provided the valuable data used in this study, which was conducted in Ulaanbaatar, Mongolia.
Competing interests
The authors declare that they have no competing interests.
Ethics approval and informed consent
As shown in methods section, the present study was approved by the Clinical Ethical Review Board of Kurume University School of Medicine. Before investigation, the participants were provided with explanations in person as to the purpose and method of the study, as well as information regarding the handling of the results. The study was carried out upon receipt of written consent.
Funding
This study was supported in part by Grants-in-Aid for Scientific Research (B) 20406001, 23406001 and (C) 26340053 and a “MEXT-Supported Program for the Strategic Research Foundation at Private Universities” from the Ministry of Education, Culture, Sports, Science and Technology (MEXT) in Japan.
Author information
Authors and Affiliations
Corresponding author
Additional files
40064_2016_2204_MOESM1_ESM.docx
Additional file 1: Table S1. Japanese subjects who visited the healthcare center in the Kumamoto prefecture (Japan) were recruited into our study. Administration of the self-completed questionnaire, body measurements, and medical examination were performed in male and female participants aged 40–79 years, and 855 subjects were eligible for analysis.
40064_2016_2204_MOESM2_ESM.docx
Additional file 2: Table S2. In the Japanese SF-36v2, the RP, GH, BP, and RE subscales consisted of the same items as the English version. Although the VT and MH factors were composed of two factors, the questions making up these subscales were not identical to the English SF-36v2. One of the factors of the VT/MH subscales included questions in the SF subscale. Two of the questions that constituted the PF subscale were classified as another independent factor. The highest factor loadings in each observed variable were expressed as italic.
40064_2016_2204_MOESM3_ESM.docx
Additional file 3: Table S3. There were no significant differences in health status measured by SF-36v2 between never-smokers and ever-smokers (ex- and current-smokers) in any of the ventilatory impairment groups.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Nakao, M., Yamauchi, K., Ishihara, Y. et al. Validation of the Mongolian version of the SF-36v2 questionnaire for health status assessment of Mongolian adults. SpringerPlus 5, 607 (2016). https://doi.org/10.1186/s40064-016-2204-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40064-016-2204-7